The Spectrum of Interstitial Lung Disease Associated with Autoimmune Diseases: Data of a 3.6-Year Prospective Study from a Referral Center of Interstitial Lung Disease and Lung Transplantation † †

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
2.3. Descriptive Statistical Analysis
3. Results
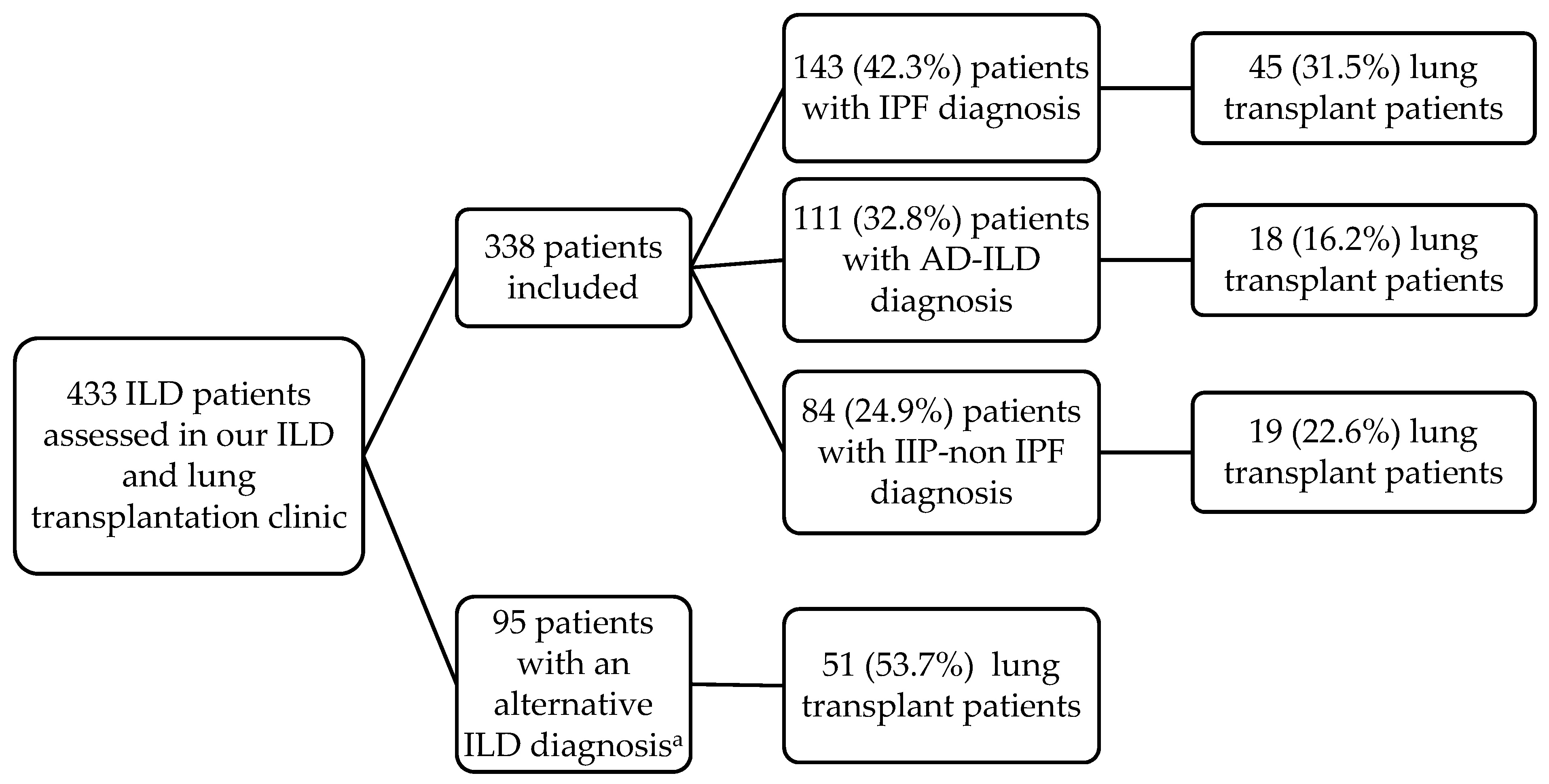
3.1. Characteristics and Categories of ILD Patients According to Their Diagnosis
3.2. Spectrum of AD-ILD Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef]
- Cottin, V.; Hirani, N.A.; Hotchkin, D.L.; Nambiar, A.M.; Ogura, T.; Otaola, M.; Skowasch, D.; Park, J.S.; Poonyagariyagorn, H.K.; Wuyts, W.; et al. Presentation, diagnosis and clinical course of the spectrum of progressive-fibrosing interstitial lung diseases. Eur. Respir. Rev. 2018, 27, 180076. [Google Scholar] [CrossRef]
- Davidson, A.; Diamond, B. Autoimmune diseases. N. Engl. J. Med. 2001, 345, 340–350. [Google Scholar] [CrossRef]
- Goldblatt, F.; O’Neill, S.G. Clinical aspects of autoimmune rheumatic diseases. Lancet 2013, 382, 797–808. [Google Scholar] [CrossRef]
- Sociedad Española de Reumatología. Tratado SER de Diagnóstico y Tratamiento de Enfermedades Autoinmunes Sistémicas, 1st ed.; Elsevier: Madrid, Spain, 2018. [Google Scholar]
- Fischer, A.; du Bois, R. Interstitial lung disease in connective tissue disorders. Lancet 2012, 380, 689–698. [Google Scholar] [CrossRef]
- Mathai, S.C.; Danoff, S.K. Management of interstitial lung disease associated with connective tissue disease. BMJ 2016, 352, h6819. [Google Scholar] [CrossRef] [PubMed]
- Walker, U.A.; Tyndall, A.; Czirják, L.; Denton, C.; Farge-Bancel, D.; Kowal-Bielecka, O.; Müller-Ladner, U.; Bocelli-Tyndall, C.; Matucci-Cerinic, M. Clinical risk assessment of organ manifestations in systemic sclerosis: A report from the EULAR scleroderma trials and research group database. Ann. Rheum. Dis. 2007, 66, 754–763. [Google Scholar] [CrossRef] [PubMed]
- Morisset, J.; Johnson, C.; Rich, E.; Collard, H.R.; Lee, J.S. Management of myositis-related interstitial lung disease. Chest 2016, 150, 1118–1128. [Google Scholar] [CrossRef]
- Marigliano, B.; Soriano, A.; Margiotta, D.; Vadacca, M.; Afeltra, A. Lung involvement in connective tissue diseases: A comprehensive review and a focus on rheumatoid arthritis. Autoimmun. Rev. 2013, 12, 1076–1084. [Google Scholar] [CrossRef]
- Atzeni, F.; Gerardi, M.C.; Barilaro, G.; Masala, I.F.; Benucci, M.; Sarzi-Puttini, P. Interstitial lung disease in systemic autoimmune rheumatic diseases: A comprehensive review. Expert Rev. Clin. Immunol. 2018, 14, 69–82. [Google Scholar] [CrossRef]
- Mittoo, S.; Gelber, A.C.; Christopher-Stine, L.; Horton, M.R.; Lechtzin, N.; Danoff, S.K. Ascertainment of collagen vascular disease in patients presenting with interstitial lung disease. Respir. Med. 2009, 103, 1152–1158. [Google Scholar] [CrossRef] [PubMed]
- Fischer, A.; Antoniou, K.M.; Brown, K.K.; Cadranel, J.; Corte, T.J.; du Bois, R.M.; Lee, J.S.; Leslie, K.O.; Lynch, D.A.; Matteson, E.L.; et al. An official European Respiratory Society/American Thoracic Society research statement: Interstitial pneumonia with autoimmune features. Eur. Respir. J. 2015, 46, 976–987. [Google Scholar] [CrossRef] [PubMed]
- Collins, B.; Raghu, G. Interstitial pneumonia with autoimmune features: The new consensus-based definition for this cohort of patients should be broadened. Eur. Respir. J. 2016, 47, 1293–1295. [Google Scholar] [CrossRef] [PubMed]
- Cavagna, L.; Gonzalez Gay, M.A.; Allanore, Y.; Matucci-Cerinic, M. Interstitial pneumonia with autoimmune features: A new classification still on the move. Eur. Respir. Rev. 2018, 27, 180047. [Google Scholar] [CrossRef] [PubMed]
- Sambataro, G.; Sambataro, D.; Torrisi, S.E.; Vancheri, A.; Pavone, M.; Rosso, R.; Schisano, M.; Crimi, C.; Pignataro, F.; Fischer, A.; et al. State of the art in interstitial pneumonia with autoimmune features: A systematic review on retrospective studies and suggestions for further advances. Eur. Respir. Rev. 2018, 27, 170139. [Google Scholar] [CrossRef]
- Park, J.H.; Kim, D.S.; Park, I.N.; Jang, S.J.; Kitaichi, M.; Nicholson, A.G.; Colby, T.V. Prognosis of fibrotic interstitial pneumonia: Idiopathic versus collagen vascular disease-related subtypes. Am. J. Respir. Crit. Care Med. 2007, 175, 705–711. [Google Scholar] [CrossRef]
- Navaratnam, V.; Ali, N.; Smith, C.J.; McKeever, T.; Fogarty, A.; Hubbard, R.B. Does the presence of connective tissue disease modify survival in patients with pulmonary fibrosis? Respir. Med. 2011, 105, 1925–1930. [Google Scholar] [CrossRef]
- Castelino, F.V.; Goldberg, H.; Dellaripa, P.F. The impact of rheumatological evaluation in the management of patients with interstitial lung disease. Rheumatology 2011, 50, 489–493. [Google Scholar] [CrossRef]
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Colby, T.V.; Cordier, J.F.; Flaherty, K.R.; Lasky, J.A.; et al. An Official ATS/ERS/JRS/ALAT statement: Idiopathic pulmonary fibrosis: Evidence-based guidelines for diagnosis and management. Am. J. Respir. Crit. Care Med. 2011, 183, 788–824. [Google Scholar] [CrossRef]
- Furini, F.; Carnevale, A.; Casoni, G.L.; Guerrini, G.; Cavagna, L.; Govoni, M.; Sciré, C.A. The role of the multidisciplinary evaluation of interstitial lung diseases: Systematic literature review of the current evidence and future perspectives. Front. Med. 2019, 6, 246. [Google Scholar] [CrossRef]
- Mikolasch, T.A.; Garthwaite, H.S.; Porter, J.C. Update in diagnosis and management of interstitial lung disease. Clin. Med. 2017, 17, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Weill, D.; Benden, C.; Corris, P.A.; Dark, J.H.; Davis, R.D.; Keshavjee, S.; Lederer, D.J.; Mulligan, M.J.; Patterson, G.A.; Singer, L.G.; et al. A consensus document for the selection of lung transplant candidates: 2014--an update from the Pulmonary Transplantation Council of the International Society for Heart and Lung Transplantation. J. Heart Lung Transplant. 2015, 34, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O. III.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef] [PubMed]
- van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A., Jr.; Carreira, P.E. 2013 classification criteria for systemic sclerosis: An American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. 2013, 65, 2737–2747. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, M.C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997, 40, 1725. [Google Scholar] [CrossRef]
- Petri, M.; Orbai, A.M.; Alarcón, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.; Wallace, D.J.; Nived, O. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [Google Scholar] [CrossRef]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheumatol. 2017, 69, 35–45. [Google Scholar] [CrossRef]
- Lundberg, I.E.; Tjärnlund, A.; Bottai, M.; Werth, V.P.; Pilkington, C.; Visser, M.; Alfredsson, L.; Amato, A.A.; Barohn, R.J.; Liang, M.H.; et al. 2017 European League Against Rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups. Ann. Rheum. Dis. 2017, 76, 1955–1964. [Google Scholar] [CrossRef]
- Fries, J.F.; Hunder, G.G.; Bloch, D.A.; Michel, B.A.; Arend, W.P.; Calabrese, L.H.; Fauci, A.S.; Leavitt, R.Y.; Lie, J.T.; Lightfoot, R.W., Jr.; et al. The American College of Rheumatology 1990 criteria for the classification of vasculitis. Summary. Arthritis Rheum. 1990, 33, 1135–1136. [Google Scholar] [CrossRef]
- Lynch, D.A.; Sverzellati, N.; Travis, W.D.; Brown, K.K.; Colby, T.V.; Galvin, J.R.; Goldin, J.G.; Hansell, D.M.; Inoue, Y.; Johkoh, T.; et al. Diagnostic criteria for idiopathic pulmonary fibrosis: A Fleischner Society White Paper. Lancet Respir. Med. 2018, 6, 138–153. [Google Scholar] [CrossRef]
- Tirelli, C.; Morandi, V.; Valentini, A.; La Carrubba, C.; Dore, R.; Zanframundo, G.; Morbini, P.; Grignaschi, S.; Franconeri, A.; Oggionni, T.; et al. Multidisciplinary Approach in the Early Detection of Undiagnosed Connective Tissue Diseases in Patients with Interstitial Lung Disease: A Retrospective Cohort Study. Front. Med. 2020, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Skolnik, K.; Ryerson, C.J. Unclassifiable interstitial lung disease: A review. Respirology 2016, 21, 51–56. [Google Scholar] [CrossRef]
- Ortona, E.; Pierdominici, M.; Maselli, A.; Veroni, C.; Aloisi, F.; Shoenfeld, Y. Sex-based differences in autoimmune diseases. Ann. Ist. Super. Sanita 2016, 52, 205–212. [Google Scholar] [PubMed]
- McInnes, I.B.; Schett, G. The pathogenesis of rheumatoid arthritis. N. Engl. J. Med. 2011, 365, 2205–2219. [Google Scholar] [CrossRef]
- Barnes, J.; Mayes, M.D. Epidemiology of systemic sclerosis: Incidence, prevalence, survival, risk factors, malignancy, and environmental triggers. Curr. Opin. Rheumatol. 2012, 24, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, L.; Nasser, M.; Ahmad, K.; Cottin, V. Interstitial Pneumonia with Autoimmune Features (IPAF). Front. Med. 2019, 6, 209. [Google Scholar] [CrossRef] [PubMed]
- Scirè, C.A.; Gonzalez-Gay, M.A.; Selva-O’Callaghan, A.; Cavagna, L. Clinical spectrum time course of interstitial pneumonia with autoimmune features in patients positive for antisynthetase antibodies. Respir. Med. 2017, 132, 265–266. [Google Scholar] [CrossRef] [PubMed]
- Sebastiani, M.; Cassone, G.; De Pasquale, L.; Cerri, S.; Della Casa, G.; Vacchi, C.; Luppi, F.; Salvarani, C.; Manfredi, A. Interstitial pneumonia with autoimmune features: A single center prospective follow-up study. Autoimmun. Rev. 2020, 19, 102451. [Google Scholar] [CrossRef] [PubMed]
- Ghrairi, N.; Aouadi, S.; Elhechmi, Y.Z.; Ben Saad, S.; Ben, A., I; Yalaoui, S. Antinuclear antibodies in interstitial lung disease: Prevalence and clinical significance. Tunis. Med. 2019, 97, 1240–1245. [Google Scholar]
- Solomon, J.J.; Brown, K.K. Rheumatoid arthritis-associated interstitial lung disease. Open Access Rheumatol. 2012, 4, 21–31. [Google Scholar]
- Klareskog, L.; Stolt, P.; Lundberg, K.; Källberg, H.; Bengtsson, C.; Grunewald, J.; Rönnelid, J.; Harris, H.E.; Ulfgren, A.K.; Rantapää-Dahlqvist, S. A new model for an etiology of rheumatoid arthritis: Smoking may trigger HLA-DR (shared epitope)-restricted immune reactions to autoantigens modified by citrullination. Arthritis Rheum. 2006, 54, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Steen, V.D. Autoantibodies in systemic sclerosis. Semin. Arthritis Rheum. 2005, 35, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Hesselstrand, R.; Scheja, A.; Shen, G.Q.; Wiik, A.; Akesson, A. The association of antinuclear antibodies with organ involvement and survival in systemic sclerosis. Rheumatology 2003, 42, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann-Vold, A.M.; Midtvedt, Ø.; Tennøe, A.H.; Garen, T.; Lund, M.B.; Aaløkken, T.M.; Andreassen, A.K.; Elhage, F.; Brunborg, C.; Taraldsrud, E.; et al. Cardiopulmonary Disease Development in Anti-RNA Polymerase III-positive Systemic Sclerosis: Comparative Analyses from an Unselected, Prospective Patient Cohort. J. Rheumatol. 2017, 44, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Mackintosh, J.A.; Stainer, A.; Barnett, J.L.; Renzoni, E.A. Systemic Sclerosis Associated Interstitial Lung Disease: A Comprehensive Overview. Semin. Respir. Crit. Care Med. 2019, 40, 208–226. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Serrano, J.; Herrera-Bringas, D.; Mejía, M.; Rivero, H.; Mateos-Toledo, H.; Figueroa, J.E. Prognostic factors in a cohort of antisynthetase syndrome (ASS): Serologic profile is associated with mortality in patients with interstitial lung disease (ILD). Clin. Rheumatol. 2015, 34, 1563–1569. [Google Scholar] [CrossRef]
- Bartoloni, E.; Gonzalez-Gay, M.A.; Scirè, C.; Castaneda, S.; Gerli, R.; Lopez-Longo, F.J.; Martinez-Barrio, J.; Govoni, M.; Furini, F.; Pina, T.; et al. Clinical follow-up predictors of disease pattern change in anti-Jo1 positive anti-synthetase syndrome: Results from a multicenter, international and retrospective study. Autoimmun. Rev. 2017, 16, 253–257. [Google Scholar] [CrossRef]
- Cavagna, L.; Trallero-Araguás, E.; Meloni, F.; Cavazzana, I.; Rojas-Serrano, J.; Feist, E.; Zanframundo, G.; Morandi, V.; Meyer, A.; Pereira da Silva, J.A.; et al. Influence of Antisynthetase Antibodies Specificities on Antisynthetase Syndrome Clinical Spectrum Time Course. J. Clin. Med. 2019, 8, 2013. [Google Scholar] [CrossRef]
- Kinder, B.W.; Collard, H.R.; Koth, L.; Daikh, D.I.; Wolters, P.J.; Elicker, B.; Jones, K.D.; King, T.E., Jr. Idiopathic nonspecific interstitial pneumonia: Lung manifestation of undifferentiated connective tissue disease? Am. J. Respir. Crit. Care Med. 2007, 176, 691–697. [Google Scholar] [CrossRef]
- Spagnolo, P.; Lee, J.S.; Sverzellati, N.; Rossi, G.; Cottin, V. The Lung in Rheumatoid Arthritis: Focus on Interstitial Lung Disease. Arthritis Rheumatol. 2018, 70, 1544–1554. [Google Scholar] [CrossRef]
- Chung, J.H.; Cox, C.W.; Montner, S.M.; Adegunsoye, A.; Oldham, J.M.; Husain, A.N.; Vij, R.; Noth, I.; Lynch, D.A.; Strek, M.E. CT Features of the Usual Interstitial Pneumonia Pattern: Differentiating Connective Tissue Disease-Associated Interstitial Lung Disease From Idiopathic Pulmonary Fibrosis. AJR Am. J. Roentgenol. 2018, 210, 307–313. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| ILD Patients, n = 338 | AD-ILD, n = 111 | IPF, n = 143 | IIP-Non IPF, n = 84 | p-Value a | p-Value b | p-Value c | p-Value d | |
|---|---|---|---|---|---|---|---|---|
| Sex (women/men), n (%) | 108/230 (32.0/68.0) | 53/58 (47.7/52.3) | 24/119 (16.8/83.2) | 31/53 (36.9/63.1) | <0.001 | <0.001 | 0.13 | <0.001 |
| Age at ILD diagnosis, years, median [IQR] | 59 (52–64) | 57 (50–63) | 60 (55–64) | 58 (44–66) | 0.01 | 0.006 | 0.87 | 0.025 |
| Smoking ever, n (%) | 232 (68.6) | 69 (62.2) | 113 (79.0) | 50 (59.5) | 0.002 | 0.003 | 0.71 | 0.002 |
| Pulmonary function tests | ||||||||
| FEV1 (% predicted), mean ± SD | 76.4 ± 22.6 | 79.2 ± 24.7 | 77.5 ± 20.3 | 70.8 ± 22.8 | 0.029 | 0.56 | 0.018 | 0.024 |
| FVC (% predicted), mean ± SD | 77.6 ± 23.0 | 81.8 ± 25.0 | 77.4 ± 19.9 | 72.4 ± 24.3 | 0.018 | 0.12 | 0.009 | 0.09 |
| FEV1/FVC (% predicted), mean ± SD | 78.9 ± 9.6 | 77.9 ± 8.7 | 79.0 ± 9.2 | 80.0 ± 11.2 | 0.33 | 0.35 | 0.15 | 0.47 |
| DLCO (% predicted) mean ± SD | 36.7 ± 15.1 | 38.2 ± 14.7 | 34.9 ± 15.4 | 37.9 ± 14.9 | 0.28 | 0.15 | 0.92 | 0.25 |
| Actual lung transplant received, n (%) | 82 (24.3) | 18 (16.2) | 45 (31.5) | 19 (22.6) | 0.018 | 0.005 | 0.26 | 0.15 |
| Rheumatic autoimmune disease | n (%) |
| Rheumatoid arthritis | 30 (27.0) |
| Systemic sclerosis | 29 (26.1) |
| Interstitial pneumonia with autoimmune features | 20 (18.0) |
| Anti-synthetase syndrome | 19 (17.1) |
| Others a | 13 (11.8) |
| Autoantibody profile b | n/N (%) |
| Rheumatoid factor | 31/79 (39.2) |
| Anti–citrullinated protein antibody | 25/59 (42.4) |
| Antinuclear antibody | 64/90 (71.1) |
| Anti-SSa (Ro) | 17/53 (32.1) |
| Anti-SSb (La) | 4/50 (8.0) |
| Anti-Scl 70 | 15/61 (24.6) |
| Myositis-associated antibodies c | 26/56 (46.4) |
| Others d | 15/67 (22.4) |
| High-resolution computed tomography pattern | n (%) |
| UIP pattern | 41 (37.3) |
| Probable UIP pattern | 16 (14.5) |
| Indeterminate for UIP pattern | 3 (2.7) |
| Features most consistent with an alternative diagnosis | |
| NSIP pattern | 43 (39.1) |
| Non-NSIP pattern | 7 (6.4) |
| RA-ILD n (%) | SSc-ILD n (%) | IPAF n (%) | Anti-Synthetase Syndrome n (%) | |
|---|---|---|---|---|
| UIP pattern | 18 (60.0) | 6 (21.5) | 8 (40.0) | 5 (26.3) |
| Probable UIP pattern | 2 (6.7) | 4 (14.3) | 4 (20.0) | 4 (21.1) |
| Indeterminate for UIP pattern | 1 (3.3) | 2 (7.1) | - | - |
| Features most consistent with an alternative diagnosis | ||||
| NSIP pattern | 8 (26.7) | 14 (50.0) | 5 (25.0) | 10 (52.6) |
| Non-NSIP pattern | 1 (3.3) | 2 (7.1) | 3 (15.0) | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atienza-Mateo, B.; Remuzgo-Martínez, S.; Mora Cuesta, V.M.; Iturbe-Fernández, D.; Fernández-Rozas, S.; Prieto-Peña, D.; Calderón-Goercke, M.; Corrales, A.; Blanco Rodríguez, G.; Gómez-Román, J.J.; et al. The Spectrum of Interstitial Lung Disease Associated with Autoimmune Diseases: Data of a 3.6-Year Prospective Study from a Referral Center of Interstitial Lung Disease and Lung Transplantation †. J. Clin. Med. 2020, 9, 1606. https://doi.org/10.3390/jcm9061606
Atienza-Mateo B, Remuzgo-Martínez S, Mora Cuesta VM, Iturbe-Fernández D, Fernández-Rozas S, Prieto-Peña D, Calderón-Goercke M, Corrales A, Blanco Rodríguez G, Gómez-Román JJ, et al. The Spectrum of Interstitial Lung Disease Associated with Autoimmune Diseases: Data of a 3.6-Year Prospective Study from a Referral Center of Interstitial Lung Disease and Lung Transplantation †. Journal of Clinical Medicine. 2020; 9(6):1606. https://doi.org/10.3390/jcm9061606
Chicago/Turabian StyleAtienza-Mateo, Belén, Sara Remuzgo-Martínez, Víctor Manuel Mora Cuesta, David Iturbe-Fernández, Sonia Fernández-Rozas, Diana Prieto-Peña, Mónica Calderón-Goercke, Alfonso Corrales, Gerardo Blanco Rodríguez, José Javier Gómez-Román, and et al. 2020. "The Spectrum of Interstitial Lung Disease Associated with Autoimmune Diseases: Data of a 3.6-Year Prospective Study from a Referral Center of Interstitial Lung Disease and Lung Transplantation †" Journal of Clinical Medicine 9, no. 6: 1606. https://doi.org/10.3390/jcm9061606
APA StyleAtienza-Mateo, B., Remuzgo-Martínez, S., Mora Cuesta, V. M., Iturbe-Fernández, D., Fernández-Rozas, S., Prieto-Peña, D., Calderón-Goercke, M., Corrales, A., Blanco Rodríguez, G., Gómez-Román, J. J., González-Gay, M. Á., & Cifrián, J. M. (2020). The Spectrum of Interstitial Lung Disease Associated with Autoimmune Diseases: Data of a 3.6-Year Prospective Study from a Referral Center of Interstitial Lung Disease and Lung Transplantation †. Journal of Clinical Medicine, 9(6), 1606. https://doi.org/10.3390/jcm9061606