Deep Brain Stimulation for Treatment-Resistant Depression: Towards a More Personalized Treatment Approach

 , ,
, ,
Abstract
:1. Introduction
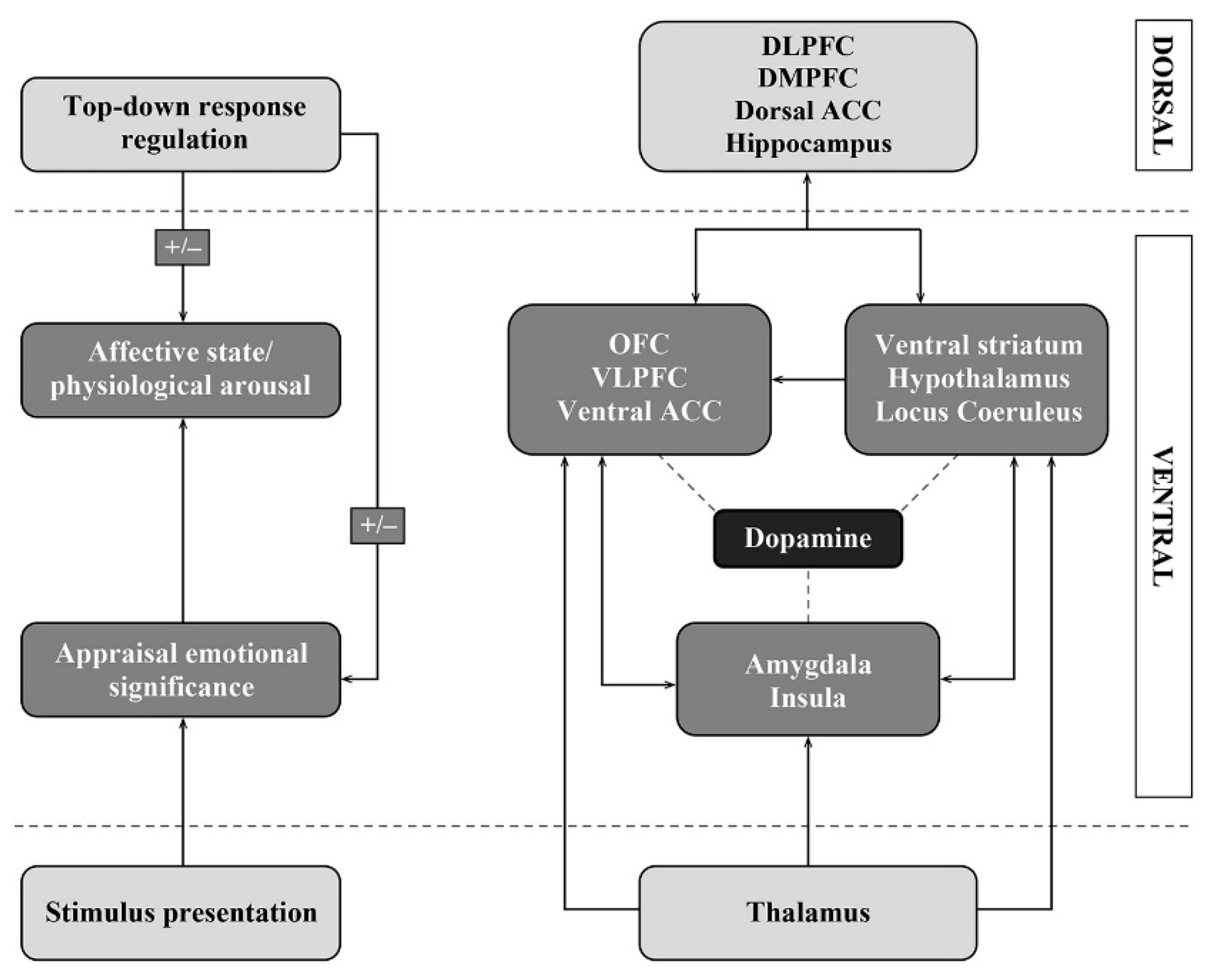
2. Recent Insights on the Pathophysiology of Depression
Expanding the Cortico-Striatal-Thalamo-Cortical Mood Circuits
3. Deep Brain Stimulation for Treatment-Resistant Depression
3.1. Subgenual Cingulate Gyrus/Cortex
3.2. Nucleus Accumbens
3.3. Ventral Capsule/Ventral Striatum
3.4. The Ventral Part of the Anterior Limb of the Internal Capsule
3.5. Lateral Habenula
3.6. Thalamic Peduncles
3.7. Bed Nucleus of the Stria Terminalis
3.8. Medial Forebrain Bundle
4. Towards a More Personalized DBS Treatment Approach for Treatment-Resistant Depression
4.1. Clinical and Neurophysiological Subtypes of Depression
4.2. Individual Tractography
4.3. Combining Deep Brain Stimulation with Cognitive-Behavioral Therapy
4.4. Biomarkers
4.5. Insights into Symptomatic Improvement after Deep Brain Stimulation
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Uher, R.; Payne, J.L.; Pavlova, B.; Perlis, R.H. Major depressive disorder in DSM-5: Implications for clinical practice and research of changes from DSM-IV. Depress. Anxiety 2014, 31, 459–471. [Google Scholar] [CrossRef] [PubMed]
- WHO. Depression and Other Common Mental Disorders Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017.
- Rush, A. Acute and Longer-Term Outcomes in Depressed Outpatients Requiring One or Several Treatment Steps: A STAR*D Report. Am. J. Psychiatry 2006, 163, 1905. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Karyotaki, E.; Weitz, E.; Andersson, G.; Hollon, S.D.; van Straten, A. The effects of psychotherapies for major depression in adults on remission, recovery and improvement: A meta-analysis. J. Affect. Disord. 2014, 159, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Gaynes, B.N.; Asher, G.; Gartlehner, G.; Hoffman, V.; Green, J.; Boland, E.; Lux, L.; Weber, R.P.; Randolph, C.; Bann, C.; et al. Definition of Treatment-Resistant Depression in the Medicare Population; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2018.
- Amital, D.; Fostick, L.; Silberman, A.; Beckman, M.; Spivak, B. Serious life events among resistant and non-resistant MDD patients. J. Affect. Disord. 2008, 110, 260–264. [Google Scholar] [CrossRef]
- Ivanova, J.I.; Birnbaum, H.G.; Kidolezi, Y.; Subramanian, G.; Khan, S.A.; Stensland, M.D. Direct and indirect costs of employees with treatment-resistant and non-treatment-resistant major depressive disorder. Curr. Med. Res. Opin. 2010, 26, 2475–2484. [Google Scholar] [CrossRef]
- Johnson, R.L.; Wilson, C.G. A review of vagus nerve stimulation as a therapeutic intervention. J. Inflamm. Res. 2018, 11, 203–213. [Google Scholar] [CrossRef] [Green Version]
- George, M.S.; Taylor, J.J.; Short, E.B. The expanding evidence base for rTMS treatment of depression. Curr. Opin. Psychiatry 2013, 26, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Mayberg, H.S.; Lozano, A.M.; Voon, V.; McNeely, H.E.; Seminowicz, D.; Hamani, C.; Schwalb, J.M.; Kennedy, S.H. Deep brain stimulation for treatment-resistant depression. Neuron 2005, 45, 651–660. [Google Scholar] [CrossRef] [Green Version]
- Alexander, G.E.; DeLong, M.R.; Strick, P.L. Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Annu. Rev. Neurosci. 1986, 9, 357–381. [Google Scholar] [CrossRef]
- Mayberg, H.S. Limbic-cortical dysregulation: A proposed model of depression. J. Neuropsychiatry Clin. Neurosci. 1997, 9, 471–481. [Google Scholar]
- Temel, Y.; Leentjens, A.F.G.; de Bie, R.M.A. Handboek Diepe Hersenstimulatie Bij Neurologische En Psychiatrische Aandoeningen; Bohn Stafleu van Loghum: Houten, The Netherlands, 2016; pp. 137–142. [Google Scholar]
- Gabriels, L.; Cosyns, P.; Nuttin, B.; Demeulemeester, H.; Gybels, J. Deep brain stimulation for treatment-refractory obsessive-compulsive disorder: Psychopathological and neuropsychological outcome in three cases. Acta Psychiatry Scand. 2003, 107, 275–282. [Google Scholar] [CrossRef]
- Greenberg, B.D.; Malone, D.A.; Friehs, G.M.; Rezai, A.R.; Kubu, C.S.; Malloy, P.F.; Salloway, S.P.; Okun, M.S.; Goodman, W.K.; Rasmussen, S.A. Three-year outcomes in deep brain stimulation for highly resistant obsessive-compulsive disorder. Neuropsychopharmacology 2006, 31, 2384–2393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moonen, A.J.H.; Wijers, A.; Dujardin, K.; Leentjens, A.F.G. Neurobiological correlates of emotional processing in Parkinson’s disease: A systematic review of experimental studies. J. Psychosom. Res. 2017, 100, 65–76. [Google Scholar] [CrossRef]
- Mayberg, H.S.; Liotti, M.; Brannan, S.K.; McGinnis, S.; Mahurin, R.K.; Jerabek, P.A.; Silva, J.A.; Tekell, J.L.; Martin, C.C.; Lancaster, J.L.; et al. Reciprocal limbic-cortical function and negative mood: Converging PET findings in depression and normal sadness. Am. J. Psychiatry 1999, 156, 675–682. [Google Scholar] [PubMed]
- Drevets, W.C.; Savitz, J.; Trimble, M. The subgenual anterior cingulate cortex in mood disorders. CNS Spectr. 2008, 13, 663–681. [Google Scholar] [CrossRef]
- Ongur, D.; Ferry, A.T.; Price, J.L. Architectonic subdivision of the human orbital and medial prefrontal cortex. J. Comp. Neurol. 2003, 460, 425–449. [Google Scholar] [CrossRef]
- Sun, C.; Wang, Y.; Cui, R.; Wu, C.; Li, X.; Bao, Y.; Wang, Y. Human Thalamic-Prefrontal Peduncle Connectivity Revealed by Diffusion Spectrum Imaging Fiber Tracking. Front. Neuroanat. 2018, 12, 24. [Google Scholar] [CrossRef] [Green Version]
- Coenen, V.A.; Panksepp, J.; Hurwitz, T.A.; Urbach, H.; Madler, B. Human medial forebrain bundle (MFB) and anterior thalamic radiation (ATR): Imaging of two major subcortical pathways and the dynamic balance of opposite affects in understanding depression. J. Neuropsychiatry Clin. Neurosci. 2012, 24, 223–236. [Google Scholar] [CrossRef]
- Lebow, M.A.; Chen, A. Overshadowed by the amygdala: The bed nucleus of the stria terminalis emerges as key to psychiatric disorders. Mol. Psychiatry 2016, 21, 450–463. [Google Scholar] [CrossRef]
- Lozano, A.M.; Lipsman, N.; Bergman, H.; Brown, P.; Chabardes, S.; Chang, J.W.; Matthews, K.; McIntyre, C.C.; Schlaepfer, T.E.; Schulder, M.; et al. Deep brain stimulation: Current challenges and future directions. Nat. Rev. Neurol. 2019, 15, 148–160. [Google Scholar] [CrossRef]
- Daneshzand, M.; Faezipour, M.; Barkana, B.D. Robust desynchronization of Parkinson’s disease pathological oscillations by frequency modulation of delayed feedback deep brain stimulation. PLoS ONE 2018, 13, e0207761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vicheva, P.; Butler, M.; Shotbolt, P. Deep brain stimulation for obsessive-compulsive disorder: A systematic review of randomised controlled trials. Neurosci. Biobehav. Rev. 2020, 109, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Agnesi, F.; Johnson, M.D.; Vitek, J.L. Deep brain stimulation: How does it work? Handb. Clin. Neurol. 2013, 116, 39–54. [Google Scholar] [PubMed]
- Cheney, P.D.; Griffin, D.M.; Van Acker, G.M., III. Neural hijacking: Action of high-frequency electrical stimulation on cortical circuits. Neuroscientist 2013, 19, 434–441. [Google Scholar] [CrossRef] [Green Version]
- Ashkan, K.; Rogers, P.; Bergman, H.; Ughratdar, I. Insights into the mechanisms of deep brain stimulation. Nat. Rev. Neurol. 2017, 13, 548–554. [Google Scholar] [CrossRef]
- Van den Munckhof, P.; Bosch, D.A.; Mantione, M.H.; Figee, M.; Denys, D.A.; Schuurman, P.R. Active stimulation site of nucleus accumbens deep brain stimulation in obsessive-compulsive disorder is localized in the ventral internal capsule. Acta Neurochir. Suppl. 2013, 117, 53–59. [Google Scholar]
- Drobisz, D.; Damborska, A. Deep brain stimulation targets for treating depression. Behav. Brain Res. 2019, 359, 266–273. [Google Scholar] [CrossRef]
- Hamani, C.; Mayberg, H.; Stone, S.; Laxton, A.; Haber, S.; Lozano, A.M. The subcallosal cingulate gyrus in the context of major depression. Biol. Psychiatry 2011, 69, 301–308. [Google Scholar] [CrossRef]
- Coryell, W.; Nopoulos, P.; Drevets, W.; Wilson, T.; Andreasen, N.C. Subgenual prefrontal cortex volumes in major depressive disorder and schizophrenia: Diagnostic specificity and prognostic implications. Am. J. Psychiatry 2005, 162, 1706–1712. [Google Scholar] [CrossRef]
- Schlaepfer, T.E.; Cohen, M.X.; Frick, C.; Kosel, M.; Brodesser, D.; Axmacher, N.; Joe, A.Y.; Kreft, M.; Lenartz, D.; Sturm, V. Deep brain stimulation to reward circuitry alleviates anhedonia in refractory major depression. Neuropsychopharmacology 2008, 33, 368–377. [Google Scholar] [CrossRef]
- Wacker, J.; Dillon, D.G.; Pizzagalli, D.A. The role of the nucleus accumbens and rostral anterior cingulate cortex in anhedonia: Integration of resting EEG, fMRI, and volumetric techniques. Neuroimage 2009, 46, 327–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makris, N.; Rathi, Y.; Mouradian, P.; Bonmassar, G.; Papadimitriou, G.; Ing, W.I.; Yeterian, E.H.; Kubicki, M.; Eskandar, E.N.; Wald, L.L.; et al. Variability and anatomical specificity of the orbitofrontothalamic fibers of passage in the ventral capsule/ventral striatum (VC/VS): Precision care for patient-specific tractography-guided targeting of deep brain stimulation (DBS) in obsessive compulsive disorder (OCD). Brain Imaging Behav. 2016, 10, 1054–1067. [Google Scholar]
- Quevedo, K.; Ng, R.; Scott, H.; Kodavaganti, S.; Smyda, G.; Diwadkar, V.; Phillips, M. Ventral Striatum Functional Connectivity during Rewards and Losses and Symptomatology in Depressed Patients. Biol. Psychol. 2017, 123, 62–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, J.W.; Xin, S.C.; Ou, Y.M.; Zhang, W.Y.; Liang, Y.L.; Chen, J.; Yang, X.Q.; Chen, X.Y.; Guo, T.W.; Yang, X.J.; et al. Enhanced default mode network connectivity with ventral striatum in subthreshold depression individuals. J. Psychiatry Res. 2016, 76, 111–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, A.; Ajilore, O.; Zhan, L.; Gadelkarim, J.; Korthauer, L.; Yang, S.; Leow, A.; Kumar, A. White matter tract integrity of anterior limb of internal capsule in major depression and type 2 diabetes. Neuropsychopharmacology 2013, 38, 1451–1459. [Google Scholar] [CrossRef] [Green Version]
- Alonso, P.; Cuadras, D.; Gabriels, L.; Denys, D.; Goodman, W.; Greenberg, B.D.; Jimenez-Ponce, F.; Kuhn, J.; Lenartz, D.; Mallet, L.; et al. Deep Brain Stimulation for Obsessive-Compulsive Disorder: A Meta-Analysis of Treatment Outcome and Predictors of Response. PLoS ONE 2015, 10, e0133591. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, M.; Hikosaka, O. Lateral habenula as a source of negative reward signals in dopamine neurons. Nature 2007, 447, 1111–1115. [Google Scholar] [CrossRef] [Green Version]
- Meng, H.; Wang, Y.; Huang, M.; Lin, W.; Wang, S.; Zhang, B. Chronic deep brain stimulation of the lateral habenula nucleus in a rat model of depression. Brain Res. 2011, 1422, 32–38. [Google Scholar] [CrossRef]
- Sartorius, A.; Henn, F.A. Deep brain stimulation of the lateral habenula in treatment resistant major depression. Med. Hypotheses 2007, 69, 1305–1308. [Google Scholar] [CrossRef]
- Ranft, K.; Dobrowolny, H.; Krell, D.; Bielau, H.; Bogerts, B.; Bernstein, H.G. Evidence for structural abnormalities of the human habenular complex in affective disorders but not in schizophrenia. Psychol. Med. 2010, 40, 557–567. [Google Scholar] [CrossRef]
- Sartorius, A.; Kiening, K.L.; Kirsch, P.; von Gall, C.C.; Haberkorn, U.; Unterberg, A.W.; Henn, F.A.; Meyer-Lindenberg, A. Remission of major depression under deep brain stimulation of the lateral habenula in a therapy-refractory patient. Biol. Psychiatry 2010, 67, e9–e11. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.J.; Dallapiazza, R.F.; De Vloo, P.; Elias, G.J.B.; Fomenko, A.; Boutet, A.; Giacobbe, P.; Lozano, A.M. Inferior thalamic peduncle deep brain stimulation for treatment-refractory obsessive-compulsive disorder: A phase 1 pilot trial. Brain Stimul. 2019, 12, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Velasco, F.; Velasco, M.; Jimenez, F.; Velasco, A.L.; Salin-Pascual, R. Neurobiological background for performing surgical intervention in the inferior thalamic peduncle for treatment of major depression disorders. Neurosurgery 2005, 57, 439–448, Discussion 439–448. [Google Scholar] [CrossRef] [PubMed]
- Schlaepfer, T.E.; Bewernick, B.H.; Kayser, S.; Madler, B.; Coenen, V.A. Rapid effects of deep brain stimulation for treatment-resistant major depression. Biol. Psychiatry 2013, 73, 1204–1212. [Google Scholar] [CrossRef]
- Schoene-Bake, J.C.; Parpaley, Y.; Weber, B.; Panksepp, J.; Hurwitz, T.A.; Coenen, V.A. Tractographic analysis of historical lesion surgery for depression. Neuropsychopharmacology 2010, 35, 2553–2563. [Google Scholar] [CrossRef] [Green Version]
- Fenoy, A.J.; Schulz, P.; Selvaraj, S.; Burrows, C.; Spiker, D.; Cao, B.; Zunta-Soares, G.; Gajwani, P.; Quevedo, J.; Soares, J. Deep brain stimulation of the medial forebrain bundle: Distinctive responses in resistant depression. J. Affect. Disord. 2016, 203, 143–151. [Google Scholar] [CrossRef]
- Neumann, W.J.; Huebl, J.; Brucke, C.; Gabriels, L.; Bajbouj, M.; Merkl, A.; Schneider, G.H.; Nuttin, B.; Brown, P.; Kuhn, A.A. Different patterns of local field potentials from limbic DBS targets in patients with major depressive and obsessive compulsive disorder. Mol. Psychiatry 2014, 19, 1186–1192. [Google Scholar] [CrossRef] [Green Version]
- Bagby, R.M.; Ryder, A.G.; Schuller, D.R.; Marshall, M.B. The Hamilton Depression Rating Scale: Has the gold standard become a lead weight? Am. J. Psychiatry 2004, 161, 2163–2177. [Google Scholar] [CrossRef]
- Kennedy, S.H.; Giacobbe, P.; Rizvi, S.J.; Placenza, F.M.; Nishikawa, Y.; Mayberg, H.S.; Lozano, A.M. Deep brain stimulation for treatment-resistant depression: Follow-up after 3 to 6 years. Am. J. Psychiatry 2011, 168, 502–510. [Google Scholar] [CrossRef]
- Bewernick, B.H.; Hurlemann, R.; Matusch, A.; Kayser, S.; Grubert, C.; Hadrysiewicz, B.; Axmacher, N.; Lemke, M.; Cooper-Mahkorn, D.; Cohen, M.X.; et al. Nucleus accumbens deep brain stimulation decreases ratings of depression and anxiety in treatment-resistant depression. Biol. Psychiatry 2010, 67, 110–116. [Google Scholar] [CrossRef]
- Bewernick, B.H.; Kayser, S.; Sturm, V.; Schlaepfer, T.E. Long-term effects of nucleus accumbens deep brain stimulation in treatment-resistant depression: Evidence for sustained efficacy. Neuropsychopharmacology 2012, 37, 1975–1985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malone, D.A., Jr.; Dougherty, D.D.; Rezai, A.R.; Carpenter, L.L.; Friehs, G.M.; Eskandar, E.N.; Rauch, S.L.; Rasmussen, S.A.; Machado, A.G.; Kubu, C.S.; et al. Deep brain stimulation of the ventral capsule/ventral striatum for treatment-resistant depression. Biol. Psychiatry 2009, 65, 267–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lozano, A.M.; Mayberg, H.S.; Giacobbe, P.; Hamani, C.; Craddock, R.C.; Kennedy, S.H. Subcallosal cingulate gyrus deep brain stimulation for treatment-resistant depression. Biol. Psychiatry 2008, 64, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Puigdemont, D.; Perez-Egea, R.; Portella, M.J.; Molet, J.; de Diego-Adelino, J.; Gironell, A.; Radua, J.; Gomez-Anson, B.; Rodriguez, R.; Serra, M.; et al. Deep brain stimulation of the subcallosal cingulate gyrus: Further evidence in treatment-resistant major depression. Int. J. Neuropsychopharmacol. 2012, 15, 121–133. [Google Scholar] [CrossRef] [Green Version]
- Lozano, A.M.; Giacobbe, P.; Hamani, C.; Rizvi, S.J.; Kennedy, S.H.; Kolivakis, T.T.; Debonnel, G.; Sadikot, A.F.; Lam, R.W.; Howard, A.K.; et al. A multicenter pilot study of subcallosal cingulate area deep brain stimulation for treatment-resistant depression. J. Neurosurg. 2012, 116, 315–322. [Google Scholar] [CrossRef]
- Holtzheimer, P.E.; Kelley, M.E.; Gross, R.E.; Filkowski, M.M.; Garlow, S.J.; Barrocas, A.; Wint, D.; Craighead, M.C.; Kozarsky, J.; Chismar, R.; et al. Subcallosal cingulate deep brain stimulation for treatment-resistant unipolar and bipolar depression. Arch. Gen. Psychiatry 2012, 69, 150–158. [Google Scholar] [CrossRef]
- Crowell, A.L.; Riva-Posse, P.; Holtzheimer, P.E.; Garlow, S.J.; Kelley, M.E.; Gross, R.E.; Denison, L.; Quinn, S.; Mayberg, H.S. Long-Term Outcomes of Subcallosal Cingulate Deep Brain Stimulation for Treatment-Resistant Depression. Am. J. Psychiatry 2019, 176, 949–956. [Google Scholar] [CrossRef]
- Merkl, A.; Schneider, G.H.; Schonecker, T.; Aust, S.; Kuhl, K.P.; Kupsch, A.; Kuhn, A.A.; Bajbouj, M. Antidepressant effects after short-term and chronic stimulation of the subgenual cingulate gyrus in treatment-resistant depression. Exp. Neurol. 2013, 249, 160–168. [Google Scholar] [CrossRef]
- Accolla, E.A.; Aust, S.; Merkl, A.; Schneider, G.H.; Kuhn, A.A.; Bajbouj, M.; Draganski, B. Deep brain stimulation of the posterior gyrus rectus region for treatment resistant depression. J. Affect. Disord. 2016, 194, 33–37. [Google Scholar] [CrossRef] [Green Version]
- Berlim, M.T.; McGirr, A.; Van den Eynde, F.; Fleck, M.P.; Giacobbe, P. Effectiveness and acceptability of deep brain stimulation (DBS) of the subgenual cingulate cortex for treatment-resistant depression: A systematic review and exploratory meta-analysis. J. Affect. Disord. 2014, 159, 31–38. [Google Scholar] [CrossRef]
- Merkl, A.; Aust, S.; Schneider, G.H.; Visser-Vandewalle, V.; Horn, A.; Kuhn, A.A.; Kuhn, J.; Bajbouj, M. Deep brain stimulation of the subcallosal cingulate gyrus in patients with treatment-resistant depression: A double-blinded randomized controlled study and long-term follow-up in eight patients. J. Affect. Disord. 2018, 227, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Holtzheimer, P.E.; Husain, M.M.; Lisanby, S.H.; Taylor, S.F.; Whitworth, L.A.; McClintock, S.; Slavin, K.V.; Berman, J.; McKhann, G.M.; Patil, P.G.; et al. Subcallosal cingulate deep brain stimulation for treatment-resistant depression: A multisite, randomised, sham-controlled trial. Lancet Psychiatry 2017, 4, 839–849. [Google Scholar] [CrossRef] [Green Version]
- Morishita, T.; Fayad, S.M.; Higuchi, M.A.; Nestor, K.A.; Foote, K.D. Deep brain stimulation for treatment-resistant depression: Systematic review of clinical outcomes. Neurotherapeutics 2014, 11, 475–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eitan, R.; Fontaine, D.; Benoit, M.; Giordana, C.; Darmon, N.; Israel, Z.; Linesky, E.; Arkadir, D.; Ben-Naim, S.; Iserlles, M.; et al. One year double blind study of high vs low frequency subcallosal cingulate stimulation for depression. J. Psychiatry Res. 2018, 96, 124–134. [Google Scholar] [CrossRef] [Green Version]
- Dougherty, D.D.; Rezai, A.R.; Carpenter, L.L.; Howland, R.H.; Bhati, M.T.; O’Reardon, J.P.; Eskandar, E.N.; Baltuch, G.H.; Machado, A.D.; Kondziolka, D.; et al. A Randomized Sham-Controlled Trial of Deep Brain Stimulation of the Ventral Capsule/Ventral Striatum for Chronic Treatment-Resistant Depression. Biol. Psychiatry 2015, 78, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Peichel, D. A Clinical Evaluation of Different Device Parameters for the Management of Patients with Treatment Resistant Major Depressive Disorder, Single or Recurrent Episode, with Deep Brain Stimulation. Available online: https://clinicaltrials.gov/ct2/show/NCT01331330 (accessed on 24 August 2020).
- Rezai, A. Feasibility, Safety and Efficacy of Deep Brain Stimulation of the Internal Capsule for Severe and Medically Refractory Major Depression. Available online: https://clinicaltrials.gov/ct2/show/NCT00555698 (accessed on 24 August 2020).
- Nuttin, B.J.; Gabriels, L.A.; Cosyns, P.R.; Meyerson, B.A.; Andreewitch, S.; Sunaert, S.G.; Maes, A.F.; Dupont, P.J.; Gybels, J.M.; Gielen, F.; et al. Long-term electrical capsular stimulation in patients with obsessive-compulsive disorder. Neurosurgery 2003, 52, 1263–1272, Discussion 1264–1272. [Google Scholar] [CrossRef]
- Abelson, J.L.; Curtis, G.C.; Sagher, O.; Albucher, R.C.; Harrigan, M.; Taylor, S.F.; Martis, B.; Giordani, B. Deep brain stimulation for refractory obsessive-compulsive disorder. Biol. Psychiatry 2005, 57, 510–516. [Google Scholar] [CrossRef]
- Van Laere, K.; Nuttin, B.; Gabriels, L.; Dupont, P.; Rasmussen, S.; Greenberg, B.D.; Cosyns, P. Metabolic imaging of anterior capsular stimulation in refractory obsessive-compulsive disorder: A key role for the subgenual anterior cingulate and ventral striatum. J. Nucl. Med. 2006, 47, 740–747. [Google Scholar]
- Bergfeld, I.O.; Mantione, M.; Hoogendoorn, M.L.; Ruhe, H.G.; Notten, P.; van Laarhoven, J.; Visser, I.; Figee, M.; de Kwaasteniet, B.P.; Horst, F.; et al. Deep Brain Stimulation of the Ventral Anterior Limb of the Internal Capsule for Treatment-Resistant Depression: A Randomized Clinical Trial. JAMA Psychiatry 2016, 73, 456–464. [Google Scholar] [CrossRef]
- Loonen, A.J.; Ivanova, S.A. Circuits Regulating Pleasure and Happiness-Mechanisms of Depression. Front. Hum. Neurosci. 2016, 10, 571. [Google Scholar] [CrossRef] [Green Version]
- Goodman, W. A Clinical Pilot Study Examining Bilateral Inhibition of the Lateral Habenula as a Target for Deep Brain Stimulation in Intractable Depression. Available online: https://clinicaltrials.gov/ct2/show/NCT01798407 (accessed on 24 August 2020).
- Rolls, E.T. A non-reward attractor theory of depression. Neurosci. Biobehav. Rev. 2016, 68, 47–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raymaekers, S.; Luyten, L.; Bervoets, C.; Gabriels, L.; Nuttin, B. Deep brain stimulation for treatment-resistant major depressive disorder: A comparison of two targets and long-term follow-up. Transl. Psychiatry 2017, 7, e1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, J.L.; Drevets, W.C. Neural circuits underlying the pathophysiology of mood disorders. Trends Cogn. Sci. 2012, 16, 61–71. [Google Scholar] [CrossRef]
- Barcia, J.A.; Avecillas-Chasin, J.M.; Nombela, C.; Arza, R.; Garcia-Albea, J.; Pineda-Pardo, J.A.; Reneses, B.; Strange, B.A. Personalized striatal targets for deep brain stimulation in obsessive-compulsive disorder. Brain Stimul. 2019, 12, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Beijers, L.; Wardenaar, K.J.; van Loo, H.M.; Schoevers, R.A. Data-driven biological subtypes of depression: Systematic review of biological approaches to depression subtyping. Mol. Psychiatry 2019, 24, 888–900. [Google Scholar] [CrossRef]
- Drysdale, A.T.; Grosenick, L.; Downar, J.; Dunlop, K.; Mansouri, F.; Meng, Y.; Fetcho, R.N.; Zebley, B.; Oathes, D.J.; Etkin, A.; et al. Resting-state connectivity biomarkers define neurophysiological subtypes of depression. Nat. Med. 2017, 23, 28–38. [Google Scholar] [CrossRef] [Green Version]
- Riva-Posse, P.; Choi, K.S.; Holtzheimer, P.E.; Crowell, A.L.; Garlow, S.J.; Rajendra, J.K.; McIntyre, C.C.; Gross, R.E.; Mayberg, H.S. A connectomic approach for subcallosal cingulate deep brain stimulation surgery: Prospective targeting in treatment-resistant depression. Mol. Psychiatry 2018, 23, 843–849. [Google Scholar] [CrossRef] [Green Version]
- Clark, D.L.; Johnson, K.A.; Butson, C.R.; Lebel, C.; Gobbi, D.; Ramasubbu, R.; Kiss, Z.H.T. Tract-based analysis of target engagement by subcallosal cingulate deep brain stimulation for treatment resistant depression. Brain Stimul. 2020, 13, 1094–1101. [Google Scholar] [CrossRef] [Green Version]
- Gormezoglu, M.; van der Vlis, T.B.; Schruers, K.; Ackermans, L.; Polosan, M.; Leentjens, A.F.G. Effectiveness, Timing and Procedural Aspects of Cognitive Behavioral Therapy after Deep Brain Stimulation for Therapy-Resistant Obsessive Compulsive Disorder: A Systematic Review. J. Clin. Med. 2020, 9, 2383. [Google Scholar] [CrossRef]
- Hacimusalar, Y.; Esel, E. Suggested Biomarkers for Major Depressive Disorder. Noro Psikiyatr Ars 2018, 55, 280–290. [Google Scholar] [CrossRef]
- MacDonald, K.; Krishnan, A.; Cervenka, E.; Hu, G.; Guadagno, E.; Trakadis, Y. Biomarkers for major depressive and bipolar disorders using metabolomics: A systematic review. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2019, 180, 122–137. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, H.D.; Shelton, R.C.; Duman, R.S. Functional biomarkers of depression: Diagnosis, treatment, and pathophysiology. Neuropsychopharmacology 2011, 36, 2375–2394. [Google Scholar] [CrossRef] [PubMed]
- Kennis, M.; Gerritsen, L.; van Dalen, M.; Williams, A.; Cuijpers, P.; Bockting, C. Prospective biomarkers of major depressive disorder: A systematic review and meta-analysis. Mol. Psychiatry 2020, 25, 321–338. [Google Scholar] [CrossRef] [Green Version]
- Rosin, B.; Nevet, A.; Elias, S.; Rivlin-Etzion, M.; Israel, Z.; Bergman, H. Physiology and pathophysiology of the basal ganglia-thalamo-cortical networks. Parkinsonism Relat. Disord. 2007, 13 (Suppl. S3), S437–S439. [Google Scholar] [CrossRef]
- Redgrave, P.; Rodriguez, M.; Smith, Y.; Rodriguez-Oroz, M.C.; Lehericy, S.; Bergman, H.; Agid, Y.; DeLong, M.R.; Obeso, J.A. Goal-directed and habitual control in the basal ganglia: Implications for Parkinson’s disease. Nat. Rev. Neurosci. 2010, 11, 760–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panksepp, J. The basic emotional circuits of mammalian brains: Do animals have affective lives? Neurosci. Biobehav. Rev. 2011, 35, 1791–1804. [Google Scholar] [CrossRef] [PubMed]
- Abelaira, H.M.; Reus, G.Z.; Quevedo, J. Animal models as tools to study the pathophysiology of depression. Braz. J. Psychiatry 2013, 35 (Suppl. S2), S112–S120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, L.W.; Prickaerts, J.; Huguet, G.; Kadar, E.; Hartung, H.; Sharp, T.; Temel, Y. Electrical stimulation alleviates depressive-like behaviors of rats: Investigation of brain targets and potential mechanisms. Transl. Psychiatry 2015, 5, e535. [Google Scholar] [CrossRef] [Green Version]
- Verhagen, S.J.; Hasmi, L.; Drukker, M.; van Os, J.; Delespaul, P.A. Use of the experience sampling method in the context of clinical trials. Evid. Based Ment. Health 2016, 19, 86–89. [Google Scholar] [CrossRef] [Green Version]
- Kramer, I.; Simons, C.J.; Hartmann, J.A.; Menne-Lothmann, C.; Viechtbauer, W.; Peeters, F.; Schruers, K.; van Bemmel, A.L.; Myin-Germeys, I.; Delespaul, P.; et al. A therapeutic application of the experience sampling method in the treatment of depression: A randomized controlled trial. World Psychiatry 2014, 13, 68–77. [Google Scholar] [CrossRef]
- Davidson, K.W.; Peacock, J.; Kronish, I.M.; Edmondson, D. Personalizing Behavioral Interventions Through Single-Patient (N-of-1) Trials. Soc. Pers. Psychol. Compass 2014, 8, 408–421. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Region (DBS) | Study | Open-Labeled, RCT or Case-Report | N | Follow-Up | Age (Mean) | Length of Current Depressive Episode, Years (Mean) | Response Rate (%) in HDRS or MADRS Scores | Remission Rate (%) | Serious Adverse Events (N) |
|---|---|---|---|---|---|---|---|---|---|
| SCG | Mayberg et al., 2005 | Open-label | 6 | 6 months | 46 | 5.58 | 33.3 (1 month), # 83 (2 months), # 66.6 (6 months), # | 0 (1 month) 33.3 (3 months) 33.3 (6 months) | Suicidal ideation: 2 Syncope: 1 Lead problem: 1 |
| Lozano et al., 2008 | Open-label | 20 | 12 months | 47.4 | 6.9 | 60 (6 months), # 55 (12 months), # | 35 (6 months) 35 (12 months) | Seizure: 1 Lead problem: 3 | |
| Kennedy et al., 2011 | Open-label | 20 | 1, 2 and 3 years, last follow-up (3–6 years) | 47.4 | 6.9 | 62.5 (1 year), # 46.2 (2 years), # 75 (3 years), # 64.3 (last follow-up), # | 18.8 (1 year) 15.4 (2 years) 50 (3 years) | Worsening depression:3 Suicidal ideation:3 | |
| Puigdemont et al., 2012 | Open-label | 8 | 12 months | 47.4 | 6.3 | 87.5 (1 week), # 37.5 (1 month), # 87.5 (6 months), # 62.5 (12 months), # | 50 (1 week) 37.5 (6 months) 50 (12 months) | Suicide attempt: 1 | |
| Lozano et al., 2012 | Open-label | 21 | 12 months | 47.3 | 5.0 | 57 (1 month), # 48 (6 months), # 29 (12 months), # | - | Suicide: 1 Suicide attempt: 1 | |
| Holtzheimer et al., 2012 | Open-label | 17 | 24 months | 42 | 5.34 | 41 (6 months), # 36 (12 months), # 92 (24 months), # | 18 (6 months) 36 (12 months) 58 (24 months) | Suicidal ideation: 1 Suicide attempt: 2 | |
| Merkl et al., 2013 | Open-label | 6 | 24 h Last follow up (24–36 weeks) | 50.66 | 2.13 | 33.33 (36 weeks), # | 33.33 (36 weeks) | Headaches: 6 Tenseness in neck region: 1 | |
| Holtzheimer et al., 2017 | RCT | 60 (52) | 6 months (24 months) | 50.53 | 12.62 | 22 (6 months), ‡ 54 (12 months), ‡ 48 (24 months), ‡ | 10 (6 months) 17 (12 months) 25 (24 months) | Suicide attempt: 2 Suicidal ideation: 2 Seizure: 2 | |
| Eitan et al., 2018 | RCT HF vs. LF DBS | 9 | 13 months | 46 | - | 44.44 (13 months), ‡ | - | - | |
| Merkl et al., 2018 | RCT | 8 | 28 months (n = 6) 4 years (n = 2) | 48.25 | 2 | 37.5 (6 months), # 43.0 (12 months), # 23.0 (28 months), # | 12.5 (6 months) 14.2 (12 months) 33.0 (24 months) 33.3 (28 months) | Manic episode: 1 | |
| Crowell et al., 2019 | Open-label | 28 | 4 (n = 14) 8 (n = 11) years | 44.9 (45.9) | 45.1 (46.6) | 18 # | 21 | Suicide attempt: 6 Suicidal ideation: 8 Anxiety: 6 Worsening depression: 2 | |
| PGR | Accolla et al., 2016 | Open-label | 5 (1) | 6 months (24 months) | 45.20 | - | - | - | - |
| NAcc | Schlaepfer et al., 2008 | Open-label | 3 | 6–24 weeks | 46.7 | 7.2 | - | - | None |
| Bewernick et al., 2010 | Open-label | 10 | 10 months | 48.6 | 10.8 | 50 (1 month), # 50 (6 months), # 50 (12 months), # | 30 (1 month) | Suicide: 1 Suicide attempt: 1 | |
| Bewernick et al., 2012 | Open-label | 11 | 12 months 24 months Last follow up (max 4 years) | 48.36 | 9.26 | 45 (12 months), # | 9.1 (24 months) | Pain: 4 Seizure: 1 Agitation: 3 Suicide:1 Suicide attempt: 1 | |
| VC/VS | Malone et al., 2009 | Open-label | 15 | 6 months (n = 15) 12 months (n = 11) | 46.3 | 21 | 20 (1 month), # 40 (6 months), # 53.3 (last follow-up) # | 20 (6 months) 40 (last follow-up) | Suicidal ideation: 2 Syncope: 1 Lead problem: 1 |
| Dougherty et al., 2015 | RCT | 30 | 24 months | 47.7 | 11.4 | 20 (16 weeks), ¥ 20 (12 months), ¥ 23.3 (24 months), ¥ | 13 (12 months) 20 (24 months) | Suicide: 1 (stimulation off) Suicide attempt: 4 Suicidal ideation: 5 Lead revision: 3 | |
| vALIC | Van der Wal et al., 2020 (follow-up of the RCT Bergfeld et al. 2016) | Open-label | 25 | 2 years | 52.5 | 7.42 | 32.0 (2 years, ITT) # | 20.0 (2 years, ITT) | Pain: 1 Agitation: 3 Suicidal ideation: 6 Fatigue: 4 |
| Bergfeld et al., 2016 | RCT | 25 | 52 weeks | 53.2 | 6.98 | 40 (after optimization of DBS settings (T2)) # | 20 (T2) | Suicide attempt: 4 Suicidal ideation: 3 Automutilation: 1 | |
| LHb | Sartorius et al., 2009 | Case-report | 1 | 60 weeks | 64.0 | 9.0 | - | - | - |
| MFB | Schlaepfer et al., 2013 | Open-label | 7 | 12–33 weeks | 42.6 | 7.6 | 86, ¥ | 57 | Cranial bleeding: 1 |
| Fenoy et al., 2016 (interim analysis) | Open-label | 4 | 52 weeks | - | - | 75 (7 days) ¥66 (26 weeks, OC) ¥ | - | - |
| Brain Region | Function | Pathological Activity in MDD | HF-DBS Effect |
|---|---|---|---|
| SCG | Contains three white matter bundles; forceps minor + uncinate fasciculus connecting to the medial frontal cortex, cingulum connecting to the rostral and dorsal ACC and fronto-striatal fibers connecting to the NAcc, CN, Pt and anterior Th Connects higher ‘top-down’ cortical regions with subcortical modulatory regions Involvement in brain DMN [30] | Increased activity [31] Reduced volume in familial depression [32] Projections to: (1) NAcc may play a role in lack of interest, disruption in reward and underlie anhedonia (2) Hth and brainstem may play a role in circadian and sleep disturbances, problems with appetite and an abnormal stress responds and cortisol metabolism [31]. | Disruption of pathological activity Modulation of multiple regions connected to the SCG [31] |
| NAcc | Receives projections from VTA, AG, OFC, mPFC, dCN, GP and Hip and projects to Cg25, mPFC, VP, Th, AG and Hth. Transmits information from emotion centers to motor control regions, causing motivational behavior to obtain rewards [33] Processes reward and pleasure information | In severe anhedonia; smaller size and less activation to reward [34] | Acute: Increase in exploratory motivation Chronic: reduction in anhedonia PET Imaging: ↑ activity in VS, bilateral dlPFC and dmPFC, cingulate cortex and bilateral AG. ↓ activity in vmPFC and vlPFC, dCN and Th [33] |
| VC/VS | Contains fibers connecting the dPFC, dACC, OFC and vmPFC with THAL, AG, Hth and brainstem (SN, VTA, RN and PTN) [35] | Increased activity [36] Activation of the connection from left vs. to left caudate has been associated with anhedonia Increased connectivity of vs. to DMN is positively correlated to higher depression scores in the CES-D score [37] | - |
| vALIC | Contains two fiber bundles: the anterior thalamic radiation and the supero-lateral branch of the MFB connecting the PFC to different subcortical structures such as the Th, NAcc, VTA and VS. Decreased integrity of the right vALIC in depressed patients [38] | - | Decreased metabolism in OFC, subgenual ACC and right DLPFC in patients with OCD [39] |
| LHb | Activity corresponds negatively to anticipation and reception of a reward [40] | Increased activity [41] Possible down regulation of serotonergic, noradrenergic and dopaminergic systems [42], volume reduction [43] | Localized metabolic increase in one patient with FDG-PET, presumably due to functional inhibition [44] |
| ITP | Interconnects the intralaminar nucleus and TRN with the OFC [30,45] | Hyperactivation in both TRN and OFC [46] | Cortical desynchronization Disruption of adrenergic and serotonergic malfunction [46] |
| MFB | Interconnects the Nacc, VTA, vmHth, lHth and AG ventromedial and lateral nuclei of the Hth and AG with convergence onto the PFC [47,48] Plays a crucial role in the reward pathway; | Dysfunctional reward system. Responders showed a strong connectivity between the active electrode contact and the mPFC pre-operatively using individual DTI [49] | Insignificant changes in metabolism in 3 patients with PET measurements pre-operatively, 6 and 12 months post-operatively [49] |
| BNST | Mayor output pathway of the AG Regulates stress response Integrates information from multiple brain areas to perform ‘valence surveillance’ [22,30] | Oscillatory activity with high a-power [50] | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roet, M.; Boonstra, J.; Sahin, E.; Mulders, A.E.P.; Leentjens, A.F.G.; Jahanshahi, A. Deep Brain Stimulation for Treatment-Resistant Depression: Towards a More Personalized Treatment Approach. J. Clin. Med. 2020, 9, 2729. https://doi.org/10.3390/jcm9092729
Roet M, Boonstra J, Sahin E, Mulders AEP, Leentjens AFG, Jahanshahi A. Deep Brain Stimulation for Treatment-Resistant Depression: Towards a More Personalized Treatment Approach. Journal of Clinical Medicine. 2020; 9(9):2729. https://doi.org/10.3390/jcm9092729
Chicago/Turabian StyleRoet, Milaine, Jackson Boonstra, Erdi Sahin, Anne E.P. Mulders, Albert F.G. Leentjens, and Ali Jahanshahi. 2020. "Deep Brain Stimulation for Treatment-Resistant Depression: Towards a More Personalized Treatment Approach" Journal of Clinical Medicine 9, no. 9: 2729. https://doi.org/10.3390/jcm9092729
APA StyleRoet, M., Boonstra, J., Sahin, E., Mulders, A. E. P., Leentjens, A. F. G., & Jahanshahi, A. (2020). Deep Brain Stimulation for Treatment-Resistant Depression: Towards a More Personalized Treatment Approach. Journal of Clinical Medicine, 9(9), 2729. https://doi.org/10.3390/jcm9092729