Is Heel Height Associated with Pain Exacerbations in Hip Osteoarthritis Patients?—Results from a Case-Crossover Study

 ,
,
Abstract
1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Study Population
2.3. Data Collection
2.4. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pereira, D.; Peleteiro, B.; Araujo, J.; Branco, J.; Santos, R.A.; Ramos, E. The effect of osteoarthritis definition on prevalence and incidence estimates: A systematic review. Osteoarthr. Cartil. 2011, 19, 1270–1285. [Google Scholar] [CrossRef]
- Zhang, Y.; Jordan, J.M. Epidemiology of osteoarthritis. Clin. Geriatr. Med. 2010, 26, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Neogi, T. The epidemiology and impact of pain in osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1145–1153. [Google Scholar] [CrossRef] [PubMed]
- Trouvin, A.-P.; Marty, M.; Goupille, P.; Perrot, S. Determinants of daily pain trajectories and relationship with pain acceptability in hip and knee osteoarthritis. A national prospective cohort study on 886 patients. Joint Bone Spine 2019, 86, 245–250. [Google Scholar] [CrossRef]
- O’Neill, T.W.; Felson, D.T. Mechanisms of osteoarthritis (oa) pain. Curr. Osteoporos. Rep. 2018, 16, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Trouvin, A.P.; Perrot, S. Pain in osteoarthritis. Implications for optimal management. Joint Bone Spine 2018, 85, 429–434. [Google Scholar] [CrossRef]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Bennell, K. Physiotherapy management of hip osteoarthritis. J. Physiother. 2013, 59, 145–157. [Google Scholar] [CrossRef]
- Sinclair, J.; Brooks, D.; Butters, B. Effects of different heel heights on lower extremity joint loading in experienced and in-experienced users: A musculoskeletal simulation analysis. Sport Sci. Health 2019, 15, 237–248. [Google Scholar] [CrossRef]
- Birmingham, T.B.; Marriott, K.A.; Leitch, K.M.; Moyer, R.F.; Lorbergs, A.L.; Walton, D.M.; Willits, K.; Litchfield, R.B.; Getgood, A.; Fowler, P.J.; et al. Association between knee load and pain: Within-patient, between-knees, case-control study in patients with knee osteoarthritis. Arthritis Care Res. (Hoboken) 2019, 71, 647–650. [Google Scholar] [CrossRef]
- Bierma-Zeinstra, S.M.A.; Koes, B.W. Risk factors and prognostic factors of hip and knee osteoarthritis. Nat. Clin. Pract. Rheumatol. 2007, 3, 78–85. [Google Scholar] [CrossRef]
- Fu, K.; Makovey, J.; Metcalf, B.; Bennell, K.; Zhang, Y.; Asher, R.; Robbins, S.; Deveza, L.; Hunter, D.J. Role of hip injury and giving way in pain exacerbation in hip osteoarthritis: An internet-based case–crossover study. Arthritis Care Res. 2019, 71, 742–747. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, M.L.; Zhang, Y.; Metcalf, B.; Makovey, J.; Bennell, K.L.; March, L.; Hunter, D.J. The influence of weather on the risk of pain exacerbation in patients with knee osteoarthritis—A case-crossover study. Osteoarthr. Cartil. 2016, 24, 2042–2047. [Google Scholar] [CrossRef]
- Zobel, I.; Erfani, T.; Bennell, K.L.; Makovey, J.; Metcalf, B.; Chen, J.S.; March, L.; Zhang, Y.; Eckstein, F.; Hunter, D.J. Relationship of buckling and knee injury to pain exacerbation in knee osteoarthritis: A web-based case-crossover study. Interact. J. Med. Res. 2016, 5, e17. [Google Scholar] [CrossRef] [PubMed]
- Makovey, J.; Metcalf, B.; Zhang, Y.; Chen, J.S.; Bennell, K.; March, L.; Hunter, D.J. Web-based study of risk factors for pain exacerbation in osteoarthritis of the knee (spark-web): Design and rationale. JMIR Res. Protoc. 2015, 4, e80. [Google Scholar] [CrossRef]
- Ricci, J.A.; Stewart, W.F.; Chee, E.; Leotta, C.; Foley, K.; Hochberg, M.C. Pain exacerbation as a major source of lost productive time in us workers with arthritis. Arthritis Rheumatol. 2005, 53, 673–681. [Google Scholar] [CrossRef]
- Fu, K.; Makovey, J.; Metcalf, B.; Bennell, K.L.; Zhang, Y.; Asher, R.; Robbins, S.R.; Deveza, L.A.; Cistulli, P.A.; Hunter, D.J. Sleep quality and fatigue are associated with pain exacerbations of hip osteoarthritis: An internet-based case-crossover study. J. Rheumatol. 2019, 46, 1524–1530. [Google Scholar] [CrossRef]
- Altman, R.; Alarcon, G.; Appelrouth, D.; Bloch, D.; Borenstein, D.; Brandt, K.; Brown, C.; Cooke, T.D.; Daniel, W.; Feldman, D.; et al. The american college of rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheumatol. 1991, 34, 505–514. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef]
- Downie, W.W.; Leatham, P.A.; Rhind, V.M.; Wright, V.; Branco, J.A.; Anderson, J.A. Studies with pain rating scales. Ann. Rheum. Dis. 1978, 37, 378–381. [Google Scholar] [CrossRef]
- Alghadir, A.H.; Anwer, S.; Iqbal, A.; Iqbal, Z.A. Test-retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J. Pain Res. 2018, 11, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Hagedorn, T.J.; Dufour, A.B.; Golightly, Y.M.; Riskowski, J.L.; Hillstrom, H.J.; Casey, V.A.; Hannan, M.T. Factors affecting center of pressure in older adults: The framingham foot study. J. Foot Ankle Res. 2013, 6, 18. [Google Scholar] [CrossRef]
- Dufour, A.B.; Broe, K.E.; Nguyen, U.S.; Gagnon, D.R.; Hillstrom, H.J.; Walker, A.H.; Kivell, E.; Hannan, M.T. Foot pain: Is current or past shoewear a factor? Arthritis Rheumatol. 2009, 61, 1352–1358. [Google Scholar] [CrossRef] [PubMed]
- Zautra, A.J.; Fasman, R.; Parish, B.P.; Davis, M.C. Daily fatigue in women with osteoarthritis, rheumatoid arthritis, and fibromyalgia. Pain 2007, 128, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Snijders, G.F.; van den Ende, C.H.; Fransen, J.; van Riel, P.L.; Stukstette, M.J.; Defoort, K.C.; Arts-Sanders, M.A.; van den Hoogen, F.H.; den Broeder, A.A. Fatigue in knee and hip osteoarthritis: The role of pain and physical function. Rheumatology (Oxford) 2011, 50, 1894–1900. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.; Luna, S. Effect of footwear on joint pain and function in older adults with lower extremity osteoarthritis. J. Geriatr. Phys. Ther. 2018, 41, 85–101. [Google Scholar] [CrossRef]
- Simonsen, E.B.; Svendsen, M.B.; Norreslet, A.; Baldvinsson, H.K.; Heilskov-Hansen, T.; Larsen, P.K.; Alkjaer, T.; Henriksen, M. Walking on high heels changes muscle activity and the dynamics of human walking significantly. J. Appl. Biomech. 2012, 28, 20–28. [Google Scholar] [CrossRef]
- Barkema, D.D.; Derrick, T.R.; Martin, P.E. Heel height affects lower extremity frontal plane joint moments during walking. Gait Posture 2012, 35, 483–488. [Google Scholar] [CrossRef]
- Esenyel, M.; Walsh, K.; Walden, J.G.; Gitter, A. Kinetics of high-heeled gait. J. Am. Podiatr. Med. Assoc. 2003, 93, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Wiedemeijer, M.M.; Otten, E. Effects of high heeled shoes on gait. A review. Gait Posture 2018, 61, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Mika, A.; Oleksy, L.; Mika, P.; Marchewka, A.; Clark, B.C. The effect of walking in high- and low-heeled shoes on erector spinae activity and pelvis kinematics during gait. Am. J. Phys. Med. Rehabil. 2012, 91, 425–434. [Google Scholar] [CrossRef]
- Hurwitz, D.E.; Hulet, C.H.; Andriacchi, T.P.; Rosenberg, A.G.; Galante, J.O. Gait compensations in patients with osteoarthritis of the hip and their relationship to pain and passive hip motion. J. Orthop. Res. 1997, 15, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Hulet, C.; Hurwitz, D.E.; Andriacchi, T.P.; Galante, J.O.; Vielpeau, C. Functional gait adaptations in patients with painful hip. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2000, 86, 581–589. [Google Scholar]
- Baaklini, E.; Angst, M.; Schellenberg, F.; Hitz, M.; Schmid, S.; Tal, A.; Taylor, W.R.; Lorenzetti, S. High-heeled walking decreases lumbar lordosis. Gait Posture 2017, 55, 12–14. [Google Scholar] [CrossRef] [PubMed]
- Cronin, N.J. The effects of high heeled shoes on female gait: A review. J. Electromyogr. Kinesiol. 2014, 24, 258–263. [Google Scholar] [CrossRef]
- Murphy, S.L.; Smith, D.M.; Clauw, D.J.; Alexander, N.B. The impact of momentary pain and fatigue on physical activity in women with osteoarthritis. Arthritis Care Res. 2008, 59, 849–856. [Google Scholar] [CrossRef]
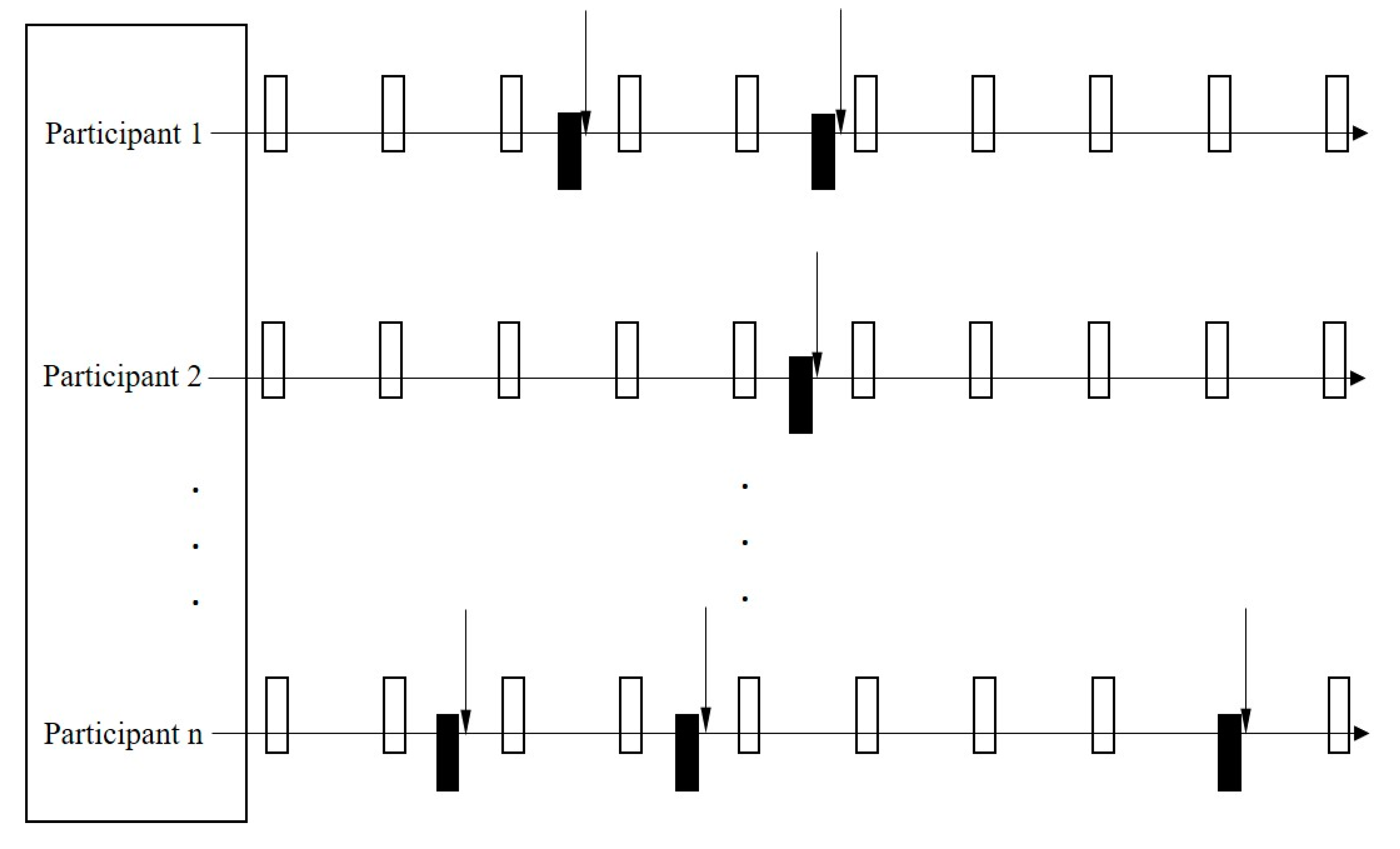
 represents every control period;
represents every control period;  represents every case period;
represents every case period;  represents every pain exacerbation report time point.
represents every control period; represents every case period; represents every pain exacerbation report time point.
represents every pain exacerbation report time point.
represents every control period; represents every case period; represents every pain exacerbation report time point.

{kind=link}
| Characteristics (Mean (SD or %)) | Participants Included (n = 137) | Participants Excluded (n = 115) |
|---|---|---|
| Age (years) | 62.6 (9.8) | 61.8 (8.3) |
| Female, n (%) | 114 (83.2%) | 85 (73.9%) |
| BMI (kg/m2) | 29.0 (6.3) | 28.3 (5.8) |
| Index hip (right) | 74 (54%) | 69 (60%) |
| Race | ||
| Caucasian | 130 (95%) | 112 (97.4%) |
| Others | 7 (5%) | 3 (2.6%) |
| Education level | ||
| Less than high school | 22 (16.1%) | 15 (13%) |
| Completed high school | 28 (20.4%) | 30 (26.1%) |
| Higher than high school | 87 (63.5%) | 70 (60.9%) |
| Occupational physical workload level | ||
| Sedentary (mostly sitting) | 58 (42.3%) | 53 (46.1%) |
| Standing occupation, physically light | 50 (36.5%) | 40 (34.8%) |
| Manual work | 26 (19%) | 21 (18.3%) |
| Heavy manual work | 3 (2.2%) | 1 (0.9%) |
| Kellgren and Lawrence grade | ||
| 2 | 48 (35.0%) | 36 (31.3%) |
| 3 | 79 (57.7%) | 63 (54.8%) |
| 4 | 10 (7.3%) | 16 (13.9%) |
| Baseline pain level (0–10) | ||
| Mildest | 2.5 (2.0) | 2.0 (1.7) |
| Worst * | 8.0 (1.7) | 7.1 (2.0) |
| IPAQ (1–3); median (IQR) | 3 (2) | 3 (2) |
| Heel Height ≥ 2.5 cm | Control Periods | Case Periods | OR (95% CI) | p Values | Adjusted OR (95% CI) * | p Values |
|---|---|---|---|---|---|---|
| No | 798 (84%) | 308 (87%) | 1.0 (Reference) | 0.046 | 1.0 (Reference) | 0.090 |
| Yes | 153 (16%) | 46 (13%) | 0.54 (0.30, 0.99) | 0.59 (0.32, 1.08) |
| Duration of Wear Time | Control Periods | Case Periods | OR (95% CI) | p for Trend | Adjusted OR (95% CI) * | p for Trend |
|---|---|---|---|---|---|---|
| 0 h | 798 (84%) | 308 (87%) | 1.0 (Reference) | 0.003 | 1.0 (Reference) | 0.006 |
| 0–6 h | 52 (6%) | 20 (6%) | 0.94 (0.47, 1.88) | 1.03 (0.50, 2.10) | ||
| >6 h | 101 (10%) | 26 (7%) | 0.28 (0.12, 0.64) | 0.31 (0.13, 0.71) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, K.; Metcalf, B.R.; Bennell, K.L.; Zhang, Y.; Gross, K.D.; Mills, K.; Deveza, L.A.; Robbins, S.R.; Hunter, D.J. Is Heel Height Associated with Pain Exacerbations in Hip Osteoarthritis Patients?—Results from a Case-Crossover Study. J. Clin. Med. 2020, 9, 1872. https://doi.org/10.3390/jcm9061872
Fu K, Metcalf BR, Bennell KL, Zhang Y, Gross KD, Mills K, Deveza LA, Robbins SR, Hunter DJ. Is Heel Height Associated with Pain Exacerbations in Hip Osteoarthritis Patients?—Results from a Case-Crossover Study. Journal of Clinical Medicine. 2020; 9(6):1872. https://doi.org/10.3390/jcm9061872
Chicago/Turabian StyleFu, Kai, Ben R. Metcalf, Kim L. Bennell, Yuqing Zhang, K. Douglas Gross, Kathryn Mills, Leticia A. Deveza, Sarah R. Robbins, and David J. Hunter. 2020. "Is Heel Height Associated with Pain Exacerbations in Hip Osteoarthritis Patients?—Results from a Case-Crossover Study" Journal of Clinical Medicine 9, no. 6: 1872. https://doi.org/10.3390/jcm9061872
APA StyleFu, K., Metcalf, B. R., Bennell, K. L., Zhang, Y., Gross, K. D., Mills, K., Deveza, L. A., Robbins, S. R., & Hunter, D. J. (2020). Is Heel Height Associated with Pain Exacerbations in Hip Osteoarthritis Patients?—Results from a Case-Crossover Study. Journal of Clinical Medicine, 9(6), 1872. https://doi.org/10.3390/jcm9061872