Low PCSK-9 levels Are Associated with Favorable Neurologic Function after Resuscitation from out of Hospital Cardiac Arrest

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Definition of Multi-Organ Failure (MOF):
2.2. Endpoints
2.3. Statistics
3. Results
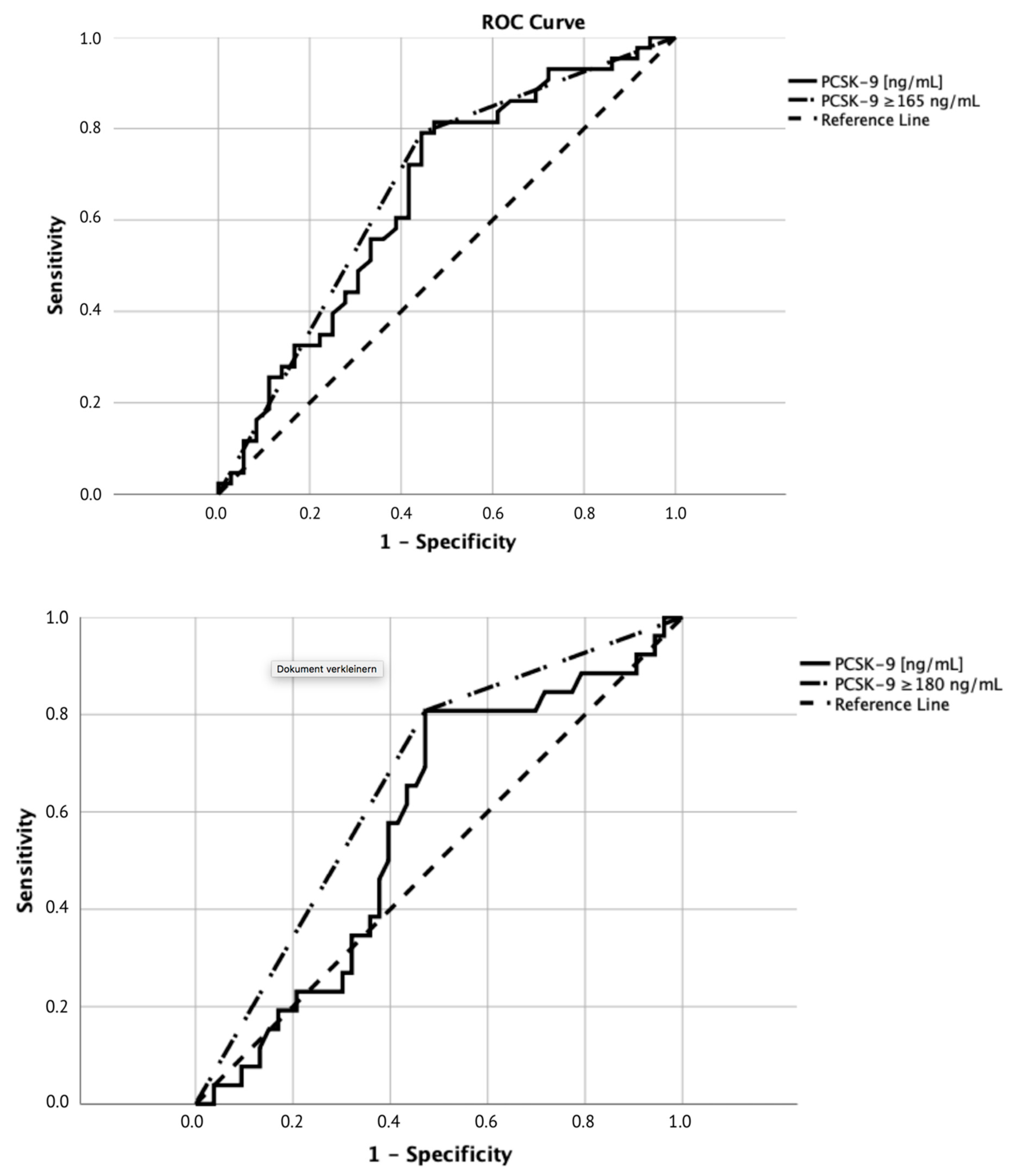
3.1. Receiver Operating Characteristic Curve Analysis
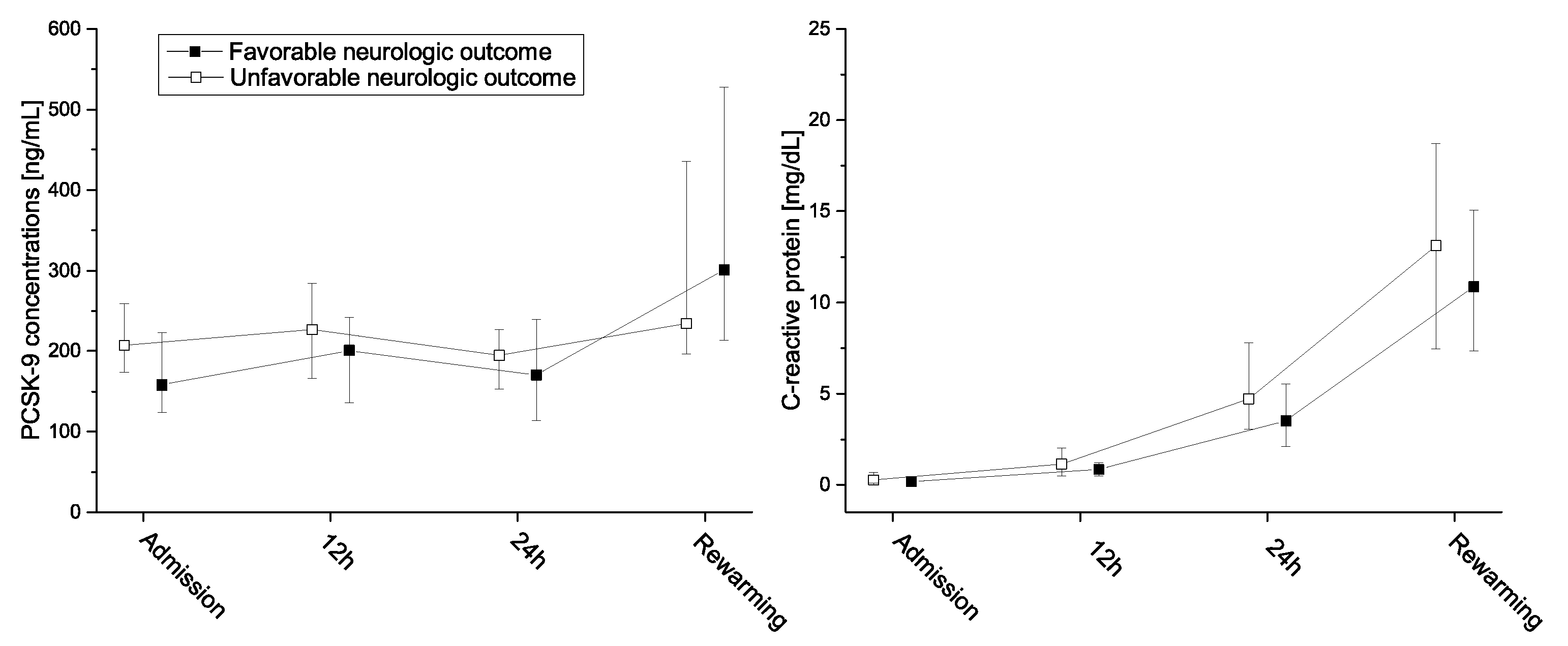
3.2. Neurologic Function
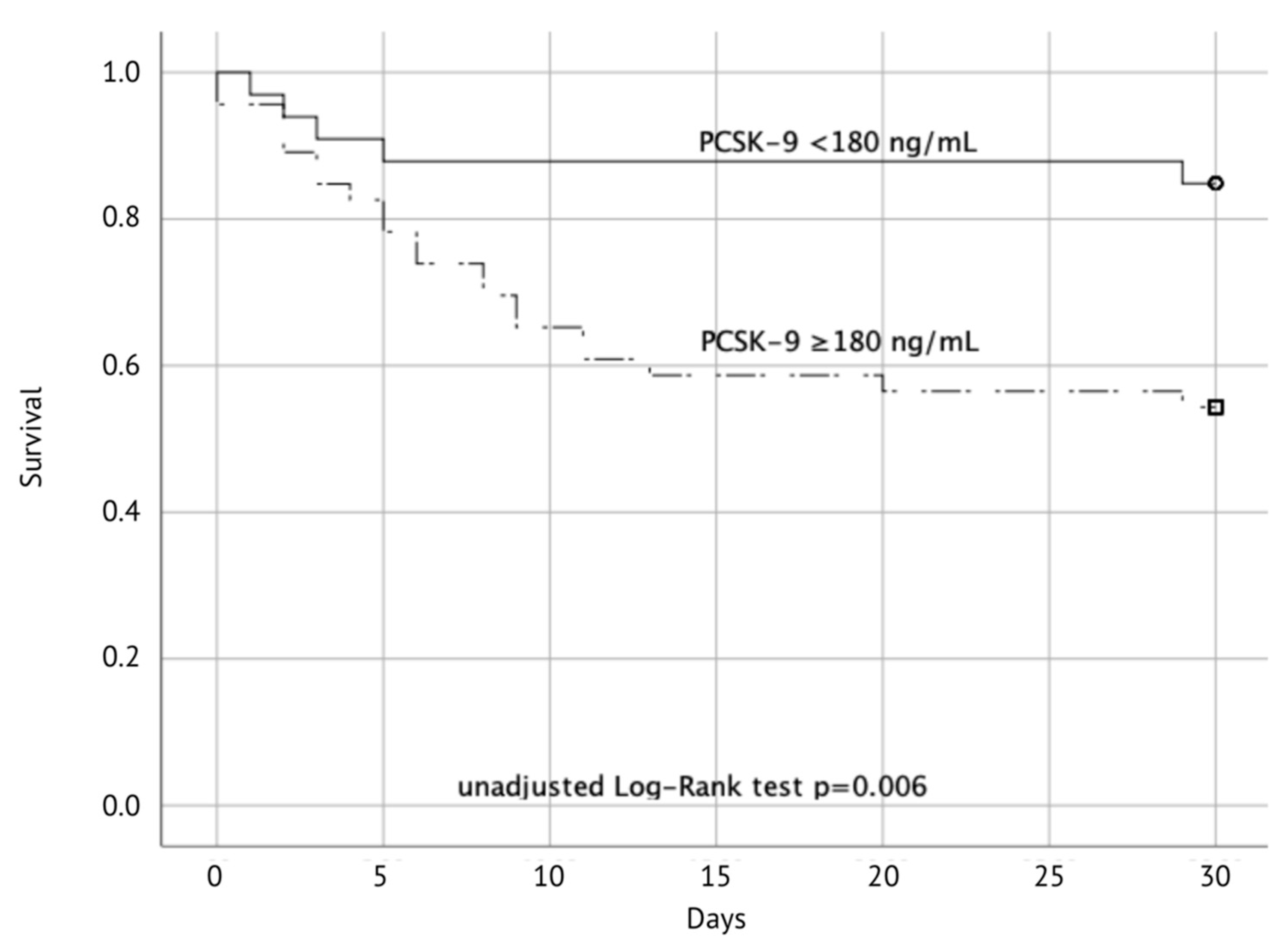
3.3. Mortality
3.4. Additional Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Multiple linear regression analysis
References
- Wicinski, M.; Zak, J.; Malinowski, B.; Popek, G.; Grzesk, G. PCSK9 signaling pathways and their potential importance in clinical practice. EPMA J. 2017, 8, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.H.; Peng, J.; Ren, Z.; Yang, J.; Li, T.T.; Li, T.H.; Wang, Z.; Wei, D.H.; Liu, L.S.; Zheng, X.L.; et al. New role of PCSK9 in atherosclerotic inflammation promotion involving the TLR4/NF-kappaB pathway. Atherosclerosis 2017, 262, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Abifadel, M.; Varret, M.; Rabes, J.P.; Allard, D.; Ouguerram, K.; Devillers, M.; Cruaud, C.; Benjannet, S.; Wickham, L.; Erlich, D.; et al. Mutations in PCSK9 cause autosomal dominant hypercholesterolemia. Nat. Genet. 2003, 34, 154–156. [Google Scholar] [CrossRef]
- Cohen, J.C.; Boerwinkle, E.; Mosley, T.H., Jr.; Hobbs, H.H. Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N. Engl. J. Med. 2006, 354, 1264–1272. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, C.; Harrington, R.A.; et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N. Engl. J. Med. 2018, 379, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef]
- Mu, G.; Xiang, Q.; Zhou, S.; Liu, Z.; Qi, L.; Jiang, J.; Gong, Y.; Xie, Q.; Wang, Z.; Zhang, H.; et al. Efficacy and Safety of PCSK9 Monoclonal Antibodies in Patients at High Cardiovascular Risk: An Updated Systematic Review and Meta-Analysis of 32 Randomized Controlled Trials. Adv. Ther. 2020, 37, 1496–1521. [Google Scholar] [CrossRef]
- Topchiy, E.; Cirstea, M.; Kong, H.J.; Boyd, J.H.; Wang, Y.; Russell, J.A.; Walley, K.R. Lipopolysaccharide Is Cleared from the Circulation by Hepatocytes via the Low Density Lipoprotein Receptor. PLoS ONE 2016, 11, e0155030. [Google Scholar] [CrossRef]
- Grin, P.M.; Dwivedi, D.J.; Chathely, K.M.; Trigatti, B.L.; Prat, A.; Seidah, N.G.; Liaw, P.C.; Fox-Robichaud, A.E. Low-density lipoprotein (LDL)-dependent uptake of Gram-positive lipoteichoic acid and Gram-negative lipopolysaccharide occurs through LDL receptor. Sci. Rep. 2018, 8, 10496. [Google Scholar] [CrossRef]
- Leung, A.K.K.; Genga, K.R.; Topchiy, E.; Cirstea, M.; Shimada, T.; Fjell, C.; Russell, J.A.; Boyd, J.H.; Walley, K.R. Reduced Proprotein convertase subtilisin/kexin 9 (PCSK9) function increases lipoteichoic acid clearance and improves outcomes in Gram positive septic shock patients. Sci. Rep. 2019, 9, 10588. [Google Scholar] [CrossRef]
- Boyd, J.H.; Fjell, C.D.; Russell, J.A.; Sirounis, D.; Cirstea, M.S.; Walley, K.R. Increased Plasma PCSK9 Levels Are Associated with Reduced Endotoxin Clearance and the Development of Acute Organ Failures during Sepsis. J. Innate Immun. 2016, 8, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Levels, J.H.; Pajkrt, D.; Schultz, M.; Hoek, F.J.; van Tol, A.; Meijers, J.C.; van Deventer, S.J. Alterations in lipoprotein homeostasis during human experimental endotoxemia and clinical sepsis. Biochim. Biophys. Acta 2007, 1771, 1429–1438. [Google Scholar] [CrossRef] [PubMed]
- Pajkrt, D.; Lerch, P.G.; van der Poll, T.; Levi, M.; Illi, M.; Doran, J.E.; Arnet, B.; van den Ende, A.; ten Cate, J.W.; van Deventer, S.J. Differential effects of reconstituted high-density lipoprotein on coagulation, fibrinolysis and platelet activation during human endotoxemia. Thromb. Haemost. 1997, 77, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Walley, K.R.; Thain, K.R.; Russell, J.A.; Reilly, M.P.; Meyer, N.J.; Ferguson, J.F.; Christie, J.D.; Nakada, T.A.; Fjell, C.D.; Thair, S.A.; et al. PCSK9 is a critical regulator of the innate immune response and septic shock outcome. Sci. Transl. Med. 2014. [Google Scholar] [CrossRef] [PubMed]
- Schoergenhofer, C.; Matzneller, P.; Muhlbacher, J.; Hell, L.; Zeitlinger, M.; Jilma, B. PCSK9 decreases during experimental endotoxemia. J. Intern. Med. 2020, 287, 333–335. [Google Scholar] [CrossRef]
- Rannikko, J.; Jacome Sanz, D.; Ortutay, Z.; Seiskari, T.; Aittoniemi, J.; Huttunen, R.; Syrjanen, J.; Pesu, M. Reduced plasma PCSK9 response in patients with bacteraemia is associated with mortality. J. Intern. Med. 2019, 286, 553–561. [Google Scholar] [CrossRef]
- Vecchie, A.; Bonaventura, A.; Meessen, J.; Novelli, D.; Minetti, S.; Elia, E.; Ferrara, D.; Ansaldo, A.M.; Scaravilli, V.; Villa, S.; et al. PCSK9 is associated with mortality in patients with septic shock: Data from the ALBIOS study. J. Intern. Med. 2020. [Google Scholar] [CrossRef]
- Grimaldi, D.; Guivarch, E.; Neveux, N.; Fichet, J.; Pene, F.; Marx, J.S.; Chiche, J.D.; Cynober, L.; Mira, J.P.; Cariou, A. Markers of intestinal injury are associated with endotoxemia in successfully resuscitated patients. Resuscitation 2013, 84, 60–65. [Google Scholar] [CrossRef]
- Grimaldi, D.; Sauneuf, B.; Guivarch, E.; Ricome, S.; Geri, G.; Charpentier, J.; Zuber, B.; Dumas, F.; Spaulding, C.; Mira, J.P.; et al. High Level of Endotoxemia Following Out-of-Hospital Cardiac Arrest Is Associated With Severity and Duration of Postcardiac Arrest Shock. Crit. Care Med. 2015, 43, 2597–2604. [Google Scholar] [CrossRef]
- Yang, C.L.; Zeng, Y.D.; Hu, Z.X.; Liang, H. PCSK9 promotes the secretion of pro-inflammatory cytokines by macrophages to aggravate H/R-induced cardiomyocyte injury via activating NF-kappaB signalling. Gen. Physiol. Biophys. 2020, 39, 123–134. [Google Scholar] [CrossRef]
- Ding, Z.; Liu, S.; Wang, X.; Deng, X.; Fan, Y.; Shahanawaz, J.; Shmookler Reis, R.J.; Varughese, K.I.; Sawamura, T.; Mehta, J.L. Cross-talk between LOX-1 and PCSK9 in vascular tissues. Cardiovasc. Res. 2015, 107, 556–567. [Google Scholar] [CrossRef] [PubMed]
- Ding, Z.; Pothineni, N.V.K.; Goel, A.; Luscher, T.F.; Mehta, J.L. PCSK9 and inflammation: Role of shear stress, pro-inflammatory cytokines, and LOX-1. Cardiovasc. Res. 2020, 116, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Mauracher, L.M.; Buchtele, N.; Schorgenhofer, C.; Weiser, C.; Herkner, H.; Merrelaar, A.; Spiel, A.O.; Hell, L.; Ay, C.; Pabinger, I.; et al. Increased Citrullinated Histone H3 Levels in the Early Post-Resuscitative Period Are Associated with Poor Neurologic Function in Cardiac Arrest Survivors—A Prospective Observational Study. J. Clin. Med. 2019, 8, 1568. [Google Scholar] [CrossRef]
- Schriefl, C.; Mayr, F.B.; Poppe, M.; Zajicek, A.; Nurnberger, A.; Clodi, C.; Herkner, H.; Sulzgruber, P.; Lobmeyr, E.; Schober, A.; et al. Time of out-of-hospital cardiac arrest is not associated with outcome in a metropolitan area: A multicenter cohort study. Resuscitation 2019, 142, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Dubuc, G.; Chamberland, A.; Wassef, H.; Davignon, J.; Seidah, N.G.; Bernier, L.; Prat, A. Statins upregulate PCSK9, the gene encoding the proprotein convertase neural apoptosis-regulated convertase-1 implicated in familial hypercholesterolemia. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 1454–1459. [Google Scholar] [CrossRef]
- Genga, K.R.; Lo, C.; Cirstea, M.S.; Leitao Filho, F.S.; Walley, K.R.; Russell, J.A.; Linder, A.; Francis, G.A.; Boyd, J.H. Impact of PCSK9 loss-of-function genotype on 1-year mortality and recurrent infection in sepsis survivors. EBioMedicine 2018, 38, 257–264. [Google Scholar] [CrossRef]
- Vaahersalo, J.; Skrifvars, M.B.; Pulkki, K.; Stridsberg, M.; Rosjo, H.; Hovilehto, S.; Tiainen, M.; Varpula, T.; Pettila, V.; Ruokonen, E.; et al. Admission interleukin-6 is associated with post resuscitation organ dysfunction and predicts long-term neurological outcome after out-of-hospital ventricular fibrillation. Resuscitation 2014, 85, 1573–1579. [Google Scholar] [CrossRef]
- Bro-Jeppesen, J.; Johansson, P.I.; Kjaergaard, J.; Wanscher, M.; Ostrowski, S.R.; Bjerre, M.; Hassager, C. Level of systemic inflammation and endothelial injury is associated with cardiovascular dysfunction and vasopressor support in post-cardiac arrest patients. Resuscitation 2017, 121, 179–186. [Google Scholar] [CrossRef]
- Bro-Jeppesen, J.; Kjaergaard, J.; Wanscher, M.; Nielsen, N.; Friberg, H.; Bjerre, M.; Hassager, C. Systemic Inflammatory Response and Potential Prognostic Implications After Out-of-Hospital Cardiac Arrest: A Substudy of the Target Temperature Management Trial. Crit. Care Med. 2015, 43, 1223–1232. [Google Scholar] [CrossRef]
- Lee, H.Y.; Lee, D.H.; Lee, B.K.; Jeung, K.W.; Jung, Y.H.; Park, J.S.; Min, J.H.; Min, Y.I. The association between lipid profiles and the neurologic outcome in patients with out-of-hospital cardiac arrest. Resuscitation 2019, 145, 26–31. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Total (n = 79) | PCSK-9–Levels (ng/mL) | ||
|---|---|---|---|---|
| <165 (n = 29) | ≥165 (n = 50) | p | ||
| Gender, male n (%) | 61 (77) | 25 (86) | 36 (72) | 0.149 |
| Age, years (IQR) | 59 (46–69) | 56 (44–67) | 59 (51–70) | 0.222 |
| Concomitant diseases, n (%) | ||||
| Hyperlipidemia | 20 (25) | 5 (17) | 15 (30) | 0.212 |
| DM II | 16 (20) | 7 (24) | 9 (18) | 0.516 |
| Coronary artery disease | 16 (20) | 7 (24) | 9 (18) | 0.516 |
| Hypertension | 31 (39) | 13 (45) | 18 (36) | 0.442 |
| Smoker | 26 (33) | 9 (31) | 17 (34) | 0.788 |
| COPD | 8 (10) | 3 (10) | 5 (10) | 0.961 |
| PAD | 6 (8) | 0 (0) | 6 (12) | 0.054 |
| Statine-use, n (%) | 14 (18) | 3 (10) | 11 (22) | 0.194 |
| CPC 1/2, n (%) | 36 (46) | 20 (69) | 16 (32) | 0.002 |
| Witnessed, n (%) | 64 (81) | 22 (76) | 42 (84) | 0.276 |
| BLS, n (%) | 55 (70) | 19 (66) | 36 (74) | 0.375 |
| Initial shockable rhythm, n (%) | 59 (75) | 22 (76) | 37 (74) | 0.855 |
| Time to sustained ROSC, min (IQR) | 25 (17–43) | 20 (13–41) | 29 (20–43) | 0.056 |
| No-flow time, min (IQR) | 0 (0–3) | 0 (0–3) | 0 (0–3) | 0.846 |
| Low-flow time, min (IQR) | 25.0 (16.0–40.5) | 20 (10–38) | 27 (20–41) | 0.064 |
| 30-day survival, n (%) | 53 (67) | 24 (83) | 29 (58) | 0.025 |
| Core body temperature (admission), °C (IQR) | 35.3 (34.8–35.8) | 35.5 (34.9–35.9) | 35.2 (34.7–35.7) | 0.314 |
| Blood gas values (admission) | ||||
| pH (IQR) | 7.2 (7.0–7.1) | 7.2 (6.9–7.3) | 7.2 (7.1–7.2) | 0.782 |
| Lactate, mmol/L (IQR) | 7.6 (5.2–10.0) | 7.2 (4.4–10.6) | 7.6 (6.1–9.9) | 0.625 |
| Laboratory values (admission) | ||||
| Hemoglobin, g/dL (IQR) | 13.9 (12.4–15.3) | 14.1 (12.8–15.4) | 13.8 (12.2–15.2) | 0.444 |
| Total Platelet count, G/L (IQR) | 205 (169–245) | 225 (179–250) | 202 (163–245) | 0.502 |
| Leukocytes, G/L (IQR) | 14.3 (10.5–18.9) | 14.9 (8.7–19.1) | 14.3 (11.0–18.4) | 0.499 |
| Troponin-T, ng/L (IQR) | 64 (32–244) | 130 (38–467) | 54 (27–192) | 0.153 |
| Prothrombin-time, % (IQR) | 77 (65–91) | 72 (59–83) | 81 (66–91) | 0.184 |
| TG, mg/dL (IQR) | 125 (81–173) | 115 (76–154) | 133 (83–179) | 0.292 |
| Creatinin, mg/dL (IQR) | 1.1 (0.9–1.3) | 1.2 (0.9–1.3) | (0.9–1.3) | 0.577 |
| Albumin, g/L (IQR) | 38 (34–40) | 39 (36–41) | 37 (33–41) | 0.048 |
| Cholinesterase, kU/L (IQR) | 6.7 (5.4–8.0) | 6.8 (5.1–8.1) | 6.7 (5.5–7.8) | 0.718 |
| Total cholesterol, mg/dL (IQR) | 163 (133–201) | 160 (139–182) | 166 (127–212) | 0.897 |
| ASAT (GOT), U/L (IQR) | 135 (78–226) | 135 (75–201) | 137 (83–264) | 0.600 |
| ALAT (GPT), U/L (IQR) | 112 (56–200) | 107 (66–164) | 127 (54–210) | 0.640 |
| Laboratory values | ||||
| PCSK–9 (admission), ng/mL (IQR) | 193 (145–239) | 126 (115–147) | 223 (194–266) | 0.000 |
| PCSK–9 (12 h), ng/mL (IQR) | 210 (151–267) | 156 (127–209) | 239 (204–298) | 0.000 |
| PCSK–9 (24 h), ng/mL (IQR) | 187 (198–457) | 145 (108–213) | 202 (178–244) | 0.002 |
| NSE (24 h), µg/L (IQR) | 33.1 (21.4–54.4) | 29.6 (20.3–44.8) | 34.7 (22.1–57.6) | 0.370 |
| S-100 (24 h), µg/L (IQR) | 0.15 (0.09–0.36) | 0.10 (0.10–0.16) | 0.17 (0.11–0.52) | 0.007 |
| CRP (admission), mg/dL (IQR) | 0.2 (0.1–0.6) | 0.2 (0.1–0.3) | 0.3 (0.1–0.8) | 0.045 |
| CRP (12 h), mg/dL (IQR) | 0.99 (0.6–1.6) | 0.8 (0.5–1.1) | 1.3 (0.7–2.1) | 0.029 |
| CRP (24 h), mg/dL (IQR) | 4.2 (2.8–6.1) | 3.8 (2.4–5.4) | 4.4 (2.8–7.7) | 0.270 |
| Low CRP Low PCSK–9 | High CRP Low PCSK–9 | Low CRP High PCSK–9 | High CRP High PCSK–9 | |
|---|---|---|---|---|
| Unfavorable neurologic function (CPC 3–5) | 28% n = 25 | 50% n = 4 | 61% n = 31 | 79% n = 19 |
| 30-day mortality | 11% n = 28 | 40% n = 5 | 36% n = 28 | 61% n = 18 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merrelaar, A.; Buchtele, N.; Schriefl, C.; Clodi, C.; Poppe, M.; Ettl, F.; Herkner, H.; Jilma, B.; Schwameis, M.; Schoergenhofer, C. Low PCSK-9 levels Are Associated with Favorable Neurologic Function after Resuscitation from out of Hospital Cardiac Arrest. J. Clin. Med. 2020, 9, 2606. https://doi.org/10.3390/jcm9082606
Merrelaar A, Buchtele N, Schriefl C, Clodi C, Poppe M, Ettl F, Herkner H, Jilma B, Schwameis M, Schoergenhofer C. Low PCSK-9 levels Are Associated with Favorable Neurologic Function after Resuscitation from out of Hospital Cardiac Arrest. Journal of Clinical Medicine. 2020; 9(8):2606. https://doi.org/10.3390/jcm9082606
Chicago/Turabian StyleMerrelaar, Anne, Nina Buchtele, Christoph Schriefl, Christian Clodi, Michael Poppe, Florian Ettl, Harald Herkner, Bernd Jilma, Michael Schwameis, and Christian Schoergenhofer. 2020. "Low PCSK-9 levels Are Associated with Favorable Neurologic Function after Resuscitation from out of Hospital Cardiac Arrest" Journal of Clinical Medicine 9, no. 8: 2606. https://doi.org/10.3390/jcm9082606
APA StyleMerrelaar, A., Buchtele, N., Schriefl, C., Clodi, C., Poppe, M., Ettl, F., Herkner, H., Jilma, B., Schwameis, M., & Schoergenhofer, C. (2020). Low PCSK-9 levels Are Associated with Favorable Neurologic Function after Resuscitation from out of Hospital Cardiac Arrest. Journal of Clinical Medicine, 9(8), 2606. https://doi.org/10.3390/jcm9082606