The Effectiveness of Virtual Reality Rehabilitation in Patients with Knee and Hip Osteoarthritis


Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
- Population—adult patients after total hip replacement OR total knee replacement OR knee osteoarthritis OR hip osteoarthritis;
- Intervention—virtual reality, exergames rehabilitation;
- Comparison—standard rehabilitation;
- Outcome—physical function, balance, gait, range of motion, muscle strength, pain, proprioception;
- Time—last 10 years (January 2010–April 2020);
- (Type of study)—randomized controlled trials.
2.2. Study Selection and Data Extraction
2.3. Quality of Included Studies
3. Results
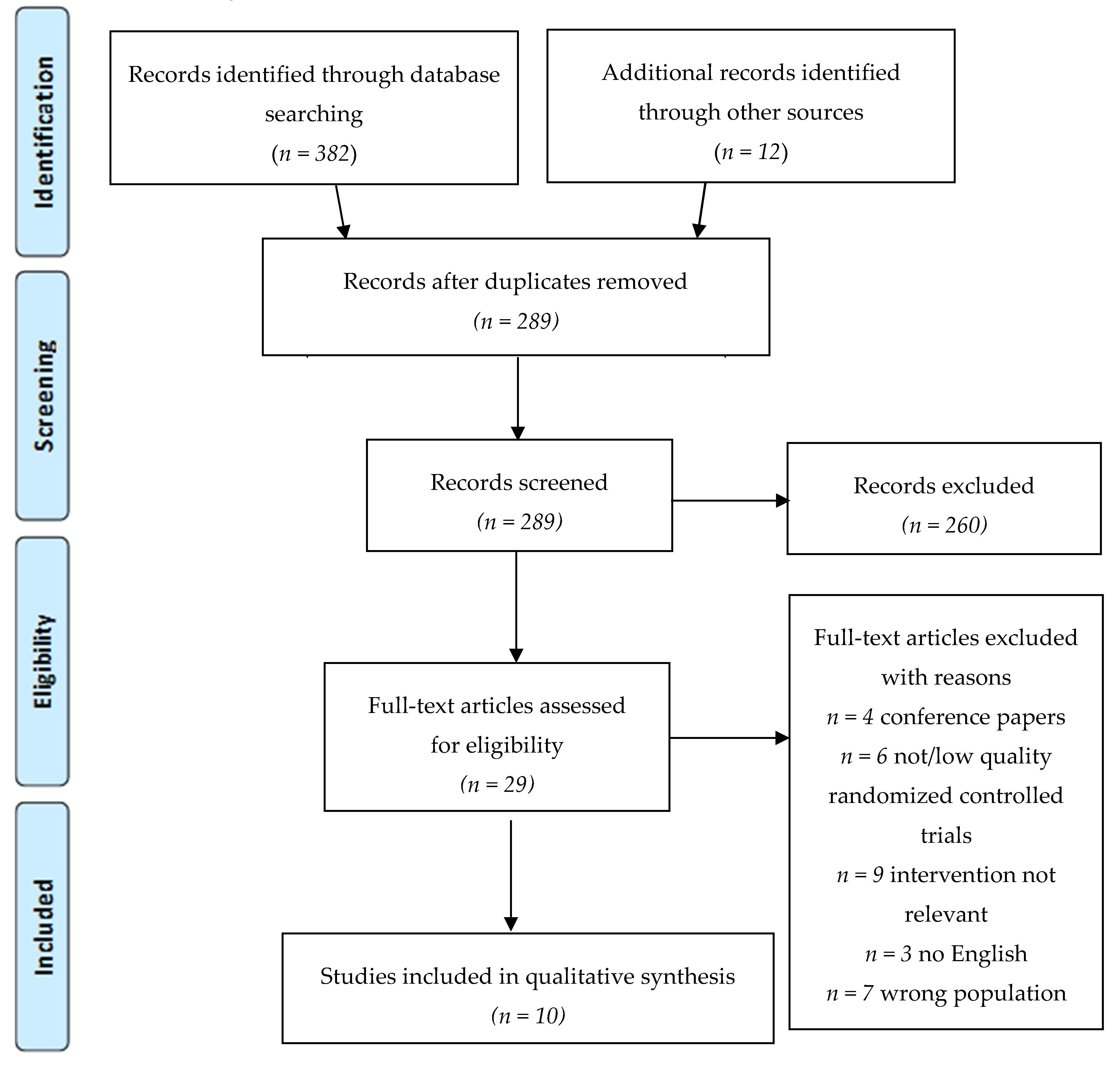
3.1. Searching Results
3.2. Demographic Data
3.3. Methodological Evaluation
3.4. Type of Technology
3.4.1. Exergames
3.4.2. Feedback
3.5. Effects of Intervention—Primary Outcomes
3.5.1. Physical Function
3.5.2. Balance
3.5.3. Gait
3.5.4. Range of Motion
3.5.5. Proprioception
3.5.6. Muscular Strength
3.5.7. Pain
3.6. Effect of Intervention—Secondary Outcomes
3.6.1. Quality of Life
3.6.2. Adherence and Motivation
3.6.3. Inpatient/Outpatient/Home Physical Therapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Attur, M.G.; Dave, M.; Akamatsu, M.; Katoh, M.; Amin, A.R. Osteoarthritis or osteoarthrosis: The definition of inflammation becomes a semantic issue in the genomic era of molecular medicine. Osteoarthr. Cartil. 2002, 10, 1–4. [Google Scholar] [CrossRef]
- Berenbaum, F. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthr. Cartil. 2013, 21, 16–21. [Google Scholar] [CrossRef]
- Vina, E.R.; Kent Kwoh, C. Epidemiology of Osteoarthritis: Literature Update Ernest. Physiol. Behav. 2018, 30, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Sarzi-Puttini, P.; Cimmino, M.A.; Scarpa, R.; Caporali, R.; Parazzini, F.; Zaninelli, A.; Atzeni, F.; Canesi, B. Osteoarthritis: An overview of the disease and its treatment strategies. Semin. Arthritis Rheum. 2005, 35, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Moskowitz, R.W. The burden of osteoarthritis: Clinical and quality-of-life issues. Am. J. Manag. Care 2009, 15, 223–229. [Google Scholar]
- World Health Organization. World Report on Ageing and Health 2015; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Jordan, K.M.; Arden, N.K.; Doherty, M.; Bannwarth, B.; Bijlsma, J.W.J.; Dieppe, P.; Gunther, K.; Hauselmann, H.; Herrero-Beaumont, G.; Kaklamanis, P.; et al. EULAR Recommendations 2003: An evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann. Rheum. Dis. 2003, 62, 1145–1155. [Google Scholar] [CrossRef]
- Zhang, W.; Doherty, M.; Arden, N.; Bannwarth, B.; Bijlsma, J.; Gunther, K.P.; Hauselmann, H.J.; Herrero-Beaumont, G.; Jordan, K.; Kaklamanis, P.; et al. EULAR evidence based recommendations for the management of hip osteoarthritis: Report of a task force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann. Rheum. Dis. 2005, 64, 669–681. [Google Scholar] [CrossRef]
- Hochberg, M.C.; Altman, R.D.; April, K.T.; Benkhalti, M.; Guyatt, G.; McGowan, J.; Towheed, T.; Welch, V.; Wells, G.; Tugwell, P. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2012, 64, 465–474. [Google Scholar] [CrossRef]
- Gademan, M.G.J.; Hofstede, S.N.; Vliet Vlieland, T.P.M.; Nelissen, R.G.H.H.; Marang-Van de Mheen, P.J. Indication criteria for total hip or knee arthroplasty in osteoarthritis: A state-of-the-science overview. BMC Musculoskelet. Disord. 2016, 17, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Coudeyre, E.; Jardin, C.; Givron, P.; Ribinik, P.; Revel, M.; Rannou, F. Could preoperative rehabilitation modify postoperative outcomes after total hip and knee arthroplasty? Elaboration of French clinical practice guidelines. Ann. Readapt. Med. Phys. 2007, 50, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H.; Wilmore, D.W. Multimodal strategies to improve surgical outcome. Am. J. Surg. 2002, 183, 630–641. [Google Scholar] [CrossRef]
- Lenssen, A.F.; De Bie, R.A. Role of physiotherapy in peri-operative management in total knee and hip surgery. Injury 2006, 37, 41–43. [Google Scholar] [CrossRef]
- Pozzi, F.; Snyder-Mackler, L.; Zeni, J. Physical exercise after knee arthroplasty: A systematic review of controlled trials. Eur. J. Phys. Rehabil. Med. 2013, 49, 877–892. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.S.Y.; Teo, W.Z.W.; Teo, W.Z.Y.; Chai, Y.W. Virtual Reality as a Bridge in Palliative Care during COVID-19. J. Palliat. Med. 2020, 23, 756. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Riva, J.J.; Malik, K.M.P.; Burnie, S.J.; Endicott, A.R.; Busse, J.W. What is your research question? An introduction to the PICOT format for clinicians. J. Can. Chiropr. Assoc. 2012, 56, 167–171. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- De Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef]
- Olivo, S.A.; Macedo, L.G.; Gadotti, I.C.; Fuentes, J.; Stanton, T.; Magee, D.J. Scales to Assess the Quality of Randomized Controlled Trials: A Systematic Review. Phys. Ther. 2008, 88, 156–175. [Google Scholar] [CrossRef]
- Ficklscherer, A.; Stapf, J.; Meissner, K.M.; Niethammer, T.; Lahner, M.; Wagenhäuser, M.; Müller, P.E.; Pietschmann, M.F. Testing the feasibility and safety of the Nintendo Wii gaming console in orthopedic rehabilitation: A pilot randomized controlled study. Arch. Med. Sci. 2016, 6, 1273–1278. [Google Scholar] [CrossRef]
- Gianola, S.; Stucovitz, E.; Castellini, G.; Mascali, M.; Vanni, F.; Tramacere, I.; Banfi, G.; Tornese, D. Effects of early virtual reality-based rehabilitation in patients with total knee arthroplasty: A randomized controlled trial. Medicine (U.S.) 2020, 99. [Google Scholar] [CrossRef]
- Lin, Y.-T.; Lee, W.-C.; Hsieh, R.-L. Active video games for knee osteoarthritis improve mobility but not WOMAC score: A randomized controlled trial. Ann. Phys. Rehabil. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Jin, C.; Feng, Y.; Ni, Y.; Shan, Z. Virtual reality intervention in postoperative rehabilitation after total knee arthroplasty: A prospective and randomized controlled clinical trial. Int. J. Clin. Exp. Med. 2018, 11, 6119–6124. [Google Scholar]
- Koo, K.I.; Park, D.K.; Youm, Y.S.; Do Cho, S.; Hwang, C.H. Enhanced Reality Showing Long-Lasting Analgesia after Total Knee Arthroplasty: Prospective, Randomized Clinical Trial. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Elshazly, F.A.A.; Nambi, G.S.; Elnegamy, T.E. Comparative study on Virtual Reality Training (VRT) over Sensory Motor Training (SMT) in Unilateral Chronic Osteoarthritis—A Randomized Control Trial. Int. J. Med. Res. Health Sci. 2016, 5, 7–16. [Google Scholar]
- Christiansen, C.L.; Bade, M.J.; Davidson, B.S.; Dayton, M.R.; Stevens-Lapsley, J.E. Effects of weight-bearing biofeedback training on functional movement patterns following total knee arthroplasty: A randomized controlled trial. J. Orthop. Sports Phys. Ther. 2015, 45, 647–655. [Google Scholar] [CrossRef]
- Ayoade, M.; Baillie, L. A novel knee rehabilitation system for the home. In Proceedings of the 32nd Annual ACM Conference on Human Factors in Computing Systems—CHI’14, Toronto Ontario, Canada, April 2014; ACM Press: New York, NY, USA, 2014; pp. 2521–2530. [Google Scholar]
- Fung, V.; Ho, A.; Shaffer, J.; Chung, E.; Gomez, M. Use of Nintendo Wii FitTM In the rehabilitation of outpatients following total knee replacement: A preliminary randomised controlled trial. Physiotherapy (U.K.) 2012, 98, 183–188. [Google Scholar] [CrossRef]
- Lehrl, S.; Gusinde, J.; Schulz-Drost, S.; Rein, A.; Schlechtweg, P.M.; Jacob, H.; Krinner, S.; Gelse, K.; Pauser, J.; Brem, M.H. Advancement of physical process by mental activation: A prospective controlled study. J. Rehabil. Res. Dev. 2012, 49, 1221. [Google Scholar] [CrossRef]
- Gluud, L.L. Bias in clinical intervention research. Am. J. Epidemiol. 2006, 163, 493–501. [Google Scholar] [CrossRef]
- Villamar, M.F.; Contreras, V.S.; Kuntz, R.E.; Fregni, F. The reporting of blinding in physical medicine and rehabilitation randomized controlled trials: A systematic review. J. Rehabil. Med. 2013, 45, 6–13. [Google Scholar] [CrossRef]
- Kucio, C.; Pilch, J. Metody zaślepiania badań klinicznych w fizjoterapii. Physiotherapy 2013, 62–64. [Google Scholar] [CrossRef]
- Nüesch, E.; Reichenbach, S.; Trelle, S.; Rutjes, A.W.S.; Liewald, K.; Sterchi, R.; Altman, D.G.; Jüni, P. The importance of allocation concealment and patient blinding in osteoarthritis trials: A meta-epidemiologic study. Arthritis Care Res. 2009, 61, 1633–1641. [Google Scholar] [CrossRef] [PubMed]
- Saltaji, H.; Armijo-olivo, S.; Cummings, G.G.; Amin, M.; Costa, B.R.; Flores-mir, C. Influence of blinding on treatment effect size estimate in randomized controlled trials of oral health interventions. BMC Med. Res. Methodol. 2018, 18, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Dettori, J.R.; Norvell, D.C. Intention-to-Treat: Is That Fair ? Glob. Spine J. 2020, 10, 361–363. [Google Scholar] [CrossRef]
- Kovach, C.R. Intention to Treat Necessary But Not Sufficient. Res. Gerontol. Nurs. 2020, 13, 62–63. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Lin, H.-T.; Li, Y.-I.; Hu, W.-P.; Huang, C.-C.; Du, Y.-C. A Scoping Review of The Efficacy of Virtual Reality and Exergaming on Patients of Musculoskeletal System Disorder. J. Clin. Med. 2019, 8, 791. [Google Scholar] [CrossRef]
- Blasco, J.M.; Igual-Camacho, C.; Blasco, M.C.; Anton-Anton, V.; Ortiz-Llueca, A.; Roig-Casasus, S. The efficacy of virtual reality tools for total knee replacement rehabilitation: A systematic review. Physiother. Theory Pract. 2019, 1–11. [Google Scholar] [CrossRef]
- Wang, X.; Hunter, D.J.D.J.; Vesentini, G.; Pozzobon, D.; Ferreira, M.L.M.L. Technology-assisted rehabilitation following total knee or hip replacement for people with osteoarthritis: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2019, 20, 506. [Google Scholar] [CrossRef]
- Li, L.; Yu, F.; Shi, D.; Shi, J.; Tian, Z.; Yang, J.; Wang, X.; Jiang, Q. Application of virtual reality technology in clinical medicine. Am. J. Transl. Res. 2017, 9, 3867–3880. [Google Scholar] [PubMed]
- Wittkopf, P.G.; Lloyd, D.M.; Johnson, M.I. Managing limb pain using virtual reality: A systematic review of clinical and experimental studies. Disabil. Rehabil. 2019, 41, 3103–3117. [Google Scholar] [CrossRef] [PubMed]
- Rutledge, T.; Velez, D.; Depp, C.; McQuaid, J.R.; Wong, G.; Jones, R.C.W.; Atkinson, J.H.; Giap, B.; Quan, A.; Giap, H. A Virtual Reality Intervention for the Treatment of Phantom Limb Pain: Development and Feasibility Results. Pain Med. 2019, 20, 2051–2059. [Google Scholar] [CrossRef] [PubMed]
- Osumi, M.; Inomata, K.; Inoue, Y.; Otake, Y.; Morioka, S.; Sumitani, M. Characteristics of Phantom Limb Pain Alleviated with Virtual Reality Rehabilitation. Pain Med. 2019, 20, 1038–1046. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Carballo, J.; Rodriguez, N.; Soler, D.; Opisso, E.; Sbert, M. Gestural Interaction and Visual Illusion for Lower Limbs’ Neuropathic Pain Treatment. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 2217–2225. [Google Scholar] [CrossRef]
- Hoermann, S.; Ferreira Dos Santos, L.; Morkisch, N.; Jettkowski, K.; Sillis, M.; Devan, H.; Kanagasabai, P.S.; Schmidt, H.; Kruger, J.; Dohle, C.; et al. Computerised mirror therapy with Augmented Reflection Technology for early stroke rehabilitation: Clinical feasibility and integration as an adjunct therapy. Disabil. Rehabil. 2017, 39, 1503–1514. [Google Scholar] [CrossRef]
- Weber, L.M.; Nilsen, D.M.; Gillen, G.; Yoon, J.; Stein, J. Immersive Virtual Reality Mirror Therapy for Upper Limb Recovery After Stroke: A Pilot Study. Am. J. Phys. Med. Rehabil. 2019, 98, 783–788. [Google Scholar] [CrossRef]
- Choi, H.-S.; Shin, W.-S.; Bang, D.-H. Mirror Therapy Using Gesture Recognition for Upper Limb Function, Neck Discomfort, and Quality of Life After Chronic Stroke: A Single-Blind Randomized Controlled Trial. Med. Sci. Monit. 2019, 25, 3271–3278. [Google Scholar] [CrossRef]
- Villafaina, S.; Collado-Mateo, D.; Domínguez-Muñoz, F.J.; Fuentes-García, J.P.; Gusi, N. Benefits of 24-Week Exergame Intervention on Health-Related Quality of Life and Pain in Women with Fibromyalgia: A Single-Blind, Randomized Controlled Trial. Games Health J. 2019, 8, 380–386. [Google Scholar] [CrossRef]
- Cacciata, M.; Stromberg, A.; Lee, J.A.; Sorkin, D.; Lombardo, D.; Clancy, S.; Nyamathi, A.; Evangelista, L.S. Effect of exergaming on health-related quality of life in older adults: A systematic review. Int. J. Nurs. Stud. 2019, 93, 30–40. [Google Scholar] [CrossRef]
- Collado-Mateo, D.; Merellano-Navarro, E.; Olivares, P.R.; García-Rubio, J.; Gusi, N. Effect of exergames on musculoskeletal pain: A systematic review and meta-analysis. Scand. J. Med. Sci. Sports 2018, 28, 760–771. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, I.F.; Leme, G.L.M.; Scheicher, M.E. The Influence of Video Game Training with and without Subpatelar Bandage in Mobility and Gait Speed on Elderly Female Fallers. J. Aging Res. 2018, 2018, 9415093. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.-Y.; Chen, I.-H.; Lin, Y.-J.; Chen, Y.; Hsu, W.-C. Effects of Virtual Reality-Based Physical and Cognitive Training on Executive Function and Dual-Task Gait Performance in Older Adults With Mild Cognitive Impairment: A Randomized Control Trial. Front. Aging Neurosci. 2019, 11, 162. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, R.E.; Hamada, H.A.; Yousef, A.M.; Aziz, K.S.A.; Koura, G.M.; Radwan, R. Impact of electronic balance training on postural instability in postmenopausal women: A randomized controlled trail. Fizjoterapia Pol. 2019, 19, 100–105. [Google Scholar]
- Pua, Y.-H.; Clark, R.A.; Ong, P.-H. Evaluation of the Wii Balance Board for walking aids prediction: Proof-of-concept study in total knee arthroplasty. PLoS ONE 2015, 10, e0117124. [Google Scholar] [CrossRef]
- Blomkvist, A.W.; Andersen, S.; De Bruin, E.; Jorgensen, M.G. Unilateral lower limb strength assessed using the Nintendo Wii Balance Board: A simple and reliable method. Aging Clin. Exp. Res. 2017, 29, 1013–1020. [Google Scholar] [CrossRef]
- Cho, C.; Hwang, W.; Hwang, S.; Chung, Y. Treadmill training with virtual reality improves gait, balance, and muscle strength in children with cerebral palsy. Tohoku J. Exp. Med. 2016, 238, 213–218. [Google Scholar] [CrossRef]
- Kiper, P.; Agostini, M.; Luque-Moreno, C.; Tonin, P.; Turolla, A. Reinforced feedback in virtual environment for rehabilitation of upper extremity dysfunction after stroke: Preliminary data from a randomized controlled trial. Biomed Res. Int. 2014, 2014, 752128. [Google Scholar] [CrossRef]
- Luque-Moreno, C.; Oliva-Pascual-Vaca, A.; Kiper, P.; Rodriguez-Blanco, C.; Agostini, M.; Turolla, A. Virtual Reality to Assess and Treat Lower Extremity Disorders in Post-stroke Patients. Methods Inf. Med. 2016, 55, 89–92. [Google Scholar] [CrossRef]
- Alemanno, F.; Houdayer, E.; Emedoli, D.; Locatelli, M.; Mortini, P.; Mandelli, C.; Raggi, A.; Iannaccone, S. Efficacy of virtual reality to reduce chronic low back pain: Proof-of-concept of a non-pharmacological approach on pain, quality of life, neuropsychological and functional outcome. PLoS ONE 2019, 14, e0216858. [Google Scholar] [CrossRef]
- Pournajaf, S.; Goffredo, M.; Criscuolo, S.; Galli, M.; Damiani, C.; Franceschini, M. Virtual reality rehabilitation in patients with total knee replacement: Preliminary results. Gait Posture 2017, 57, 17–18. [Google Scholar] [CrossRef]
- Sohn, J.; Kim, S. Falls study: Proprioception, postural stability, and slips. Biomed. Mater. Eng. 2015, 26, S693–S703. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, H.; Hakim, M.N.; Hamid, T.A.; Amri, S.B.; Razeghi, M.; Farazdaghi, M.; Shakoor, E. The effect of exergaming on knee proprioception in older men: A randomized controlled trial. Arch. Gerontol. Geriatr. 2017, 69, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Gschwind, Y.J.; Schoene, D.; Lord, S.R.; Ejupi, A.; Valenzuela, T.; Aal, K.; Woodbury, A.; Delbaere, K. The effect of sensor-based exercise at home on functional performance associated with fall risk in older people—A comparison of two exergame interventions. Eur. Rev. Aging Phys. Act. 2015, 12. [Google Scholar] [CrossRef]
- Cho, S.; Ku, J.; Cho, Y.K.; Kim, I.Y.; Kang, Y.J.; Jang, D.P.; Kim, S.I. Development of virtual reality proprioceptive rehabilitation system for stroke patients. Comput. Methods Programs Biomed. 2014, 113, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Santos, G.O.R.; Wolf, R.; Silva, M.M.; Rodacki, A.L.F.; Pereira, G. Does exercise intensity increment in exergame promote changes in strength, functional capacity and perceptual parameters in pre-frail older women? A randomized controlled trial. Exp. Gerontol. 2019, 116, 25–30. [Google Scholar] [CrossRef]
- Villafaina, S.; Borrega-Mouquinho, Y.; Fuentes-García, J.P.; Collado-Mateo, D.; Gusi, N. Effect of Exergame Training and Detraining on Lower-Body Strength, Agility, and Cardiorespiratory Fitness in Women with Fibromyalgia: Single-Blinded Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 17, 161. [Google Scholar] [CrossRef]
- Cheng, S.-T. Cognitive Reserve and the Prevention of Dementia: The Role of Physical and Cognitive Activities. Curr. Psychiatry Rep. 2016, 18, 85. [Google Scholar] [CrossRef]
- Allan, L.M.; Ballard, C.G.; Rowan, E.N.; Kenny, R.A. Incidence and prediction of falls in dementia: A prospective study in older people. PLoS ONE 2009, 4, e5521. [Google Scholar] [CrossRef]
- Terkelsen, A.J.; Andersen, O.K.; Molgaard, H.; Hansen, J.; Jensen, T.S. Mental stress inhibits pain perception and heart rate variability but not a nociceptive withdrawal reflex. Acta Physiol. Scand. 2004, 180, 405–414. [Google Scholar] [CrossRef]
- Norouzi, E.; Vaezmosavi, M.; Gerber, M.; Puhse, U.; Brand, S. Dual-task training on cognition and resistance training improved both balance and working memory in older people. Phys. Sportsmed. 2019, 47, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Molina, K.I.; Ricci, N.A.; De Moraes, S.A.; Perracini, M.R. Virtual reality using games for improving physical functioning in older adults: A systematic review. J. Neuroeng. Rehabil. 2014, 11, 156. [Google Scholar] [CrossRef]
- Gonzalez-Franco, M.; Gilroy, S.; Moore, J.O. Empowering patients to perform physical therapy at home. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 6308–6311. [Google Scholar] [CrossRef]
- Piqueras, M.; Marco, E.; Coll, M.; Escalada, F.; Ballester, A.; Cinca, C.; Belmonte, R.; Muniesa, J.M. Effectiveness of an interactive virtual telerehabilitation system in patients after total knee arthroplasty: A randomized controlled trial. J. Rehabil. Med. 2013, 45, 392–396. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, T.; Jonsdottir, J.; Ferrarin, M.; Marzegan, A.; Bowman, T.; Turolla, A.; Carpinella, I. Effects of planar robotic rehabilitation on muscle synergies of the upper limbs in post-stroke subjects. Gait Posture 2016, 49, S4. [Google Scholar] [CrossRef]


{kind=link}
| No | First Author, Year, Country | PEDro Scale | Main Objective | Participants | Intervention/Technology | Outcomes | Research Tools | Main Results |
|---|---|---|---|---|---|---|---|---|
| 1 | Gianola et al. [23] 2020, Italy | 7/10 | The effectiveness of VR rehabilitation vs. standard rehabilitation for physical function after primary TKA | Adults 45–80 years old 3–4 days after primary unilateral TKA: all n = 74 study n = 35 controls n = 39 | Sixty minute daily training for at least 5 days All participants performed passive ROM exercises on Kinetec knee continuous passive motion system and functional exercises. Study—VR games focused on balance, proprioception and function of lower limbs Controls—standard postoperative physiotherapy | Pain; knee disability quality of life; patients’ assessment of their condition; functional performance; leg muscle strength; knee ROM; proprioception; balance; medication assumption | VAS WOMAC EQ-5D GPE FIM dynamometer goniometer stabilometric platform VRRS | No significant difference in pain reduction and other outcomes, except improved proprioception in the study VR group. |
| 2 | Lin et al. [24] 2020, Taiwan | 8/10 | A comparison of VR games exercises and standard physical exercises in patients with knee OA | Patients aged 40–85 with knee OA (Kellgren and Lawrence Score ≥ 2): all n = 80 study n = 40 controls n = 40 | Three times a week for 4 weeks with a follow-up All received 20 min of hot packs and 20 min of TENS Study—active video games using the Hot Plus system focused on muscle strength, coordination and ROM of limbs Controls—standard exercises | knee disability; quality of life; psychosocial distress; fatigue; pain; work ability; balance | WOMAC WHOQOL-BREF HADS MFI CPG WAI Biodex Stability System | No significant difference between VR training and standard exercises in improving knee disability, but games improved dynamic balance, physical functional performance, and physical health more than therapeutic exercises. |
| 3 | Jin et al. [25] 2018, China | 5/10 | The effects and benefits of VR training in postoperative patients after TKA | Patients after primary unilateral TKA: all n = 66 study n = 33 controls n = 33 | Standard therapeutic exercises + 30 min three times a day: Study—VR training (Mide Technology) from the second day of therapy, focus on knee flexion (rowing boat) Controls—3 sets of active knee flexion exercises | knee disability; evaluation of early results of TKA; pain; ROM | WOMAC HSS VAS goniometer | VR training effects better at improving knee functional recovery, ROM and relieving pain after TKA than standard exercises. |
| 4 | Koo et al. [26] 2018, South Korea | 6/10 | The effectiveness of enhanced reality on analgesia and physical function after TKA | Patients with unilateral TKA: all n = 42 study n = 22 controls n = 20 | Enhanced reality analgesia visual biofeedback (combination of the VR, real-time motion capture, mirror therapy using real-time image processing technique) Study—intervention was provided shortly after physiotherapy for five times a week for 2 weeks Controls—intervention was provided for five times a week for 1 week | Pain; ROM; knee disability; endurance and aerobic capacity; lower extremities; strength; medication assumption; | VAS goniometer WOMAC 6MWT TST | Analgesia and improvement in ROM in both groups were achieved, but in the study group that lasted longer than in controls. |
| 5 | Ficklscherer et al. [22] 2016, Germany | 4/10 | The assessment of the Nintendo Wii as an appropriate and safe tool in rehabilitation after orthopedic knee surgery | Patients with TKA or anterior cruciate ligament (ACL) tear: all n = 30 study n = 17 controls = 13 | Four weeks of intervention Study—exergames on The Nintendo Wii and standard physical therapy Controls—standard physical therapy | Knee function and disability | IKDC MCKRS TLKS | No significant difference between VR training and standard exercises in improving knee disability, but slightly greater improvement in the Wii group. Intervention without a negative influence on patients. |
| 6 | Elshazly et al. [27] 2016, Saudi Arabia | 7/10 | A comparison of the effectiveness of VR training over sensory motor training in the treatment of osteoarthritis | Patients with chronic OA (> 3 mths) WOMAC: 71 points: all n = 60 virtual reality training n = 20 Qsensory motor training n = 20 controls n = 20 | Three times per week for 8 weeks Study—virtual reality training Light Race VR interactive game 15-30′ ControlsI—sensory motor progressive training II—conventional exercise training warm-up, walking, cool-down | Pain intensity; joint proprioception; knee disability; quality of life | VAS perception sense WOMAC HRQOL | Significant improvement in the outcome measures in all the training methods. VR training showed a substantial improvement over the other methods. |
| 7 | Christiansen et al. [28] 2015, USA | 7/10 | The effectiveness of weight-bearing (WB) biofeedback training on WB symmetry and functional joint moments following unilateral total knee arthroplasty | Patients with unilateral TKA: all n = 26 study n = 13 controls n = 13 | Study—weight-bearing biofeedback on the Nintendo Wii Fit Plus and Wii Balance Board and physical therapy daily for 6 weeks Controls—physical therapy twice per day for 6 weeks | Gait/walking speed; lower limb; weight-bearing ratios (WBRs); lower limb joint movement | 12 m walkway—gait speed FTSST | No significant difference between VR training and controls in WBR. FTSST time improved in the study group compared to the control group. The tendency for improved walking speed in the study group at 26 weeks (P = 0.068). |
| 8 | Ayoade et al. [29] 2014, Canada | 4/10 | The presentation of rehabilitation visualization system (RVS); the assessment of usability and feasibility of the RVS at home | Patients with TKA in the early phase of post-operative rehabilitation: all n = 21 study n = 11 controls n = 10 | Ten days of training in the hospital and then at home for up to 6 weeks Study—rehabilitation visualization system and exercise handbook Controls—exercise handbook only | Knee ROM; functional performance; health surveys; rehabilitation experience; usability | Goniometer OKS SF-12 survey IMI SUS | Overall, no significant difference between RVS training and controls. However, RVS made home rehabilitation more engaging and improved the communication between patients and the therapist. |
| 9 | Fung et al. [30] 2012, Canada | 5/10 | The examination of the Nintendo Wii Fit as an acceptable adjunct to physiotherapy concerning balance, ROM, muscle strength and function in outpatients following TKA | Outpatients after TKA: all n = 50 study n = 27 controls n = 23 | Twice a week for 75 min Study—15 min of exergames focused on postural control and balance in The Nintendo Wii Fit and 60 min of physical therapy Controls—60 min of physical therapy and 15 min of lower extremity strengthening and balance training | Balance; knee ROM; postural control; lower leg function; pain | 2MWT Goniometer ABCS LFES NPRS satisfaction survey | No significant difference between study and controls. Wii Fit is potentially acceptable as an adjunct to physical therapy intervention in view of balance, postural control and use of the lower extremities. |
| 10 | Lehrl et al. [31] 2012, Germany | 5/10 | The enhancing of rehabilitation using mental activation | Patients after THA: all n = 32 study n = 16 controls n = 16 | Study—30 min per day for 12 days of video game Dr. Kawashima’s Brain Training: How Old Is Your Brain? Controls—without intervention | Hip function and disability | HHS PMA | Significant improvement in hip function obtained in the study group in HHS, but not in PMA. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byra, J.; Czernicki, K. The Effectiveness of Virtual Reality Rehabilitation in Patients with Knee and Hip Osteoarthritis. J. Clin. Med. 2020, 9, 2639. https://doi.org/10.3390/jcm9082639
Byra J, Czernicki K. The Effectiveness of Virtual Reality Rehabilitation in Patients with Knee and Hip Osteoarthritis. Journal of Clinical Medicine. 2020; 9(8):2639. https://doi.org/10.3390/jcm9082639
Chicago/Turabian StyleByra, Joanna, and Krzysztof Czernicki. 2020. "The Effectiveness of Virtual Reality Rehabilitation in Patients with Knee and Hip Osteoarthritis" Journal of Clinical Medicine 9, no. 8: 2639. https://doi.org/10.3390/jcm9082639
APA StyleByra, J., & Czernicki, K. (2020). The Effectiveness of Virtual Reality Rehabilitation in Patients with Knee and Hip Osteoarthritis. Journal of Clinical Medicine, 9(8), 2639. https://doi.org/10.3390/jcm9082639