Identification of a Plasma Microrna Signature as Biomarker of Subaneurysmal Aortic Dilation in Patients with High Cardiovascular Risk


Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design and Population
2.2. Sample Collection
2.3. RNA Isolation
2.4. cDNA Synthesis and Identification of Plasma miR Expression Profiling
2.5. Validation of Plasma miR Expression Profiling by qRT-PCR Analysis
2.6. Target Gene Prediction and Functional Enrichment Analysis
2.7. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Patients
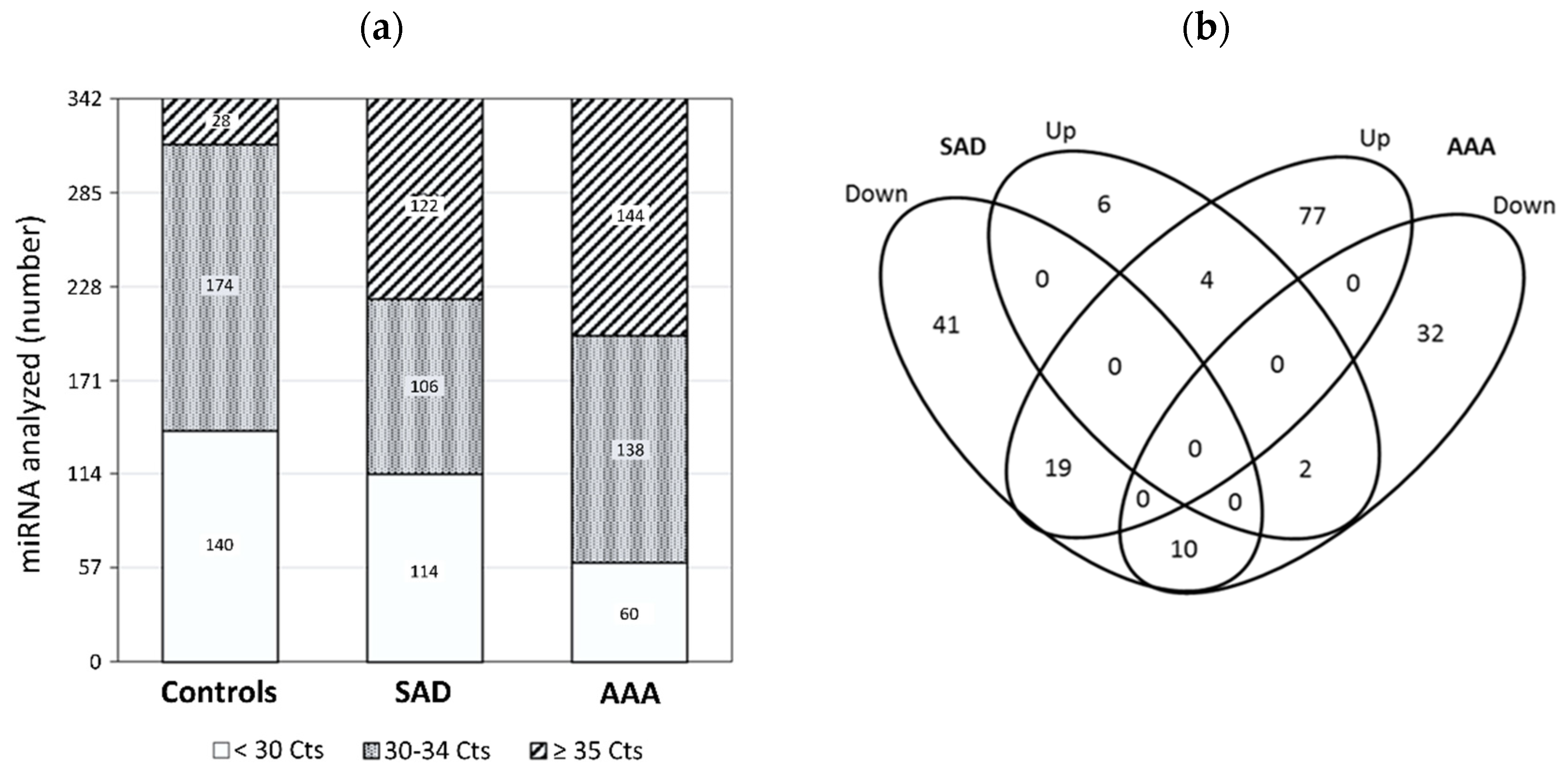
3.2. Identification of Plasma miRs Differentially Expressed in Patients with SAD
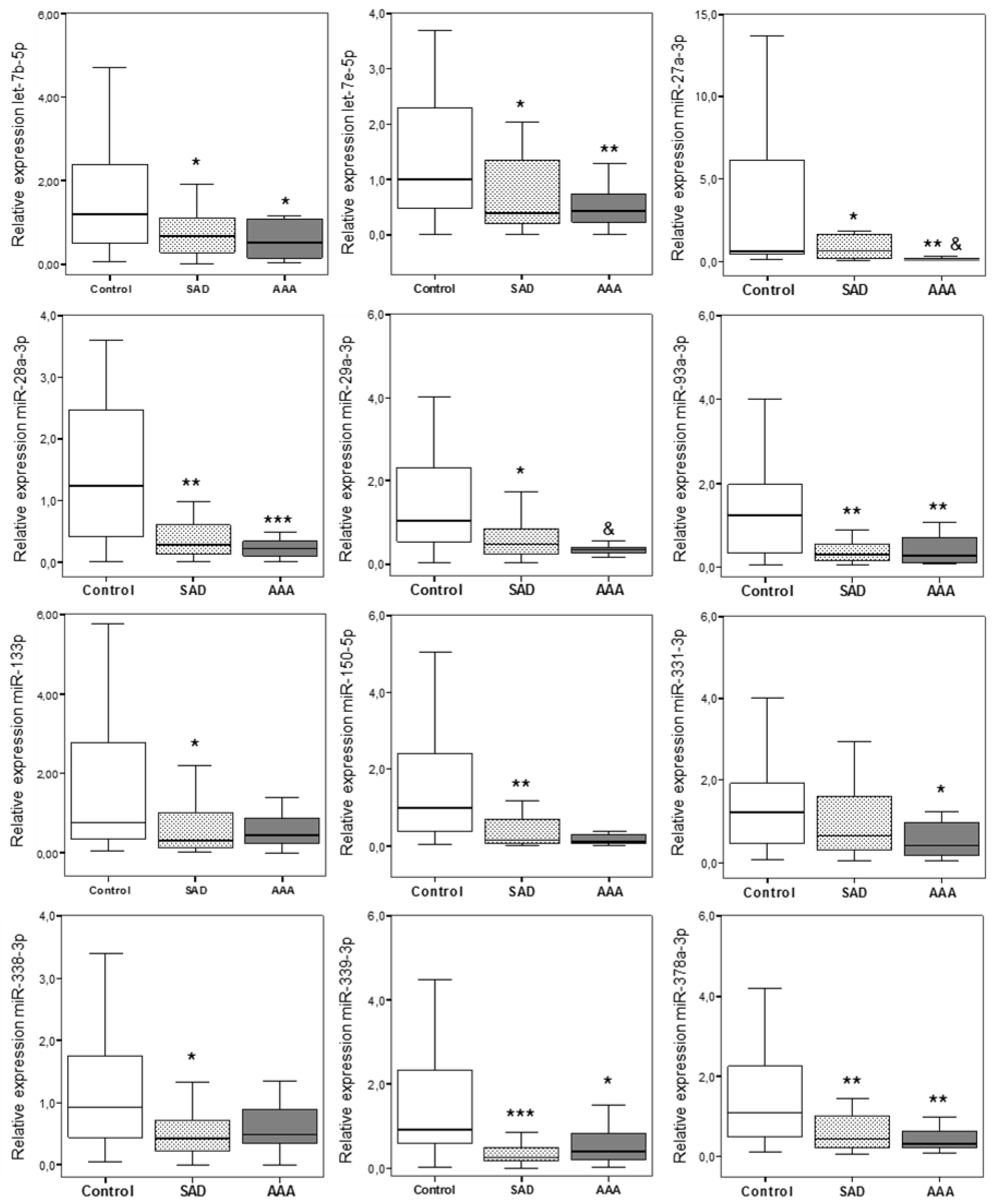
3.3. Validation of miR Expression by Individual qRT-PCR
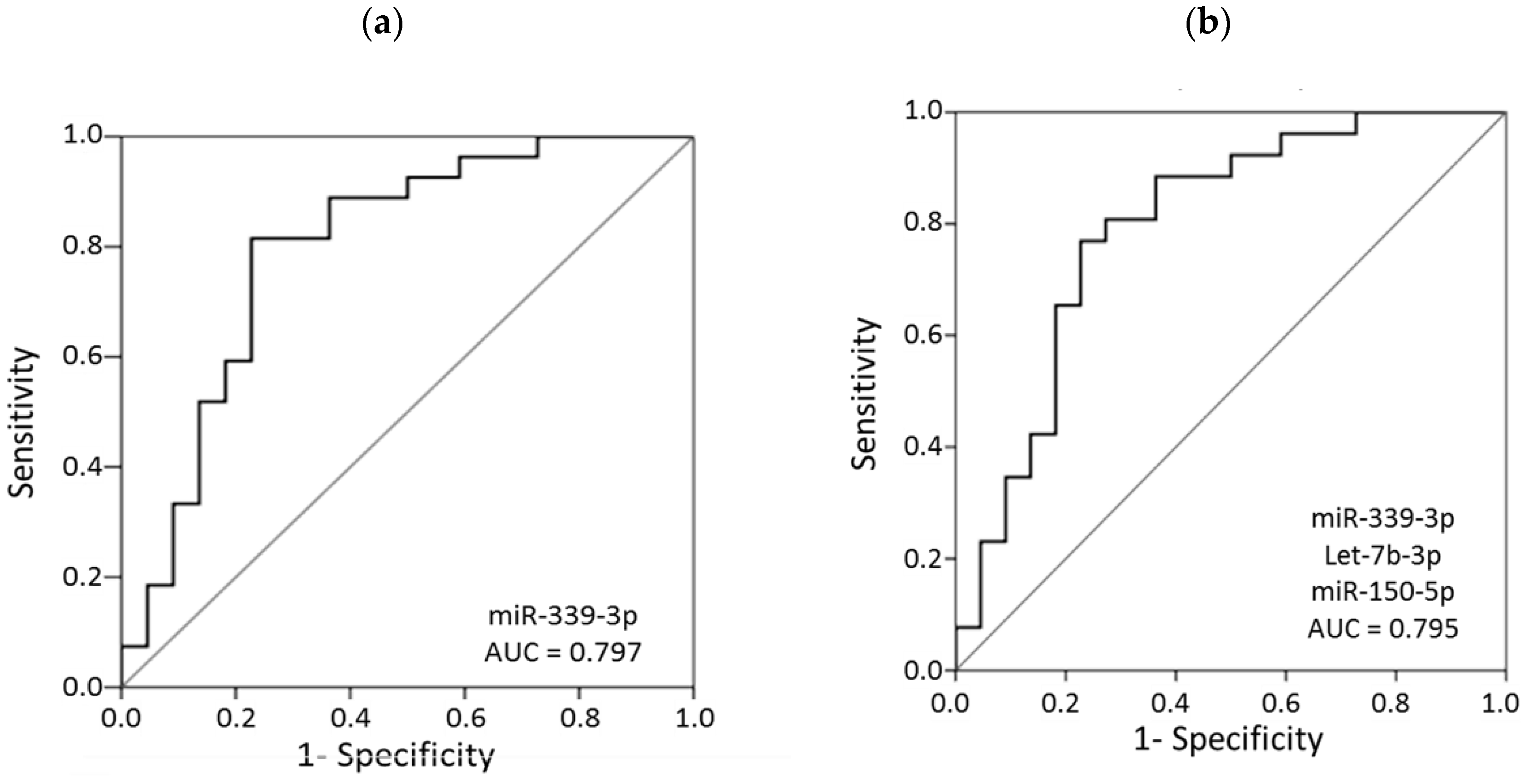
3.4. Plasma miRs as Predictors of SAD in Patients with High Cardiovascular Risk
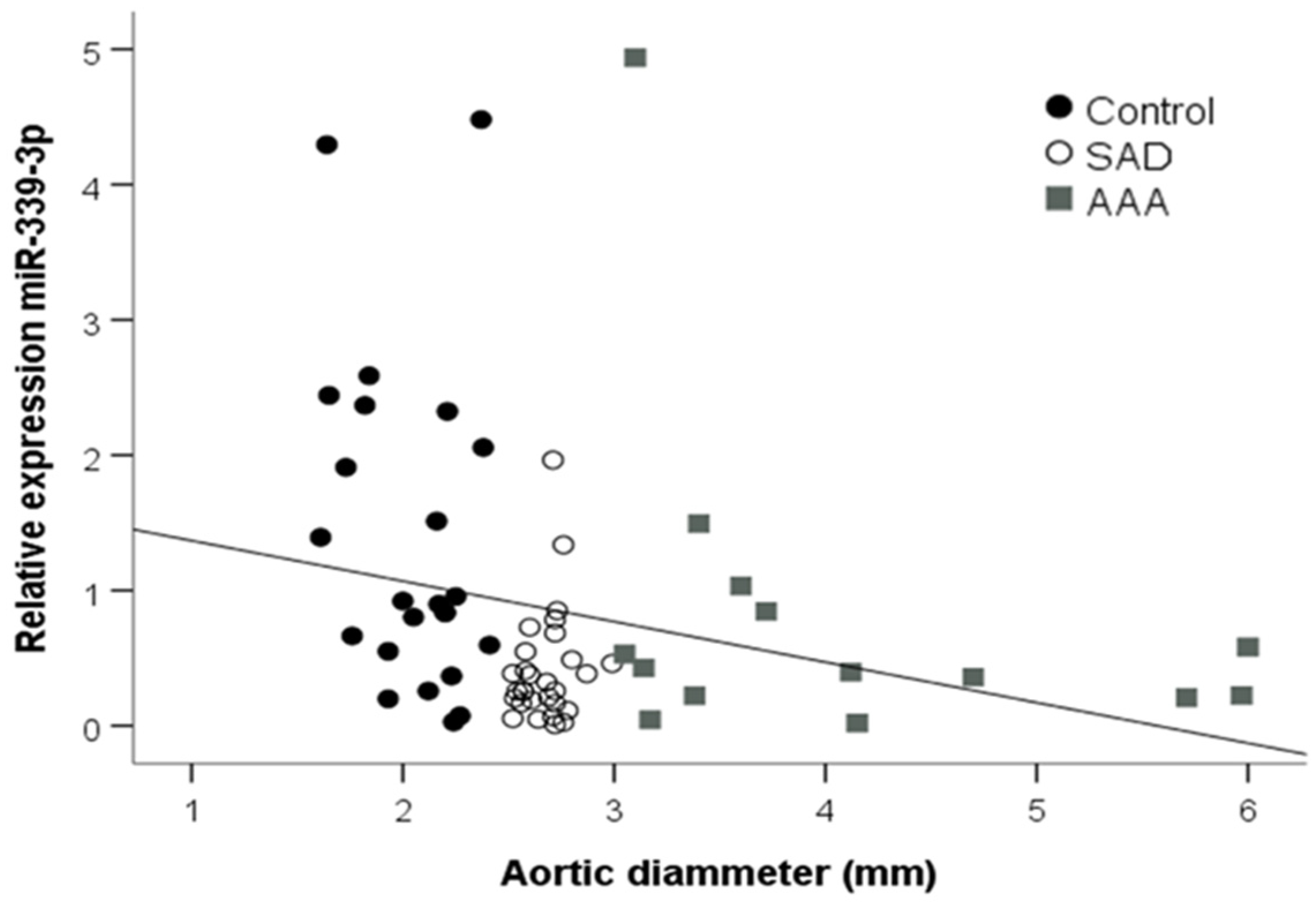
3.5. Correlations of miRs with Clinical Parameters
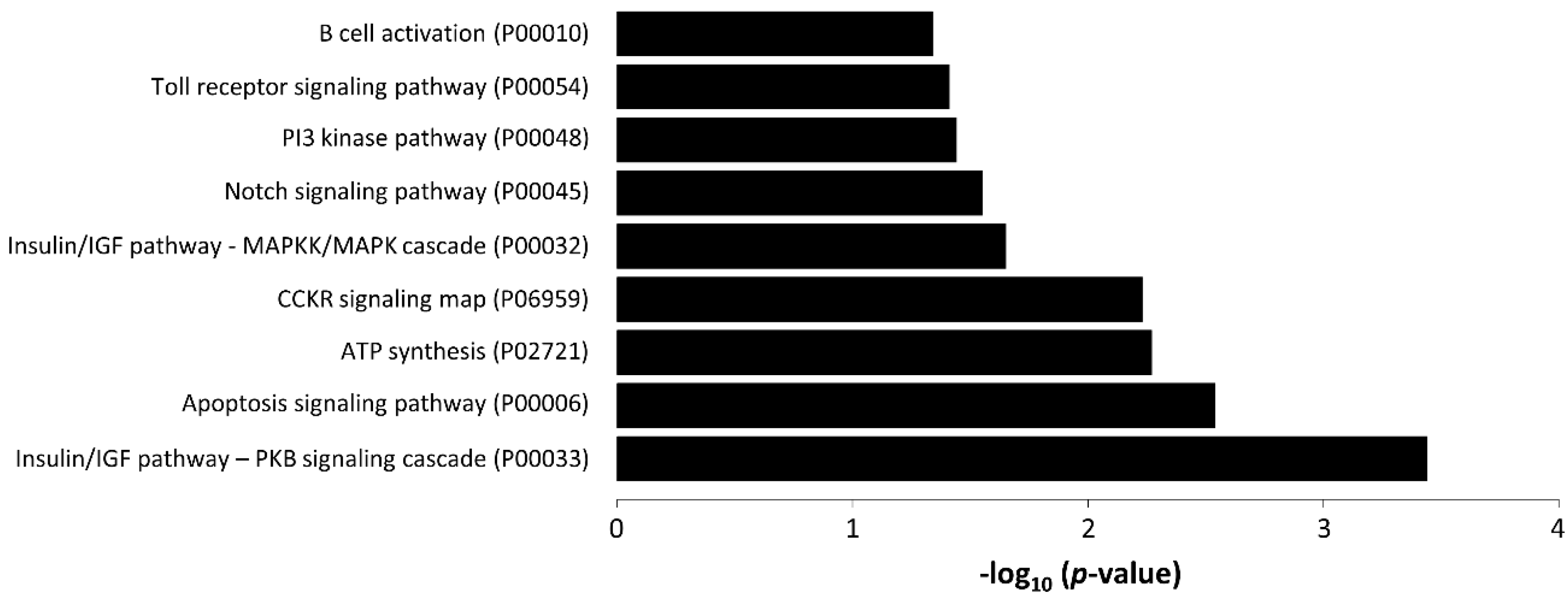
3.6. Target Gene Prediction and Functional Enrichment Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Heikkinen, M.; Salenius, J.P.; Auvinen, O. Ruptured abdominal aortic aneurysm in a well-defined geographic area. J. Vasc. Surg. 2002, 36, 291–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dabare, D.; Lo, T.T.; McCormack, D.J.; Kung, V.W. What is the role of screening in the management of abdominal aortic aneurysms? Interact. Cardiovasc. Thorac. Surg. 2012, 14, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Kent, K.C. Abdominal aortic aneurysms. N. Engl. J. Med. 2014, 371, 2101–2108. [Google Scholar] [CrossRef] [PubMed]
- U.S. Preventive Services Task Force; Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Doubeni, C.A.; Epling, J.W.; Kubik, M.; et al. Screening for abdominal aortic aneurysm. JAMA 2019, 322, 2211–2218. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, R.J.; Shaw, E.; Whyman, M.R.; Earnshaw, J.; Poskitt, K.R.; Heather, B.P. Recommendations for screening intervals for small aortic aneurysms. BJS 2003, 90, 821–826. [Google Scholar] [CrossRef]
- Lindholt, J.; Vammen, S.; Juul, S.; Fasting, H.; Henneberg, E.; Lindholt, J.S. Optimal interval screening and surveillance of abdominal aortic aneurysms. Eur. J. Vasc. Endovasc. Surg. 2000, 20, 369–373. [Google Scholar] [CrossRef]
- Norman, P.E.; Muller, J.; Golledge, J. The cardiovascular and prognostic significance of the infrarenal aortic diameter. J. Vasc. Surg. 2011, 54, 1817–1820. [Google Scholar] [CrossRef] [Green Version]
- Saucedo, M.C.; García-Gil, D.; Romero, F.B.; Rego, A.T.D.; Romero, L.B.; Sala, E.R.; Guerra, G.A.; Martínez, J.V.; Rojo, J.C.; Macho, J.T.; et al. Prevalence of abdominal aortic aneurysm in patients with high cardiovascular risk. Rev. Clin. Esp. 2018, 218, 461–467. [Google Scholar] [CrossRef]
- Wild, J.; Stather, P.; Biancari, F.; Choke, E.; Earnshaw, J.; Grant, S.; Hafez, H.; Holdsworth, R.; Juvonen, T.; Lindholt, J.S.; et al. A Multicentre Observational study of the outcomes of screening detected sub-aneurysmal aortic dilatation. Eur. J. Vasc. Endovasc. Surg. 2013, 45, 128–134. [Google Scholar] [CrossRef] [Green Version]
- Duncan, J.L.; Harrild, K.A.; Iversen, L.; Lee, A.J.; Godden, D.J. Long term outcomes in men screened for abdominal aortic aneurysm: Prospective cohort study. BMJ 2012, 344, e2958. [Google Scholar] [CrossRef] [Green Version]
- Chun, K.C.; Anderson, R.C.; Smothers, H.C.; Sood, K.; Irwin, Z.T.; Wilson, M.D.; Lee, E.S. Risk of developing an abdominal aortic aneurysm after ectatic aorta detection from initial screening. J. Vasc. Surg. 2020, 71, 1913–1919. [Google Scholar] [CrossRef] [PubMed]
- Schäberle, W.; Leyerer, L.; Schierling, W.; Pfister, K. Ultrasound diagnostics of the abdominal aorta. Gefässchirurgie 2015, 20, 22–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnafy, T.; Lacroix, P.; Desormais, I.; Labrunie, A.; Marin, B.; Leclerc, A.; Oueslati, A.; Rollé, F.; Vignon, P.; Aboyans, V. Reliability of the measurement of the abdominal aortic diameter by novice operators using a pocket-sized ultrasound system. Arch. Cardiovasc. Dis. 2013, 106, 644–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, J.; Hayder, H.; Zayed, Y.; Peng, C. Overview of microRNA biogenesis, mechanisms of actions, and circulation. Front. Endocrinol. 2018, 9, 402. [Google Scholar] [CrossRef] [Green Version]
- Siasos, G.; Bletsa, E.; Stampouloglou, P.K.; Oikonomou, E.; Tsigkou, V.; Paschou, S.A.; Vlasis, K.; Marinos, G.; Vavuranakis, M.; Stefanadis, C.; et al. MicroRNAs in cardiovascular disease. Hell. J. Cardiol. 2020. [Google Scholar] [CrossRef]
- Raffort, J.; Lareyre, F.; Clement, M.; Mallat, Z. Micro-RNAs in abdominal aortic aneurysms: Insights from animal models and relevance to human disease. Cardiovasc. Res. 2016, 110, 165–177. [Google Scholar] [CrossRef] [Green Version]
- Iyer, V.; Rowbotham, S.; Biros, E.; Bingley, J.; Golledge, J. A systematic review investigating the association of microRNAs with human abdominal aortic aneurysms. Atherosclerosis 2017, 261, 78–89. [Google Scholar] [CrossRef]
- Chen, X.; Ba, Y.; Ma, L.; Cai, X.; Yin, Y.; Wang, K.; Guo, J.; Zhang, Y.; Chen, J.; Guo, X.; et al. Characterization of microRNAs in serum: A novel class of biomarkers for diagnosis of cancer and other diseases. Cell Res. 2008, 18, 997–1006. [Google Scholar] [CrossRef] [Green Version]
- Farr, R.J.; Januszewski, A.S.; Joglekar, M.V.; Liang, H.; McAulley, A.K.; Hewitt, A.W.; Thomas, H.E.; Loudovaris, T.; Kay, T.W.; Jenkins, A.; et al. A comparative analysis of high-throughput platforms for validation of a circulating microRNA signature in diabetic retinopathy. Sci. Rep. 2015, 5, 10375. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Shang, T.; Huang, C.; Yu, T.; Liu, C.; Qiao, T.; Huang, D.; Liu, Z.; Liu, C.J. Plasma microRNAs serve as potential biomarkers for abdominal aortic aneurysm. Clin. Biochem. 2015, 48, 988–992. [Google Scholar] [CrossRef]
- Wanhainen, A.; Mani, K.; Vorkapic, E.; De Basso, R.; Björck, M.; Länne, T.; Wågsäter, D. Screening of circulating microRNA biomarkers for prevalence of abdominal aortic aneurysm and aneurysm growth. Atherosclerosis 2017, 256, 82–88. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Liu, D.; Chen, X.; Li, J.; Li, L.; Bian, Z.; Sun, F.; Lu, J.; Yin, Y.; Cai, X.; et al. Secreted monocytic mir-150 enhances targeted endothelial cell migration. Mol. Cell 2010, 39, 133–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef] [PubMed]
- Marín-Royo, G.; Ortega-Hernández, A.; Martínez-Martínez, E.; Jurado-López, R.; Luaces, M.; Islas, F.; Gómez-Garre, D.; Delgado-Valero, B.; Lagunas, E.; Ramchandani, B.; et al. The impact of cardiac lipotoxicity on cardiac function and mirnas signature in obese and non-obese rats with myocardial infarction. Sci. Rep. 2019, 9, 444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mestdagh, P.; Van Vlierberghe, P.; De Weer, A.; Muth, D.; Westermann, F.; Speleman, F.; Vandesompele, J. A novel and universal method for microRNA RT-qPCR data normalization. Genome Biol. 2009, 10, R64. [Google Scholar] [CrossRef] [Green Version]
- Fan, Y.; Siklenka, K.; Arora, S.K.; Ribeiro, P.; Kimmins, S.; Xia, J. MiRNet—Dissecting miRNA-target interactions and functional associations through network-based visual analysis. Nucleic Acids Res. 2016, 44, W135–W141. [Google Scholar] [CrossRef]
- Mi, H.; Huang, X.; Muruganujan, A.; Tang, H.; Mills, C.; Kang, D.; Thomas, P.D. PANTHER version 11: Expanded annotation data from Gene Ontology and Reactome pathways, and data analysis tool enhancements. Nucleic Acids Res. 2016, 45, D183–D189. [Google Scholar] [CrossRef] [Green Version]
- Biroš, E.; Moran, C.S.; Wang, Y.; Walker, P.J.; Cardinal, J.; Golledge, J. MicroRNA profiling in patients with abdominal aortic aneurysms: The significance of miR-155. Clin. Sci. 2014, 126, 795–803. [Google Scholar] [CrossRef] [PubMed]
- Kin, K.; Miyagawa, S.; Fukushima, S.; Shirakawa, Y.; Torikai, K.; Shimamura, K.; Daimon, T.; Kawahara, Y.; Kuratani, T.; Sawa, Y. Tissue- and plasma-specific microRNA signatures for atherosclerotic abdominal aortic aneurysm. J. Am. Heart Assoc. 2012, 1, e000745. [Google Scholar] [CrossRef] [Green Version]
- Annambhotla, S.; Bourgeois, S.; Wang, X.; Lin, P.H.; Yao, Q.; Chen, C. Recent advances in molecular mechanisms of abdominal aortic aneurysm formation. World J. Surg. 2008, 32, 976–986. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Komers, R.; Carew, R.; Winbanks, C.E.; Xu, B.; Herman-Edelstein, M.; Koh, P.; Thomas, M.; Jandeleit-Dahm, K.; Gregorevic, P.; et al. Suppression of microRNA-29 expression by TGF-β1 promotes collagen expression and renal fibrosis. J. Am. Soc. Nephrol. 2011, 23, 252–265. [Google Scholar] [CrossRef] [Green Version]
- Jones, J.A.; Stroud, R.E.; O’Quinn, E.C.; Black, L.E.; Barth, J.L.; Elefteriades, J.A.; Bavaria, J.E.; Gorman, J.H.; Gorman, R.C.; Spinale, F.G.; et al. Selective microRNA suppression in human thoracic aneurysms: Relationship of miR-29a to aortic size and proteolytic induction. Circ. Cardiovasc. Genet. 2011, 4, 605–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Wang, M.; Zhang, J.; Xu, P.; Wang, H. MicroRNA-29a-3p regulates abdominal aortic aneurysm development and progression via direct interaction with PTEN. J. Cell. Physiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Robinson, H.C.; Baker, A.H. How do microRNAs affect vascular smooth muscle cell biology? Curr. Opin. Lipidol. 2012, 23, 405–411. [Google Scholar] [CrossRef]
- Fang, Y.C.; Yeh, C.H. Role of microRNAs in vascular remodeling. Curr. Mol. Med. 2015, 15, 684–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, M.H.; Feng, X.; Zhang, Y.W.; Lou, X.Y.; Cheng, Y.; Zhou, H.H. Let-7 in cardiovascular diseases, heart development and cardiovascular differentiation from stem cells. Int. J. Mol. Sci. 2013, 14, 23086–23102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meeuwsen, J.; van Hof, F.T.; Van Rheenen, W.; Rinkel, G.; Veldink, J.H.; Ruigrok, Y.M. Circulating microRNAs in patients with intracranial aneurysms. PLoS ONE 2017, 12, e0176558. [Google Scholar] [CrossRef] [Green Version]
- Sawada, H.; Naito, Y.; Oboshi, M.; Soyama, Y.; Nishimura, K.; Eguchi, A.; Ando, T.; Okuhara, Y.; Morisawa, D.; Iwasaku, T.; et al. Increment of pentraxin3 expression in abdominal aortic aneurysm. Int. J. Cardiol. 2015, 195, 281–282. [Google Scholar] [CrossRef]
- Luo, X.Y.; Zhu, X.Q.; Li, Y.; Wang, X.B.; Yin, W.; Ge, Y.S.; Ji, W.-M. MicroRNA-150 restores endothelial cell function and attenuates vascular remodeling by targeting PTX3 through the NF-κB signaling pathway in mice with acute coronary syndrome. Cell Biol. Int. 2018, 42, 1170–1181. [Google Scholar] [CrossRef]
- Chen, J.; Cui, X.; Li, L.; Qu, J.; Raj, J.U.; Gou, D. MiR-339 inhibits proliferation of pulmonary artery smooth muscle cell by targeting FGF signaling. Physiol. Rep. 2017, 5, e13441. [Google Scholar] [CrossRef]
- Li, H.; Bai, S.; Ao, Q.; Wang, X.; Tian, X.; Li, X.; Tong, H.; Hou, W.; Fan, J. Modulation of immune-inflammatory responses in abdominal aortic aneurysm: Emerging molecular targets. J. Immunol. Res. 2018, 2018, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Xing, L.; Zeng, C.; Wu, T.; Gui, Y.; Li, W.; Lan, T.; Yang, Y.; Gu, Q.; Qi, C.; et al. Inactivation of PI3K induces vascular injury and promotes aneurysm development by upregulating the AP-1/MMP-12 pathway in macrophages. Arter. Thromb. Vasc. Biol. 2014, 35, 368–377. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.Y.; Simons, M.; Friesel, R. FRS2 via fibroblast growth factor receptor 1 is required for platelet-derived growth factor receptor β-mediated regulation of vascular smooth muscle marker gene expression. J. Biol. Chem. 2009, 284, 15980–15992. [Google Scholar] [CrossRef] [Green Version]
- Vele, E.; Kurtcehajic, A.; Zerem, E.; Maskovic, J.; Alibegovic, E.; Hujdurovic, A. Plasma D-dimer as a predictor of the progression of abdominal aortic aneurysm. J. Thromb. Haemost. 2016, 14, 2298–2303. [Google Scholar] [CrossRef] [PubMed]
- Saw, S.T.; Leong, B.; Aziz, D.A. Early detection of undiagnosed abdominal aortic aneurysm and sub-aneurysmal aortic dilatations in patients with high-risk coronary artery disease: The value of targetted screening programme. Vasc. Health Risk Manag. 2020, 16, 215–229. [Google Scholar] [CrossRef] [PubMed]
- Lu, B.; Liu, L.; Wang, J.; Chen, Y.; Li, Z.; Gopinath, S.C.B.; Lakshmipriya, T.; Huo, Z. Detection of microRNA-335-5p on an interdigitated electrode surface for determination of the severity of abdominal aortic aneurysms. Nanoscale Res. Lett. 2020, 15, 1–8. [Google Scholar] [CrossRef]
- Azimzadeh, M.; Rahaie, M.; Nasirizadeh, N.; Daneshpour, M.; Naderi-Manesh, H. Electrochemical miRNA biosensors: The benefits of nanotechnology. Nanomed. Res. J. 2017, 2, 36–48. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | CT | SAD | AAA | |
|---|---|---|---|---|
| (n = 300) | (n = 231) | (n = 47) | (n = 22) | |
| Age, years | 67 ± 3 | 67 ± 3 | 66 ± 5 | 75 ± 3 * |
| Male, n (%) | 162 (54.0) | 105 (45.5) | 40 (85.1) * | 17 (77.3) * |
| BMI, kg/m2 | 28.3 ± 1.1 | 28.4 ± 1.0 | 28.7 ± 1.7 | 27.5 ± 2.3 |
| WC, cm | 98 ± 3 | 97 ± 3 | 101 ± 4 | 100 ± 4 |
| Smoking habits, n (%) | 131 (35.7) | 85 (36.8) | 31 (66.0) * | 15 (68.2) * |
| Alcohol, n (%) | 51 (17.1) | 29 (12.6) | 16 (34.0) * | 6 (27.3) * |
| Hypertension, n (%) | 300 (100) | 231 (100) | 47 (100) | 22 (100) |
| SBP (mmHg) | 140 ± 3 | 141 ± 3 | 140 ± 4 | 132 ± 7 |
| DBP (mmHg) | 80 ± 5 | 80 ± 3 | 80 ± 5 | 75 ± 4 |
| Dyslipidemia, n (%) | 178 (59.3) | 134 (58.0) | 31 (66.0) | 13 (59.1) |
| Triglycerides, mg/dL | 96 (74–134) | 98 (74–129) | 110 (71–156) | 102 (80–142) |
| TC, mg/dL | 188 ± 8 | 189 ± 8 | 182 ± 11 | 163 ± 13 * |
| LDL-c, mg/dL | 111 ± 7 | 111 ± 7 | 111 ± 10 | 92 ± 14 |
| HDL-c, mg/dL | 54 ± 3 | 52 ± 3 | 53 ± 5 | 47 ± 6 * |
| T2DM, n (%) | 66 (22.0) | 50 (21.6) | 11 (23.4) | 5 (22.7) |
| Glucose, mg/dL | 99 (90–111) | 99 (89–111) | 98 (94–116) | 99 (90–119) |
| CHD, n (%) | 19 (6.3) | 9 (3.9) | 6 (12.8) * | 4 (18.2) * |
| CVD, n (%) | 23 (7.7) | 16 (6.9) | 6 (12.8) * | 1 (4.5) |
| PAD, n (%) | 12 (4.0) | 6 (2.6) | 2 (4.3) * | 4 (18.2) * |
| eGFR, ml/min/1.72 m2 | 84.0 ± 4.5 | 84.5 ± 4.3 | 86.0 ± 7.3 | 70.5 ± 7.5 * |
| AUC | 95% Confidence Interval | Specificity * | p-Value | |
|---|---|---|---|---|
| miR-339-3p † | 0.797 | 0.665–0.930 | 77.3 | <0.001 |
| miR-28-3p | 0.741 | 0.599–0.884 | 54.5 | 0.004 |
| miR-93-3p | 0.731 | 0.582–0.880 | 63.6 | 0.006 |
| miR-378a-3p | 0.731 | 0.589–0.873 | 40.9 | 0.006 |
| miR-150-5p | 0.729 | 0.583–0.875 | 45.5 | 0.007 |
| miR-338-3p | 0.713 | 0.560–0.867 | 54.5 | 0.012 |
| miR-29a-3p | 0.710 | 0.562–0.857 | 38.7 | 0.013 |
| let-7b-5p | 0.698 | 0.546–0.849 | 45.5 | 0.019 |
| miR-133b | 0.687 | 0.538–0.836 | 34.1 | 0.027 |
| let-7e-5p | 0.677 | 0.524–0.829 | 31.8 | 0.037 |
| miR-331-3p | 0.626 | 0.467–0.785 | 31.8 | 0.136 |
| miR-27a-3p | 0.542 | 0.377–0.707 | 27.3 | 0.619 |
| r | p-Value | |
|---|---|---|
| let-7b-5p | −0.172 | 0.184 |
| let-7e-5p | −0.363 | 0.005 |
| miR-27a-3p | −0.295 | 0.021 |
| miR-28-3p | −0.392 | 0.002 |
| miR-29a-3p | −0.519 | <0.001 |
| miR-93-3p | −0.354 | 0.005 |
| miR-133b | −0.311 | 0.017 |
| miR-150-5p | −0.477 | <0.001 |
| miR-331-3p | −0.282 | 0.030 |
| miR-338-3p | −0.259 | 0.044 |
| miR-339-3p | −0.345 | <0.001 |
| miR-378a-3p | −0.349 | 0.007 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torres-Do Rego, A.; Barrientos, M.; Ortega-Hernández, A.; Modrego, J.; Gómez-Gordo, R.; Álvarez-Sala, L.A.; Cachofeiro, V.; Gómez-Garre, D. Identification of a Plasma Microrna Signature as Biomarker of Subaneurysmal Aortic Dilation in Patients with High Cardiovascular Risk. J. Clin. Med. 2020, 9, 2783. https://doi.org/10.3390/jcm9092783
Torres-Do Rego A, Barrientos M, Ortega-Hernández A, Modrego J, Gómez-Gordo R, Álvarez-Sala LA, Cachofeiro V, Gómez-Garre D. Identification of a Plasma Microrna Signature as Biomarker of Subaneurysmal Aortic Dilation in Patients with High Cardiovascular Risk. Journal of Clinical Medicine. 2020; 9(9):2783. https://doi.org/10.3390/jcm9092783
Chicago/Turabian StyleTorres-Do Rego, Ana, María Barrientos, Adriana Ortega-Hernández, Javier Modrego, Rubén Gómez-Gordo, Luis A. Álvarez-Sala, Victoria Cachofeiro, and Dulcenombre Gómez-Garre. 2020. "Identification of a Plasma Microrna Signature as Biomarker of Subaneurysmal Aortic Dilation in Patients with High Cardiovascular Risk" Journal of Clinical Medicine 9, no. 9: 2783. https://doi.org/10.3390/jcm9092783
APA StyleTorres-Do Rego, A., Barrientos, M., Ortega-Hernández, A., Modrego, J., Gómez-Gordo, R., Álvarez-Sala, L. A., Cachofeiro, V., & Gómez-Garre, D. (2020). Identification of a Plasma Microrna Signature as Biomarker of Subaneurysmal Aortic Dilation in Patients with High Cardiovascular Risk. Journal of Clinical Medicine, 9(9), 2783. https://doi.org/10.3390/jcm9092783