UnReal? Investigating the Sense of Reality and Psychotic Symptoms with Virtual Reality


Abstract
1. Introduction
1.1. Sense of Reality
1.2. A Theoretical Framework of SoR
1.3. Failures of SoR as a Conceptual Framework
1.4. Modeling SoR Using Virtual Reality
1.5. The Present Study: Goals and Predictions
2. Methods
2.1. Participants
2.2. Hardware
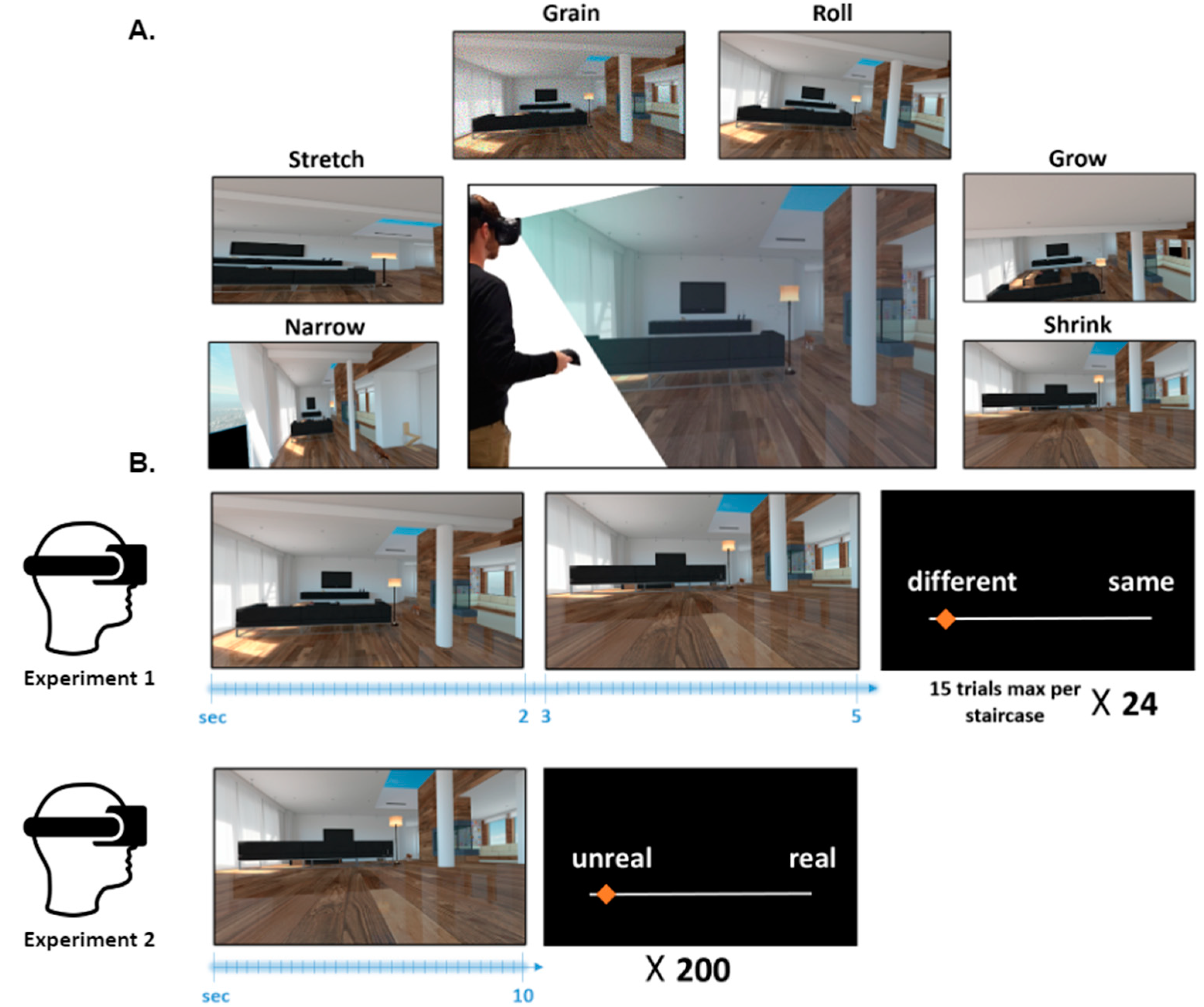
2.3. Experimental Design
2.4. Virtual Environment
2.5. Alterations of Reality
2.6. Experiment 1: Psychophysics of Virtually Altered Reality
2.6.1. Experimental Procedure
2.6.2. Questionnaires
2.7. Experiment 2: Subjective Assessment of Virtually Altered Reality
Experimental Procedure
2.8. Data Analysis
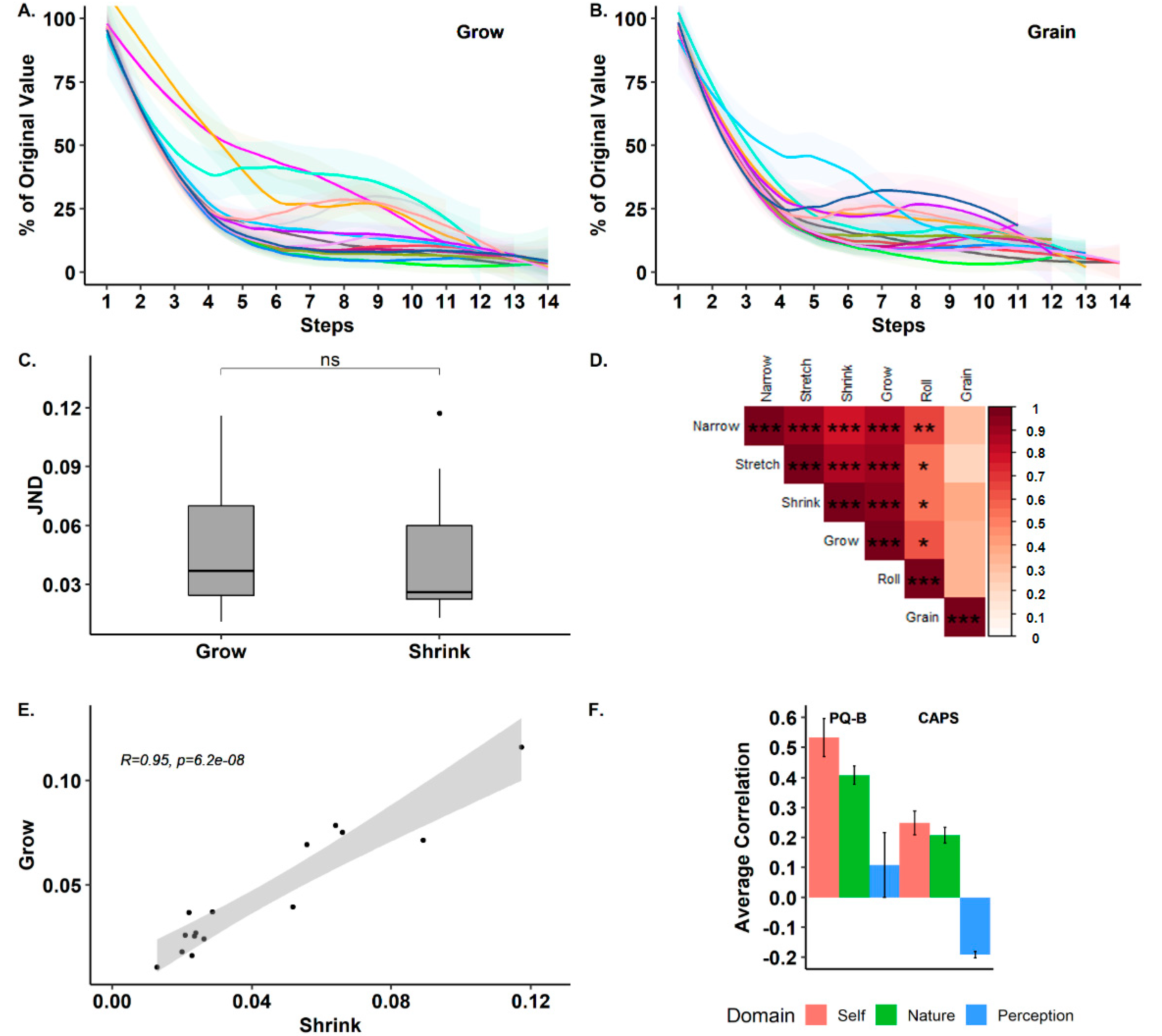
2.8.1. Experiment 1
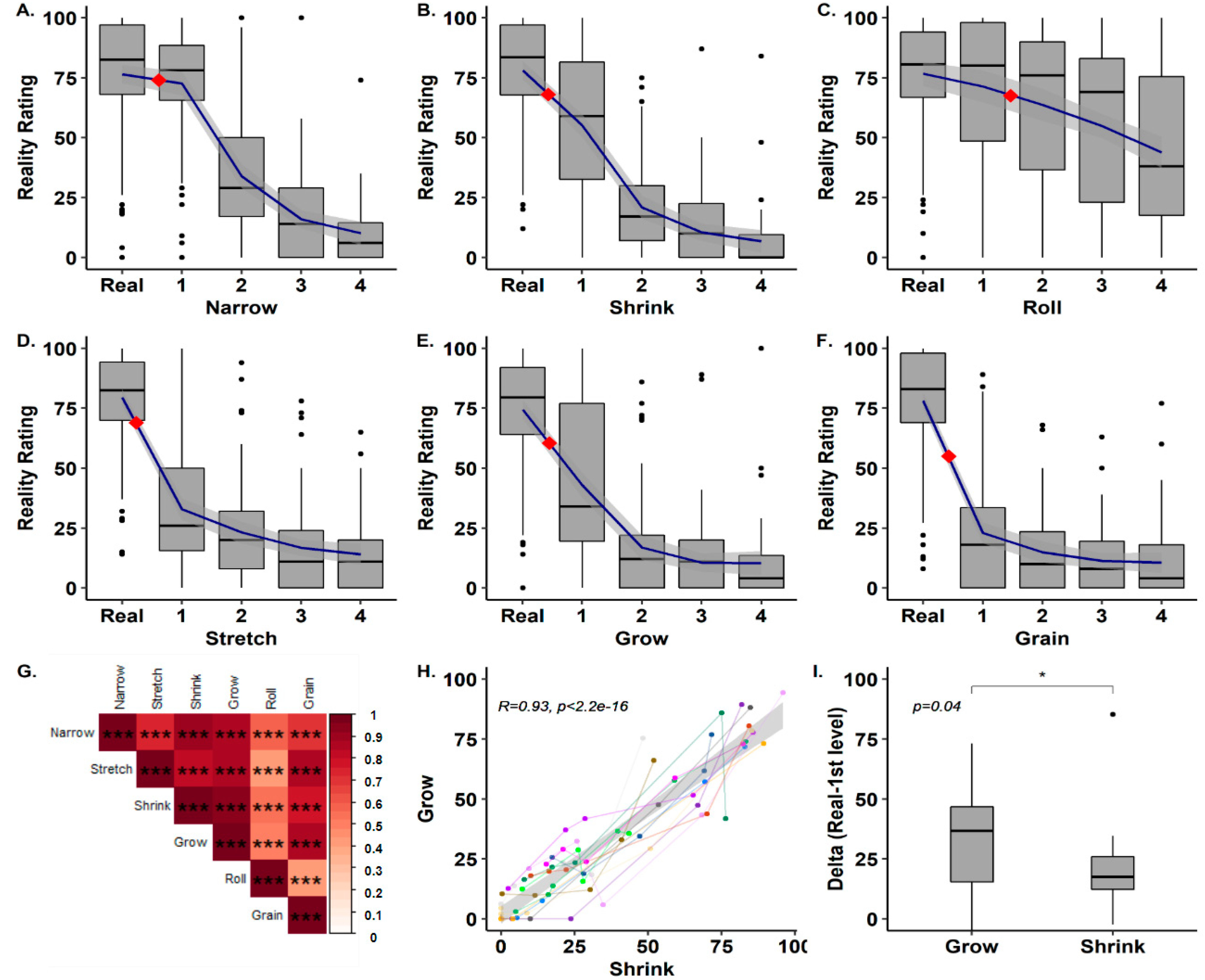
2.8.2. Experiment 2
3. Results
3.1. Experiment 1
3.2. Experiment 2 (Subjective Reality Rating)
4. Discussion
4.1. The Psychophysics of SoR
4.2. Subjective Modulation of SoR
4.3. Limitations
4.4. Summary
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Metzinger, T. How does the brain encode epistemic reliability? Perceptual presence, phenomenal transparency, and counterfactual richness. Cogn. Neurosci. 2014, 5, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Ratcliffe, M. Feelings of Being: Phenomenology, Psychiatry and the Sense of Reality; Oxford University Press: Oxford, UK, 2008; ISBN 0-19-920646-5. [Google Scholar]
- APA. DSM 5; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Barnes, J.; Boubert, L.; Harris, J.; Lee, A.; David, A.S. Reality monitoring and visual hallucinations in Parkinson’s disease. Neuropsychologia 2003, 41, 565–574. [Google Scholar] [CrossRef]
- Bentall, R.P.; Baker, G.A.; Havers, S. Reality monitoring and psychotic hallucinations. Br. J. Clin. Psychol. 1991, 30, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.K. Reality monitoring: An experimental phenomenological approach. J. Exp. Psychol. Gen. 1988, 117, 390. [Google Scholar] [CrossRef]
- Johnson, M.K.; Hashtroudi, S.; Lindsay, D.S. Source monitoring. Psychol. Bull. 1993, 114, 3. [Google Scholar] [CrossRef]
- Raye, C.L.; Johnson, M.K. Reality monitoring vs. discriminating between external sources of memories. Bull. Psychon. Soc. 1980, 15, 405–408. [Google Scholar] [CrossRef]
- Garrison, J.R.; Bond, R.; Gibbard, E.; Johnson, M.K.; Simons, J.S. Monitoring what is real: The effects of modality and action on accuracy and type of reality monitoring error. Cortex 2017, 87, 108–117. [Google Scholar] [CrossRef]
- Simons, J.S.; Garrison, J.R.; Johnson, M.K. Brain Mechanisms of Reality Monitoring. Trends Cogn. Sci. 2017, 21, 462–473. [Google Scholar] [CrossRef]
- Ohayon, M.M. Prevalence of hallucinations and their pathological associations in the general population. Psychiatry Res. 2000, 97, 153–164. [Google Scholar] [CrossRef]
- Blanke, O.; Pozeg, P.; Hara, M.; Heydrich, L.; Serino, A.; Yamamoto, A.; Higuchi, T.; Salomon, R.; Seeck, M.; Landis, T.; et al. Neurological and robot-controlled induction of an apparition. Curr. Biol. 2014, 24, 2681–2686. [Google Scholar] [CrossRef]
- Rao, R.P.N.; Ballard, D.H. Predictive coding in the visual cortex: A functional interpretation of some extra-classical receptive-field effects. Nat. Neurosci. 1999, 2, 79. [Google Scholar] [CrossRef] [PubMed]
- Clark, A. Whatever next? Predictive brains, situated agents, and the future of cognitive science. Behav. Brain Sci. 2013, 36, 181–204. [Google Scholar] [CrossRef] [PubMed]
- Friston, K. The free-energy principle: A rough guide to the brain? Trends Cogn. Sci. (Regul. Ed.) 2009, 13, 293–301. [Google Scholar] [CrossRef] [PubMed]
- de Lange, F.P.; Heilbron, M.; Kok, P. How do expectations shape perception? Trends Cogn. Sci. 2018, 22, 764–779. [Google Scholar] [CrossRef] [PubMed]
- Friston, K.J.; Stephan, K.E. Free-energy and the brain. Synthese 2007, 159, 417–458. [Google Scholar] [CrossRef]
- Wiese, W.; Metzinger, T.K. Vanilla PP for Philosophers: A Primer on Predictive Processing; Philosophy and Predictive Processing; MIND Group: Frankfurt am Main, Germany, 2017; ISBN 978-3-95857-302-4. [Google Scholar]
- Lau, H. Consciousness, Metacognition, & Perceptual Reality Monitoring. PsyArXiv 2019. [Google Scholar] [CrossRef]
- Fletcher, P.C.; Frith, C.D. Perceiving is believing: A Bayesian approach to explaining the positive symptoms of schizophrenia. Nat. Rev. Neurosci. 2008, 10, 48–58. [Google Scholar] [CrossRef]
- Corlett, P.R.; Horga, G.; Fletcher, P.C.; Alderson-Day, B.; Schmack, K.; Powers, A.R. Hallucinations and Strong Priors. Trends Cogn. Sci. 2019, 23, 114–127. [Google Scholar] [CrossRef]
- Sterzer, P.; Adams, R.A.; Fletcher, P.; Frith, C.; Lawrie, S.M.; Muckli, L.; Petrovic, P.; Uhlhaas, P.; Voss, M.; Corlett, P.R. The Predictive Coding Account of Psychosis. Biol. Psychiatry 2018, 84, 634–643. [Google Scholar] [CrossRef]
- Powers, A.R.; Mathys, C.; Corlett, P.R. Pavlovian conditioning–induced hallucinations result from overweighting of perceptual priors. Science 2017, 357, 596–600. [Google Scholar] [CrossRef]
- Griffin, J.D.; Fletcher, P.C. Predictive Processing, Source Monitoring, and Psychosis. Annu. Rev. Clin. Psychol. 2017, 13, 265–289. [Google Scholar] [CrossRef]
- Frith, C.; Done, D. Experiences of alien control in schizophrenia reflect a disorder in the central monitoring of action. Psychol. Med. 2009, 19, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Ford, J.M.; Palzes, V.A.; Roach, B.J.; Mathalon, D.H. Did I do that? Abnormal predictive processes in schizophrenia when button pressing to deliver a tone. Schizophr. Bull. 2014, 40, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Salomon, R.; Progin, P.; Griffa, A.; Rognini, G.; Do, K.Q.; Conus, P.; Marchesotti, S.; Bernasconi, F.; Hagmann, P.; Serino, A. Sensorimotor Induction of Auditory Misattribution in Early Psychosis. Schizophr. Bull. 2020. [Google Scholar] [CrossRef] [PubMed]
- Teunisse, R.J.; Zitman, F.G.; Cruysberg, J.R.M.; Hoefnagels, W.H.L.; Verbeek, A.L.M. Visual hallucinations in psychologically normal people: Charles Bonnet’s syndrome. Lancet 1996, 347, 794–797. [Google Scholar] [CrossRef]
- Perivoliotis, D.; Grant, P.M.; Peters, E.R.; Ison, R.; Kuipers, E.; Beck, A.T. Cognitive insight predicts favorable outcome in cognitive behavioral therapy for psychosis. Psychosis 2010, 2, 23–33. [Google Scholar] [CrossRef]
- Gerretsen, P.; Menon, M.; Mamo, D.C.; Fervaha, G.; Remington, G.; Pollock, B.G.; Graff-Guerrero, A. Impaired insight into illness and cognitive insight in schizophrenia spectrum disorders: Resting state functional connectivity. Schizophr. Res. 2014, 160, 43–50. [Google Scholar] [CrossRef]
- Nair, A.; Palmer, E.C.; Aleman, A.; David, A.S. Relationship between cognition, clinical and cognitive insight in psychotic disorders: A review and meta-analysis. Schizophr. Res. 2014, 152, 191–200. [Google Scholar] [CrossRef]
- Baker, D.; Hunter, E.; Lawrence, E.; Medford, N.; Patel, M.; Senior, C.; Sierra, M.; Lambert, M.V.; Phillips, M.L.; David, A.S. Depersonalisation disorder: Clinical features of 204 cases. Br. J. Psychiatry 2003, 182, 428–433. [Google Scholar] [CrossRef]
- Sass, L.; Pienkos, E.; Nelson, B.; Medford, N. Anomalous self-experience in depersonalization and schizophrenia: A comparative investigation. Conscious. Cogn. 2013, 22, 430–441. [Google Scholar] [CrossRef]
- Harris, C.S. Adaptation to displaced vision: Visual, motor, or proprioceptive change? Science 1963, 140, 812–813. [Google Scholar] [CrossRef]
- Mudrik, L.; Breska, A.; Lamy, D.; Deouell, L.Y. Integration without awareness. Psychol. Sci. 2011, 22, 764. [Google Scholar] [CrossRef]
- Bohil, C.J.; Alicea, B.; Biocca, F.A. Virtual reality in neuroscience research and therapy. Nat. Rev. Neurosci. 2011, 12, 752–762. [Google Scholar] [CrossRef]
- Sanchez-Vives, M.V.; Slater, M. From presence to consciousness through virtual reality. Nat. Rev. Neurosci. 2005, 6, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Krugwasser, A.R.; Harel, E.V.; Salomon, R. The boundaries of the self: The sense of agency across different sensorimotor aspects. J. Vis. 2019, 19, 14. [Google Scholar] [CrossRef] [PubMed]
- Salomon, R.; Fernandez, N.; van Elk, M.; Vachicouras, N.; Sabatier, F.; Tychinskaya, A.; Llobera, J.; Blanke, O. Changing motor perception by sensorimotor conflicts and body ownership. Sci. Rep. 2016, 6, 25847. [Google Scholar] [CrossRef] [PubMed]
- Blom, J.D. Alice in Wonderland syndrome. Neurol. Clin. Pract. 2016, 6, 259–270. [Google Scholar] [CrossRef]
- Bentall, R. The Illusion of Reality: A Review and Integration of Psychological Research on Hallucinations. Psychol. Bull. 1990, 107, 82–95. [Google Scholar] [CrossRef]
- Preller, K.H.; Vollenweider, F.X. Phenomenology, Structure, and Dynamic of Psychedelic States. In Behavioral Neurobiology of Psychedelic Drugs; Halberstadt, A.L., Vollenweider, F.X., Nichols, D.E., Eds.; Current Topics in Behavioral Neurosciences; Springer: Berlin/Heidelberg, Germany, 2018; pp. 221–256. ISBN 978-3-662-55880-5. [Google Scholar]
- Blanke, O.; Metzinger, T. Full-body illusions and minimal phenomenal selfhood. Trends Cogn. Sci. 2009, 13, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Dudley, R.; Aynsworth, C.; Mosimann, U.; Taylor, J.-P.; Smailes, D.; Collerton, D.; McCarthy-Jones, S.; Urwyler, P. A comparison of visual hallucinations across disorders. Psychiatry Res 2019, 272, 86–92. [Google Scholar] [CrossRef]
- Parnas, J. Self and schizophrenia: A phenomenological perspective. Self Neurosci. Psychiatry 2003, 1, 217–241. [Google Scholar]
- Levitt, H. Transformed up-down methods in psychoacoustics. J. Acoust. Soc. Am. 1971, 49, 467–477. [Google Scholar] [CrossRef]
- Hettinger, L.J.; Riccio, G.E. Visually induced motion sickness in virtual environments. Presence: Teleoperators Virtual Environ. 1992, 1, 306–310. [Google Scholar] [CrossRef]
- Bell, V.; Halligan, P.W.; Ellis, H.D. The Cardiff Anomalous Perceptions Scale (CAPS): A new validated measure of anomalous perceptual experience. Schizophr. Bull. 2005, 32, 366–377. [Google Scholar] [CrossRef] [PubMed]
- Bell, V.; Halligan, P.W.; Pugh, K.; Freeman, D. Correlates of perceptual distortions in clinical and non-clinical populations using the Cardiff Anomalous Perceptions Scale (CAPS): Associations with anxiety and depression and a re-validation using a representative population sample. Psychiatry Res. 2011, 189, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Loewy, R.L.; Pearson, R.; Vinogradov, S.; Bearden, C.E.; Cannon, T.D. Psychosis risk screening with the Prodromal Questionnaire—Brief version (PQ-B). Schizophr. Res. 2011, 129, 42–46. [Google Scholar] [CrossRef]
- Kline, E.; Wilson, C.; Ereshefsky, S.; Tsuji, T.; Schiffman, J.; Pitts, S.; Reeves, G. Convergent and discriminant validity of attenuated psychosis screening tools. Schizophr. Res. 2012, 134, 49–53. [Google Scholar] [CrossRef]
- MATLAB. MATLAB 9.6.0.(R2019a); The MathWorks Inc.: Natick, MA, USA, 2019. [Google Scholar]
- JASP Team. JASP (Version 0.11.1) [Computer Software]; Department of Psychological Methods: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Nelson, B.; Thompson, A.; Yung, A.R. Basic Self-Disturbance Predicts Psychosis Onset in the Ultra High Risk for Psychosis “Prodromal” Population. Schizophr. Bull. 2012, 38, 1277–1287. [Google Scholar] [CrossRef]
- Blanke, O.; Mohr, C. Out-of-body experience, heautoscopy, and autoscopic hallucination of neurological origin: Implications for neurocognitive mechanisms of corporeal awareness and self-consciousness. Brain Res. Rev. 2005, 50, 184–199. [Google Scholar] [CrossRef]
- Nelson, B.; Fornito, A.; Harrison, B.J.; Yücel, M.; Sass, L.A.; Yung, A.R.; Thompson, A.; Wood, S.J.; Pantelis, C.; McGorry, P.D. A disturbed sense of self in the psychosis prodrome: Linking phenomenology and neurobiology. Neurosci. Biobehav. Rev. 2009, 33, 807–817. [Google Scholar] [CrossRef]
- Faivre, N.; Vuillaume, L.; Bernasconi, F.; Salomon, R.; Blanke, O.; Cleeremans, A. Sensorimotor conflicts alter metacognitive and action monitoring. Cortex 2020, 124, 224–234. [Google Scholar] [CrossRef]
- Salomon, R.; Noel, J.-P.; Łukowska, M.; Faivre, N.; Metzinger, T.; Serino, A.; Blanke, O. Unconscious integration of multisensory bodily inputs in the peripersonal space shapes bodily self-consciousness. Cognition 2017, 166, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Park, H.-D.; Bernasconi, F.; Bello-Ruiz, J.; Pfeiffer, C.; Salomon, R.; Blanke, O. Transient modulations of neural responses to heartbeats covary with bodily self-consciousness. J. Neurosci. 2016, 36, 8453–8460. [Google Scholar] [CrossRef] [PubMed]
- Perruchoud, D.; Pisotta, I.; Carda, S.; Murray, M.M.; Ionta, S. Biomimetic rehabilitation engineering: The importance of somatosensory feedback for brain–machine interfaces. J. Neural Eng. 2016, 13, 041001. [Google Scholar] [CrossRef] [PubMed]
- Lubianiker, N.; Goldway, N.; Fruchtman-Steinbok, T.; Paret, C.; Keynan, J.N.; Singer, N.; Cohen, A.; Kadosh, K.C.; Linden, D.E.; Hendler, T. Process-based framework for precise neuromodulation. Nat. Hum. Behav. 2019, 3, 436–445. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Reeve, S.; Robinson, A.; Ehlers, A.; Clark, D.; Spanlang, B.; Slater, M. Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol. Med. 2017, 47, 2393–2400. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| JND | ||||||
| Narrow | Stretch | Shrink | Grow | Roll | Grain | |
| Mean | 0.09 | 0.12 | 0.04 | 0.05 | 2.57 | 0.01 |
| Std. Deviation | 0.06 | 0.06 | 0.03 | 0.03 | 2.37 | 0.05 |
| Minimum | 0.04 | 0.07 | 0.01 | 0.01 | 0.31 | 0.03 |
| Maximum | 0.24 | 0.29 | 0.12 | 0.12 | 9.5 | 0.19 |
| Within-Subject Variability | ||||||
| Narrow | Stretch | Shrink | Grow | Roll | Grain | |
| Mean | 0.003 | 0.004 | 0.001 | 8.0e -4 | 0.93 | 0.002 |
| Std. Deviation | 0.003 | 0.009 | 0.002 | 0.002 | 1.05 | 0.003 |
| Minimum | 0 | 0 | 0 | 0 | 0.003 | 0 |
| Maximum | 0.008 | 0.04 | 0.007 | 0.006 | 3.92 | 0.01 |
| Convergence Rate | ||||||
| Narrow | Stretch | Shrink | Grow | Roll | Grain | |
| Mean | 5.99 | 8.73 | 7.03 | 6.57 | 5.74 | 6.76 |
| Std. Deviation | 1.47 | 0.91 | 1.6 | 1.98 | 2.23 | 1.76 |
| Minimum | 3 | 7 | 4 | 3 | 1 | 4 |
| Maximum | 9 | 10 | 9.5 | 9.75 | 10 | 10 |
| Subjective Ratings | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alteration Magnitude | Narrow | Stretch | Shrink | Grow | Roll | Grain | ||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Real | 76.84 | 10.42 | 79.42 | 14.34 | 76.26 | 15.85 | 75 | 13.99 | 76.96 | 12.95 | 78.78 | 12.51 |
| 1 | 72.59 | 12.68 | 32.88 | 14.46 | 55.08 | 19.4 | 42.88 | 18.35 | 71.41 | 17.7 | 22.99 | 16.72 |
| 2 | 33.89 | 16.27 | 23.2 | 13.8 | 20.96 | 10.98 | 16.93 | 13.2 | 63.68 | 25.19 | 14.95 | 13.24 |
| 3 | 17.92 | 11.54 | 16.67 | 12.5 | 14.31 | 11.67 | 13.68 | 12.4 | 55.2 | 28.97 | 11.65 | 10.61 |
| 4 | 9.63 | 8.59 | 14.09 | 9.015 | 5.76 | 7.92 | 9.57 | 8.47 | 43.79 | 24.82 | 10.47 | 12.02 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drori, G.; Bar-Tal, P.; Stern, Y.; Zvilichovsky, Y.; Salomon, R. UnReal? Investigating the Sense of Reality and Psychotic Symptoms with Virtual Reality. J. Clin. Med. 2020, 9, 1627. https://doi.org/10.3390/jcm9061627
Drori G, Bar-Tal P, Stern Y, Zvilichovsky Y, Salomon R. UnReal? Investigating the Sense of Reality and Psychotic Symptoms with Virtual Reality. Journal of Clinical Medicine. 2020; 9(6):1627. https://doi.org/10.3390/jcm9061627
Chicago/Turabian StyleDrori, Gad, Paz Bar-Tal, Yonatan Stern, Yair Zvilichovsky, and Roy Salomon. 2020. "UnReal? Investigating the Sense of Reality and Psychotic Symptoms with Virtual Reality" Journal of Clinical Medicine 9, no. 6: 1627. https://doi.org/10.3390/jcm9061627
APA StyleDrori, G., Bar-Tal, P., Stern, Y., Zvilichovsky, Y., & Salomon, R. (2020). UnReal? Investigating the Sense of Reality and Psychotic Symptoms with Virtual Reality. Journal of Clinical Medicine, 9(6), 1627. https://doi.org/10.3390/jcm9061627