Lighting Up the Tumor—Fluorescein-Guided Resection of Gangliogliomas

 ,
, 
 ,
,  and
and
Abstract
:1. Introduction
2. Experimental Section
2.1. Patients and Pre- and Postoperative Clinical and Radiological Evaluation
2.2. Surgical Protocol
2.3. Preoperative Use of Glucocorticoids
2.4. Intraoperative Fluorescence Characteristics and Side Effects
2.5. Extent of Resection
2.6. Ethical Approval
3. Results
3.1. Fluorescence
3.2. Extent of Resection
3.3. Karnofsky Performance Scale (KPS)
3.4. Adverse Events
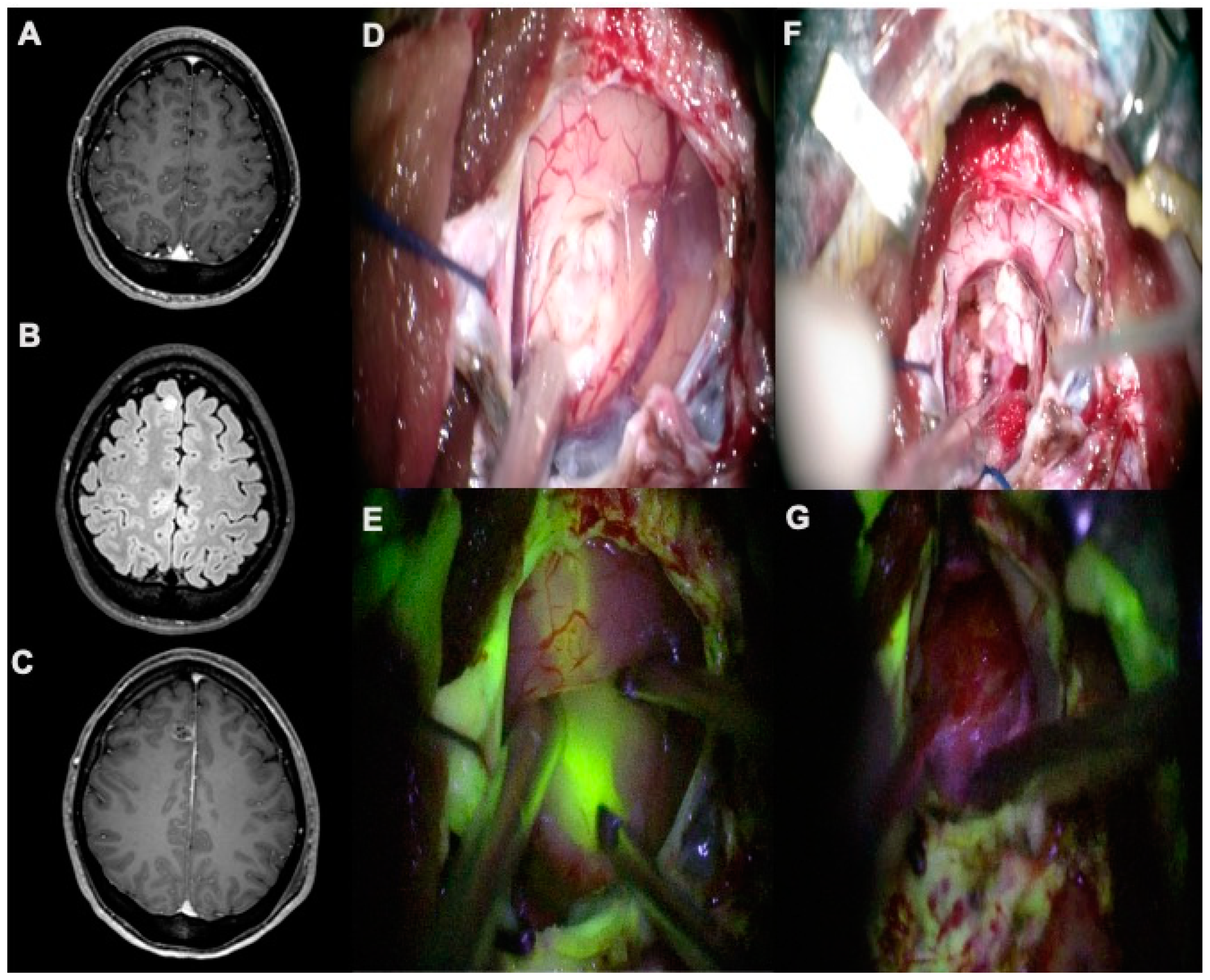
3.5. Representative Case
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Demierre, B.; Stichnoth, F.A.; Hori, A.; Spoerri, O. Intracerebral ganglioglioma. J. Neurosurg. 1986, 65, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Courville, C.B. Ganglioglioma: Tumor of the central nervous system.; review of the literature and report of two cases. Arch. Neurol. Psychiatry 1930, 24, 439–491. [Google Scholar] [CrossRef]
- Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.; Burger, P.C.; Jouvet, A.; Scheithauer, B.W.; Kleihues, P. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007, 114, 97–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, N.R.; Wang, K.C.; Bang, J.S.; Choe, G.; Park, Y.; Kim, S.K.; Cho, B.K.; Chi, J.G. Glioblastomatous transformation of ganglioglioma: Case report with reference to molecular genetic and flow cytometric analysis. Pathol. Int. 2003, 53, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Zentner, J.; Wolf, H.K.; Ostertun, B.; Hufnagel, A.; Campos, M.G.; Solymosi, L.; Schramm, J. Gangliogliomas: Clinical, radiological, and histopathological findings in 51 patients. J. Neurol. Neurosurg. Psychiatry 1994, 57, 1497–1502. [Google Scholar] [CrossRef] [PubMed]
- Luyken, C.; Blumcke, I.; Fimmers, R.; Urbach, H.; Wiestler, O.D.; Schramm, J. Supratentorial gangliogliomas: Histopathologic grading and tumor recurrence in 184 patients with a median follow-up of 8 years. Cancer 2004, 101, 146–155. [Google Scholar] [CrossRef]
- Dudley, R.W.; Torok, M.R.; Gallegos, D.R.; Mulcahy-Levy, J.M.; Hoffman, L.M.; Liu, A.K.; Handler, M.H.; Hankinson, T.C. Pediatric low-grade ganglioglioma: Epidemiology, treatments, and outcome analysis on 348 children from the surveillance, epidemiology, and end results database. Neurosurgery 2015, 76, 313–319. [Google Scholar] [CrossRef] [Green Version]
- Song, J.Y.; Kim, J.H.; Cho, Y.H.; Kim, C.J.; Lee, E.J. Treatment and outcomes for gangliogliomas: A single-center review of 16 patients. Brain Tumor Res. Treat. 2014, 2, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Ruban, D.; Byrne, R.W.; Kanner, A.; Smith, M.; Cochran, E.J.; Roh, D.; Whisler, W.W. Chronic epilepsy associated with temporal tumors: Long-term surgical outcome. Neurosurg. Focus 2009, 27, E6. [Google Scholar] [CrossRef]
- Provenzale, J.M.; Ali, U.; Barboriak, D.P.; Kallmes, D.F.; Delong, D.M.; McLendon, R.E. Comparison of patient age with MR imaging features of gangliogliomas. AJR Am. J. Roentgenol. 2000, 174, 859–862. [Google Scholar] [CrossRef]
- Lang, F.F.; Epstein, F.J.; Ransohoff, J.; Allen, J.C.; Wisoff, J.; Abbott, I.R.; Miller, D.C. Central nervous system gangliogliomas. Part 2: Clinical outcome. J. Neurosurg. 1993, 79, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Rumana, C.S.; Valadka, A.B. Radiation therapy and malignant degeneration of benign supratentorial gangliogliomas. Neurosurgery 1998, 42, 1038–1043. [Google Scholar] [CrossRef] [PubMed]
- Preuss, M.; Renner, C.; Krupp, W.; Christiansen, H.; Fischer, L.; Merkenschlager, A.; Kiess, W.; Muller, W.; Manzo, N.; Meixensberger, J.; et al. The use of 5-aminolevulinic acid fluorescence guidance in resection of pediatric brain tumors. Childs Nerv. Syst. ChNS 2013, 29, 1263–1267. [Google Scholar] [CrossRef]
- Valdes, P.A.; Jacobs, V.; Harris, B.T.; Wilson, B.C.; Leblond, F.; Paulsen, K.D.; Roberts, D.W. Quantitative fluorescence using 5-aminolevulinic acid-induced protoporphyrin IX biomarker as a surgical adjunct in low-grade glioma surgery. J. Neurosurg. 2015, 123, 771–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goryaynov, S.A.; Widhalm, G.; Goldberg, M.F.; Chelushkin, D.; Spallone, A.; Chernyshov, K.A.; Ryzhova, M.; Pavlova, G.; Revischin, A.; Shishkina, L.; et al. The Role of 5-ALA in low-grade gliomas and the influence of antiepileptic drugs on intraoperative fluorescence. Front. Oncol. 2019, 9, 423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.Y.; Thawani, J.P.; Pierce, J.; Zeh, R.; Martinez-Lage, M.; Chanin, M.; Venegas, O.; Nims, S.; Learned, K.; Keating, J.; et al. Intraoperative near-infrared optical imaging can localize gadolinium-enhancing gliomas during surgery. Neurosurgery 2016, 79, 856–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acerbi, F.; Broggi, M.; Schebesch, K.M.; Hohne, J.; Cavallo, C.; De Laurentis, C.; Eoli, M.; Anghileri, E.; Servida, M.; Boffano, C.; et al. Fluorescein-guided surgery for resection of high-grade gliomas: A multicentric prospective phase II study (FLUOGLIO). Clin. Cancer Res. 2017. [Google Scholar] [CrossRef] [Green Version]
- Schebesch, K.M.; Proescholdt, M.; Hohne, J.; Hohenberger, C.; Hansen, E.; Riemenschneider, M.J.; Ullrich, W.; Doenitz, C.; Schlaier, J.; Lange, M.; et al. Sodium fluorescein-guided resection under the YELLOW 560 nm surgical microscope filter in malignant brain tumor surgery—A feasibility study. Acta Neurochir. 2013, 155, 693–699. [Google Scholar] [CrossRef]
- Rey-Dios, R.; Cohen-Gadol, A.A. Intraoperative fluorescence for resection of hemangioblastomas. Acta Neurochir. 2013, 155, 1287–1292. [Google Scholar] [CrossRef]
- Hohne, J.; Hohenberger, C.; Proescholdt, M.; Riemenschneider, M.J.; Wendl, C.; Brawanski, A.; Schebesch, K.M. Fluorescein sodium-guided resection of cerebral metastases-an update. Acta Neurochir. 2016, 159, 363–367. [Google Scholar] [CrossRef]
- Acerbi, F.; Cavallo, C.; Schebesch, K.M.; Akcakaya, M.O.; de Laurentis, C.; Hamamcioglu, M.K.; Broggi, M.; Brawanski, A.; Falco, J.; Cordella, R.; et al. Fluorescein-guided resection of intramedullary spinal cord tumors: Results from a preliminary, multicentric, retrospective study. World Neurosurg. 2017, 108, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Akcakaya, M.O.; Goker, B.; Kasimcan, M.O.; Hamamcioglu, M.K.; Kiris, T. Use of sodium fluorescein in meningioma surgery performed under the YELLOW-560 nm surgical microscope filter: Feasibility and preliminary results. World Neurosurg. 2017, 107, 966–973. [Google Scholar] [CrossRef] [PubMed]
- Hamamcioglu, M.K.; Akcakaya, M.O.; Goker, B.; Kasimcan, M.O.; Kiris, T. The use of the YELLOW 560nm surgical microscope filter for sodium fluorescein-guided resection of brain tumors: Our preliminary results in a series of 28 patients. Clin. Neurol. Neurosurg. 2016, 143, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Nduom, E.K.; Yang, C.; Merrill, M.J.; Zhuang, Z.; Lonser, R.R. Characterization of the blood-brain barrier of metastatic and primary malignant neoplasms. J. Neurosurg. 2013, 119, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Watkins, S.; Robel, S.; Kimbrough, I.F.; Robert, S.M.; Ellis-Davies, G.; Sontheimer, H. Disruption of astrocyte-vascular coupling and the blood-brain barrier by invading glioma cells. Nat. Commun. 2014, 5, 4196. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Baird, A.; Eliceiri, B.P. In vivo measurement of glioma-induced vascular permeability. Methods Mol. Biol. 2011, 763, 417–422. [Google Scholar] [CrossRef] [Green Version]
- Novotny, H.R.; Alvis, D.L. A method of photographing fluorescence in circulating blood in the human retina. Circulation 1961, 24, 82–86. [Google Scholar] [CrossRef] [Green Version]
- Ferroli, P.; Acerbi, F.; Albanese, E.; Tringali, G.; Broggi, M.; Franzini, A.; Broggi, G. Application of intraoperative indocyanine green angiography for CNS tumors: Results on the first 100 cases. Acta Neurochir. Suppl. 2011, 109, 251–257. [Google Scholar] [CrossRef]
- Rey-Dios, R.; Cohen-Gadol, A.A. Technical principles and neurosurgical applications of fluorescein fluorescence using a microscope-integrated fluorescence module. Acta Neurochir. 2013, 155, 701–706. [Google Scholar] [CrossRef]
- Okuda, T.; Kataoka, K.; Yabuuchi, T.; Yugami, H.; Kato, A. Fluorescence-guided surgery of metastatic brain tumors using fluorescein sodium. J. Clin. Neurosci. 2010, 17, 118–121. [Google Scholar] [CrossRef]
- Minkin, K.; Naydenov, E.; Gabrovski, K.; Dimova, P.; Penkov, M.; Tanova, R.; Nachev, S.; Romanski, K. Intraoperative fluorescein staining for benign brain tumors. Clin. Neurol. Neurosurg. 2016, 149, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Dilek, O.; Ihsan, A.; Tulay, H. Anaphylactic reaction after fluorescein sodium administration during intracranial surgery. J. Clin. Neurosci. 2011, 18, 430–431. [Google Scholar] [CrossRef] [PubMed]
- Tanahashi, S.; Lida, H.; Dohi, S. An anaphylactoid reaction after administration of fluorescein sodium during neurosurgery. Anesth. Analg. 2006, 103, 503. [Google Scholar] [CrossRef] [PubMed]
- Varshneya, K.; Sarmiento, J.M.; Nuno, M.; Lagman, C.; Mukherjee, D.; Nuno, K.; Babu, H.; Patil, C.G. A national perspective of adult gangliogliomas. J. Clin. Neurosci. 2016, 30, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Diaz, R.J.; Dios, R.R.; Hattab, E.M.; Burrell, K.; Rakopoulos, P.; Sabha, N.; Hawkins, C.; Zadeh, G.; Rutka, J.T.; Cohen-Gadol, A.A. Study of the biodistribution of fluorescein in glioma-infiltrated mouse brain and histopathological correlation of intraoperative findings in high-grade gliomas resected under fluorescein fluorescence guidance. J. Neurosurg. 2015, 122, 1360–1369. [Google Scholar] [CrossRef] [Green Version]
- Neira, J.A.; Ung, T.H.; Sims, J.S.; Malone, H.R.; Chow, D.S.; Samanamud, J.L.; Zanazzi, G.J.; Guo, X.; Bowden, S.G.; Zhao, B.; et al. Aggressive resection at the infiltrative margins of glioblastoma facilitated by intraoperative fluorescein guidance. J. Neurosurg. 2016, 127, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Eljamel, M.S.; Mahboob, S.O. The effectiveness and cost-effectiveness of intraoperative imaging in high-grade glioma resection; a comparative review of intraoperative ALA, fluorescein, ultrasound and MRI. Photodiagn. Photodyn. Ther. 2016, 16, 35–43. [Google Scholar] [CrossRef]


{kind=link}
| Pat. | Age | Sex | Location | Presenting Symptom | EOR | FLI | Histology | KPS Pre | KPS Post |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 52 | f | Left frontal | Headache | STR | ++ | Ganglioglioma (WHO grade I) | 100 | 100 |
| 2 | 21 | f | Left frontal | Seizure | GTR | ++ | Ganglioglioma (WHO grade I) | 100 | 100 |
| 3 | 32 | f | Left temporal | Headache | GTR | ++ | Ganglioglioma (WHO grade I) | 100 | 100 |
| 4 | 37 | m | Left temporal | Expressive language disorder | GTR | ++ | Ganglioglioma (WHO grade I) | 100 | 100 |
| 5 | 19 | f | Right frontal | Seizure | GTR | + | Ganglioglioma (WHO grade I) | 100 | 100 |
| 6 | 55 | m | Left parieto-occipital | Loss of consciousness | GTR | ++ | Ganglioglioma (WHO grade I) | 100 | 100 |
| 7 | 3 | f | Medulla oblongata | Trigeminal pain | NTR Biopsy | + | Ganglioglioma (WHO grade I) | 100 | 60 |
| 8 | 8 | m | Sellar and suprasellar | Visual disturbance, hormonal deficit | STR (i) | + | Ganglioglioma (WHO grade I) | 70 | 70 |
| 9 | 16 | m | Left frontal | Seizures | GTR | + | Ganglioglioma (WHO grade I) | 100 | 100 |
| 10 | 78 | f | Left temporal | Expressive language disorder | GTR | ++ | Anaplastic ganglioglioma (WHO grade II) | 90 | 30 |
| 11 | 20 | f | Right frontal | Seizure | GTR | ++ | Ganglioglioma (WHO grade I) | 90 | 90 |
| 12 | 17 | f | Left temporal | Seizure, cognitive deficit | GTR | ++ | Ganglioglioma and subependymal giant cell astrocytoma (WHO grade I) | 80 | 80 |
| 13 | 3 | f | Right temporal | Abnormal head posture | NTR (i) | + | Ganglioglioma (WHO grade I) | 90 | 90 |
| 14 | 16 | f | Left temporoparietal | Seizure | GTR | + | Ganglioglioma (WHO grade I) | 90 | 80 |
| 15 | 15 | f | Left parietal | Follow-up in NF 1 | GTR | ++ | Ganglioglioma (WHO grade I) | 100 | 100 |
| 7 | 4 | f | Multifocal right temporal Biopsy | Follow-up (Patient 7) | Biopsy | ++ | Ganglioglioma (WHO grade I) | 90 | 90 |
| 16 | 14 | m | Right parietal | Seizure | GTR | ++ | Ganglioglioma (WHO grade I) | 90 | 90 |
| 17 | 3 | f | Vermis, cerebellar | Ataxia | STR (i) | ++ | Desmoplastic infantile ganglioglioma (WHO grade I) | 80 | 60 |
| 18 | 23 | f | Cerebellar, vermis, midbrain, pineal | Headache | NTR (i) | + | Ganglioglioma (WHO grade I) | 100 | 70 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Höhne, J.; Acerbi, F.; Falco, J.; Akçakaya, M.O.; Schmidt, N.O.; Kiris, T.; de Laurentis, C.; Ferroli, P.; Broggi, M.; Schebesch, K.-M. Lighting Up the Tumor—Fluorescein-Guided Resection of Gangliogliomas. J. Clin. Med. 2020, 9, 2405. https://doi.org/10.3390/jcm9082405
Höhne J, Acerbi F, Falco J, Akçakaya MO, Schmidt NO, Kiris T, de Laurentis C, Ferroli P, Broggi M, Schebesch K-M. Lighting Up the Tumor—Fluorescein-Guided Resection of Gangliogliomas. Journal of Clinical Medicine. 2020; 9(8):2405. https://doi.org/10.3390/jcm9082405
Chicago/Turabian StyleHöhne, Julius, Francesco Acerbi, Jacopo Falco, Mehmet Osman Akçakaya, Nils Ole Schmidt, Talat Kiris, Camilla de Laurentis, Paolo Ferroli, Morgan Broggi, and Karl-Michael Schebesch. 2020. "Lighting Up the Tumor—Fluorescein-Guided Resection of Gangliogliomas" Journal of Clinical Medicine 9, no. 8: 2405. https://doi.org/10.3390/jcm9082405
APA StyleHöhne, J., Acerbi, F., Falco, J., Akçakaya, M. O., Schmidt, N. O., Kiris, T., de Laurentis, C., Ferroli, P., Broggi, M., & Schebesch, K.-M. (2020). Lighting Up the Tumor—Fluorescein-Guided Resection of Gangliogliomas. Journal of Clinical Medicine, 9(8), 2405. https://doi.org/10.3390/jcm9082405