Walking Speed is the Sole Determinant Criterion of Sarcopenia of Mild Cognitive Impairment in Japanese Elderly Patients with Type 2 Diabetes Mellitus



Abstract
1. Introduction
2. Methods
2.1. Study Design and Subjects
2.2. Measurements
2.2.1. Patients’ Medical Records
2.2.2. Measurements of Parameters
2.2.3. Assessment of Mild Cognitive Impairment (MCI)
2.2.4. Assessment of Sarcopenia
2.3. Statistical Analyses
3. Results
3.1. General Characteristics
3.2. Unadjusted Odds Ratio
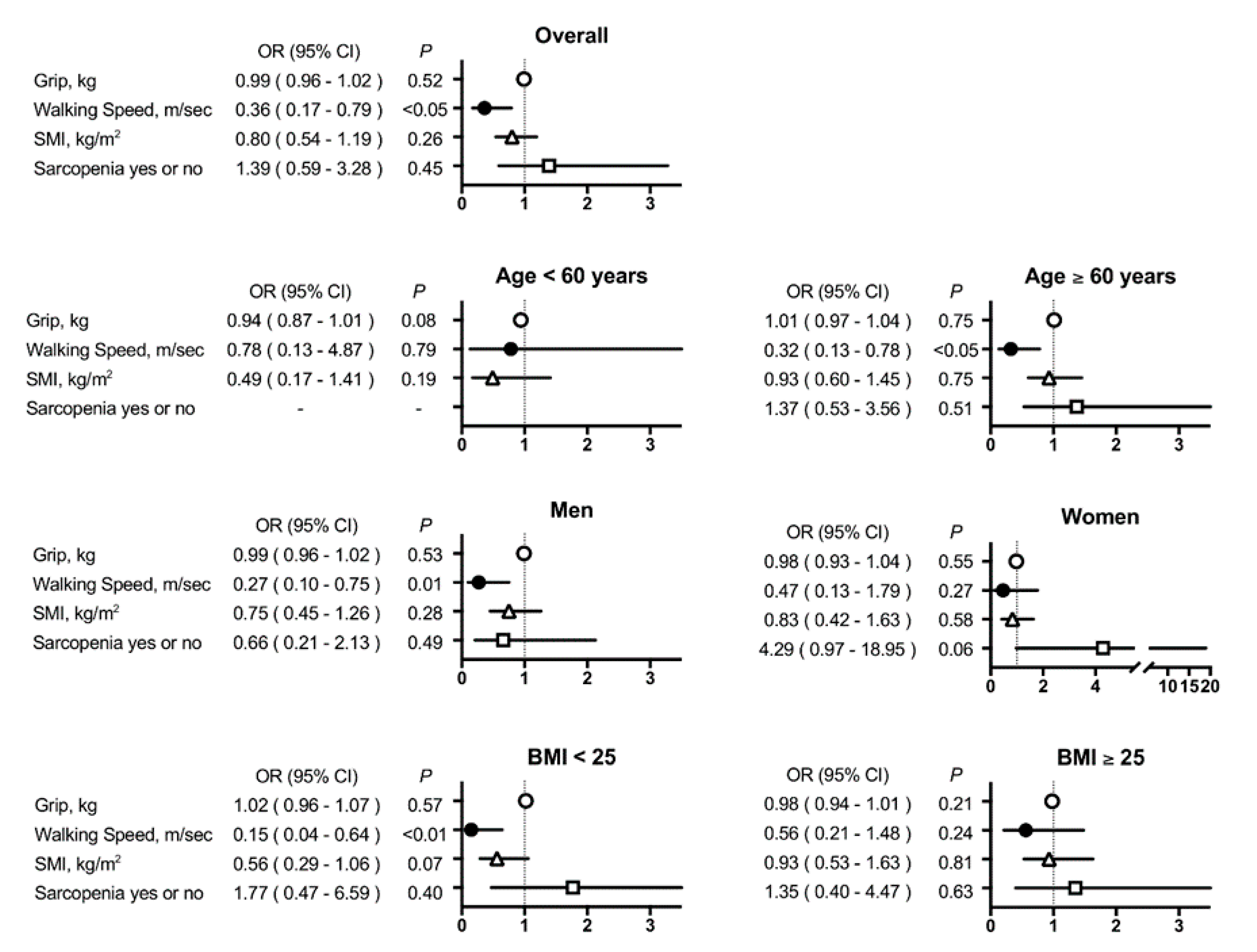
3.3. Multivariate-Adjusted Odds Ratio
4. Discussion
4.1. Characteristics of Patients in the MCI Group
4.2. Walking Speed and MCI
4.3. Why is Reduced Walking Speed Associated with MCI?
4.4. Walking Speed and MCI in the Subgroups
4.4.1. Elderly vs. Young
4.4.2. Non-Overweight Versus Overweight
4.4.3. Men vs. Women
4.5. Clinical Usefulness
4.6. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. 6D71 Mild Neurocognitive Disorder; 2018. Available online: http://icd.who.int/ (accessed on 15 April 2020).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM-5; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Flicker, C.; Ferris, S.H.; Reisberg, B. Mild cognitive impairment in the elderly: Predictors of dementia. Neurology 1991, 41, 1006–1009. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild cognitive impairment: Clinical characterization and outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Sommerlad, A.; Lyketsos, C.G.; Livingston, G. Modifiable predictors of dementia in mild cognitive impairment: A systematic review and meta-analysis. Am. J. Psychiatry 2015, 172, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Gillis, C.; Mirzaei, F.; Potashman, M.; Ikram, M.A.; Maserejian, N. The incidence of mild cognitive impairment: A systematic review and data synthesis. Alzheimers Dement. 2019, 11, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Biessels, G.J.; Despa, F. Cognitive decline and dementia in diabetes mellitus: Mechanisms and clinical implications. Nat. Rev. Endocrinol. 2018, 14, 591–604. [Google Scholar] [CrossRef]
- Biessels, G.J.; Whitmer, R.A. Cognitive dysfunction in diabetes: How to implement emerging guidelines. Diabetologia 2019, 63, 3–9. [Google Scholar] [CrossRef]
- Xue, M.; Xu, W.; Ou, Y.N.; Cao, X.P.; Tan, M.S.; Tan, L.; Yu, J.T. Diabetes mellitus and risks of cognitive impairment and dementia: A systematic review and meta-analysis of 144 prospective studies. Ageing Res. Rev. 2019, 55, 100944. [Google Scholar] [CrossRef]
- Ohara, T.; Doi, Y.; Ninomiya, T.; Hirakawa, Y.; Hata, J.; Iwaki, T.; Kanba, S.; Kiyohara, Y. Glucose tolerance status and risk of dementia in the community: The Hisayama study. Neurology 2011, 77, 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Feinkohl, I.; Price, J.F.; Strachan, M.W.J.; Frier, B.M. The impact of diabetes on cognitive decline: Potential vascular, metabolic, and psychosocial risk factors. Alzheimer’s Res. Ther. 2015, 7, 46. [Google Scholar] [CrossRef]
- Haroon, N.N.; Austin, P.C.; Shah, B.R.; Wu, J.; Gill, S.S.; Booth, G.L. Risk of dementia in seniors with newly diagnosed diabetes: A population-based study. Diabetes Care 2015, 38, 1868–1875. [Google Scholar] [CrossRef]
- Gomez-Gomez, M.E.; Zapico, S.C. Frailty, Cognitive Decline, Neurodegenerative Diseases and Nutrition Interventions. Int. J. Mol. Sci. 2019, 20, 2842. [Google Scholar] [CrossRef]
- Schernthaner, G.; Schernthaner-Reiter, M.H. Diabetes in the older patient: Heterogeneity requires individualisation of therapeutic strategies. Diabetologia 2018, 61, 1503–1516. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zúñiga, C.; Arai, H.; Boirie, Y.; Chen, L.-K.; Fielding, R.A.; Martin, F.C.; Michel, J.-P.; et al. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef]
- Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10600000-Daijinkanboukouseikagakuka/0000069410.pdf (accessed on 15 April 2020).
- Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10600000-Daijinkanboukouseikagakuka/0000080278.pdf (accessed on 15 April 2020).
- Kim, M.; Shinkai, S.; Murayama, H.; Mori, S. Comparison of segmental multifrequency bioelectrical impedance analysis with dual-energy X-ray absorptiometry for the assessment of body composition in a community-dwelling older population. Geriatr. Gerontol. Int. 2015, 15, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Ahn, S.; Kim, Y.J.; Ji, M.J.; Kim, K.M.; Choi, S.H.; Jang, H.C.; Lim, S. Comparison between Dual-Energy X-ray Absorptiometry and Bioelectrical Impedance Analyses for Accuracy in Measuring Whole Body Muscle Mass and Appendicular Skeletal Muscle Mass. Nutrients 2018, 10, 738. [Google Scholar] [CrossRef]
- Ng, S.S.M.; Ng, P.C.M.; Lee, C.Y.W.; Ng, E.S.W.; Tong, M.H.W.; Fong, S.S.M.; Tsang, W.W.N. Assessing the walking speed of older adults: The influence of walkway length. Am. J. Phys. Med. Rehabil. 2013, 92, 776–780. [Google Scholar] [CrossRef] [PubMed]
- Middleton, A.; Fritz, S.L.; Lusardi, M. Walking speed: The functional vital sign. J. Aging Phys. Act. 2015, 23, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, Y.; Suzuki, H.; Yasunaga, M.; Sugiyama, M.; Ijuin, M.; Sakuma, N.; Inagaki, H.; Iwasa, H.; Ura, C.; Yatomi, N.; et al. Brief screening tool for mild cognitive impairment in older Japanese: Validation of the Japanese version of the Montreal Cognitive Assessment. Geriatr. Gerontol. Int. 2010, 10, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.D.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice guideline update summary: Mild cognitive impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Pal, K.; Mukadam, N.; Petersen, I.; Cooper, C. Mild cognitive impairment and progression to dementia in people with diabetes, prediabetes and metabolic syndrome: A systematic review and meta-analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 1149–1160. [Google Scholar] [CrossRef]
- Rosenberg, I.H. Sarcopenia: Origins and clinical relevance. J. Nutr. 1997, 127, 990s–991s. [Google Scholar] [CrossRef]
- Geijselaers, S.L.C.; Sep, S.J.S.; Stehouwer, C.D.A.; Biessels, G.J. Glucose regulation, cognition, and brain MRI in type 2 diabetes: A systematic review. Lancet Diabetes Endocrinol. 2015, 3, 75–89. [Google Scholar] [CrossRef]
- Crane, P.K.; Walker, R.; Hubbard, R.A.; Li, G.; Nathan, D.M.; Zheng, H.; Haneuse, S.; Craft, S.; Montine, T.J.; Kahn, S.E.; et al. Glucose levels and risk of dementia. N. Engl. J. Med. 2013, 369, 540–548. [Google Scholar] [CrossRef]
- Hirose, D.; Hanyu, H.; Fukasawa, R.; Hatanaka, H.; Namioka, N.H.S. Frailty in diabetes-related dementia. Geriatr. Gerontol. Int. 2016, 16, 653–655. [Google Scholar] [CrossRef] [PubMed]
- Tsugawa, A.; Ogawa, Y.; Takenoshita, N.; Kaneko, Y.; Hatanaka, H.; Jaime, E.; Fukasawa, R.; Hanyu, H. Decreased Muscle Strength and Quality in Diabetes-Related Dementia. Dement. Geriatr. Cogn. Disord. Extra 2017, 7, 454–462. [Google Scholar] [CrossRef]
- Arnold, S.E.; Arvanitakis, Z.; Macauley-Rambach, S.L.; Koenig, A.M.; Wang, H.Y.; Ahima, R.S.; Craft, S.; Gandy, S.; Buettner, C.; Stoeckel, L.E.; et al. Brain insulin resistance in type 2 diabetes and Alzheimer disease: Concepts and conundrums. Nat. Rev. Neurol. 2018, 14, 168–181. [Google Scholar] [CrossRef]
- Liu, Z.Q.; Zhang, M.X.; Wang, J.; Ding, N. Analysis of correlation between the mild cognitive impairment (MCI) and level of adiponectin in elderly patients with type 2 diabetes mellitus (T2DM). Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 5471–5477. [Google Scholar] [CrossRef]
- McMillan, J.M.; Mele, B.S.; Hogan, D.B.; Leung, A.A. Impact of pharmacological treatment of diabetes mellitus on dementia risk: Systematic review and meta-analysis. BMJ Open Diabetes Res. Care 2018, 6, e000563. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Rosenblat, J.D.; Brietzke, E.; Park, C.; Lee, Y.; Musial, N.; Pan, Z.; Mansur, R.B.; McIntyre, R.S. Comparative efficacy and acceptability of antidiabetic agents for Alzheimer’s disease and mild cognitive impairment: A systematic review and network meta-analysis. Diabetes Obes. Metab. 2018, 20, 2467–2471. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Huang-Fu, Z.; Lang, X.Y.; Chun, P.; Chi, Y.Y.; Yuan, X.Y.; Wang, X.G. Pathological and cognitive changes in patients with type 2 diabetes mellitus and comorbid MCI and protective hypoglycemic therapies: A narrative review. Rev. Neurosci. 2019, 30, 757–770. [Google Scholar] [CrossRef] [PubMed]
- Jedrziewski, M.K.; Lee, V.M.; Trojanowski, J.Q. Physical activity and cognitive health. Alzheimers Dement. 2007, 3, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Larson, E.B.; Wang, L.; Bowen, J.D.; McCormick, W.C.; Teri, L.; Crane, P.; Kukull, W. Exercise is associated with reduced risk for incident dementia among persons 65 years of age and older. Ann. Intern. Med. 2006, 144, 73–81. [Google Scholar] [CrossRef]
- Murai, J.; Nishizawa, H.; Otsuka, A.; Fukuda, S.; Tanaka, Y.; Nagao, H.; Sakai, Y.; Suzuki, M.; Yokota, S.; Tada, H.; et al. Low muscle quality in Japanese type 2 diabetic patients with visceral fat accumulation. Cardiovasc. Diabetol. 2018, 17, 112. [Google Scholar] [CrossRef]
- Holtzer, R.; George, C.J.; Izzetoglu, M.; Wang, C. The effect of diabetes on prefrontal cortex activation patterns during active walking in older adults. Brain Cogn. 2018, 125, 14–22. [Google Scholar] [CrossRef]
- Podcasy, J.L.; Epperson, C.N. Considering sex and gender in Alzheimer disease and other dementias. Dialogues Clin. Neurosci. 2016, 18, 437–446. [Google Scholar]
- Chatterjee, S.; Peters, S.A.E.; Woodward, M.; Mejia Arango, S.; Batty, G.D.; Beckett, N.; Beiser, A.; Borenstein, A.R.; Crane, P.K.; Haan, M.; et al. Type 2 Diabetes as a Risk Factor for Dementia in Women Compared With Men: A Pooled Analysis of 2.3 Million People Comprising More Than 100,000 Cases of Dementia. Diabetes Care 2016, 39, 300. [Google Scholar] [CrossRef]


{kind=link}
| All Patients | MOCA-J Score ≥ 26 | MOCA-J Score < 26 | p-Value | |
|---|---|---|---|---|
| Variables | n = 438 | n = 221 | n = 217 | |
| Age, years | 69 (60, 74) | 63 (53, 70) | 71 (66, 78) | <0.01 |
| Male, n (%) | 244 (56) | 122 (55) | 122 (56) | 0.83 |
| MOCA-J, points | 26 (23, 27) | 27 (27, 29) | 23 (21, 25) | <0.01 |
| Anthropometry | ||||
| Systolic blood pressure, mmHg | 132 (120, 143) | 130 (120, 142) | 134 (121, 145) | 0.20 |
| Diastolic blood pressure, mmHg | 74 ± 12 | 75 ± 12 | 72 ± 11 | <0.05 |
| Body weight, kg | 65.4 (56.5, 78.0) | 67.7 (59.3, 80.6) | 61.8 (54.0, 75.0) | <0.01 |
| Body mass index (BMI), kg/m² | 25.1 (22.1, 29.3) | 25.8 (22.4, 30.5) | 24.7 (22.0, 28.2) | <0.05 |
| Waist circumference, cm | 92.3 (82.0, 100.7) | 92.0 (82.3, 102.3) | 90.0 (81.3, 98.8) | 0.11 |
| Fat mass, kg | 20.9 (14.3, 29.0) | 21.6 (14.5, 31.6) | 19.8 (14.2, 26.7) | <0.05 |
| Fat ratio, % | 32.5 (25.1, 39.1) | 33.1 (24.2, 40.6) | 31.6 (25.4, 38.5) | 0.50 |
| Hand grip strength, kg | 32.0 (25.0, 42.0) | 34.0 (25.0, 43.5) | 30.0 (23.0, 40.0) | <0.01 |
| Walking speed, m/sec | 1.54 (1.43, 1.82) | 1.67 (1.43, 1.82) | 1.54 (1.25, 1.67) | <0.01 |
| Muscle mass, kg | 42.7 (36.1, 48.9) | 42.2 (37.8, 49.7) | 41.6 (34.4, 47.0) | <0.01 |
| Skeletal muscle index, kg/m² | 7.1 (6.3, 7.9) | 7.3 (6.6, 8.1) | 6.9 (6.1, 7.8) | <0.01 |
| Sarcopenia, n (%) | 38 (9) | 9 (4) | 29 (13) | <0.01 |
| Comorbidities | ||||
| Duration of diabetes mellitus, years | 15 (9, 21) | 12 (7, 18) | 16 (11, 23) | <0.01 |
| Hypertension, n (%) | 304 (69) | 150 (68) | 154 (71) | 0.48 |
| Dyslipidemia, n (%) | 302 (69) | 156 (71) | 146 (67) | 0.41 |
| Coronary heart diseases, n (%) | 64 (15) | 30 (14) | 34 (10) | 0.54 |
| Stroke, n (%) | 36 (9) | 13 (6) | 23 (11) | 0.07 |
| Life habits | ||||
| Regular walking, n (%) | 173 (40) | 87 (40) | 86 (40) | 0.99 |
| Current or ex-smoker, n (%) | 231 (53) | 128 (58) | 103 (48) | 0.11 |
| Current or ex-drinker, n (%) | 195 (45) | 105 (48) | 90 (42) | 0.52 |
| Blood measurements | ||||
| Albumin, g/dL | 4.3 (4.0, 4.4) | 4.3 (4.1, 4.5) | 4.2 (4.0, 4.4) | <0.01 |
| AST, U/L | 21 (17, 28) | 21 (18, 28) | 21 (17, 28) | 0.41 |
| ALT, U/L | 19 (14, 29) | 20 (14, 32) | 18 (13, 27) | <0.01 |
| γGT, U/L | 24 (17, 40) | 25 (18, 44) | 23 (16, 38) | 0.11 |
| Fasting plasma Glucose, mg/dL | 132 (118, 153) | 131 (116, 150) | 134 (121, 157) | <0.05 |
| HbA1c, % | 6.9 (6.4, 7.5) | 6.8 (6.4, 7.4) | 7.0 (6.5, 7.5) | 0.17 |
| LDL cholesterol, mg/dL | 101 (82, 118) | 104 (84, 125) | 99 (81, 116) | <0.05 |
| HDL cholesterol, mg/dL | 54 (46, 64) | 54 (47, 64) | 53 (44, 63) | 0.09 |
| Triglycerides, mg/dL | 103 (73, 153) | 107 (70, 162) | 101 (74, 143) | 0.34 |
| Creatinine, mg/dl | 0.82 (0.69, 0.99) | 0.79 (0.68, 0.97) | 0.88 (0.73, 1.02) | <0.01 |
| eGFR, ml/min/1.73 m² | 64.3 ± 18.6 | 67.9 ± 18.7 | 60.6 ± 17.7 | <0.01 |
| Medications | ||||
| Sulfonylurea, n (%) | 43 (10) | 19 (9) | 24 (11) | 0.39 |
| Insulin, n (%) | 125 (29) | 60 (27) | 65 (30) | 0.52 |
| Biguanide, n (%) | 224 (51) | 103 (48) | 121 (55) | 0.13 |
| Glinide, n (%) | 113 (26) | 58 (27) | 55 (25) | 0.66 |
| Pioglitazone, n (%) | 138 (32) | 66 (30) | 72 (33) | 0.63 |
| α-Glucosidase Inhibitor, n (%) | 87 (20) | 47 (22) | 40 (18) | 0.35 |
| Dipeptidyl peptidase-4 inhibitors, n (%) | 271 (62) | 141 (65) | 130 (59) | 0.19 |
| Glucagon-like peptide 1 receptor agonist, n (%) | 33 (8) | 14 (7) | 19 (9) | 0.40 |
| Sodium–glucose cotransporter (SGLT) inhibitors, n (%) | 95 (22) | 44 (20) | 51 (23) | 0.48 |
| Variables | Unadjusted Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Age, years | 1.08 (1.06–1.11) | <0.01 |
| Male, yes or no | 1.04 (0.72–1.52) | 0.83 |
| Anthropometry | ||
| Systolic blood pressure, mmHg | 1.01 (0.99–1.02) | 0.38 |
| Diastolic blood pressure, mmHg | 0.98 (0.96–1.00) | <0.05 |
| Body weight, kg | 0.98 (0.97–0.99) | <0.01 |
| BMI, kg/m2 | 0.96 (0.93–0.99) | <0.05 |
| Waist, cm | 0.99 (0.98–1.00) | 0.09 |
| Fat mass, kg | 0.98 (0.97–1.00) | <0.05 |
| Fat ratio, % | 0.99 (0.98–1.01) | 0.50 |
| Hand grip strength, kg | 0.97 (0.95–0.99) | <0.01 |
| Walking speed, m/sec | 0.16 (0.08–0.31) | <0.01 |
| Muscle mass, kg | 0.95 (0.93–0.98) | <0.01 |
| Skeletal muscle index, kg/m2 | 0.73 (0.61–0.86) | <0.01 |
| Sarcopenia, yes or no | 3.63 (1.68–7.87) | <0.01 |
| Comorbidities | ||
| Duration of diabetes mellitus, years | 1.05 (1.03–1.07) | <0.01 |
| Hypertension, yes or no | 1.16 (0.77–1.74) | 0.48 |
| Dyslipidemia, yes or no | 0.84 (0.56–1.27) | 0.41 |
| Coronary heart diseases, n (%) | 1.18 (0.70–2.01) | 0.54 |
| Stroke, n (%) | 1.90 (0.94–3.85) | 0.08 |
| Life habits | ||
| Regular walking, yes or no | 1.00 (0.68–1.46) | 0.99 |
| Current or ex-smoker, yes or no | 0.85 (0.69–1.04) | 0.11 |
| Current or ex-drinker, yes or no | 0.92 (0.71–1.19) | 0.52 |
| Blood measurements | ||
| Albumin, g/dL | 0.37 (0.21–0.66) | <0.01 |
| AST, U/L | 0.99 (0.98–1.01) | 0.32 |
| ALT, U/L | 0.98 (0.97–1.00) | <0.01 |
| γGT, U/L | 1.00 (1.00 - 1.00) | 0.58 |
| Fasting plasma Glucose, mg/dL | 1.00 (1.00–1.01) | 0.15 |
| HbA1c, % | 1.09 (0.90–1.21) | 0.39 |
| LDLcholesterol, mg/dL | 0.99 (0.99–1.00) | <0.05 |
| HDL cholesterol, mg/dL | 0.99 (0.97–1.00) | 0.09 |
| Triglycerides, mg/dL | 1.00 (1.00–1.00) | 0.74 |
| Creatinine, mg/dl | 1.21 (0.82–1.79) | 0.34 |
| eGFR, ml/min/1.73 m2 | 0.98 (0.97–0.99) | <0.01 |
| Medications | ||
| Sulfonylurea, yes or no | 1.32 (0.70–2.49) | 0.39 |
| Insulin, yes or no | 1.15 (0.76–1.74) | 0.52 |
| Biguanide, yes or no | 0.75 (0.51–1.09) | 0.13 |
| Glinide, yes or no | 1.10 (0.72–1.69) | 0.66 |
| Pioglitazone, yes or no | 0.91 (0.60–1.35) | 0.63 |
| α-Glucosidase Inhibitor, yes or no | 1.25 (0.78–2.00) | 0.35 |
| Dipeptidyl peptidase-4 inhibitors, yes or no | 1.30 (0.88–1.91) | 0.19 |
| Glucagon-like peptide 1 receptor agonist, yes or no | 0.73 (0.36–1.50) | 0.40 |
| Sodium–glucose cotransporter (SGLT) inhibitors, yes or no | 0.85 (0.54–1.34) | 0.48 |
| Model 1 (Unadjusted) | p | Model 2 | p | Model 3 | p | Model 4 | p | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |||||||||
| Overall | ||||||||||||
| Hand grip strength, kg | 0.97 (0.95–0.99) | <0.01 | 0.99 (0.96–1.02) | 0.49 | 0.99 (0.96–1.02) | 0.46 | 0.99 (0.96–1.02) | 0.52 | ||||
| Walking Speed, m/sec | 0.16 (0.08–0.31) | <0.01 | 0.34 (0.16–0.72) | <0.01 | 0.35 (0.16–0.75) | <0.01 | 0.36 (0.17–0.79) | <0.05 | ||||
| Skeletal muscle index, kg/m² | 0.73 (0.61–0.86) | <0.01 | 0.76 (0.52–1.11) | 0.15 | 0.78 (0.52–1.15) | 0.20 | 0.80 (0.54–1.19) | 0.26 | ||||
| Sarcopenia yes or no | 3.63 (1.68–7.87) | <0.01 | 1.51 (0.65–3.47) | 0.34 | 1.46 (0.62–3.43) | 0.39 | 1.39 (0.59–3.28) | 0.45 | ||||
| Age < 60 yearls old | ||||||||||||
| Hand grip strength, kg | 0.99 (0.95–1.03) | 0.54 | 0.94 (0.88–1.00) | 0.07 | 0.93 (0.87–1.00) | 0.06 | 0.94 (0.87–1.01) | 0.08 | ||||
| Walking Speed, m/sec | 0.63 (0.13–3.02) | 0.56 | 0.67 (0.13–3.56) | 0.64 | 0.69 (0.12–4.12) | 0.68 | 0.78 (0.13–4.87) | 0.79 | ||||
| Skeletal muscle index, kg/m² | 1.00 (0.68–1.49) | 0.98 | 0.45 (0.18–1.15) | 0.1 | 0.40 (0.14–1.10) | 0.08 | 0.49 (0.17–1.41) | 0.19 | ||||
| Sarcopenia yes or no | - | - | - | - | - | - | - | - | ||||
| Age ≥ 60 yearls old | ||||||||||||
| Hand grip strength, kg | 0.98 (0.96–1.00) | <0.05 | 1.01 (0.97–1.04) | 0.76 | 1.01 (0.97–1.04) | 0.79 | 1.01 (0.97–1.04) | 0.75 | ||||
| Walking Speed, m/sec | 0.16 (0.08–0.35) | <0.01 | 0.31 (0.13–0.74) | <0.01 | 0.31 (0.13–0.76) | <0.05 | 0.32 (0.13–0.78) | <0.05 | ||||
| Skeletal muscle index, kg/m² | 0.83 (0.67–1.02) | 0.08 | 0.89 (0.58–1.34) | 0.57 | 0.91 (0.59–1.42) | 0.68 | 0.93 (0.60–1.45) | 0.75 | ||||
| Sarcopenia yes or no | 3.26 (1.38–7.68) | <0.01 | 1.49 (0.59–3.77) | 0.4 | 1.41 (0.55–3.65) | 0.47 | 1.37 (0.53–3.56) | 0.51 | ||||
| Men | ||||||||||||
| Hand grip strength, kg | 0.95 (0.92–0.98) | <0.01 | 0.99 (0.96–1.02) | 0.44 | 0.99 (0.95–1.02) | 0.44 | 0.99 (0.96–1.02) | 0.53 | ||||
| Walking Speed, m/sec | 0.13 (0.05–0.32) | <0.01 | 0.26 (0.10–0.69) | <0.01 | 0.25 (0.09–0.69) | <0.01 | 0.27 (0.10–0.75) | 0.01 | ||||
| Skeletal muscle index, kg/m² | 0.68 (0.51–0.89) | <0.01 | 0.73 (0.45–1.18) | 0.2 | 0.71 (0.43–1.18) | 0.19 | 0.75 (0.45–1.26) | 0.28 | ||||
| Sarcopenia yes or no | 1.73 (0.61–4.91) | 0.31 | 0.72 (0.24–2.19) | 0.56 | 0.73 (0.23–2.29) | 0.59 | 0.66 (0.21–2.13) | 0.49 | ||||
| Women | ||||||||||||
| Hand grip strength, kg | 0.92 (0.88–0.97) | <0.01 | 0.99 (0.94–1.05) | 0.75 | 0.98 (0.93–1.04) | 0.52 | 0.98 (0.93–1.04) | 0.55 | ||||
| Walking Speed, m/sec | 0.18 (0.07–0.50) | <0.01 | 0.49 (0.15–1.63) | 0.25 | 0.47 (0.13–1.71) | 0.25 | 0.47 (0.13–1.79) | 0.27 | ||||
| Skeletal muscle index, kg/m² | 0.63 (0.47–0.84) | <0.01 | 0.82 (0.44–1.52) | 0.52 | 0.81 (0.42–1.59) | 0.55 | 0.83 (0.42–1.63) | 0.58 | ||||
| Sarcopenia yes or no | 8.00 (2.28–28.0) | <0.01 | 3.51 (0.90–13.7) | 0.07 | 4.33 (0.99–19.0) | 0.05 | 4.29 (0.97–19.0) | 0.06 | ||||
| BMI < 25 | ||||||||||||
| Hand grip strength, kg | 0.97 (0.95–1.00) | 0.07 | 1.01 (0.96–1.05) | 0.83 | 1.01 (0.96–1.06) | 0.84 | 1.02 (0.96–1.07) | 0.57 | ||||
| Walking Speed, m/sec | 0.07 (0.02–0.24) | <0.01 | 0.14 (0.04–0.52) | <0.01 | 0.13 (0.03–0.52) | <0.01 | 0.15 (0.04–0.64) | <0.01 | ||||
| Skeletal muscle index, kg/m² | 0.67 (0.48–0.95) | <0.05 | 0.57 (0.31–1.04) | 0.07 | 0.51 (0.27–0.95) | <0.05 | 0.56 (0.29–1.06) | 0.07 | ||||
| Sarcopenia yes or no | 3.51 (1.12–11.1) | <0.05 | 1.64 (0.48–5.58) | 0.43 | 1.91 (0.52–6.98) | 0.33 | 1.77 (0.47–6.59) | 0.4 | ||||
| BMI ≥ 25 | ||||||||||||
| Hand grip strength, kg | 0.97 (0.95–0.99) | <0.01 | 0.98 (0.95–1.02) | 0.28 | 0.98 (0.94–1.01) | 0.22 | 0.98 (0.94–1.01) | 0.21 | ||||
| Walking Speed, m/sec | 0.23 (0.10–0.52) | <0.01 | 0.55 (0.21–1.40) | 0.21 | 0.56 (0.21–1.47) | 0.24 | 0.56 (0.21–1.48) | 0.24 | ||||
| Skeletal muscle index, kg/m² | 0.75 (0.60–0.95) | <0.05 | 0.96 (0.57–1.61) | 0.88 | 0.94 (0.54–1.63) | 0.81 | 0.93 (0.53–1.63) | 0.81 | ||||
| Sarcopenia yes or no | 3.55 (1.24–10.2) | <0.05 | 1.36 (0.43–4.33) | 0.61 | 1.35 (0.41–4.41) | 0.62 | 1.35 (0.40–4.47) | 0.63 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machii, N.; Kudo, A.; Saito, H.; Tanabe, H.; Iwasaki, M.; Hirai, H.; Masuzaki, H.; Shimabukuro, M. Walking Speed is the Sole Determinant Criterion of Sarcopenia of Mild Cognitive Impairment in Japanese Elderly Patients with Type 2 Diabetes Mellitus. J. Clin. Med. 2020, 9, 2133. https://doi.org/10.3390/jcm9072133
Machii N, Kudo A, Saito H, Tanabe H, Iwasaki M, Hirai H, Masuzaki H, Shimabukuro M. Walking Speed is the Sole Determinant Criterion of Sarcopenia of Mild Cognitive Impairment in Japanese Elderly Patients with Type 2 Diabetes Mellitus. Journal of Clinical Medicine. 2020; 9(7):2133. https://doi.org/10.3390/jcm9072133
Chicago/Turabian StyleMachii, Noritaka, Akihiro Kudo, Haruka Saito, Hayato Tanabe, Mariko Iwasaki, Hiroyuki Hirai, Hiroaki Masuzaki, and Michio Shimabukuro. 2020. "Walking Speed is the Sole Determinant Criterion of Sarcopenia of Mild Cognitive Impairment in Japanese Elderly Patients with Type 2 Diabetes Mellitus" Journal of Clinical Medicine 9, no. 7: 2133. https://doi.org/10.3390/jcm9072133
APA StyleMachii, N., Kudo, A., Saito, H., Tanabe, H., Iwasaki, M., Hirai, H., Masuzaki, H., & Shimabukuro, M. (2020). Walking Speed is the Sole Determinant Criterion of Sarcopenia of Mild Cognitive Impairment in Japanese Elderly Patients with Type 2 Diabetes Mellitus. Journal of Clinical Medicine, 9(7), 2133. https://doi.org/10.3390/jcm9072133