Reproducibility of Ablated Volume Measurement Is Higher with Contrast-Enhanced Ultrasound than with B-Mode Ultrasound after Benign Thyroid Nodule Radiofrequency Ablation—A Preliminary Study

 , , ,
, , ,  , and
, and 
Abstract
1. Introduction
2. Experimental Section
2.1. Patients
2.2. Preablation Assessment and Procedure
2.3. Follow-Up Examinations
2.4. Radiofrequency-Ablated Volume Assessment
2.5. Statistical Analysis
3. Results
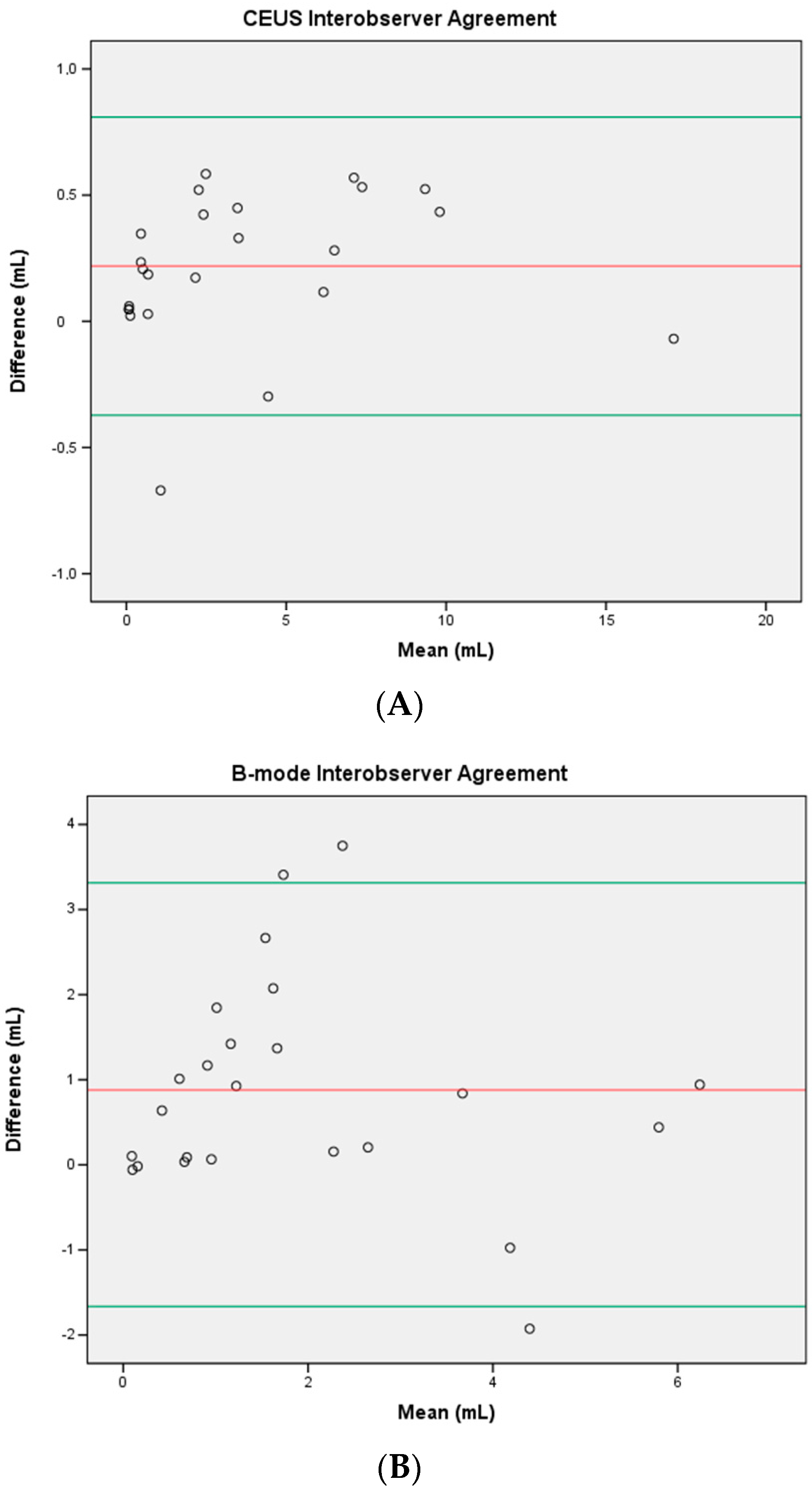
3.1. Inter-observer Agreement
3.2. Intra-observer Agreement
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Gharib, H.; Papini, E. Thyroid Nodules: Clinical Importance, Assessment, and Treatment. Endocrinol. Metab. Clin. North Am. 2007, 36, 707–735. [Google Scholar] [CrossRef] [PubMed]
- Guth, S.; Theune, U.; Aberle, J.; Galach, A.; Bamberger, C.M. Very High Prevalence of Thyroid Nodules Detected by High Frequency (13 MHz) Ultrasound Examination. Eur. J. Clin. Invest. 2009, 39, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Papini, E.; Pacella, C.M.; Hegedus, L. Diagnosis of Endocrine Disease: Thyroid Ultrasound (US) and US-Assisted Procedures: From the Shadows into an Array of Applications. Eur. J. Endocrinol. 2014, 170, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Filetti, S.; Durante, C.; Torlontano, M. Nonsurgical Approaches to the Management of Thyroid Nodules. Nat. Clin. Pract. Endocrinol. Metab. 2006, 2, 384–394. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Baek, J.H.; Chung, J.; Ha, E.J.; Kim, J.H.; Lee, Y.H.; Lim, H.K.; Moon, W.J.; Na, D.G.; Park, J.S.; et al. Ultrasonography Diagnosis and Imaging-Based Management of Thyroid Nodules: Revised Korean Society of Thyroid Radiology Consensus Statement and Recommendations. Korean J. Radiol. 2016, 17, 370–395. [Google Scholar] [CrossRef]
- Kim, J.; Baek, J.H.; Lim, H.K.; Ahn, H.S.; Baek, S.M.; Choi, Y.J.; Choi, Y.J.; Chung, S.R.; Ha, E.J.; Hahn, S.Y.; et al. 2017 Thyroid Radiofrequency Ablation Guideline: Korean Society of Thyroid Radiology. Korean J. Radiol. 2018, 19. [Google Scholar] [CrossRef]
- Baek, J.H.; Lee, J.H.; Valcavi, R.; Pacella, C.M.; Rhim, H.; Na, D.G. Thermal Ablation for Benign Thyroid Nodules: Radiofrequency and Laser. Korean J. Radiol. 2011, 12, 525–540. [Google Scholar] [CrossRef]
- Mauri, G.; Gennaro, N.; Lee, M.K.; Baek, J.H. Laser and Radiofrequency Ablations for Benign and Malignant Thyroid Tumors. Int. J. Hyperth. 2019, 36, 13–20. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Müller, T.; Bojunga, J.; Dong, Y.; Mauri, G.; Radzina, M.; Dighe, M.; Cui, X.W.; Grünwald, F.; Schuler, A.; et al. Statement and Recommendations on Interventional Ultrasound as a Thyroid Diagnostic and Treatment Procedure. Ultrasound Med. Biol. 2018, 44, 14–36. [Google Scholar] [CrossRef]
- Papini, E.; Pacella, C.M.; Solbiati, L.A.; Achille, G.; Barbaro, D.; Bernardi, S.; Cantisani, V.; Cesareo, R.; Chiti, A.; Cozzaglio, L.; et al. Minimally-Invasive Treatments for Benign Thyroid Nodules: A Delphi-Based Consensus Statement from the Italian Minimally-Invasive Treatments of the Thyroid (MITT) Group. Int. J. Hyperth. 2019, 36, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.K.; Lee, J.H.; Ha, E.J.; Sung, J.Y.; Kim, J.K.; Baek, J.H. Radiofrequency Ablation of Benign Non-Functioning Thyroid Nodules: 4-Year Follow-up Results for 111 Patients. Eur. Radiol. 2013, 23, 1044–1049. [Google Scholar] [CrossRef] [PubMed]
- Sim, J.S.; Baek, J.H.; Lee, J.; Cho, W.; Jung, S.I. Radiofrequency Ablation of Benign Thyroid Nodules: Depicting Early Sign of Regrowth by Calculating Vital Volume. Int. J. Hyperth. 2017, 33, 905–910. [Google Scholar] [CrossRef] [PubMed]
- Valcavi, R.; Riganti, F.; Bertani, A.; Formisano, D.; Pacella, C.M. Percutaneous Laser Ablation of Cold Benign Thyroid Nodules: A 3-Year Follow-up Study in 122 Patients. Thyroid 2010, 20, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Mauri, G.; Pacella, C.M.; Papini, E.; Solbiati, L.; Goldberg, S.N.; Ahmed, M.; Sconfienza, L.M. Image-Guided Thyroid Ablation: Proposal for Standardization of Terminology and Reporting Criteria. Thyroid 2019, 29, 611–618. [Google Scholar] [CrossRef]
- Sim, J.S.; Baek, J.H.; Cho, W. Initial Ablation Ratio: Quantitative Value Predicting the Therapeutic Success of Thyroid Radiofrequency Ablation. Thyroid 2018, 28, 1443–1449. [Google Scholar] [CrossRef]
- Sidhu, P.; Cantisani, V.; Dietrich, C.; Gilja, O.; Saftoiu, A.; Bartels, E.; Bertolotto, M.; Calliada, F.; Clevert, D.-A.; Cosgrove, D.; et al. The EFSUMB Guidelines and Recommendations for the Clinical Practice of Contrast-Enhanced Ultrasound (CEUS) in Non-Hepatic Applications: Update 2017 (Short Version). Ultraschall der Medizin - Eur. J. Ultrasound 2018, 39, 154–180. [Google Scholar]
- Meloni, M.F.; Andreano, A.; Zimbaro, F.; Lava, M.; Lazzaroni, S.; Sironi, S. Contrast Enhanced Ultrasound: Roles in Immediate Post-Procedural and 24-h Evaluation of the Effectiveness of Thermal Ablation of Liver Tumors. J. Ultrasound 2012, 15, 207–214. [Google Scholar] [CrossRef]
- Prada, F.; Del Bene, M.; Fornaro, R.; Vetrano, I.G.; Martegani, A.; Aiani, L.; Sconfienza, L.M.; Mauri, G.; Solbiati, L.; Pollo, B.; et al. Identification of Residual Tumor with Intraoperative Contrast-Enhanced Ultrasound during Glioblastoma Resection. Neurosurg. Focus 2016, 40. [Google Scholar] [CrossRef]
- Mauri, G.; Porazzi, E.; Cova, L.; Restelli, U.; Tondolo, T.; Bonfanti, M.; Cerri, A.; Ierace, T.; Croce, D.; Solbiati, L. Intraprocedural Contrast-Enhanced Ultrasound (CEUS) in Liver Percutaneous Radiofrequency Ablation: Clinical Impact and Health Technology Assessment. Insights Imaging 2014, 5, 209–216. [Google Scholar] [CrossRef]
- Russ, G.; Bonnema, S.J.; Erdogan, M.F.; Durante, C.; Ngu, R.; Leenhardt, L. European Thyroid Association Guidelines for Ultrasound Malignancy Risk Stratification of Thyroid Nodules in Adults: The EU-TIRADS. Eur. Thyroid J. 2017, 6, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Chung, H.W.; Baek, J.H.; Lee, J.S.; Lee, S.H.; Lee, M.H.; Shin, M.J. Ultrasonography-Guided Radiofrequency Ablation of Malignant Musculoskeletal Soft-Tissue Tumors Using the “Moving-Shot” Technique at a Single-Institution Experience. Ultrasound Q. 2014, 30, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Shyn, P.B.; Mauri, G.; Alencar, R.O.; Tatli, S.; Shah, S.H.; Morrison, P.R.; Catalano, P.J.; Silverman, S.G. Percutaneous Imaging-Guided Cryoablation of Liver Tumors: Predicting Local Progression on 24-Hour MRI. AJR. Am. J. Roentgenol. 2014, 203, W181–W191. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Shyn, P.B.; Tatli, S.; Sahni, V.A.; Sadow, C.A.; Forgione, K.; Mauri, G.; Morrison, P.R.; Catalano, P.J.; Silverman, S.G. PET/CT-Guided Percutaneous Liver Mass Biopsies and Ablations: Targeting Accuracy of a Single 20 s Breath-Hold PET Acquisition. Clin. Radiol. 2014, 69, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Mauri, G.; Nicosia, L.; Varano, G.M.; Bonomo, G.; Della Vigna, P.; Monfardini, L.; Orsi, F. Tips and Tricks for a Safe and Effective Image-Guided Percutaneous Renal Tumour Ablation. Insights Imaging 2017, 8, 357–363. [Google Scholar] [CrossRef]
- Pacella, C.M.; Patelli, G.; Iapicca, G.; Manenti, G.; Perretta, T.; Ryan, C.P.; Esposito, R.; Mauri, G. Transperineal Laser Ablation for Percutaneous Treatment of Benign Prostatic Hyperplasia: A Feasibility Study. Results at 6 and 12 Months from a Retrospective Multi-Centric Study. Prostate Cancer Prostatic Dis. 2019. [Google Scholar] [CrossRef]
- de Baere, T.; Tselikas, L.; Gravel, G.; Hakime, A.; Deschamps, F.; Honoré, C.; Mir, O.; Lecesne, A. Interventional Radiology: Role in the Treatment of Sarcomas. Eur. J. Cancer 2018, 94, 148–155. [Google Scholar] [CrossRef]
- Forner, A.; Llovet, J.M.; Bruix, J. Hepatocellular Carcinoma. Lancet 2012, 379, 1245–1255. [Google Scholar] [CrossRef]
- Ljungberg, B.; Bensalah, K.; Canfield, S.; Dabestani, S.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; Lam, T.; Marconi, L.; Merseburger, A.S.; et al. EAU Guidelines on Renal Cell Carcinoma: 2014 Update. Eur. Urol. 2015, 67, 913–924. [Google Scholar] [CrossRef]
- Monfardini, L.; Gennaro, N.; Della Vigna, P.; Bonomo, G.; Varano, G.; Maiettini, D.; Bonello, L.; Solbiati, L.; Orsi, F.; Mauri, G. Cone-Beam CT-Assisted Ablation of Renal Tumors: Preliminary Results. Cardiovasc. Intervent. Radiol. 2019, 42, 1718–1725. [Google Scholar] [CrossRef]
- Monfardini, L.; Orsi, F.; Caserta, R.; Sallemi, C.; Della Vigna, P.; Bonomo, G.; Varano, G.; Solbiati, L.; Mauri, G. Ultrasound and Cone Beam CT Fusion for Liver Ablation: Technical Note. Int. J. Hyperth. 2018, 0, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Bai, H.X.; Chan, L.; Su, C.; Zhang, P.J.; Yang, L.; Zhang, Z. Sublobar Resection Compared with Stereotactic Body Radiation Therapy and Ablation for Early Stage Non–Small Cell Lung Cancer: A National Cancer Database Study. J. Thorac. Cardiovasc. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Mauri, G.; Cova, L.; Ierace, T.; Baroli, A.; Di Mauro, E.; Pacella, C.M.; Goldberg, S.N.; Solbiati, L. Treatment of Metastatic Lymph Nodes in the Neck from Papillary Thyroid Carcinoma with Percutaneous Laser Ablation. Cardiovasc. Intervent. Radiol. 2016, 39, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Pacella, C.M.; Mauri, G.; Achille, G.; Barbaro, D.; Bizzarri, G.; De Feo, P.; Di Stasio, E.; Esposito, R.; Gambelunghe, G.; Misischi, I.; et al. Outcomes and Risk Factors for Complications of Laser Ablation for Thyroid Nodules: A Multicenter Study on 1531 Patients. J. Clin. Endocrinol. Metab. 2015, 100, 3903–3910. [Google Scholar] [CrossRef]
- Trimboli, P.; Castellana, M.; Sconfienza, L.M.; Virili, C.; Pescatori, L.C.; Cesareo, R.; Giorgino, F.; Negro, R.; Giovanella, L.; Mauri, G. Efficacy of Thermal Ablation in Benign Non-Functioning Solid Thyroid Nodule: A Systematic Review and Meta-Analysis. Endocrine 2020, 67, 35–43. [Google Scholar] [CrossRef]
- Kim, J.H.; Yoo, W.S.; Park, Y.J.; Park, D.J.; Yun, T.J.; Choi, S.H.; Sohn, C.H.; Lee, K.E.; Sung, M.W.; Youn, Y.K.; et al. Efficacy and Safety of Radiofrequency Ablation for Treatment of Locally Recurrent Thyroid Cancers Smaller than 2 Cm. Radiology 2015, 276, 909–918. [Google Scholar] [CrossRef]
- Cesareo, R.; Palermo, A.; Benvenuto, D.; Cella, E.; Pasqualini, V.; Bernardi, S.; Stacul, F.; Angeletti, S.; Mauri, G.; Ciccozzi, M.; et al. Efficacy of Radiofrequency Ablation in Autonomous Functioning Thyroid Nodules. A Systematic Review and Meta-Analysis. Rev. Endocr. Metab. Disord. 2019, 20, 37–44. [Google Scholar] [CrossRef]
- Mauri, G.; Cova, L.; Monaco, C.G.; Sconfienza, L.M.; Corbetta, S.; Benedini, S.; Ambrogi, F.; Milani, V.; Baroli, A.; Ierace, T.; et al. Benign Thyroid Nodules Treatment Using Percutaneous Laser Ablation (PLA) and Radiofrequency Ablation (RFA). Int. J. Hyperth. 2017, 33, 295–299. [Google Scholar] [CrossRef]
- Mauri, G.; Cova, L.; De Beni, S.; Ierace, T.; Tondolo, T.; Cerri, A.; Goldberg, S.N.; Solbiati, L. Real-Time US-CT/MRI Image Fusion for Guidance of Thermal Ablation of Liver Tumors Undetectable with US: Results in 295 Cases. Cardiovasc. Intervent. Radiol. 2015, 38, 143–151. [Google Scholar] [CrossRef]
- Mauri, G.; Nicosia, L.; Della vigna, P.; Varano, G.M.; Maiettini, D.; Bonomo, G.; Giuliano, G.; Orsi, F.; Solbiati, L.; De fiori, E.; et al. Percutaneous Laser Ablation for Benign and Malignant Thyroid Diseases. Ultrasonography 2019, 38, 25–36. [Google Scholar] [CrossRef]
- Liu, W.; Zhou, P.; Zhao, Y.; Tian, S.; Wu, X. Superb Microvascular Imaging Compared with Contrast-Enhanced Ultrasound for Assessing Laser Ablation Treatment of Benign Thyroid Nodules. Biomed Res. Int. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Meloni, M.F.; Smolock, A.; Cantisani, V.; Bezzi, M.; D’Ambrosio, F.; Proiti, M.; Lee, F.; Aiani, L.; Calliada, F.; Ferraioli, G. Contrast Enhanced Ultrasound in the Evaluation and Percutaneous Treatment of Hepatic and Renal Tumors. Eur. J. Radiol. 2015, 84, 1666–1674. [Google Scholar] [CrossRef] [PubMed]
- Pacella, C.M.; Mauri, G.; Cesareo, R.; Paqualini, V.; Cianni, R.; De Feo, P.; Gambelunghe, G.; Raggiunti, B.; Tina, D.; Deandrea, M.; et al. A Comparison of Laser with Radiofrequency Ablation for the Treatment of Benign Thyroid Nodules: A Propensity Score Matching Analysis. Int. J. Hyperth. 2017, 33, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Kim, E.K.; Kwak, J.Y.; Kim, M.J.; Son, E.J. Interobserver and Intraobserver Variations in Ultrasound Assessment of Thyroid Nodules. Thyroid 2010, 20, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Friedrich-Rust, M.; Meyer, G.; Dauth, N.; Berner, C.; Bogdanou, D.; Herrmann, E.; Zeuzem, S.; Bojunga, J. Interobserver Agreement of Thyroid Imaging Reporting and Data System (TIRADS) and Strain Elastography for the Assessment of Thyroid Nodules. PLoS ONE 2013, 8, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Dobruch-Sobczak, K.; Migda, B.; Krauze, A.; Mlosek, K.; Słapa, R.Z.; Wareluk, P.; Bakuła-Zalewska, E.; Adamczewski, Z.; Lewiński, A.; Jakubowski, W.; et al. Prospective Analysis of Inter-Observer and Intra-Observer Variability in Multi Ultrasound Descriptor Assessment of Thyroid Nodules. J. Ultrason. 2019, 19, 198–206. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| N | 23 | |
| Females/Males | 20/3 | |
| Mean age (± standard deviation) | 60 (±14) years | |
| Nodule location | Right | 9 |
| Isthmic | 3 | |
| Left | 11 | |
| Nodule mean volume before treatment (mL) | 23.90 ± 17.2 (range 7.3–62.5) | |
| Mean ablated volume (± standard deviation) assessed with CEUS (mL) | Reader 1 | 3.947 ± 4.243 |
| Reader 2 | 3.729 ± 4.196 | |
| Mean ablated volume (± standard deviation) assessed with B-mode (mL) | Reader 1 | 2.441 ± 1.735 |
| Reader 2 | 1.562 ± 1.965 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schiaffino, S.; Serpi, F.; Rossi, D.; Ferrara, V.; Buonomenna, C.; Alì, M.; Monfardini, L.; Sconfienza, L.M.; Mauri, G. Reproducibility of Ablated Volume Measurement Is Higher with Contrast-Enhanced Ultrasound than with B-Mode Ultrasound after Benign Thyroid Nodule Radiofrequency Ablation—A Preliminary Study. J. Clin. Med. 2020, 9, 1504. https://doi.org/10.3390/jcm9051504
Schiaffino S, Serpi F, Rossi D, Ferrara V, Buonomenna C, Alì M, Monfardini L, Sconfienza LM, Mauri G. Reproducibility of Ablated Volume Measurement Is Higher with Contrast-Enhanced Ultrasound than with B-Mode Ultrasound after Benign Thyroid Nodule Radiofrequency Ablation—A Preliminary Study. Journal of Clinical Medicine. 2020; 9(5):1504. https://doi.org/10.3390/jcm9051504
Chicago/Turabian StyleSchiaffino, Simone, Francesca Serpi, Duccio Rossi, Valerio Ferrara, Ciriaco Buonomenna, Marco Alì, Lorenzo Monfardini, Luca Maria Sconfienza, and Giovanni Mauri. 2020. "Reproducibility of Ablated Volume Measurement Is Higher with Contrast-Enhanced Ultrasound than with B-Mode Ultrasound after Benign Thyroid Nodule Radiofrequency Ablation—A Preliminary Study" Journal of Clinical Medicine 9, no. 5: 1504. https://doi.org/10.3390/jcm9051504
APA StyleSchiaffino, S., Serpi, F., Rossi, D., Ferrara, V., Buonomenna, C., Alì, M., Monfardini, L., Sconfienza, L. M., & Mauri, G. (2020). Reproducibility of Ablated Volume Measurement Is Higher with Contrast-Enhanced Ultrasound than with B-Mode Ultrasound after Benign Thyroid Nodule Radiofrequency Ablation—A Preliminary Study. Journal of Clinical Medicine, 9(5), 1504. https://doi.org/10.3390/jcm9051504