Evaluation of Myocardial Gene Expression Profiling for Superior Diagnosis of Idiopathic Giant-Cell Myocarditis and Clinical Feasibility in a Large Cohort of Patients with Acute Cardiac Decompensation

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Analysis of Myocardial Morphology and Inflammation
2.3. Nucleic Acid Isolation, Reverse Transcription (RT) and nPCR for cDNA
2.4. Preamplification and Gene-Expression Analysis
2.5. Statistics
3. Results
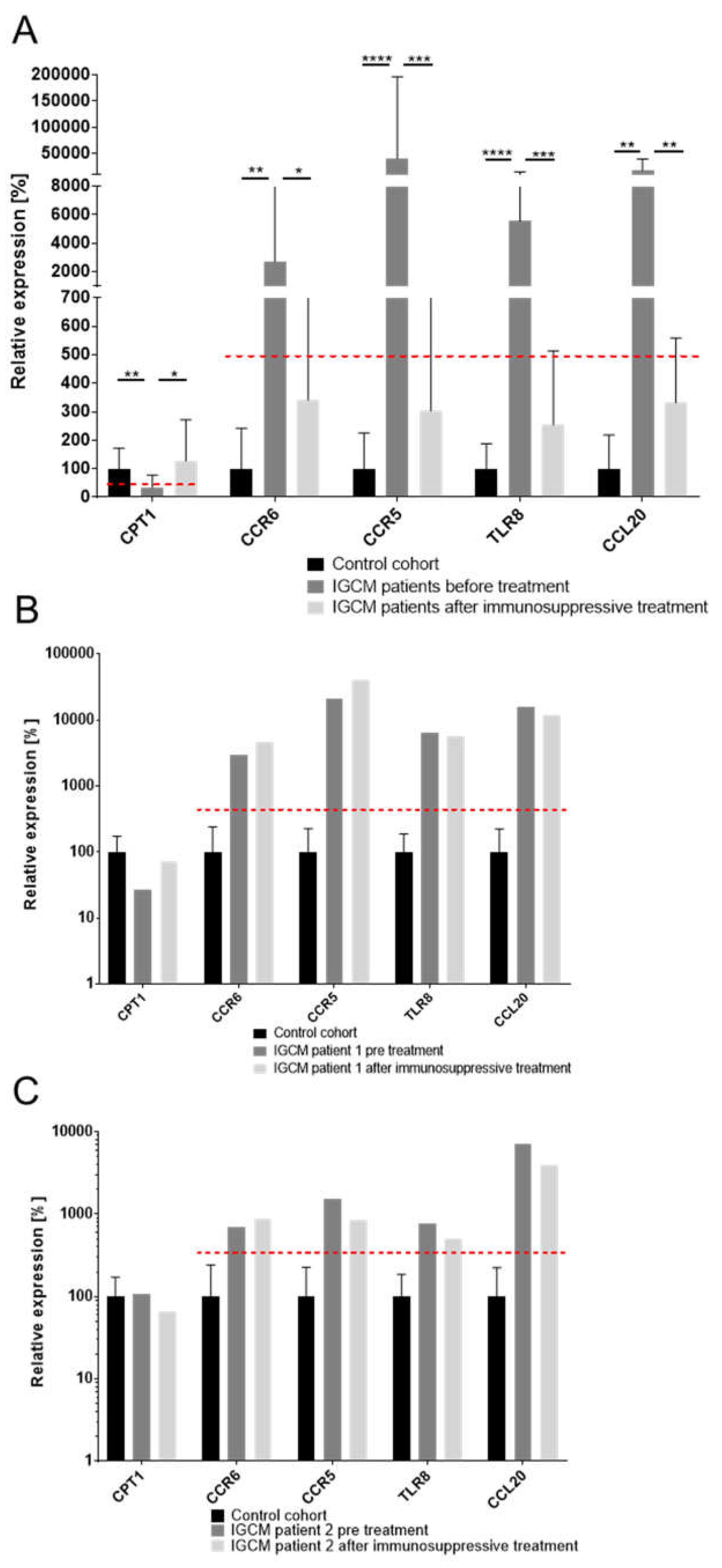
3.1. Distinctive Myocardial Gene-Expression Profiles Which Serve to Identify IGCM
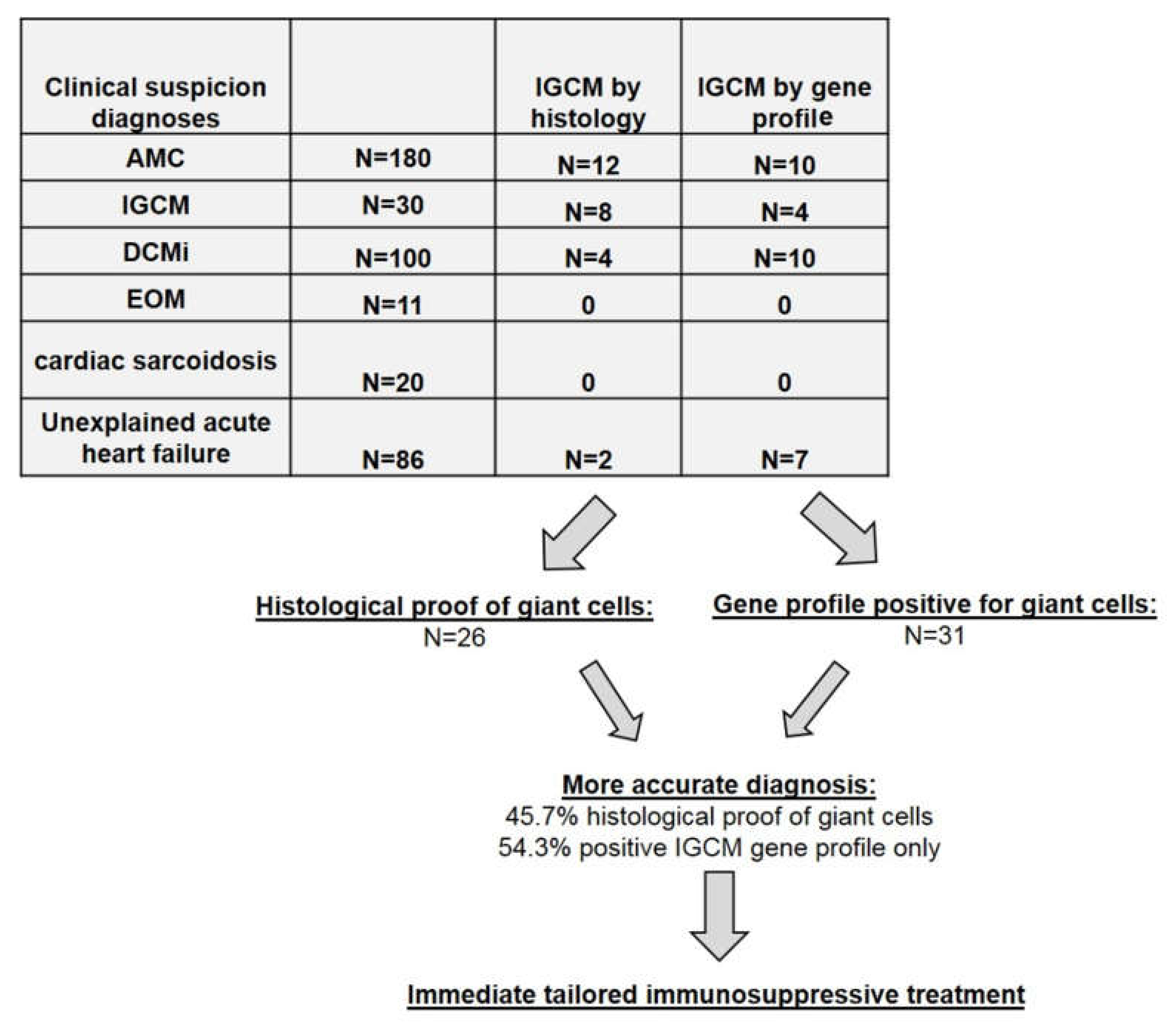
3.2. Application of IGCM-Specific Gene Profiling across the Entire Cohort of Patients with Acute Cardiac Decompensation
3.3. Immunohistologic Analysis of Intramyocardial Infiltration in GCM Patients
3.4. Correlation of Immunohistochemical Markers with Deregulated Genes
3.5. EMB-Based Diagnosis Out of The Entire Study Group
3.6. Clinical and Hemodynamic Outcome of IGCM Patients at Follow-Up after Immunosuppressive Treatment
4. Discussion
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CCL20 | chemokine (C-C motif) ligand 20 |
| CCR5 | chemokine receptor 5 |
| CCR6 | chemokine receptor 6 |
| CPT1 | carnitine palmitoyltransferase I |
| DCM | dilated cardiomyopathy |
| DCMi | inflammatory DCM |
| EMB | endomyocardial biopsy |
| EOM | eosinophilic myocarditis |
| EvG | elastic van Gieson stain |
| GCs | giant cells |
| IGCM | idiopathic giant cell myocarditis |
| IVSD | intraventricular septum diameter |
| LVEDD | left ventricular end-diastolic diameter |
| LVEF | left ventricular ejection fraction |
| LVPW | left ventricular posterior wall |
| NYHA | New York Heart Association Classification |
| RT-qPCR | reverse transcription-quantitative polymerase chain reaction |
| TAPSE | tricuspid annular plane systolic excursion |
| TLR8 | toll-like receptor 8 |
References
- Ammirati, E.; Camici, P.G. Still poor prognosis for patients with giant cell myocarditis in the era of temporary mechanical circulatory supports. Int. J. Cardiol. 2018, 253, 122–123. [Google Scholar] [CrossRef] [PubMed]
- Blauwet, L.A.; Cooper, L.T. Idiopathic giant cell myocarditis and cardiac sarcoidosis. Heart Fail. Rev. 2013, 18, 733–746. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.T., Jr.; Berry, G.J.; Shabetai, R. Idiopathic giant-cell myocarditis--natural history and treatment. Multicenter Giant Cell Myocarditis Study Group Investigators. N. Engl. J. Med. 1997, 336, 1860–1866. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.T., Jr.; Shabetai, R. Giant Cell Myocarditis Study Group. Am. Heart J. 1995, 130, 1312. [Google Scholar] [CrossRef]
- Cooper, L.T., Jr.; ElAmm, C. Giant cell myocarditis. Diagnosis and treatment. Herz 2012, 37, 632–636. [Google Scholar] [CrossRef]
- Schultheiss, H.P.; Kuhl, U.; Cooper, L.T. The management of myocarditis. Eur. Heart J. 2011, 32, 2616–2625. [Google Scholar] [CrossRef] [Green Version]
- Cooper, L.T., Jr.; Berry, G.J.; Rizeq, M.; Schroeder, J.S. Giant cell myocarditis. J. Heart Lung Transplant. 1995, 14, 394–401. [Google Scholar] [CrossRef]
- Frustaci, A.; Chimenti, C.; Pieroni, M.; Salvatori, L.; Morgante, E.; Sale, P.; Ferretti, E.; Petrangeli, E.; Gulino, A.; Russo, M.A. Cell death, proliferation and repair in human myocarditis responding to immunosuppressive therapy. Mod. Pathol. 2006, 19, 755–765. [Google Scholar] [CrossRef] [Green Version]
- Kandolin, R.; Lehtonen, J.; Salmenkivi, K.; Raisanen-Sokolowski, A.; Lommi, J.; Kupari, M. Diagnosis, treatment, and outcome of giant-cell myocarditis in the era of combined immunosuppression. Circ. Heart Fail. 2013, 6, 15–22. [Google Scholar] [CrossRef] [Green Version]
- Kittleson, M.M.; Minhas, K.M.; Irizarry, R.A.; Shui, Q.Y.; Edness, G.; Breton, E.; Conte, J.V.; Tomaselli, G.; Garcia, J.G.; Hare, J.M. Gene expression in giant cell myocarditis: Altered expression of immune response genes. Int. J. Cardiol. 2005, 102, 333–340. [Google Scholar] [CrossRef]
- Lassner, D.; Kühl, U.; Siegismund, C.S.; Rohde, M.; Elezkurtaj, S.; Escher, F.; Tschöpe, C.; Gross, U.M.; Poller, W.; Schultheiss, H.P. Improved diagnosis of idiopathic giant cell myocarditis and cardiac sarcoidosis by myocardial gene expression profiling. Eur. Heart J. 2014, 35, 2186–2195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faust, J.J.; Christenson, W.; Doudrick, K.; Ros, R.; Ugarova, T.P. Development of fusogenic glass surfaces that impart spatiotemporal control over macrophage fusion: Direct visualization of multinucleated giant cell formation. Biomaterials 2017, 128, 160–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyriakides, T.R.; Foster, M.J.; Keeney, G.E.; Tsai, A.; Giachelli, C.M.; Clark-Lewis, I.; Rollins, B.J.; Bornstein, P. The CC chemokine ligand, CCL2/MCP1, participates in macrophage fusion and foreign body giant cell formation. Am. J. Pathol. 2004, 165, 2157–2166. [Google Scholar] [CrossRef] [Green Version]
- McNally, A.K.; DeFife, K.M.; Anderson, J.M. Interleukin-4-induced macrophage fusion is prevented by inhibitors of mannose receptor activity. Am. J. Pathol. 1996, 149, 975–985. [Google Scholar]
- Loupy, A.; Duong Van Huyen, J.P.; Hidalgo, L.; Reeve, J.; Racapé, M.; Aubert, O.; Venner, J.M.; Falmuski, K.; Bories, M.C.; Beuscart, T.; et al. Gene Expression Profiling for the Identification and Classification of Antibody-Mediated Heart Rejection. Circulation 2017, 135, 917–935. [Google Scholar] [CrossRef] [Green Version]
- Pham, M.X.; Teuteberg, J.J.; Kfoury, A.G.; Starling, R.C.; Deng, M.C.; Cappola, T.P.; Kao, A.; Anderson, A.S.; Cotts, W.G.; Ewald, G.A.; et al. Gene-expression profiling for rejection surveillance after cardiac transplantation. N. Engl. J. Med. 2010, 362, 1890–1900. [Google Scholar] [CrossRef] [Green Version]
- Bodez, D.; Hocini, H.; Tchitchek, N.; Tisserand, P.; Benhaiem, N.; Barau, C.; Kharoubi, M.; Guellich, A.; Guendouz, S.; Radu, C.; et al. Myocardial Gene Expression Profiling to Predict and Identify Cardiac Allograft Acute Cellular Rejection: The GET-Study. PLoS ONE 2016, 11, e0167213. [Google Scholar] [CrossRef]
- Aretz, H.T. Myocarditis: The Dallas criteria. Hum. Pathol. 1987, 18, 619–624. [Google Scholar] [CrossRef]
- Escher, F.; Kühl, U.; Lassner, D.; Stroux, A.; Gross, U.; Westermann, D.; Pieske, B.; Poller, W.; Schultheiss, H.P. High Perforin-Positive Cardiac Cell Infiltration and Male Sex Predict Adverse Long-Term Mortality in Patients with Inflammatory Cardiomyopathy. J. Am. Heart. Assoc. 2017, 6, e005352. [Google Scholar] [CrossRef]
- Caforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef]
- Kuhl, U.; Rohde, M.; Lassner, D.; Gross, U.M.; Escher, F.; Schultheiss, H.P. miRNA as activity markers in Parvo B19 associated heart disease. Herz 2012, 37, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Krzysiek, R.; Lefevre, E.A.; Bernard, J.; Foussat, A.; Galanaud, P.; Louache, F.; Richard, Y. Regulation of CCR6 chemokine receptor expression and responsiveness to macrophage inflammatory protein-3alpha/CCL20 in human B cells. Blood 2000, 96, 2338–2345. [Google Scholar] [CrossRef] [PubMed]
- Krasniqi, N.; Eriksson, U. Gene expression profiling: Time to file diagnostic uncertainty in inflammatory heart diseases? Eur. Heart J. 2014, 35, 2138–2139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elezkurtaj, S.; Lassner, D.; Schultheiss, H.P.; Escher, F. Vascular involvement in cardiac giant cell myocarditis: A new pathophysiological aspect. Clin. Res. Cardiol. 2014, 103, 161–163. [Google Scholar] [CrossRef] [PubMed]
- Kasouridis, I.; Majo, J.; MacGowan, G.; Clark, A.L. Giant cell myocarditis presenting with acute heart failure. BMJ Case Rep. 2017, 2017. [Google Scholar] [CrossRef]
- Terasaki, F.; Ukimura, A.; Tsukada, B.; Fujita, S.; Katashima, T.; Otsuka, K.; Otsuka, K.; Kanzaki, Y.; Shimomura, H.; Fujita, M.; et al. Enhanced expression of type 1 helper T-cell cytokines in the myocardium of active cardiac sarcoidosis. Circ. J. 2008, 72, 1303–1307. [Google Scholar] [CrossRef] [Green Version]
- Facco, M.; Baesso, I.; Miorin, M.; Bortoli, M.; Cabrelle, A.; Boscaro, E.; Gurrieri, C.; Trentin, L.; Zambello, R.; Calabrese, F.; et al. Expression and role of CCR6/CCL20 chemokine axis in pulmonary sarcoidosis. J. Leukoc. Biol. 2007, 82, 946–955. [Google Scholar] [CrossRef] [Green Version]
- Fluschnik, N.; Escher, F.; Blankenberg, S.; Westermann, D. Fatal recurrence of fulminant giant cell myocarditis and recovery after initialisation of an alternative immunosuppressive regime. BMJ Case Rep. 2014, 2014. [Google Scholar] [CrossRef] [Green Version]
- Frustaci, A.; Chimenti, C.; Pieroni, M.; Gentiloni, N. Giant cell myocarditis responding to immunosuppressive therapy. Chest 2000, 117, 905–907. [Google Scholar] [CrossRef] [Green Version]
- Fukuhara, T.; Morino, M.; Sakoda, S.; Bito, K.; Kinoshita, M.; Kawakita, S. Myocarditis with multinucleated giant cells detected in biopsy specimens. Clin. Cardiol. 1988, 11, 341–344. [Google Scholar] [CrossRef]
- Maleszewski, J.J.; Orellana, V.M.; Hodge, D.O.; Kuhl, U.; Schultheiss, H.P.; Cooper, L.T. Long-term risk of recurrence, morbidity and mortality in giant cell myocarditis. Am. J. Cardiol. 2015, 115, 1733–1738. [Google Scholar] [CrossRef] [PubMed]
- Shields, R.C.; Tazelaar, H.D.; Berry, G.J.; Cooper, L.T., Jr. The role of right ventricular endomyocardial biopsy for idiopathic giant cell myocarditis. J. Card. Fail. 2002, 8, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Shih, J.A.; Shih, J.A. Small steps for idiopathic giant cell myocarditis. Curr. Heart Fail. Rep. 2015, 12, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.T., Jr.; Hare, J.M.; Tazelaar, H.D.; Edwards, W.D.; Starling, R.C.; Deng, M.C.; Menon, S.; Mullen, G.M.; Jaski, B.; Bailey, K.R.; et al. Usefulness of immunosuppression for giant cell myocarditis. Am. J. Cardiol. 2008, 102, 1535–1539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escher, F.; Kühl, U.; Lassner, D.; Poller, W.; Westermann, D.; Pieske, B.; Tschöpe, C.; Schultheiss, H.P. Long-term outcome of patients with virus-negative chronic myocarditis or inflammatory cardiomyopathy after immunosuppressive therapy. Clin. Res. Cardiol. 2016, 105, 1011–1020. [Google Scholar] [CrossRef]
- Frustaci, A.; Chimenti, C. Immunosuppressive therapy in myocarditis. Circ. J. 2015, 79, 4–7. [Google Scholar] [CrossRef] [Green Version]
- Menghini, V.V.; Savcenko, V.; Olson, L.J.; Tazelaar, H.D.; Dec, G.W.; Kao, A.; Cooper, L.T., Jr. Combined immunosuppression for the treatment of idiopathic giant cell myocarditis. Mayo Clin. Proc. 1999, 74, 1221–1226. [Google Scholar] [CrossRef]
- Schultheiss, H.P. Immunosuppressive therapy in myocarditis and dilated cardiomyopathy? Internist (Berl) 1992, 33, 650–662. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | 23 |
|---|---|
| Age (years) | 48.5 ± 12.9 |
| LVEF (%) | 51.5 ± 15.4 |
| LVEDD (mm) | 55.5 ± 9.3 |
| TAPSE (mm) | 23 ± 4.1 |
| IVSD (mm) | 11.8 ± 3.1 |
| LVPW (mm) | 11.2 ± 2.8 |
| Patient Data | Entire Cohort |
|---|---|
| n | 427 |
| Age (years) | 47.03 ± 15.69 |
| LVEF (%) | 38.54 ± 17.89 |
| LVEDD (mm) | 54.51 ± 8.75 |
| TAPSE (mm) | 22.40 ± 5.93 |
| IVSD (mm) | 11.31 ± 2.80 |
| LVPW (mm) | 10.84 ± 2.40 |
| NYHA I/II/III/VI (n) | 0/0/250/177 |
| Suspected clinical diagnoses (No., n): | |
| - AMC | 180 |
| - IGCM | 30 |
| - DCMi | 100 |
| - EOM | 11 |
| - cardiac sarcoidosis | 20 |
| - unexplained acute heart failure | 86 |
| Patient Data | IGCM (By Histology) | IGCM (By Gene Profiling) |
|---|---|---|
| Immunohistology | ||
| - CD3+ lymphocytes infiltration/mm2 | 312.4 ± 297.3 | 125.8 ± 196.3 * |
| - LFA-1+ lymphocytes infiltration/mm2 | 462.6 ± 413.8 | 183.4 ± 215.0 * |
| - CD45R0+ T memory cell infiltration/mm2 | 533.3 ± 349.6 | 114.9 ± 502.3 * |
| - perforin+ cell infiltration/mm2 | 16.23 ± 26.00 | 14.14 ± 32.23 |
| - Mac-1+ macrophages infiltration/mm2 | 428.8 ± 344.0 | 181.1 ± 227.1 * |
| Patient Data | IGCM (By Histology) At baseline | IGCM (By Histology) After therapy | IGCM (By Gene Profiling) At baseline | IGCM (By Gene Profiling) After therapy |
|---|---|---|---|---|
| n | 17 | 17 | 23 | 23 |
| LVEF (%) | 19.0 ± 14.22 * | 47.25 ± 12.27 | 31.3 ± 15.0 * | 49.9 ± 12.4 |
| LVEDD (mm) | 56.23 ± 5.23 | 55.62 ± 8.43 | 56.43 ± 7.28 | 55.93 ± 4.29 |
| TAPSE (mm) | 20.48 ± 5.13 | 21.23 ± 5.34 | 21.96 ± 7.53 | 21.81 ± 6.33 |
| IVSD (mm) | 10.98 ± 3.15 | 10.42 ± 4.21 | 11.12 ± 3.15 | 11.02 ± 4.12 |
| LVPW (mm) | 10.14 ± 2.41 | 10.05 ± 2.24 | 10.25 ± 2.16 | 10.58 ± 2.07 |
| NYHA I/II/III/VI | 0/0/6/11 | 0/11/6/0 | 0/0/11/12 | 0/18/5/0 |
| Immunohistologic Analysis | ||||
| CD3+ T lymphocytes infiltration/mm2 | 397.3.4 ± 305.3 ** | 23.57 ± 19.23 | 169.1 ± 111.5 ** | 15.72 ± 17.94 |
| LFA-1+ lymphocytes infiltration/mm2 | 612.6 ± 405.5 ** | 40.91 ± 21.00 | 190.8 ± 119.6 * | 23.77 ± 20.69 |
| CD45R0+ T memory cells/mm2 | 584.5 ± 340.5 * | 63.95 ± 59.47 | 208.1 ± 158.3 | 33.99 ± 25.62 |
| perforin+ cytotoxic cells/mm2 | 21.70 ± 28.42 | 0.97 ± 0.72 | 39.22 ± 48.64 | 2.17 ± 4.73 |
| Mac-1+ macrophages infiltration/mm2 | 569.3 ± 311.5 ** | 59.44 ± 18.92 | 200.5 ± 111.3 ** | 40.10 ± 26.42 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Escher, F.; Pietsch, H.; Aleshcheva, G.; Wenzel, P.; Fruhwald, F.; Stumpf, C.; Westermann, D.; Bauersachs, J.; Enseleit, F.; Ruschitzka, F.; et al. Evaluation of Myocardial Gene Expression Profiling for Superior Diagnosis of Idiopathic Giant-Cell Myocarditis and Clinical Feasibility in a Large Cohort of Patients with Acute Cardiac Decompensation. J. Clin. Med. 2020, 9, 2689. https://doi.org/10.3390/jcm9092689
Escher F, Pietsch H, Aleshcheva G, Wenzel P, Fruhwald F, Stumpf C, Westermann D, Bauersachs J, Enseleit F, Ruschitzka F, et al. Evaluation of Myocardial Gene Expression Profiling for Superior Diagnosis of Idiopathic Giant-Cell Myocarditis and Clinical Feasibility in a Large Cohort of Patients with Acute Cardiac Decompensation. Journal of Clinical Medicine. 2020; 9(9):2689. https://doi.org/10.3390/jcm9092689
Chicago/Turabian StyleEscher, Felicitas, Heiko Pietsch, Ganna Aleshcheva, Philip Wenzel, Friedrich Fruhwald, Christian Stumpf, Dirk Westermann, Johann Bauersachs, Frank Enseleit, Frank Ruschitzka, and et al. 2020. "Evaluation of Myocardial Gene Expression Profiling for Superior Diagnosis of Idiopathic Giant-Cell Myocarditis and Clinical Feasibility in a Large Cohort of Patients with Acute Cardiac Decompensation" Journal of Clinical Medicine 9, no. 9: 2689. https://doi.org/10.3390/jcm9092689
APA StyleEscher, F., Pietsch, H., Aleshcheva, G., Wenzel, P., Fruhwald, F., Stumpf, C., Westermann, D., Bauersachs, J., Enseleit, F., Ruschitzka, F., Nägele, H., Laugwitz, K.-L., Haake, H., Frey, N., Brachmann, J., Huber, K., Braun-Dullaeus, R. C., Bergmann, M. W., Strotmann, J., ... Schultheiss, H.-P. (2020). Evaluation of Myocardial Gene Expression Profiling for Superior Diagnosis of Idiopathic Giant-Cell Myocarditis and Clinical Feasibility in a Large Cohort of Patients with Acute Cardiac Decompensation. Journal of Clinical Medicine, 9(9), 2689. https://doi.org/10.3390/jcm9092689