Preoperative, Intraoperative and Postoperative Corticosteroid Use as an Adjunctive Treatment for Rhegmatogenous Retinal Detachment

 ,
,  , , ,
, , , 

 ,
,
Abstract
1. Introduction
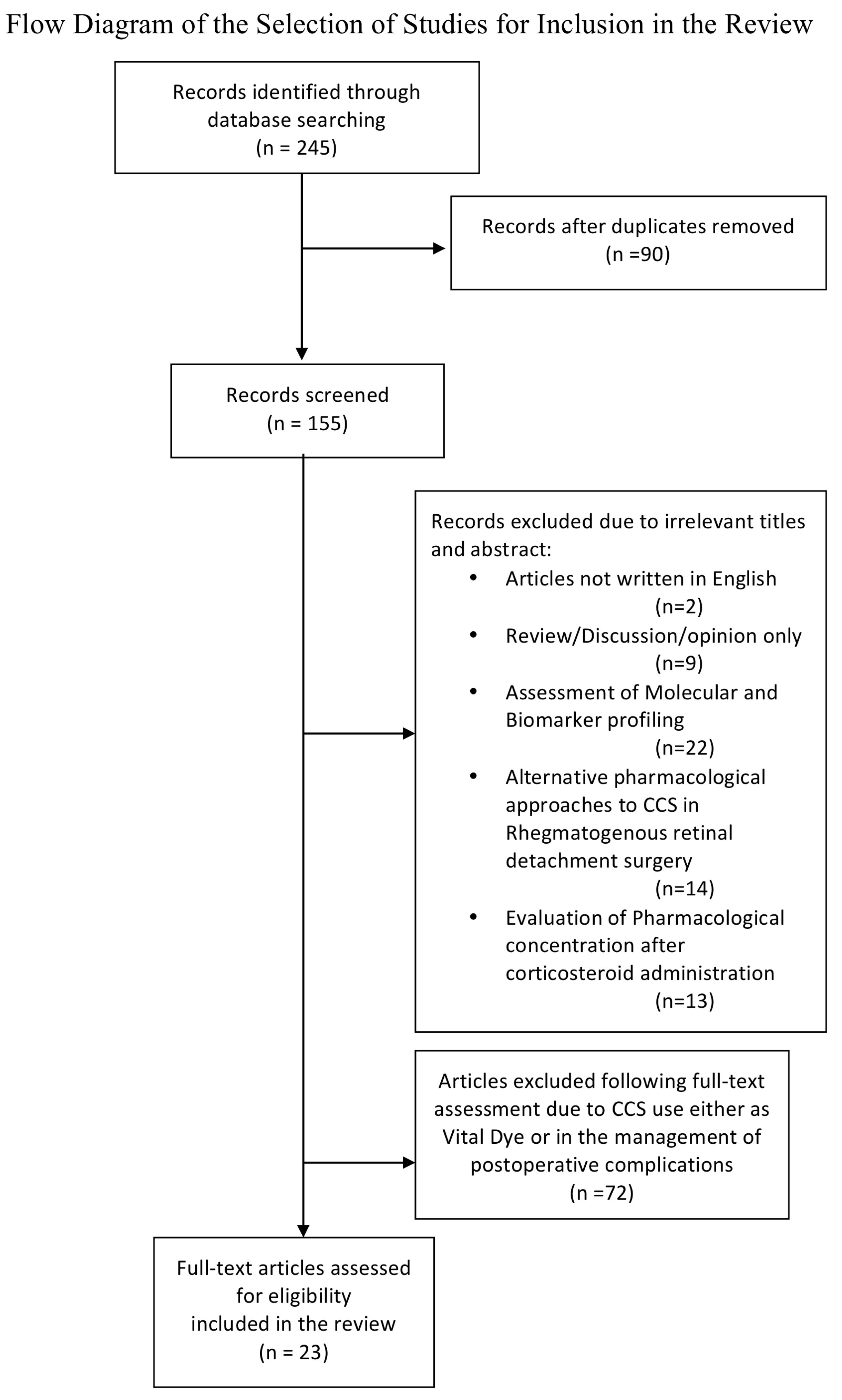
2. Methods
2.1. Search Methods for Identification of Studies
2.2. Eligibility Criteria
2.3. Data Collection
- (1)
- Study design: retrospective, prospective, comparative and non-comparative, randomized and non-randomized, single-center and multicenter and case report
- (2)
- Clinical outcomes: anatomical and functional
- (3)
- 3Number of eyes studied
- (4)
- Primary treatment
- (5)
- Follow-up (duration of the study)
- (6)
- Main results
- (7)
- Side effects
3. Results
3.1. Preoperative Use
3.2. Intraoperative Use
3.3. Postoperative Use
4. Conclusions
5. Recommendation
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Liao, L.; Zhu, X.H. Advances in the treatment of rhegmatogenous retinal detachment. Int. J. Ophthalmol. 2019, 12, 660–667. [Google Scholar] [PubMed]
- Sodhi, A.; Leung, L.S.; Do, D.V.; Gower, E.W.; Schein, O.D.; Handa, J.T. Recent trends in the management of rhegmatogenous retinal detachment. Surv. Ophthalmol. 2008, 53, 50–67. [Google Scholar] [CrossRef] [PubMed]
- Kunikata, H.; Yasuda, M.; Aizawa, N.; Tanaka, Y.; Abe, T.; Nakazawa, T. Intraocular concentrations of cytokines and chemokines in rhegmatogenous retinal detachment and the effect of intravitreal triamcinolone acetonide. Am. J. Ophthalmol. 2013, 155, 1028–1037. [Google Scholar] [CrossRef] [PubMed]
- Kwon, O.W.; Song, J.H.; Roh, M.I. Retinal detachment and proliferative vitreoretinopathy. Dev. Ophthalmol. 2016, 55, 154–162. [Google Scholar] [PubMed]
- Josifovska, N.; Lumi, X.; Szatmari-Tóth, M.; Kristóf, E.; Russell, G.; Nagymihály, R.; Anisimova, N. Clinical and molecular markers in retinal detachment from hyperreflective points to stem cells and inflammation. PLoS ONE 2019, 14, e0217548. [Google Scholar] [CrossRef] [PubMed]
- Jarrett, W.H. Rhegmatogenous retinal detachment complicated by severe intraocular inflammation, hypotony, and choroidal detachment. Trans. Am. Ophthalmol. Soc. 1981, 79, 664–683. [Google Scholar]
- Ben, Y.S.; Kahloun, R.; Abroug, N.; Kalibi, I.; Laadhari, G.; Ielliti, B.; Khairallah, M. Comparative effect of topical diclofenac and topical dexamethasone on anterior chamber flare and postoperative pain following rhegmatogenous retinal detachment surgery. Int. Ophthalmol. 2016, 36, 623–628. [Google Scholar] [CrossRef]
- Barnes, P.J. Anti inflammatory mechanism of glucorticoids. Biochem. Soc. Trans. 1995, 23, 940–945. [Google Scholar] [CrossRef]
- Shi, H.; Guo, T.; Liu, P.C.; Wang, Q.Y.; Du, Y.R.; Liu, Q.Y.; He, M.M.; Liu, J.L.; Yu, J. Steroids as an adjunct for reducing the incidence of proliferative vitreoretinopathy after rhegmatogenous retinal detachment surgery: A systematic review and meta-analysis. Drug Des. Dev. Ther. 2015, 9, 1393–1400. [Google Scholar]
- Ando, N.; Sen, H.A.; Berkowitz, B.A.; Wilson, C.A.; De Juan, E., Jr. Localization and quantitation of blood-retinal barrier breakdown in experimental proliferative vitreoretinopathy. Arch. Ophthalmol. 1994, 112, 117–122. [Google Scholar] [CrossRef]
- Bali, E.; Feron, E.; Peperkamp, E.; Veeckeneer Mulder, P.; Van Meurs, J. The effect of a preoperative subconjunctival injection of dexamethasone on blood- retinal barrier breakdown following scleral buckling retinal detachment surgery: A prospective randomized placebo-controlled double blind clinical trial. Graefes Arch. Clin. Exp. Ophthalmol. 2010, 248, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Weijtens, O.; Schoemaker, R.C.; Lentjes, E.G.; Romijn, F.P.; Cohen, A.F.; Van Meurs, J.C. Dexamethasone concentration in the subretinal fluid after a subconjunctival injection, a peribulbar Injection or an oral dose. Ophthalmology 2000, 107, 1932–1938. [Google Scholar] [CrossRef]
- Weijtens, O.; Van der Sluijs, F.A.; Schoemaker, R.C.; Lentjes, E.G.; Cohen, A.F.; Romijn, F.P.; Van Meurs, J.C. Peribulbar corticosteroid injection:vitreal and serum concentrations after dexamethasone disodium phosphate injection. Am. J. Ophthalmol. 1997, 123, 358–363. [Google Scholar] [CrossRef]
- Weijtens, O.; Schoemaker, R.C.; Cohen, A.F.; Romijn, F.P.; Lentjes, E.G.; Van Rooij, J.; Van Meurs, J.C. Dexamethasone concentration in vitreous and serum after oral administration. Am. J. Ophthalmol. 1998, 125, 673–679. [Google Scholar] [CrossRef]
- Weijtens, O.; Feron, E.J.; Schoemaker, R.C.; Cohen, A.F.; Lentjes, E.G.; Romijn, F.P.; Van Meurs, J.C. High concentration of dexamethasone in aqueous and vitreous after subconjunctival injection. Am. J. Ophthalmol. 1999, 128, 192–197. [Google Scholar] [CrossRef]
- Shen, L.; You, Y.; Sun, S.; Chen, Y.; Qu, J.; Cheng, L. Intraocular and systemic pharmacokinetics of triamcinolone acetonide after a single 40-mg posterior subtenon application. Ophthalmology 2010, 117, 2365–2371. [Google Scholar] [CrossRef]
- Kovacs, K.; Wagley, S.; Quirk, M.T.; Ceron, O.M.; Silva, P.A.; Singh, R.J.; Gukasyan, H.J.; Arroyo, J.G. Pharmacokinetic Study of Vitreous and Serum Concentrations of Triamcinolone Acetonide after Posterior Sub-Tenon’s Injection. Am. J. Ophthalmol. 2012, 53, 939–948. [Google Scholar] [CrossRef]
- Inoue, M.; Takeda, K.; Morita, K.; Yamada, M.; Tanigawara, Y.; Oguchi, Y. Vitreous concentrations of triamcinolone acetonide in human eyes after intravitreal or subtenon injection. Am. J. Ophthalmol. 2004, 138, 1046–1048. [Google Scholar] [CrossRef]
- Huscher, D.; Thiele, K.; Gromnica-Ihle, E.; Hein, G.; Demary, W.; Dreher, R.; Zink, A.; Buttgereit, F. Dose-related patterns of glucocorticoid-induced side effects. Ann. Rheum. Dis. 2009, 68, 1119–1124. [Google Scholar] [CrossRef]
- Elena, C.; Chiara, M.; Angelica, B.; Chiara, M.A.; Laura, N.; Chiara, C.; Claudio, C.; Antonella, F.; Nicola, G. Hyperglycemia and Diabetes Induced by Glucocorticoids in Nondiabetic and Diabetic Patients: Revision of Literature and Personal Considerations. Curr. Pharm. Biotechnol. 2018, 19, 1210–1220. [Google Scholar] [CrossRef]
- Carnahan, M.C.; Goldstein, D.A. Ocular Complications of Topical, Peri-Ocular, and Systemic Corticosteroids. Curr. Opin. Ophthalmol. 2000, 11, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Veritti, D.; Di Giulio, A.; Sarao, V.; Lanzetta, P. Drug safety evaluation of intravitreal triamcinolone acetonide. Expert Opin. Drug Saf. 2012, 11, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, M.; Hirano, Y.; Nozaki, M.; Yoshida, M.; Ogura, Y. Incidence of posterior subcapsular cataract progression after triamcinolone acetonide administration. Nippon Ganka Gakkai Zasshi 2008, 112, 786–789. [Google Scholar]
- Reibaldi, M.; Avitabile, T.; Russo, A.; Bonfiglio, V.; Mariotti, C.; Romano, M.R.; Boscia, F.; Cennamo, G.; Fallico, M.; Parisi, G.; et al. Late onset ocular hypertension after vitrectomy: A multicenter study of 6048 eyes. Retina 2019, 39, 2107–2115. [Google Scholar] [CrossRef] [PubMed]
- Maeda, Y.; Ishikawa, H.; Nishikawa, H.; Shimizu, M.; Kinoshita, T.; Ogihara, R.; Kitano, S.; Yamanaka, C.; Mitamura, Y.; Sugimoto, M.; et al. Intraocular pressure elevation after subtenon triamcinolone acetonide injection; Multicentre retrospective cohort study in Japan. PLoS ONE 2019, 14, e0226118. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Kuppermann, B.D.; Bandello, F.; Lanzetta, P.; Zur, D.; Park, S.W.; Yu, H.G. Intraocular Pressure (IOP) After Intravitreal Dexamethasone Implant (Ozurdex) Amongst Different Geographic populations-GEODEX-IOP Study. Eye 2019, 30, 1–6. [Google Scholar] [CrossRef]
- Sharma, T.; Gopal, L.; Reddy, R.K.; Kasinathan, N.; Shah, N.A.; Sulochana, K.N.; Miriam, K.C.; Arvind, K.; Ramakrishnan, S.; Sukumar, B. Primary vitrectomy for combined rhegmatogenous retinal detachment and choroidal detachment with or without oral corticosteroids: A pilot study. Retina 2005, 25, 152–157. [Google Scholar] [CrossRef]
- Wei, Y.; Wang, N.; Chen, F.; Wang, H.; Bi, C.; Zu, Z.; Yang, X. Vitrectomy combined with periocular/intravitreal injection of steroids for rhegmatogenous retinal detachment associated with choroidal detachment. Retina 2014, 34, 136–141. [Google Scholar] [CrossRef]
- Shen, L.J.; Mao, J.B.; Sun, S.M.; Dong, Y.G.; Chen, Y.Q.; Cheng, L.Y. Perioperative pharmacological management of choroidal detachment associated with rhegmatogenous retinal detachment. Acta Ophthalmol. 2016, 94, 391–396. [Google Scholar] [CrossRef]
- Alibet, Y.; Levytska, G.; Umanets, N.; Pasyechnikova, N.; Henrich, P.B. Ciliary body thickness changes after preoperative anti-inflammatory treatment in rhegmatogenous retinal detachment complicated by choroidal detachment. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 1503–1508. [Google Scholar] [CrossRef]
- Denwattana, A.; Prahkunhungsit, S.; Thoongsuwan, S.; Rodanant, N.; Phasukkijwatana, N. Surgical outcomes of preoperative steroid for rhegmatogenous retinal detachment with associated choroidal detachment. Eye 2018, 32, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Yue, Y.; Tong, N.; Zheng, P.; Liu, W.; An, M. Anatomic Outcomes and Prognostic Factors of Vitrectomy in Patients with Primary Rhegmatogenous Retinal Detachment Associated with Choroidal Detachment. Curr. Eye Res. 2019, 44, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Seelenfreund, M.H.; Kraushar, M.F.; Schepens, C.L.; Freilich, D.B. Choroidal detachment associated with primary retinal detachment. Arch. Ophthalmol. 1974, 91, 254–258. [Google Scholar] [CrossRef] [PubMed]
- Rahman, N.; Harris, G. Choroidal detachment associated with retinal detachment as a presenting finding. Can. J. Ophthalmol. 1992, 27, 245–248. [Google Scholar]
- Loo, A.; Fitt, A.W.D.; Ramchadani, M.; Kirkby, G.R. Pars plana vitrectomy with silicon oil in the management of combined rhegmatogenous retinal and choroidal detachment. Eye 2001, 15, 612–615. [Google Scholar] [CrossRef]
- Gui, J.M.; Jia, L.; Liu, L.; Liu, J.D. Vitrectomy, lensectomy and silicone oil tamponade in the management of retinal detachment associated with choroidal detachment. Int. J. Ophthalmol. 2013, 6, 337–341. [Google Scholar]
- Yu, Y.; An, M.; Yang, Z.; Liu, W. Risk factors for choroidal detachment following rhagmatogenous retinal detachment in a chinese population. BMC Ophthalmol. 2016, 16, 140. [Google Scholar] [CrossRef]
- Sharma, T.; Gopal, L.; Badrinath, S.S. Primary vitrectomy for regmatogenous retinal detachment associated with coroideal detachment. Ophalmology 1998, 105, 2282–2285. [Google Scholar] [CrossRef]
- Dai, Y.; Wu, Z.; Sheng, H.; Zhang, Z.; Yu, M.; Zhang, Q. Identification of inflammatory mediators in patients with rhegmatogenous retinal detachment associated with chroidal detachment. Mol. Vis. 2015, 21, 417–427. [Google Scholar]
- Munir, W.M.; Pulido, J.S.; Sharma, M.C.; Buerk, B.M. Intravitreal triamcinolone for treatment of complicated proliferative diabetic retinopathy and proliferative vitreoretinopathy. Can. J. Ophthalmol. 2005, 40, 598–604. [Google Scholar] [CrossRef]
- Cheema, R.A.; Peyman, G.A.; Fang, T.; Jones, A.; Lukaris, A.D.; Lim, K. Triamcinolone acetonide as an adjuvant in the surgical treatment of retinal detachment with proliferative vitreoretinopathy. Ophthalmic Surg. Lasers Imaging 2007, 38, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Admaideh, H.; Feghhi, M.; Tabatabaei, H.; Shoeibi, N.; Ramezani, A.; Mohebbi, M.R. Triamcinolone acetonide in silicone-filled eyes as adjunctive treatment for proliferative vitreoretinopathy: A randomized clinical trial. Ophthalmology 2008, 115, 1938–1943. [Google Scholar]
- Yamakiri, K.; Sakamoto, T.; Noda, Y.; Nakahara, M.; Ogino, N.; Kubota, T.; Yokoyama, M.; Furukawa, M.; Shibashi, T. One-year results of a multicenter controlled clinical trial of triamcinolone in pars plana vitrectomy. Graefes Arch. Clin. Exp. Ophthalmol. 2008, 246, 959–966. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chen, W.; Chen, H.; Hou, P.; Fok, A.; Hu, Y.; Lam, D.S. Midterm results of low dose intravitreal triamcinolone as adjunctive treatment for proliferative vitreoretinopathy. Retina 2011, 31, 1137–1142. [Google Scholar] [CrossRef]
- Reibaldi, M.; Russo, A.; Longo, A.; Bonfiglio, V.; Uva, M.G.; Gagliano, C.; Toro, M.D.; Avitabile, T. Regmatogenous retinal detachment with a high risk of proliferative vitreoretinopathy treated with episcleral surgery and an intravitreal dexamethasone 0.7-mg implant. Case Rep. Ophthalmol. 2013, 4, 79–83. [Google Scholar] [CrossRef]
- Mirshahi, A.; Karkhaneh, R.; Zamani Amir, J.; Movassat, M.; Azadi, P. Influence of intravitreal triamcinolone acetonide injection in sclera buckling surgery for macula-off retinal detachment. Ophthalmic Res. 2014, 52, 160–164. [Google Scholar] [CrossRef]
- Sherif, M.; Wolfensberger, T.J. Intraocular dexamethasone implant as adjunct to silicone oil tamponade for proliferative vitreoretinopathy. Klin. Mon. Augenheilkd. 2017, 234, 501–504. [Google Scholar] [CrossRef]
- Banerjee, P.J.; Quartilho, A.; Bunce, C.; Xing, W.; Zvobgo, T.M.; Harris, N.; Charteris, D.G. Slow release dexamethasone in proliferative vitreoretinopathy:a prospective, randomized controlled clinical trial. Ophthalmology 2017, 124, 757–767. [Google Scholar] [CrossRef]
- Cho, A.R.; Yoon, Y.H. Adjunctive dexamethasone implant in patients with atopic dermatitis and retinal detachment undergoing vitrectomy and silicone oil tamponade: An interventional case series. BMC Ophthalmol. 2019, 19, 86. [Google Scholar] [CrossRef]
- Reibaldi, M.; Fallico, M.; Longo, A.; Avitabile, T.; Astuto, M.; Murabito, P.; Minardi, C.; Bonfiglio, V.; Boscia, F.; Furino, C.; et al. Efficacy of three different prophylactic treatments for postoperative nausea and vomiting after vitrectomy: A randomized Clinical Trial. J. Clin. Med. 2019, 8, 391. [Google Scholar] [CrossRef]
- Tseng, W.; Cortez, R.T.; Ramirez, G.; Stinnett, S.; Jaffe, G.J. Prevalence and risk factors for proliferative vitreoretinopathy in eyes with rhegmatogenous retinal detachment but no previous vitreoretinal surgery. Am. J. Ophthalmol. 2004, 137, 1105–1115. [Google Scholar] [CrossRef] [PubMed]
- Cowley, M.; Conway, B.P.; Campochiaro, P.A.; Kaiser, D.; Gaskin, H. Clinical risk factors for proliferative vitreoretinopathy. Arch. Ophthalmol. 1989, 107, 1147–1151. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, M.; Fleury, J.; Guenoun, S.; Yaniali, A.; Dumas, C.; Hajjar, C. Cryopexy in primary rhegmatogenous retinal detachment: A risk factor for postoperative proliferative vitreoretinopathy? Graefes Arch. Clin. Exp. ophthalmol. 1996, 234, 739–743. [Google Scholar] [CrossRef] [PubMed]
- Gagliano, C.; Toro, M.D.; Avitabile, T.; Stella, S.; Uva, M.G. Intravitreal steroids for the prevention of PVR After Surgery for Retinal Detachment. Curr. Pharm. Des. 2015, 21, 4698–4702. [Google Scholar] [CrossRef]
- Moysidis, S.; Thanos, A.; Vavvas, D.G. Mechanisms of Inflammation in Proliferative Vitreoretinopathy: From Bench to Bedside. Mediat. Inflamm. 2012, 2012, 815937. [Google Scholar] [CrossRef]
- Ricker, L.J.; Kessels, A.G.; De Jager, W.; Hendrikse, F.; Kijlstra, A.; la Heij, E.C. Prediction of proliferative vitreoretinopathy after retinal detachment surgery: Potential of biomarker profiling. Am. J. Ophthalmol. 2012, 154, 347–354. [Google Scholar] [CrossRef]
- Bonfiglio, V.; Reibaldi, M.; Fallico, M.; Russo, A.; Pizzo, A.; Fichera, S.; Rapisarda, C.; Macchi, I.; Avitabile, T.; Longo, A. Widening use of dexamethasone implant for the treatment of macular edema. Drug Des. Dev. Ther. 2017, 11, 2359–2372. [Google Scholar] [CrossRef]
- Chang-Lin, J.E.; Burke, J.A.; Peng, Q.; Lin, T.; Orilla, W.C.; Ghosn, C.R.; Zhang, K.M. Pharmacokinetics of a sustained-release dexamethasone intravitreal implant in vitrectomized and nonvitrectomized eyes. Investig. Ophthalmol. Vis. Sci. 2011, 52, 4605–4609. [Google Scholar] [CrossRef]
- Chin, H.S.; Park, T.S.; Moon, Y.S.; Oh, J.H. Difference in clearance of intravitreal triamcinolone acetonide between vitrectomized and nonvitrectomized eyes. Retina 2005, 25, 556–560. [Google Scholar] [CrossRef]
- Beer, P.M.; Bakri, S.J.; Singh, R.J.; Liu, W.; Peters, G.B.; Miller, M. Intraocular concentration and pharmacokinetics of triamcinolone acetonide after a single intravitreal injection. Ophthalmology 2003, 110, 681–686. [Google Scholar] [CrossRef]
- Pessoa, B.; Coelho, J.; Correia, N.; Ferreira, N.; Beirão, M.; Meireles, A. Fluocinolone acetonide intravitreal implant 190 μg (ILUVIEN®) in vitrectomized versus nonvitrectomized eyes for the treatment of chronic diabetic macular edema. Ophthalmic Res. 2018, 59, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Coelho, J.; Malheiro, L.; Melo Beirão, J.; Meireles, A.; Pessoa, B. Real-world retropective comparison of 0.19 mg fluocinolone acetonide and 0.7 mg dexamethasone intravitreal implants for the treatment of diabetic macular edema in vitrectomized eyes. Clin. Ophthalmol. 2019, 13, 1751–1759. [Google Scholar] [CrossRef] [PubMed]
- McCuen, B.W., II; Bessler, M.; Tano, Y.; Chandler, D.; Machemer, R. The lack of toxicity of intravitreally administered triamcinolone acetonide. Am. J. Ophthalmol. 1981, 91, 785–788. [Google Scholar] [CrossRef]
- Jonas, J.B.; Hayler, J.K.; Panda-Jonas, S. Intravitreal injection of crystalline cortisone as adjunctive treatment of proliferative vitreoretinopathy. Br. J. Ophthalmol. 2000, 84, 1064–1067. [Google Scholar] [CrossRef]
- Jonas, J.B.; Hayler, J.K.; Sofker, A.; Panda-Jonas, S. Intravitreal injection of crystalline cortisone as adjunctive treatment of proliferative diabetic retinopathy. Am. J. Ophthalmol. 2001, 131, 468–471. [Google Scholar] [CrossRef]
- Jonas, J.B.; Sofker, A.; Degenring, R. Intravitreal triamcinolone acetonide as an additional tool in pars plana vitrecto¬my for proliferative diabetic retinopathy. Eur. J. Ophthalmol. 2003, 13, 468–473. [Google Scholar] [CrossRef]
- Kivilcim, M.; Peyman, G.A.; El-Dessouky, E.S.; Kazi, A.A.; Cheema, R.; Hegazy, H. Retinal toxicity of triamcinolone acetonide in silicone-filled eyes. Ophthalmic Surg. Lasers 2000, 31, 474–478. [Google Scholar]
- Perkins, S.; Gallemore, R.; Yang, C.; Guo, H.; Ashton, P.; Jaffe, G. Pharmacokinetics of fluocinolone/5- fluorouracil Cudrug in the Gas- Filled Eye. Retina 2000, 20, 514–519. [Google Scholar] [CrossRef]
- Jonas, J.B. Concentration of intravitreally injected triamcinolone acetonide in intraocular silicone oil. Br. J. Ophthalmol. 2002, 86, 1450–1451. [Google Scholar] [CrossRef][Green Version]
- Spitzer, M.S.; Kaczmarek, R.T.; Yoeruek, E.; Petermeier, K.; Wong, D.; Heimann, H.; Jaissle, G.B. The distribution, release kinetics and biocompatibility of triamcinolone injected and dispersed in silicone oil. Investig. Ophthalmol. Vis. Sci. 2009, 50, 2337–2343. [Google Scholar] [CrossRef]
- Flores-Villalobos, E.O.; Ramírez-Estudillo, J.A.; Robles-Contreras, A.; Oliva-Ramírez, J.L. Dexamethasone implant in silicone oil: In vitro behavior. Int. J. Retin. Vitr. 2018, 4, 24. [Google Scholar] [CrossRef] [PubMed]
- Bakri, S.J.; Alniemi, S.T. Fibrotic encapsulation of a dexamethasone intravitreal implant following vitrectomy and silicone oil for rhegmatogenous retinal detachment. Ophthalmic surgery, lasers and imaging retina. Ophthalmic Surg. Lasers Imaging Retin. 2014, 45, 243–245. [Google Scholar] [CrossRef] [PubMed]
- Dehghan, M.H.; Ahmadieh, H.; Soheilian, M.; Azarmina, M.; Moradian, S.; Ramezani, A.R.; Tavallal, A.; Naghibozakerin, J. Effect of oral prednisolone on visual outcomes and complications after scleral buckling. Eur. J. Ophthalmol. 2010, 20, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Lin, C.J.; Hwang, J.F.; Chen, S.N. Influence of systemic steroids on subretinal fluid after scleral buckle surgery for macula-off retinal detachment. Retina 2011, 31, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Koerner, F.; Koener-Stiefbold, U.; Garweg, J.G. Systemic corticosteroids reduce the risk of cellophane membranes after retinal detachment surgery: A prospective randomized placebo-controlled double-blind clinical trial. Graefes Arch. Clin. Exp. Ophthalmol. 2012, 250, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, K.; Motohashi, R.; Kotake, O.; Nakagawa, H.; Noma, H.; Shimura, M. Comparative effects of topical diclofenac and betamethasone on inflammation after vitrectomy and cataract surgery in various vitreoretinal diseases. J. Ocul. Pharmacol. Ther. 2016, 32, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Hagimura, N.; Lida, T.; Suto, K.; Kishi, S. Persistent foveal retinal detachment after successful regmatogenous retinal detachment surgery. Am. J. Ophthalmol. 2002, 133, 516–520. [Google Scholar] [CrossRef]
- Seo, J.H.; Woo, S.J.; Park, K.H.; Yu, Y.S.; Chung, H. Influence of persistent submacular fluid on visual outcome after successful scleral buckle surgery for macula-off retinal detachment. Am. J. Ophthalmol. 2008, 145, 915–922. [Google Scholar] [CrossRef]
- Benson, S.E.; Schlottmann, P.G.; Bunce, C.; Xing, W.; Charteris, D.G. Optical coherence tomography analysis of the macula after scleral buckle surgery for retinal detachment. Ophthalmology 2007, 114, 108–112. [Google Scholar] [CrossRef]
- Benson, S.E.; Ratclliffe, S.; Van Raders, P.; Schlottmann, P.G.; Khan, I.; Newsom, R.; Langford, R.M.; Charteris, D.G. A randomized comparison of parecoxib/valdecoxib and placebo for the prevention of cystoid macular edema after scleral buckling surgery. Retina 2009, 29, 387–394. [Google Scholar] [CrossRef]


{kind=link}
| Author (Year) | Study Design | Outcomes | Number of Eyes | Primary Treatment | Follow-Up | Main Results | Side Effects |
|---|---|---|---|---|---|---|---|
| Sharma T et al. (2005) [27] India | Prospective randomized study | 1. Anatomic primary success 2. Anatomic final outcomes 3. Functional success (≥2 lines improvement) | 20 RRDCD eyes: (4 eyes PPV; 16 PPV + SB) | GROUP 1 (11 eyes) oral prednisolone for 7 days before PPV GROUP 2 (9 eyes) early PPV | Group 1 11.7 months (mean) Group 2 mean 30.3 months (mean) | 1. Anatomic primary success 81.8% (group 1) vs. 66.7 (group 2) *** 2. Anatomic final success 100% (group 1) vs. 100% (group 2) *** 3. Functional outcomes: ≥ 2 lines improvement 72.73% (group 1) vs. 88.9% (group 2) *** | No specified |
| Sharma T et al. (2005) [27] India | Prospective randomized study | 1. Anatomic primary success 2. Anatomic final outcomes Functional success (≥2 lines improvement) | 20 RRDCD eyes (4 PPV; 16 PPV + SB) | GROUP 1 (11 eyes) oral prednisolone for 7 days before PPV GROUP 2 (9 eyes) early PPV | Group 1 11.7 months (mean) Group 2 30.3 months (mean) | 1. Anatomic primary success 81.8% (group 1) vs. 66.7% (group 2) *** 2. Anatomic final success 100% (group 1) vs. 100% (group 2) *** 3. Functional outcomes: ≥ 2 lines improvement 72.73% (group 1) vs. 88.9% (group 2) *** | No specified |
| Wei Y et al. [28] (2014) China | Retrospective clinical trial | 1. Retinal reattachment rate after single operation 2. BCVA improvement | 77 RRDCD eyes treated by PPV: GROUP A (31 eyes) Oral prednisolone for 3 to 7 days before PPV GROUP B (46 eyes) 40 mg peri-ocular injection on methyl-prednisolone for 3 to 7 days before surgery | GROUP A1 (18 eyes) PPV + SO GROUP A2 (13 eyes) PPV + C3F8 GROUP B1 (17 eyes) PPV + SO + IVT TA (4 mg) GROUP B2 (15 eyes) PPV + SO GROUP B3 (14 eyes) PPV + C3F8 | 12 months | 1. Retinal reattachment rate: • 77.4% (group A) vs. 73.9% (group B) *** • 83.3% (group A1) vs. 82.4% (group B1) *** • 69.2% (group A2) vs. 83.3% (group A1) *** • 73.3% (group B2) vs. 82.4% (group B1) *** • 64.3% (group B3) vs. 82.4 (group B1) *** 2. BCVA improvement: • 83.9% (group A) vs. 80.4% (group B) *** • 88.9% (group A1) vs. 88.2% (group B1) *** • 76.9% (group A2) vs. 88.9% (group A1) *** • 80.0% (group B2) vs. 88.2% (group B1) *** • 71.4% (group B3) vs. 88.2 (group B1) *** | Cataract development: • Group A = 5/31 yes • Group B = 10/46 Glaucoma: • Group A = 5/31 eyes • Group B = 11/46 eyes |
| Shen LJ et al. [29] (2016) China | Prospective study | 1. Pre-operative CD change 2.Blood sugar 3. Systemic and vitreous steroid levels 4. Macular thickness by OCT 5. BCVA change | 30 RRDCD eyes treated by PPV | - TA GROUP (16 eyes) ST injection of TA 5 days before surgery - DEX GROUP (14 eyes) 10 mg dexamethasone sodium phosphate EV once a day for 5 days prior to surgery | 6 months | TA GROUP vs. DEX GROUP (1) IOP elevation §: 3.29 ± 4.56 mmHg vs. 1.16 ± 1.60 mmHg ** (2) CD height decrease §: 3.55 ± 1.33 mm vs. 1.84 ± 1.5 mm ** (3) Increase of blood sugar level §: 5.75 ± 1.08 mmol vs. 9.01 ± 3.3 mmol/L ** (4) Steroid levels: Aqueous = 85.03 ± 72.92 ng/mL (5 days) vs. 89.57 ± 88.53 ng/mL (45 min) ** Vitreous = 17.95 ± 10.67 ng/mL (5 days) vs. 15.65 ± 10.87 ng/mL (45 min) ** (5) Suppressed plasma cortisol level = 51.9 ± 35.9 ng/mL vs. 8.35 ± 10.35 ng/mL ** (6) Macular thickness: 1 month = (13 eyes) 256 ± 66 vs. (10 eyes) 401 ± 96 ** 3-month = (11 eyes) 260 ± 68 vs. (10 eyes) 319 ±130 *** (7) BCVA change (LogMAR): 1 month = 1.33 ± 0.61 vs. 1.51 ± 0.56 3 month = 1.21 ± 0.59 vs. 1.38 ± 0.58 *** | • IOP elevation (>21 mmHg): - 4 eyes in TA group vs. 1 eye in DEX group • Retinal re-detachment: 1 eye in TA group |
| Alibet Y et al. [30] (2017) Switzerland, Ukraine | Prospective non-randomized study | 1. CBT by UBM 2. Ciliary body and choroidal reattachment 3. Sign on intraocular inflammation | 49 RRDCD eyes treated by PPV and pre-operative topical dexamethasone phosphate 0.1 and cyclopentolate hydrochloride | GROUP 1 (30 eyes) received 4 mg of TA IVT GROUP 2 (19 eyes) 4 mg of TA IVT + 0.4–0.8 mL of perfluorpropane | Non specified | 1. Total mean CBT value from baseline following IV injection = from 0.83 (0.09) mm to 0.65 (0.09) mm ** 2. 100% ciliary body and choroidal reattachment rate in both groups 3. No sign of intraocular inflammation (ciliary tenderness conjunctival injection and posterior synechiae) 1-2 days after IVTA | IOP increase from 6.9 (1.5) to 13.3 (0.9) mmHg 1–4 days after TA IVT. ** |
| Denwattana A et al. [31] (2017) Thailand | Retrospective study | 1. Retinal reattachment rate 2. BCVA improvement at 3 months 3. CD improvement prior to surgery | 76 RRDCD eyes treated by PPV or PPV + SB | GROUP A (37 eyes) no pre-operative steroids GROUP B (39 eyes) steroids for a median of 7 days prior to surgery: - 34 eyes: - oral prednisone 0.5–1mg/kg/day - 5 eyes: 20 mg in 2 eyes, 40 mg in 3 eyes of ST TA | 20 months (mean) | 1. Reattachment rate at 3 months: after 1 operation: 59% (group A) vs. 51% (group B) *** after 2 operation: 70% (group A) vs. 69% (group B) *** 2. BCVA improvement at 3 months: Group A from 2.54 to 2.01 LogMAR ** Group B from 2.53 to 1.97 LogMAR ** Group A vs. group B *** 3. Preoperative CD improvement: None = 70% group A vs. 18% group B ** Partial = 24% group A vs. 46% group B ** Complete = 6% group A vs. 36% group B ** | — |
| Yu Y et al. [32] (2019) China | Retrospective study | 1. Retinal reattachment rate 2. Factors influencing primary reattachment rate 3. Factors influencing final reattachment rate | 175 RRDCD eyes treated by PPV + preoperative variables | GROUP 1 (59 EYES) no pre-operative steroid treatment GROUP 2 (43 eyes) oral prednisolone 1 mg/kg/day for 5 to 7 days before surgery GROUP 3 (32 eyes) peri-ocular injection of 20 mg methylprednisolone every other day for 5 to 7 days before surgery GROUP 4 (41 eyes) pre-operative 4 mg TA IVT for 5 to 7 days before surgery | — | 1. Retinal reattachment rate: - Overall = 72.57% (primary reattachment°) vs. 89.14% (final reattachment) - Group 1 (69.49%) vs. Group 2 (74.42%) ** - Group 4 vs. Group 1 ** (OR = 4.60) 2. Baseline factors influencing primary reattachment rate: - Age = primary reattachment increase with increasing age ** (OR = 1.03). - PVR grade C vs. A-B (OR = 0.31) ** PVR grade D vs. PVR A-B (OR = 0.03) ** - Steroid treatment: Group 1 (69.49%) vs. group 2 (74.42%) *** Group 1 (69.49%) vs. group 3 (62.50%) *** Group 1 (69.49%) vs. group 4 (82.93%) ** 3. Baseline factors significantly influencing final reattachment rate: - Age = final reattachment increase with increasing age (OR = 1.05) ** | — |
| Author, Year | Study Design | Outcomes | Number of Eyes | Primary Treatment | Follow-Up | Main Results | Side Effects |
|---|---|---|---|---|---|---|---|
| Munir WM et al. [40] (2005) United States of America | Retrospective study | 1. Visual acuity 2. IOP changes | 13 RRD eyes + PDR + severe PVR | PPV + SO + IVTA (4 mg) | Mean = 4.7 months (range 1–15) | 1. Visual acuity: - Improvements = 4 eyes (2 lines) - Worsened = 4 eyes - Stable = 5 eyes 2. IOP changes: From 10.8 ± 6.22 mmHg (pre-operative) to 9.6 ± 3.86 mmHg (last follow-up) *** | — |
| Cheema RA et al. [41] (2007) United Kingdom | Interventional non comparative prospective study | 1. Retinal reattachment rate 2. BCVA improvement | 24 RRD eyes + PVR grade ≥ C2 | PPV + membrane peeling + SO + IVTA (4 mg) | 6 months | 1. Reattachment rate: 87% 2. BCVA improvement (p < 0.5) | — |
| Admaideh H et al. [42]36 (2008) Iran | Prospective randomized clinical trial | 1. Retinal reattachment rate 2. BCVA improvement 3. Rate of recurrent PVR 4. Redetachment rate 5. Macular pucker | 75 RRD eyes + PVR grade C treated by PPV + SO | GROUP 1 (38 eyes) IVTA GROUP 2 (37 eyes) no IVTA (4 mg) | 6 months | 1. Retinal reattachment rate:84.2% (group 1) vs. 78.4% (group 2) *** 2. BCVA improvement (logMAR)^: Group 1 from 2.1 ± 0.7 to 1.2 ± 0.7 ** Group 2 from 2.4 ± 0.6 to 1.4 ± 0.6 ** Final BCVA group 1 vs. group 2 *** 3. Rate of recurrent PVR grade C: 28.9% (group 1) vs. 29.7% (group 2) *** 4. Reattachment rate: 15.8% (group 1) vs. 21.6% (group 2) *** 5. Macular pucker: 21.1 (group 1) vs. 35.1 (group 2) *** | Pseudohypopyon = 2 eyes. Rise of IOP^: - Group 1 from 9.5 ± 5.8 vs. 14.7 ± 5.1 mmHg ** - Group 2 from 11.2 ± 7.2 to 16.4 ± 5.9 mmHg ** - Group 1 vs. group 2 *** |
| Yamakiri K et al. [43] (2008) Japan | Multi-center prospective controlled clinical trial | 1. Changes of visual acuity 2. Post-operative complications (ERM, IOP increase) 3. Additional surgery | 774 eyes treated by PPV (various disease) | GROUP 1 (391 eyes) TA-assisted PPV (20.5% RRD) GROUP 2 (383 eyes) conventional PPV (20.1% RRD) | 1 year | 1. Changes of visual acuity: - Improvement Group 1 (322 out of 391 eyes) vs. Group 2 (312 out of 383 eyes) *** - DeteriorationGroup 1 (48 out of 391 eyes) vs. Group 2 (26 out of 383 eyes) *** 2. Post-operative complications: Group 1 vs. Group 2 *** 3. Additional surgery: Group 1 vs. Group 2 *** | — |
| Chen et al. (2011) [44] China | Retrospective interventional case series | 1. Retinal reattachment rate BCVA improvement (≥ 0.3 logMAR) | 32 eyes with PVR grade C or D secondary to RRD 5 eyes with PVR grade C or D secondary to ocular trauma | PPV + SO + membrane peeling + IVT TA (2 mg) | Mean = 22.9 ± 9.6 months | 1. Reattachment rate = 97.3% 2. BCVA (logMAR): - 1.76 ± 0.56 (baseline) vs. 0.87 ± 0.56 (last follow-up) ** - 1.30 ± 0.47 (before SO removal) vs. 0.87 ± 0.56 (last follow-up) ** - Improved BCVA = 83.8% - Unchanged in BCVA = 13.5% - Decreased in BCVA = 2.7%. | • IOP > 21 mmHg: 1 eye • Hypopyon: 1 eye Cataract: 2 eyes |
| Reibaldi M et al. [45] (2013) Italy | Case report | 1. PVR development 2. BCVA improvement | 1 RRD eye + PVR grade B treated by SB | DEX implant at the end of SB | 9 months | 1. PVR development: No PVR sign 2. BCVA improvement: from hand-motion to 0.2 LogMAR | No rise of IOP |
| Mirshahi et al. (2014) [46] Iran | Prospective consecutive case series | 1. BCVA improvement 2. CME rate 3. Incidence of persistence SRF 4. Extent of detachment 5. Post-operative inflammation (conjunctival injection) | 62 macula off-RRD eyes treated by SB | GROUP 1 (29 EYES) received IVT TA (2 mg) at the end of SB GROUP 2 (33 eyes) received IVT NaCl at the end of SB | 1 week, 1, 2, 3 month | 1. BCVA improvement: 1. 1 week and 1–2 month group 1 vs. group 2 *** 2. 3 month group 1 > group 2 ** 2. CME rate: group 1 (20,75%) vs. group 2 (33.3%) *** 3. Incidence of persistence SRF: Group 1 (34%) vs. group 2 (45%) *** 4. Extent of detachment: group 1 vs. group 2 *** 5. Post-operative inflammation (conjunctival injection): group 1 (4 eyes-13%) vs. group 2 (10 eyes - 30%) ** There was no correlation between the incidence of persistent SRF and extent of the detachment in both groups (p = 0.83) | - Rise of IOP > 21 mmHg in 4 eyes of group 1 No cataract progression |
| Sherif M and Wolfensberger TJ. [47] (2017) Switzerland | Retrospective review | 1. BCVA improvement 2. Stable retinal reattachment with SO 3. Stable retinal reattachment with removal of SO | 5 recurrent RRD + PVR stage C + retinal edema | PPV + membrane peeling+ retinectomy+ DEX implant + 5500cs SO | 8.8 ± 6.4 months under SO 4–8 months in 3 of the 5 eyes | 1. BCVA improvement patient 1: from 0.15 to 0.32 logMAR patient 2: from HM to 0.05 logMAR patient 3: from HM to 0.1 logMAR patient 4: from HM to 0.2 logMAR patient 5: from CF to 0.05 logMAR 2. Stable retinal reattachment with SO: 5 out of 5 eyes 3. Stable retinal reattachment with removal of SO 3 out of 5 eyes | - |
| Banerjee PJ at al. [48] (2017) United Kingdom | Prospective randomized controlled clinical trial | 1. Stable retinal reattachment with removal of SO without additional surgical intervention at 6 months 2. Final VA and proportion of patients achieving a VA of 55 letters 3. Macular findings at 6 months 4. Development PVR recurrence 5. Retinal reattachment: complete and posterior (post-equatorial) 6. Quality of life | 140 RRD eyes | GROUP 1 (70 eyes): PPV + SO GROUP 2 (70 eyes): PPV + SO + DEX implant | 2 years | 1. Stable retinal reattachment with removal of SO without additional surgical intervention at 6 months: 42% (group 1) vs. 49% (group 2) *** 2. Final VA: - ETDRS letters at 6 months: group 1 (40.2 letters - SD = 21.1) vs. group 2 (38.3 letters - SD = 23.7) *** - Proportion of patients achieving a visual acuity of 55 ETDRS letters or better: group 1 (24%) vs. group 2 (30%) *** 3. Macular findings at 6 months: - Macular edema group 1 (67.2%) vs. group 2 (42.7%) ** - Median foveal thickness and macular volume group 1 (365 μ and 9.23 mm3) vs. group 2 (297 μ and 8.85 mm3) - Proportion of eyes with foveal thickness ≧ 300 μ group 1 (67.7%) vs. group 2 (47.6%) ** 4. Development PVR recurrence: group 1 (59%) vs. group 2 (57%) 5. Retinal reattachment: - Complete group 1 (62.3%) vs. group 2 (53.6%) - Posterior group 1 (69.6%) vs. group 2 (69.7%) 6. Quality of life: no difference using Mean Social Functioning 36-point Questionnaire and Visual Functioning 25-point Questionnaire: no differences between the 2 treatment groups | 1. Hypotony (at least 1 episode): group 1 (24.3%) vs. group 2 (20%) 2. IOP (at least 1 episode): group 1 (31.4%) vs. group 2 (45.7%) 3. Macular pucker/epiretinal membranes: group 1 (58.6%) vs. group 2 (57.1%) 4. Patients undergoing cataract surgery: group 1 (86.1%) vs. group 2 (75.8%) 5. Tractional retinal detachment: group 1 (19%) vs. group 2 (22%) |
| Cho AR Et Al. [49] (2019) Korea | Retrospective interventional case series | 1. BCVA 2. Retinal attachment rate and maintenance | 7 eyes—AD patients with RD | PPV+ SO + DEX implant | 15–37 months | 1. BCVA maintained in 5 out of 7 eyes. 2. Retinal attachment rate and maintenance: 100%. | - 1 eye required additional procedure for a recurrent inferior RD at 2 months. - Uveitis: 1 eye. - IOP > 21 mmHg: surgical iridotomy (1 eye), Ahmed valve (2 eyes) topical treatment (3 eyes). - PVR recurrence: 1 eye who had history of multiple PPV - 1 eye repeated DEX implants injection for CME |
| Reibaldi M et al. [50] (2019) Italy | Prospective randomized multicenter double-blind trial | 1. Complete response (absence of PONV: no nausea, no vomiting, no retching, no use of anti-emetic rescue medication) 2. Severity standardized score of PONV (higher intensity) 3. Postoperative pain | 1287 eyes affected by various disease treated by PPV GROUP A = 181 RRD eyes GROUP B = 183 RRD eyes GROUP C = 187 RRD eyes GROUP D = 190 RRD eyes | GROUP A (321 eyes) Placebo (IV at the start and 15 min before the end of surgery) GROUP B (316 eyes) ondansetron (4 mg diluted to 10 mL IV 15 min before the end of surgery) + placebo (at the start of surgery) GROUP C (328 eyes) DEX (4 mg diluted to 10 mL IV at the start of surgery) + placebo (15 min before the end of surgery) GROUP D (322 eyes) DEX (4 mg diluted to 10 mL IV at the start of surgery) + ondansetron (4 mg diluted to 10 mL IV 15 min before the end of surgery) | 24 h after surgery | 1. Complete response (absence of PONV: no nausea, no vomiting, no retching, no use of anti-emetic rescue medication): GROUP D (95.96%, 309/322 patients) vs. GROUP B (80.38%, 254/316 patients), GROUP C (80.79%, 265/328 patients), GROUP A (71.96%, 231/321 patients) ** GROUP B (80.38%, 254/316 patients), GROUP C (80.79%, 265/328 patients) vs. GROUP A (71.96%, 231/321 patients) ** GROUP B (80.38%, 254/316 patients) vs. GROUP C (80.79%, 265/328 patients) *** 2. Severity standardized score of PONV (higher intensity): GROUP A > GROUP B GROUP A > GROUP C GROUP A >> GROUP D ** GROUP B vs. GROUP C *** Postoperative pain *** | No serious non-ocular adverse events CD: GROUP A (4) GROUP B (3) GROUP C (3) GROUP D (2) IOP ≥ 30 mmHg: GROUP A (12) GROUP B (8) GROUP C (9) GROUP D (8) Hypotony ≤ 6 mmHg: GROUP A (4) GROUP B (6) GROUP C (3) GROUP D (7) Suprachoroidal hemorrhage: GROUP A (2) GROUP B (1) GROUP C (1) |
| GROUP D (322 eyes) DEX (4 mg diluted to 10 mL IV at the start of surgery) + ondansetron (4 mg diluted to 10 mL IV 15 min before the end of surgery) | 3. Postoperative pain *** | RD: GROUP A (1) GROUP C (1) Vitreous hemorrhage: GROUP A (2) GROUP B (2) GROUP C (5) GROUP D (3) |
| Author. Year | Study Design | Outcomes | Number of Eyes | Primary Treatment | Follow-Up | Main Results | Side Effects |
|---|---|---|---|---|---|---|---|
| Dehghan MH et AL. [73] (2009) Iran | Randomized double-blind placebo-controlled trials | 1. BCVA logMar 2. Retinal redetachment 3. Macular edema 4. PVR | 52 RRD eyes + PVR grade a or B treated by SB | GROUP 1 (25 eyes) post-operative oral prednisolone for 10 days GROUP 2 (27 eyes) placebo | 6 months | 1. BCVA logMar - Final group 1 (0.62 ± 0.39) vs. group 2 (0.78 ± 0.58) *** - Difference between preoperative and postoperative: group 1 (0.85 ± 0.62) vs. group 2 (0.65 ± 0.61) *** 2. Macular edema within 6 weeks: group 1 (12%) vs. group 2 (18.5) *** 3. PVR within 6 months: group 1 (4%) vs. group 2 (11.1%) *** | CD (within 1 week): group 1 (16%) vs. group 2 (11.1%) *** |
| Wu JS et al. [74] (2011) Taiwan | Prospective interventional study | 1. SRF incidence and duration 2. BCVA (logMar) | 60 RRD eyes treated by SB | GROUP 1 (30 eyes) Oral prednisone for 3 days post-SB: - GROUP 1A (11 eyes) = 0.5 mg/kg - GROUP 1B (19 eyes) = 1 mg/kg GROUP 2 (30 eyes) No oral prednisolone post-SB | 1 year | 1. SRF - Incidence (6 weeks after operation): group 1 (56.6%) vs. group 2 (80%) group 1A (54.5%) vs. group 1B (57.9%) *** - Duration days: group 1 (218.1 ± 122.1 days) vs. group 2 (286.5 ± 141 days) ** group 1A (188.0 ± 114.1) vs. group 1B (237.2 ± 128.5) *** 2. BCVA (logMar) - Final (12 months): group 1 (0.27 ± 0,28) vs. group 2 (0.29 ± 0.31) *** group 1A (0.38 ± 0.36) vs. group 1B (0.20 ± 0.19) *** - BCVA improvement: group 1 (1.38 ± 1.05) vs. group 2 (0.74 ± 0.78) ** group 1A (1.47 ± 0.94) vs. group 1B (1.22 ± 1.24) *** | No systemic complications |
| Koemer F et al. [75] (2012) Switzerland | Prospective randomized, placebo, controlled, double blind clinical trial | 1. PVR stage B incidence 2. Cellophane appearance 3. Retinal rigidity 4. Epiretinal membranes 5. PVR stage C | 220 RRD eyes treated by SB | GROUP 1 (110 eyes) Oral prednisolone after SB GROUP 2 (110 eyes) Placebo after SB | 30, 90, 180 days | 1. PVR stage B incidence: - 30 days group 1 (26.4%) vs. group 2 (40.4%) ** - 90 days group 1 (25.2%) vs. group 2 (45.5%) ** - 180 days group 1 (22.5%) vs. group 2 (45.7) ** 2. Cellophane appearance: group 1 vs. group 2 *** 3. Retinal rigidity: group 1 vs. group 2 *** 4. Epiretinal membranes: group 1 vs. group 2 *** 5. PVR grade C: group 1 vs. group 2 *** | — |
| Ben YS et al. [7] (2016) Tunisia | Prospective study | 1. Intensity of post-operative pain by VAS 2. ACAF 3. IOP | 40 RRD eyes | GROUP 1 (28 eyes) treated by SB: - GROUP 1A = 13 eyes (46.4%) topical dexamethasone 4 times daily for 28 days after surgery - GROUP 1B = 15 eyes (53.6%) topical diclofenac sodium 0,1% 3 times daily for 28 days after surgery GROUP 2 (12 eyes) treated by PPV: - GROUP 2A = 6 eyes (50%) dexamethasone - GROUP 2B = 6 eyes (50%) diclofenac | 7. 14. 28. 90 (days) | 1. Intensity of post-operative pain: GROUP1 - 7 days = group 1A (2.48 ± 0.94) vs. group 1B (1.77 ±0,87) ** - 14 days = group 1A (1.06 ± 0.45) vs. group 1B (0.43 ± 0.63) ** - 28 days = group 1A (0.5 ± 0.35) vs. group 1B (0.26 ± 0.18) ** - 90 days = group 1A vs. group 1B *** GROUP 2 - 7 days = group 2A (1.92 ± 0.87) vs. group 2B (1.73 ± 0.78) ** - 14 days = group 2A (0.82 ± 0.39) vs. group 2B (0.28 ± 0.34) ** - 28 days = group 2A (0.4 ± 0.19) vs. group 2B (0.14 ± 1.14) ** - 90 days = group 2A vs. group 2B *** 2. ACAF (ph/ms): group 1A vs. group 1B *** group 2A vs. group 2B *** 3. IOP: group 1A vs. group 1B *** group 2A vs. group 2B *** | No post-operative complications |
| Yasuda K et al. [76] (2016) Japan | Prospective interventional study | 1. ACAF 2. IOP 3. BCVA 4. Total OT 5. Dynamic maxPOI changes 6. maxPOI | 200 eyes with CATARACT + MH/ERM/DME/RRD + SF6 | Sutureless cataract surgery + PPV: - GROUP 1: 106 eyes treated by topic post-operative diclofenac 0.1% (18 RRD) - GROUP 2: 85 topic post-operative betamethasone 0.1% (18 RRD) | 12 weeks | 1. ACAF: Group 1 = RRD (10.3 ± 3.5) vs. other disease *** Group 2 = RRD (11.9 ± 6.4) vs. other disease *** Group 1 vs. Group 2 *** 2. Pre-operative IOP: Group 1 = RRD (12.6 ± 2.8) < other disease ** Group 2 = RRD (12.6 ± 4.2) < other disease ** Post-operative IOP: RRD = Group 2 > Group 1 ** 3. BCVA: Group 1 vs. Group 2 *** 4. Total OT: Group 1 = RRD (40.9 ± 6.8) > other disease ** Group 2 = RRD (44.1 ± 12.4) > other disease ** Group 1 vs. Group 2 *** 5. Dinamic maxPOI changes:Group 1 vs. Group 2 *** 6. RRD maxPOI: significantly correlated with the number of endophotocoagulations, total OT in group 1 and indentation during PPV in group 1 and 2 | — |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonfiglio, V.; Reibaldi, M.; Macchi, I.; Fallico, M.; Pizzo, C.; Patane, C.; Russo, A.; Longo, A.; Pizzo, A.; Cillino, G.; et al. Preoperative, Intraoperative and Postoperative Corticosteroid Use as an Adjunctive Treatment for Rhegmatogenous Retinal Detachment. J. Clin. Med. 2020, 9, 1556. https://doi.org/10.3390/jcm9051556
Bonfiglio V, Reibaldi M, Macchi I, Fallico M, Pizzo C, Patane C, Russo A, Longo A, Pizzo A, Cillino G, et al. Preoperative, Intraoperative and Postoperative Corticosteroid Use as an Adjunctive Treatment for Rhegmatogenous Retinal Detachment. Journal of Clinical Medicine. 2020; 9(5):1556. https://doi.org/10.3390/jcm9051556
Chicago/Turabian StyleBonfiglio, Vincenza, Michele Reibaldi, Iacopo Macchi, Matteo Fallico, Corrado Pizzo, Clara Patane, Andrea Russo, Antonio Longo, Alessandra Pizzo, Giovanni Cillino, and et al. 2020. "Preoperative, Intraoperative and Postoperative Corticosteroid Use as an Adjunctive Treatment for Rhegmatogenous Retinal Detachment" Journal of Clinical Medicine 9, no. 5: 1556. https://doi.org/10.3390/jcm9051556
APA StyleBonfiglio, V., Reibaldi, M., Macchi, I., Fallico, M., Pizzo, C., Patane, C., Russo, A., Longo, A., Pizzo, A., Cillino, G., Cillino, S., Vadalà, M., Rinaldi, M., Rejdak, R., Nowomiejska, K., Toro, M. D., Avitabile, T., & Ortisi, E. (2020). Preoperative, Intraoperative and Postoperative Corticosteroid Use as an Adjunctive Treatment for Rhegmatogenous Retinal Detachment. Journal of Clinical Medicine, 9(5), 1556. https://doi.org/10.3390/jcm9051556