Development of Algorithm for Clinical Management of Sickle Cell Bone Disease: Evidence for a Role of Vertebral Fractures in Patient Follow-up

 ,
,  and
and 
Abstract
1. Introduction
2. Methods
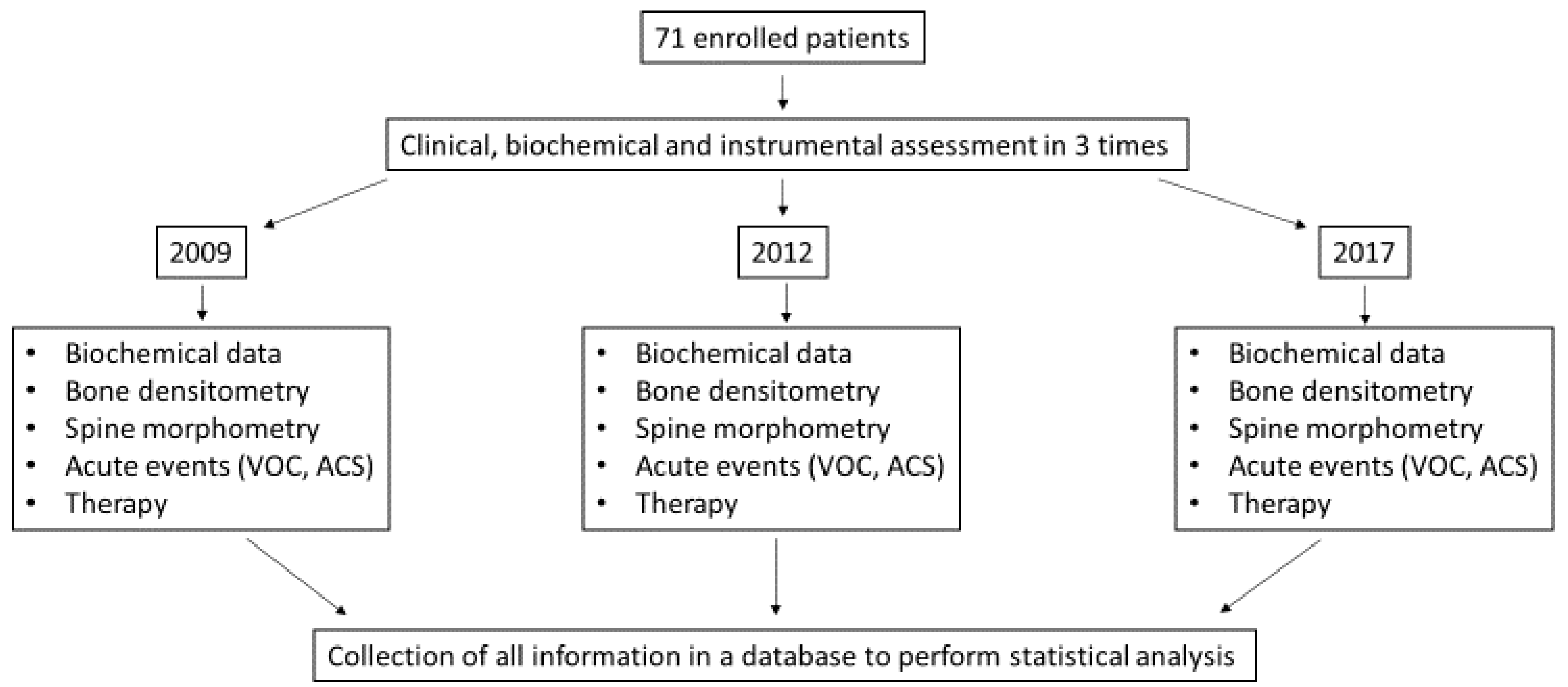
2.1. Patients and Design of the Study
2.2. Clinical and Therapeutic Assessment
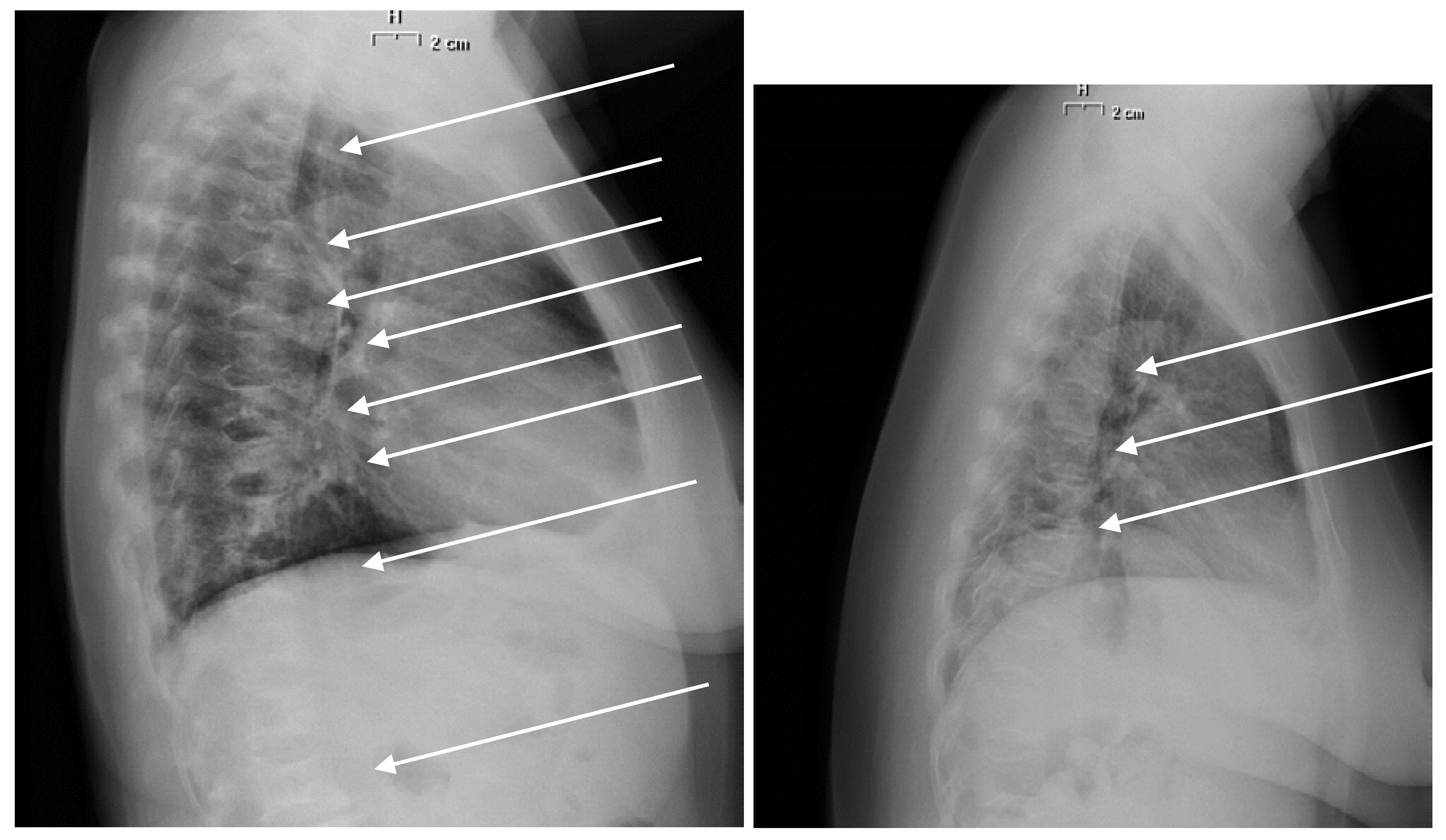
2.3. Biochemical and Radiological Assessment
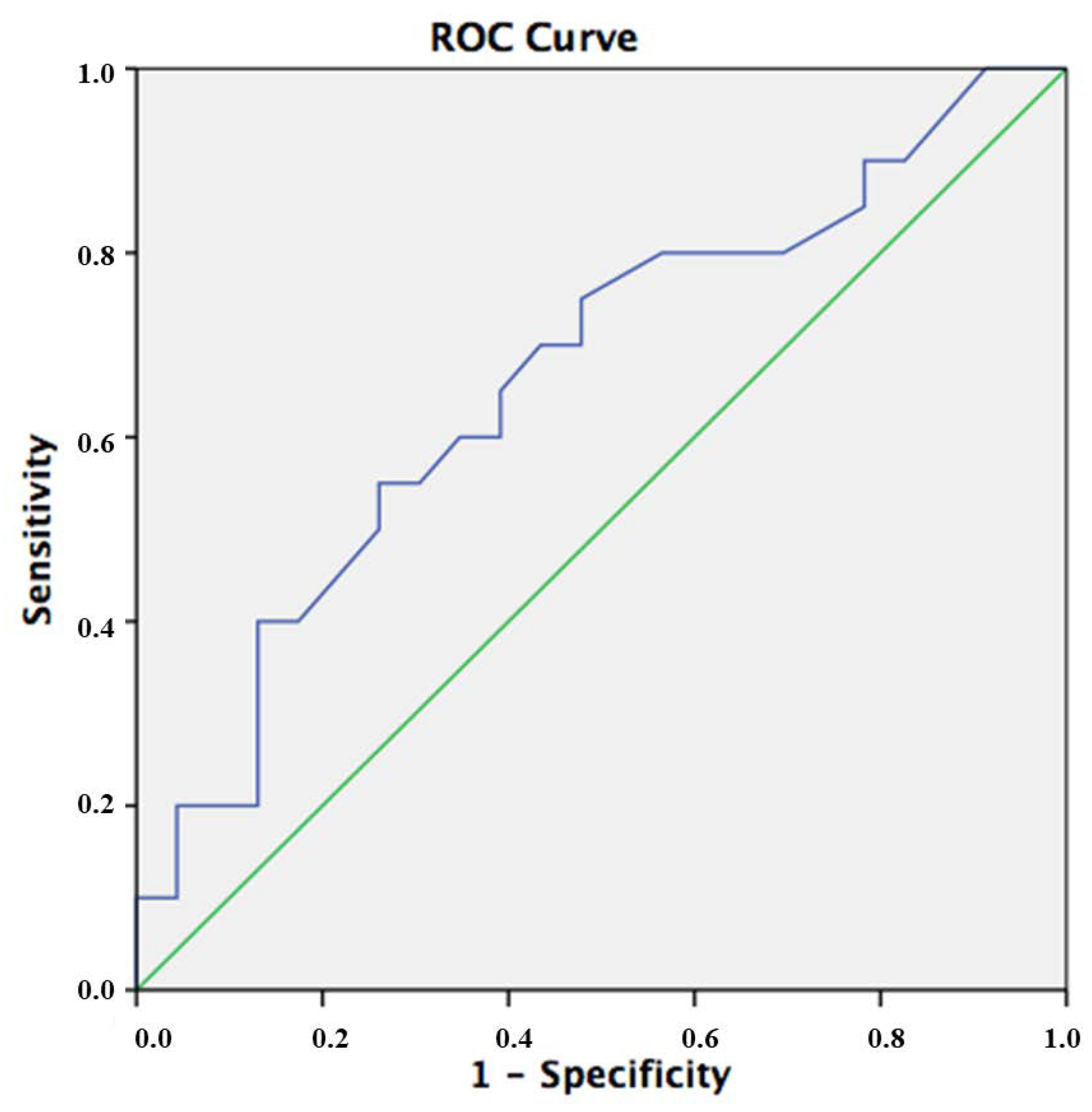
3. Statistical Analysis
4. Results
4.1. Population of the Study
4.2. Biochemical Evaluations
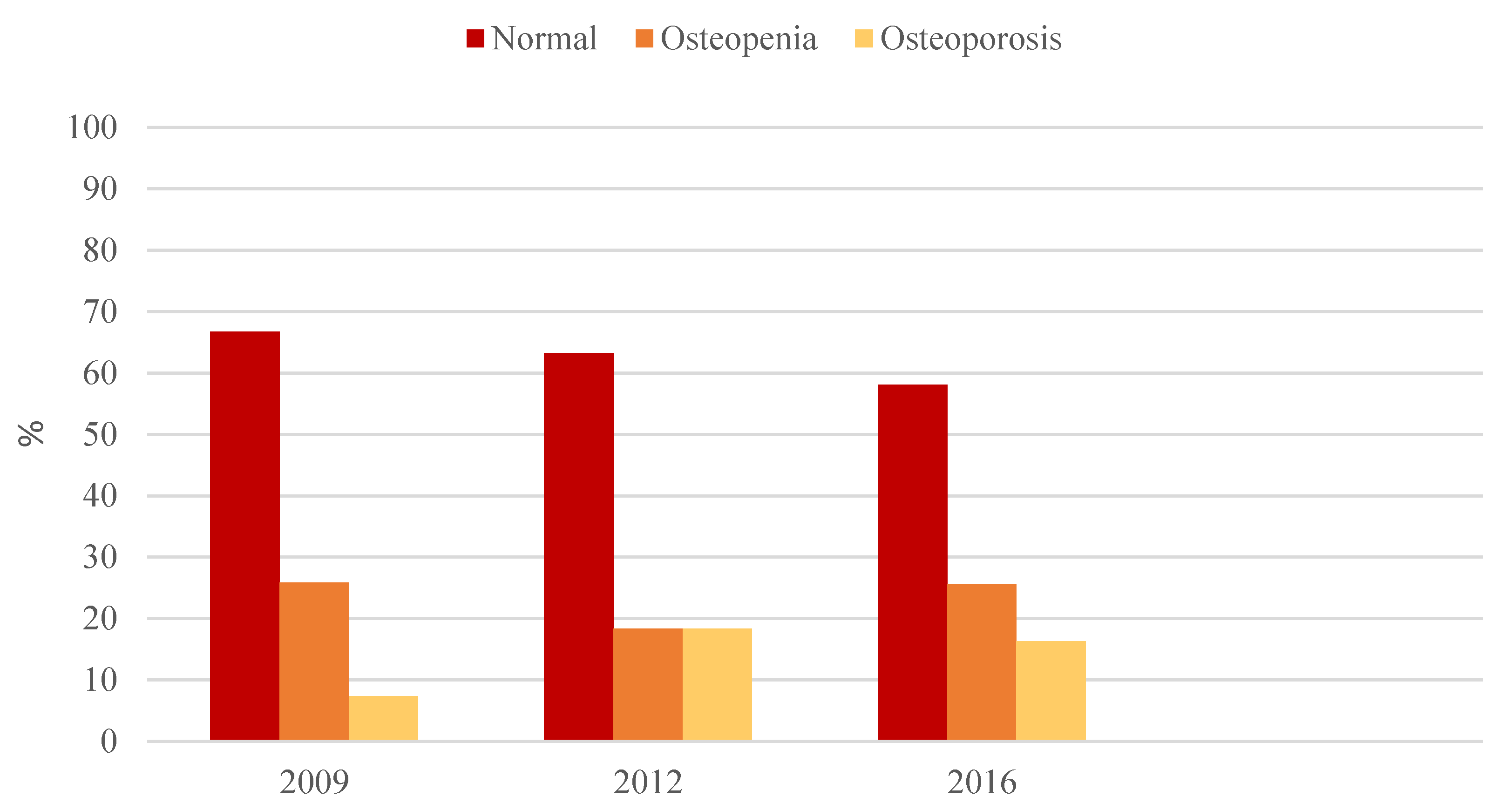
4.3. Bone Density
5. Discussion
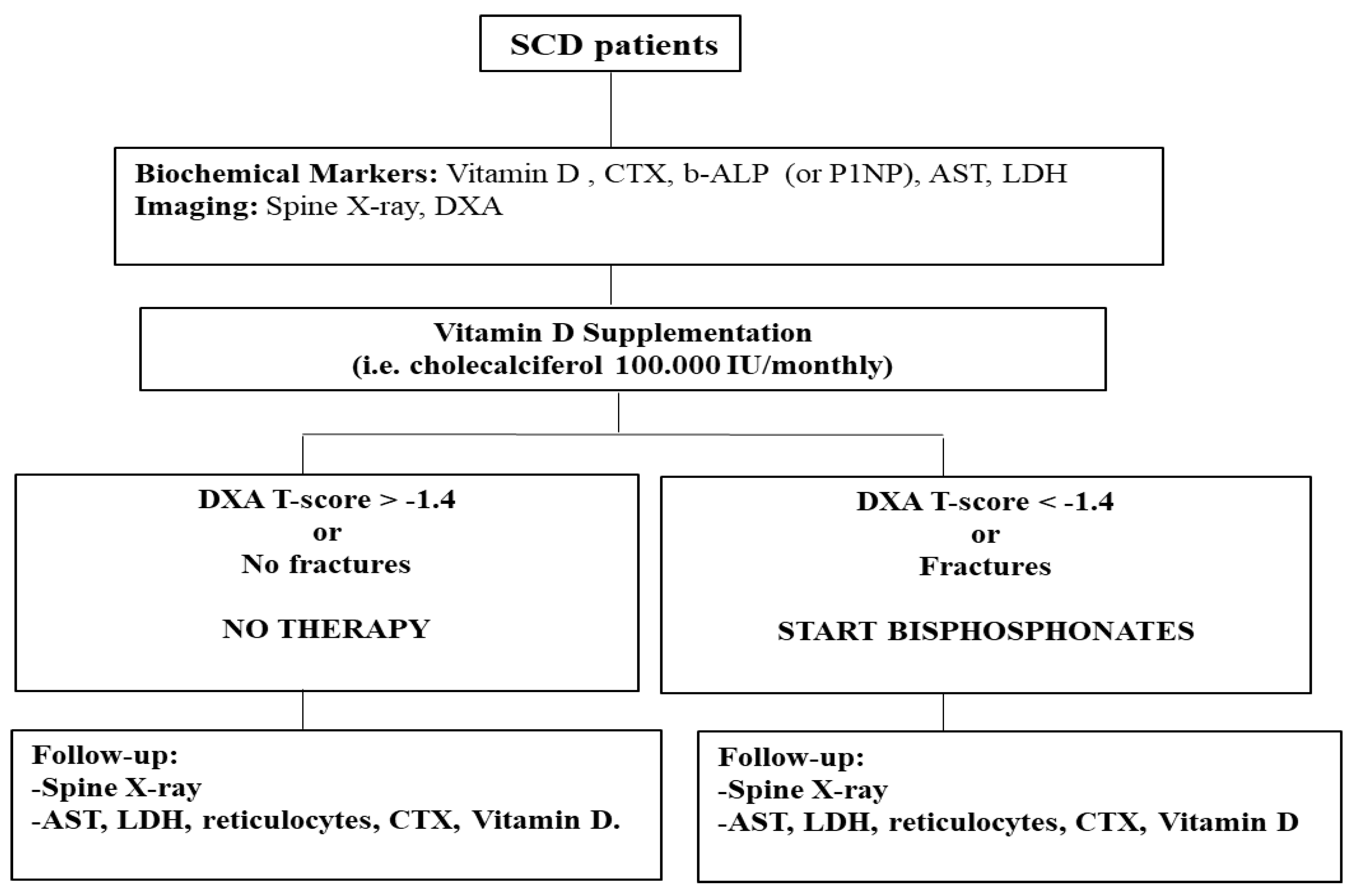
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Piel, F.; Steinberg, M.; Rees, D. Sickle Cell Disease. New Engl. J. Med. 2017, 376, 1561–1573. [Google Scholar] [CrossRef]
- Dalle Carbonare, L.; Matte, A.; Valenti, M.T.; Siciliano, A.; Mori, A.; Schweiger, V.; Zampieri, G.; Perbellini, L.; De Franceschi, L. Hypoxia-reperfusion affects osteogenic lineage and promotes sickle cell bone disease. Blood 2015, 126, 2320–2328. [Google Scholar] [CrossRef]
- Matte, A.; Recchiuti, A.; Federti, E.; Koehl, B.; Mintz, T.; El Nemer, W.; Tharaux, P.L.; Brousse, V.; Andolfo, I.; Lamolinara, A.; et al. Resolution of sickle cell disease-associated inflammation and tissue damage with 17R-resolvin D1. Blood 2019, 133, 252–265. [Google Scholar] [CrossRef]
- De Franceschi, L.; Cappellini, M.D.; Olivieri, O. Thrombosis and sickle cell disease. Semin. Thromb. Hemost. 2011, 37, 226–236. [Google Scholar] [CrossRef]
- Vinchi, F.; De Franceschi, L.; Ghigo, A.; Townes, T.; Cimino, J.; Silengo, L.; Hirsch, E.; Altruda, F.; Tolosano, E. Hemopexin therapy improves cardiovascular function by preventing heme-induced endothelial toxicity in mouse models of hemolytic diseases. Circulation 2013, 127, 1317–1329. [Google Scholar] [CrossRef]
- Kalish, B.T.; Matte, A.; Andolfo, I.; Iolascon, A.; Weinberg, O.; Ghigo, A.; Cimino, J.; Siciliano, A.; Hirsch, E.; Federti, E.; et al. Dietary omega-3 fatty acids protect against vasculopathy in a transgenic mouse model of sickle cell disease. Haematologica 2015, 100, 870–880. [Google Scholar] [CrossRef]
- Miller, R.G.; Segal, J.B.; Ashar, B.H.; Leung, S.; Ahmed, S.; Siddique, S.; Rice, T.; Lanzkron, S. High prevalence and correlates of low bone mineral density in young adults with sickle cell disease. Am. J. Hematol. 2006, 81, 236–241. [Google Scholar] [CrossRef]
- De Luna, G.; Ranque, B.; Courbebaisse, M.; Ribeil, J.A.; Khimoud, D.; Dupeux, S.; Silvera, J.; Offredo, L.; Pouchot, J.; Arlet, J.B. High bone mineral density in sickle cell disease: Prevalence and characteristics. Bone 2018, 110, 199–203. [Google Scholar] [CrossRef]
- Garadah, T.S.; Hassan, A.B.; Jaradat, A.A.; Diab, D.E.; Kalafalla, H.O.; Kalifa, A.K.; Sequeira, R.P.; Alawadi, A.H. Predictors of abnormal bone mass density in adult patients with homozygous sickle-cell disease. Clin. Med. Insights Endocrinol. Diabetes 2015, 8, 35–40. [Google Scholar] [CrossRef]
- Vaishya R, Agarwal AK, Edomwonyi EO, Vijay V: Musculoskeletal Manifestations of Sickle Cell Disease: A Review. Cureus 2015, 7, e358.
- Ramirez, I.; Chew, F.S. Sickle Cell Anemia Skeletal Imaging; Medscape: New York, NY, USA, 2019. [Google Scholar]
- Park, S.Y.; Matte, A.; Jung, Y.; Ryu, J.; Wilson, A.B.; Han, E.Y.A.; Liu, M.; Carbone, C.; Melisi, D.; Nagasawa, T.; et al. Pathologic angiogenesis in the bone marrow of humanized sickle cell mice is reversible by blood transfusion. Blood 2020. [Google Scholar] [CrossRef] [PubMed]
- Arlet, J.B.; Courbebaisse, M.; Chatellier, G.; Eladari, D.; Souberbielle, J.C.; Friedlander, G.; de Montalembert, M.; Prie, D.; Pouchot, J.; Ribeil, J.A. Relationship between vitamin D deficiency and bone fragility in sickle cell disease: A cohort study of 56 adults. Bone 2013, 52, 206–211. [Google Scholar] [CrossRef]
- Dalle Carbonare, L.; Valenti, M.T.; Del Forno, F.; Caneva, E.; Pietrobelli, A. Vitamin D: Daily vs. Monthly Use in Children and Elderly-What Is Going On? Nutrients 2017, 9, 652. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Zhang, X.; Saraf, S.L.; Gowhari, M.; Molokie, R.E.; Hassan, J.; Jain, S.; Shah, B.N.; Abbasi, T.; Machado, R.F.; et al. Risk factors for vitamin D deficiency in sickle cell disease. Br. J. Haematol. 2018, 181, 828–835. [Google Scholar] [CrossRef]
- Almeida, A.; Roberts, I. Bone involvement in sickle cell disease. Br. J. Haematol. 2005, 129, 482–490. [Google Scholar] [CrossRef]
- Nath, K.A.; Hebbel, R.P. Sickle cell disease: Renal manifestations and mechanisms. Nat. Rev. Nephrol. 2015, 11, 161–171. [Google Scholar] [CrossRef]
- Soe, H.H.; Abas, A.B.; Than, N.N.; Ni, H.; Singh, J.; Said, A.R.; Osunkwo, I. Vitamin D supplementation for sickle cell disease. Cochrane Database Syst. Rev. 2017, 1, CD010858. [Google Scholar] [CrossRef]
- Lee, M.T.; Kattan, M.; Fennoy, I.; Arpadi, S.M.; Miller, R.L.; Cremers, S.; McMahon, D.J.; Nieves, J.W.; Brittenham, G.M. Randomized phase 2 trial of monthly vitamin D to prevent respiratory complications in children with sickle cell disease. Blood Adv. 2018, 2, 969–978. [Google Scholar] [CrossRef]
- Voskaridou, E.; Ntanasis-Stathopoulos, I.; Christoulas, D.; Sonnleitner, L.; Papaefstathiou, A.; Dimopoulou, M.; Missbichler, A.; Kanellias, N.; Repa, K.; Papatheodorou, A.; et al. Denosumab effects on serum levels of the bone morphogenetic proteins antagonist noggin in patients with transfusion-dependent thalassemia and osteoporosis. Hematology 2019, 24, 318–324. [Google Scholar] [CrossRef]
- Giusti, A.; Pinto, V.; Forni, G.L.; Pilotto, A. Management of beta-thalassemia-associated osteoporosis. Ann. N. Y. Acad. Sci. 2016, 1368, 73–81. [Google Scholar] [CrossRef]
- De Franceschi, L.; Baldini, M.; Dalle Carbonare, L.; Giusti, A.; Origa, R.; Perrotta, S.; Pinto, V. Raccomandazioni Per il Management Delle Malattie Metaboliche Dell’osso Nelle Emoglobinopatie; SITE, Symposia Srl: Roma, Italy, 2016; pp. 73–81. [Google Scholar]
- Genant, H.K.; Jergas, M.; Palermo, L.; Nevitt, M.; Valentin, R.S.; Black, D.; Cummings, S.R. Comparison of semiquantitative visual and quantitative morphometric assessment of prevalent and incident vertebral fractures in osteoporosis The Study of Osteoporotic Fractures Research Group. J. Bone Min. Res. 1996, 11, 984–996. [Google Scholar] [CrossRef]
- Serarslan, Y.; Kalaci, A.; Ozkan, C.; Dogramaci, Y.; Cokluk, C.; Yanat, A.N. Morphometry of the thoracolumbar vertebrae in sickle cell disease. J. Clin. Neurosci. 2010, 17, 182–186. [Google Scholar] [CrossRef]
- Guglielmi, G.; Diacinti, D.; van Kuijk, C.; Aparisi, F.; Krestan, C.; Adams, J.E.; Link, T.M. Vertebral morphometry: Current methods and recent advances. Eur. Radiol. 2008, 18, 1484–1496. [Google Scholar] [CrossRef]
- Ruosi, C.; Liccardo, S.; Rubino, M.; Colella, G.; Di Somma, C.; Colao, A. Importance of spinal deformity index in risk evaluation of VCF (vertebral compression fractures) in obese subjects: Prospective study. Eur. Spine J. 2013, 22, S945–S949. [Google Scholar] [CrossRef]
- Nolan, V.G.; Nottage, K.A.; Cole, E.W.; Hankins, J.S.; Gurney, J.G. Prevalence of vitamin D deficiency in sickle cell disease: A systematic review. PLoS ONE 2015, 10, e0119908. [Google Scholar] [CrossRef]
- Cohn, M.R.; Gianakos, A.L.; Grueter, K.; Rosen, N.; Cong, G.T.; Lane, J.M. Update on the Comprehensive Approach to Fragility Fractures. J. Orthop. Trauma 2018, 32, 480–490. [Google Scholar] [CrossRef]
- Nouraie, M.; Cheng, K.; Niu, X.; Moore-King, E.; Fadojutimi-Akinsi, M.F.; Minniti, C.P.; Sable, C.; Rana, S.; Dham, N.; Campbell, A.; et al. Predictors of osteoclast activity in patients with sickle cell disease. Haematologica 2011, 96, 1092–1098. [Google Scholar] [CrossRef]
- Bolarin, D.M.; Azinge, E.C. Osteocalcin and specific markers of bone resorption in sickle cell disease. Acta Physiol. Hung. 2010, 97, 290–296. [Google Scholar] [CrossRef]
- Adewoye, A.H.; Chen, T.C.; Ma, Q.; McMahon, L.; Mathieu, J.; Malabanan, A.; Steinberg, M.H.; Holick, M.F. Sickle cell bone disease: Response to vitamin D and calcium. Am. J. Hematol. 2008, 83, 271–274. [Google Scholar] [CrossRef]
- Correia, A.; Azevedo Mdo, S.; Gondim, F.; Bandeira, F. Ethnic aspects of vitamin D deficiency. Arq. Bras. Endocrinol. Metab. 2014, 58, 540–544. [Google Scholar] [CrossRef][Green Version]
- Uchida, S.; Miyaaki, H.; Ichikawa, T.; Taura, N.; Miuma, S.; Honda, T.; Shibata, H.; Haraguchi, M.; Senoo, T.; Nakao, K. Risk factors for osteoporosis in patients with end-stage liver disease. Biomed. Rep. 2016, 5, 629–633. [Google Scholar] [CrossRef]
- Valenti, M.T.; Pietrobelli, A.; Romanelli, M.G.; Franzolin, E.; Malerba, G.; Zipeto, D.; Mottes, M.; Dalle Carbonare, L. Molecular and Lifestyle Factors Modulating Obesity Disease. Biomedicines 2020, 8, 46. [Google Scholar] [CrossRef]
- Dalle Carbonare, L.; Valenti, M.T.; Del Forno, F.; Piacentini, G.; Pietrobelli, A. Vitamin D Daily versus Monthly Administration: Bone Turnover and Adipose Tissue Influences. Nutrients 2018, 10, 1934. [Google Scholar] [CrossRef]
- Rafiq, R.; Walschot, F.; Lips, P.; Lamb, H.J.; de Roos, A.; Rosendaal, F.R.; Heijer, M.D.; de Jongh, R.T.; de Mutsert, R. Associations of different body fat deposits with serum 25-hydroxyvitamin D concentrations. Clin. Nutr. 2019, 38, 2851–2857. [Google Scholar] [CrossRef]
- Cehic, M.; Lerner, R.G.; Achten, J.; Griffin, X.L.; Prieto-Alhambra, D.; Costa, M.L. Prescribing and adherence to bone protection medications following hip fracture in the United Kingdom: Results from the World Hip Trauma Evaluation (WHiTE) cohort study. Bone Jt. J. 2019, 101-B, 1402–1407. [Google Scholar] [CrossRef]
- Torre, C.; Guerreiro, J.; Mendes, Z.; Miranda, A.; Braganca, F.; Cristino, J.; Canhao, H.; Branco, J.C. Low persistence with oral biphosphonate treatment in postmenopausal osteoporosis. Acta Reum. Port. 2019, 44, 114–125. [Google Scholar]
- Khundmiri, S.J.; Murray, R.D.; Lederer, E. PTH and Vitamin, D. Compr. Physiol. 2016, 6, 561–601. [Google Scholar]
- Voskaridou, E.; Stoupa, E.; Antoniadou, L.; Premetis, E.; Konstantopoulos, K.; Papassotiriou, I.; Terpos, E. Osteoporosis and osteosclerosis in sickle cell/beta-thalassemia: The role of the RANKL/osteoprotegerin axis. Haematologica 2006, 91, 813–816. [Google Scholar]
- Griffith, J.F.; Yeung, D.K.; Tsang, P.H.; Choi, K.C.; Kwok, T.C.; Ahuja, A.T.; Leung, K.S.; Leung, P.C. Compromised bone marrow perfusion in osteoporosis. J. Bone Min. Res. 2008, 23, 1068–1075. [Google Scholar] [CrossRef]
- Ficat, R.P. Aseptic necrosis of the femur head. Preliminary remarks concerning staging: Stage O. Acta. Orthop. Belg. 1981, 47, 239–241. [Google Scholar]
- Barbu, E.C.; Chitu-Tisu, C.E.; Lazar, M.; Olariu, C.; Bojinca, M.; Ionescu, R.A.; Ion, D.A.; Badarau, I.A. Hepatic Osteodystrophy: A Global (Re)View of the Problem. Acta Clin. Croat. 2017, 56, 512–525. [Google Scholar] [CrossRef] [PubMed]
- Jamil, Z.; Arif, S.; Khan, A.; Durrani, A.A.; Yaqoob, N. Vitamin D Deficiency and Its Relationship with Child-Pugh Class in Patients with Chronic Liver Disease. J. Clin. Transl. Hepatol. 2018, 6, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Karoli, Y.; Karoli, R.; Fatima, J.; Manhar, M. Study of Hepatic Osteodystrophy in Patients with Chronic Liver Disease. J. Clin. Diagn. Res. 2016, 10, OC31–OC34. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male | 31 (44%) |
| Female | 40 (56%) |
| Age (yrs) | 38.99 ± 10.26 |
| SS | 22 (31%) |
| SC | 11 (15%) |
| Sβ0 | 38 (53%) |
| African | 26 (37%) |
| Caucasian | 35 (50%) |
| South American | 5 (7%) |
| Central American | 4 (6%) |
| Erytroapheresis | 34 (48%) |
| Hydroxyurea | 30 (42%) |
| Untreated pts for SCD | 7 (10%) |
| Vitamin D supplementation | 38 (53%) |
| Vitamin D + Bisphosphonates | 9 (13%) |
| No bone therapy | 24 (34%) |
| 2009 | 2012 | 2017 | |
|---|---|---|---|
| Erythrocytes (1012/L) | 3.80 ± 0.70 | 3.88 ±0.57 | 3.75 ± 0.58 |
| Hematocrit (%) | 31.66 ± 4.06 | 32.56 ± 3.64 | 31.51 ± 3.38 |
| Hemoglobin (g/dL) | 10.57 ± 1.36 | 10.76 ± 1.13 | 10.52 ± 1.23 |
| MCV (fL) | 85.38 ± 9.72 | 86.81 ± 9.95 | 85.31 ± 9.24 |
| MCH (pg) | 28.44 ± 4.00 | 28.27 ± 3.34 | 28.35 ± 3.76 |
| MCHC (g/dL) | 40.20 ± 14.17 | 32.56 ± 1.05 | 31.92 ± 2.59 |
| RDW (%) | – | 18.43 ± 1.99 | 18.24 ± 2.30 |
| Reticulocytes (109/L) | 225.68 ± 217.98 | 106.31 ± 137.95 | 284.57 ± 132.54 |
| Platelets (109/L) | 399 ± 104.61 | 412.21 ± 133.67 | 375.99 ± 116.87 |
| Leukocytes (109/L) | 9.67 ± 2.24 | 9.58 ± 2.97 | 9.93 ± 3.25 |
| AST (U/L) | 40.06 ± 16.28 | 36.36 ± 12.03 | 38.50 ± 15.15 |
| Indirect bilirubin (mg/dL) | 2.46 ± 1.35 | 1.35 ± 0.68 | 1.36 ± 0.78 |
| LDH (U/L) (135–225) | 634.25 ± 190.52 | 624.26 ± 131.95 | 689.27 ± 266.48 |
| ALT (U/L) (6–50) | 32.53 ± 16.10 | 31.34 ± 12.72 | 28.38 ± 12.93 |
| Ferritin (mcg/L) (30–400) | – | 1097.50 ± 899.32 | 1194.74±1097.75 |
| Creatinine (mg/dL) (0.59–1.29) | 0.71 ± 0.18 | 0.67 ± 0.16 | 0.80 ± 0.31 |
| Calcium (mg/dL)(8.41–10.42) | 9.23 ± 0.34 | 9.38 ± 0.32 | 9.12 ± 0.42 |
| Phosphates (mg/dL) (2.63–4.49) | 4.02 ± 0.5 | 3.52 ± 0.42 | 4.41 ± 1.80 |
| Calcium/Creatinine (<0.57) | – | 0.11 ± 0.07 | 0.35 ± 0.18 |
| ALP (U/L) (50–130) | 77.95 ± 22.74 | 76.00 ± 24.94 | 77.3 ± 27.46 |
| CTX (ng/mL) (0100–0700) | 0.44 ± 0.04 | 0.50 ± 0.21 | 0.47 ± 0.17 |
| P1NP (mcg/L)(28–128) | – | – | 64.81 ± 24.31 |
| PTH (pg/mL) (1.6–6.9) | 64.9 ± 11.72 | 33.67 ± 13.53 | 43.05 ± 22.10 |
| Vitamin D (ng/mL) (>30) | 14.05 ± 6.65 | 13.34 ± 6.33 | 17.65 ± 9.64 |
| 2009 | 2012 | 2017 | |
|---|---|---|---|
| Spine BMD (g/cm2) | 1.10 ± 0.15 | 1.12 ± 0.17 | 1.16 ± 0.21 |
| Spine T score (SD) | −0.50 ± 1.38 | −0.27 ± 1.50 | −0.33 ± 1.68 |
| Spine Z score (SD) | −0.27 ± 1.43 | −0.04 ± 1.54 | −0.07 ± 1.64 |
| Femur total BMD (g/cm2) | 1.01 ± 0.16 | 1.01 ± 0.15 | 1.01 ± 0.14 |
| Femur total T score (SD) | −0.22 ± 1.10 | −0.22 ± 0.99 | −0.30 ± 0.98 |
| Femur total Z score (SD) | −0.08 ± 1.15 | −0.04 ± 1.01 | −0.01 ± 0.98 |
| Femur neck BMD (g/cm2) | 0.89 ± 0.12 | 0.88 ± 0.11 | 0.87 ± 0.12 |
| Femur neck T score (SD) | −0.76 ± 0.91 | −0.70 ± 0.85 | −1.03 ± 0.78 |
| Femur neck Z score (SD) | −0.42 ± 0.88 | −0.39 ± 0.84 | −0.61 ± 0.80 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Franceschi, L.; Gabbiani, D.; Giusti, A.; Forni, G.; Stefanoni, F.; Pinto, V.M.; Sartori, G.; Balocco, M.; Dal Zotto, C.; Valenti, M.T.; et al. Development of Algorithm for Clinical Management of Sickle Cell Bone Disease: Evidence for a Role of Vertebral Fractures in Patient Follow-up. J. Clin. Med. 2020, 9, 1601. https://doi.org/10.3390/jcm9051601
De Franceschi L, Gabbiani D, Giusti A, Forni G, Stefanoni F, Pinto VM, Sartori G, Balocco M, Dal Zotto C, Valenti MT, et al. Development of Algorithm for Clinical Management of Sickle Cell Bone Disease: Evidence for a Role of Vertebral Fractures in Patient Follow-up. Journal of Clinical Medicine. 2020; 9(5):1601. https://doi.org/10.3390/jcm9051601
Chicago/Turabian StyleDe Franceschi, Lucia, Daniele Gabbiani, Andrea Giusti, Gianluca Forni, Filippo Stefanoni, Valeria Maria Pinto, Giulia Sartori, Manuela Balocco, Chiara Dal Zotto, Maria Teresa Valenti, and et al. 2020. "Development of Algorithm for Clinical Management of Sickle Cell Bone Disease: Evidence for a Role of Vertebral Fractures in Patient Follow-up" Journal of Clinical Medicine 9, no. 5: 1601. https://doi.org/10.3390/jcm9051601
APA StyleDe Franceschi, L., Gabbiani, D., Giusti, A., Forni, G., Stefanoni, F., Pinto, V. M., Sartori, G., Balocco, M., Dal Zotto, C., Valenti, M. T., & Dalle Carbonare, L. (2020). Development of Algorithm for Clinical Management of Sickle Cell Bone Disease: Evidence for a Role of Vertebral Fractures in Patient Follow-up. Journal of Clinical Medicine, 9(5), 1601. https://doi.org/10.3390/jcm9051601