The Effect of an Abnormal BMI on Orthopaedic Trauma Patients: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Methods
Statistical Analysis
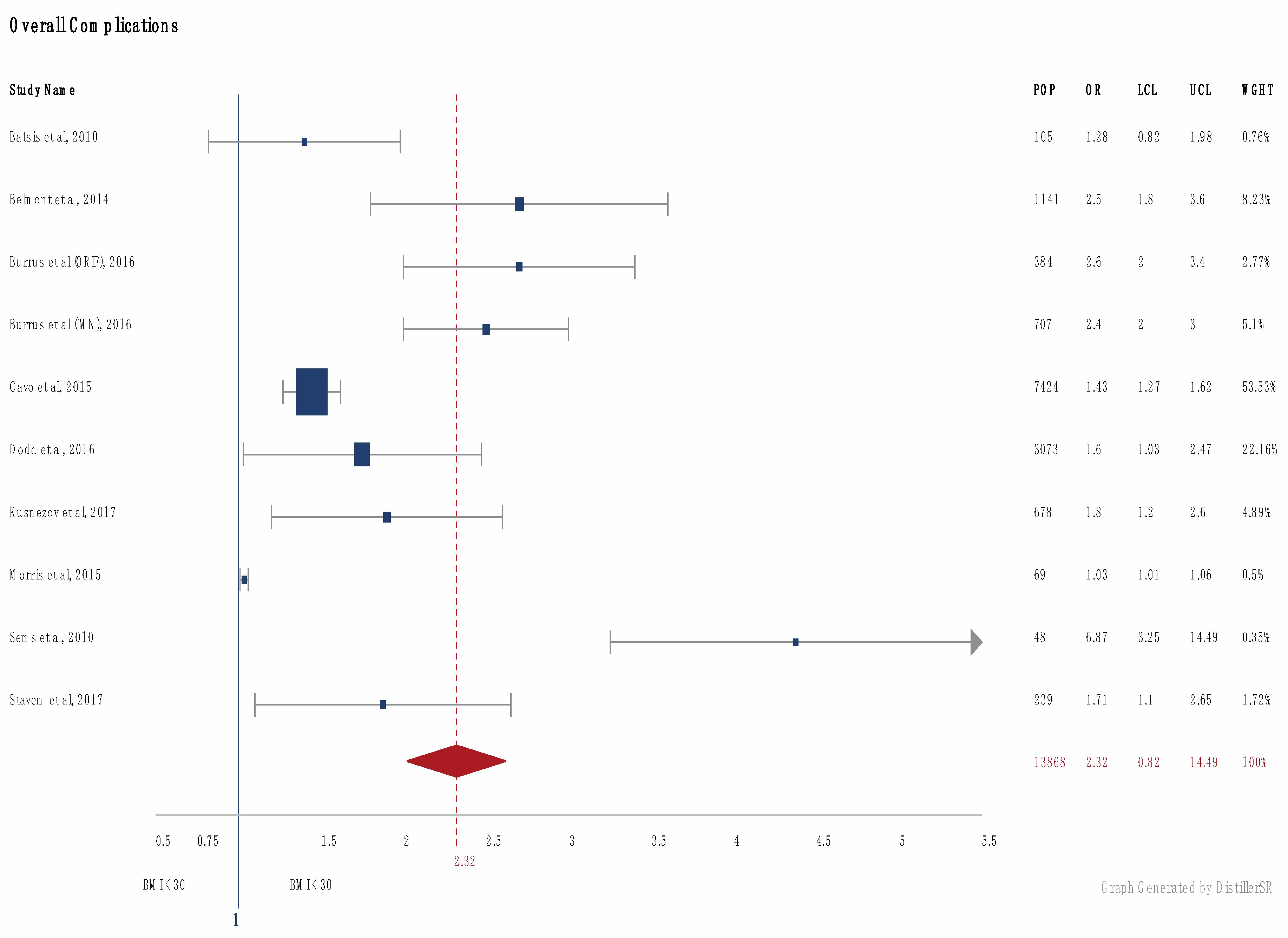
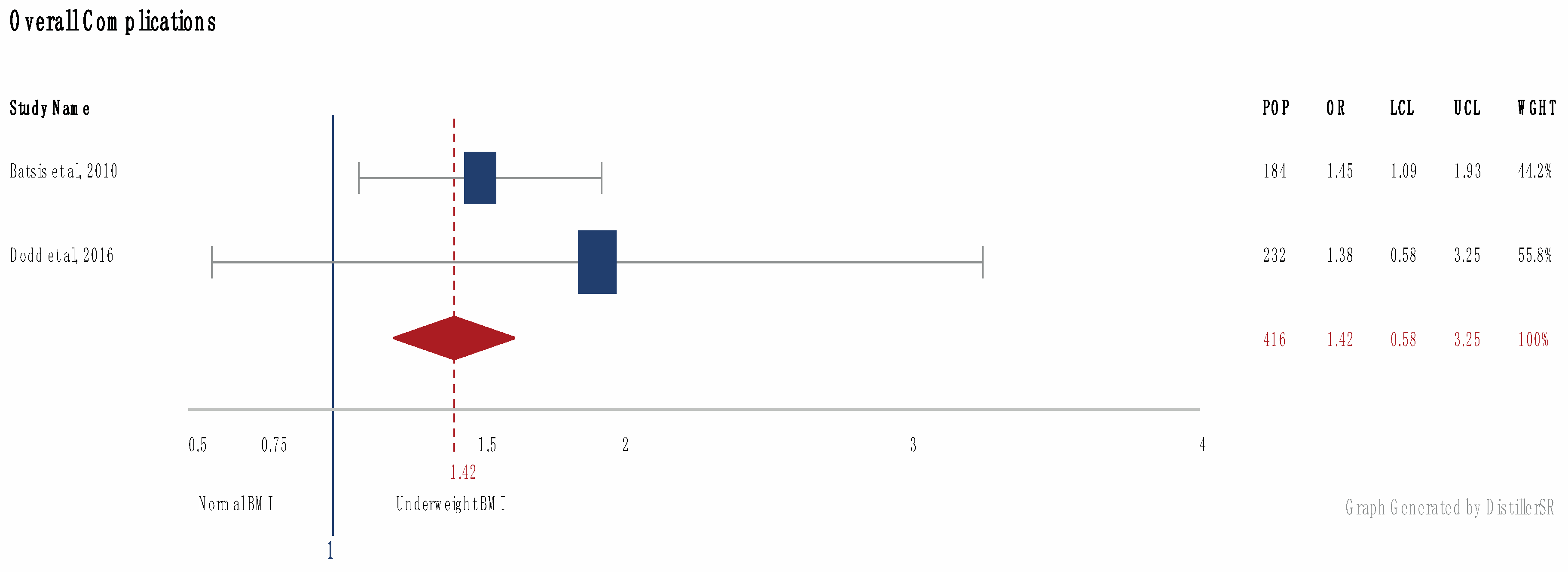
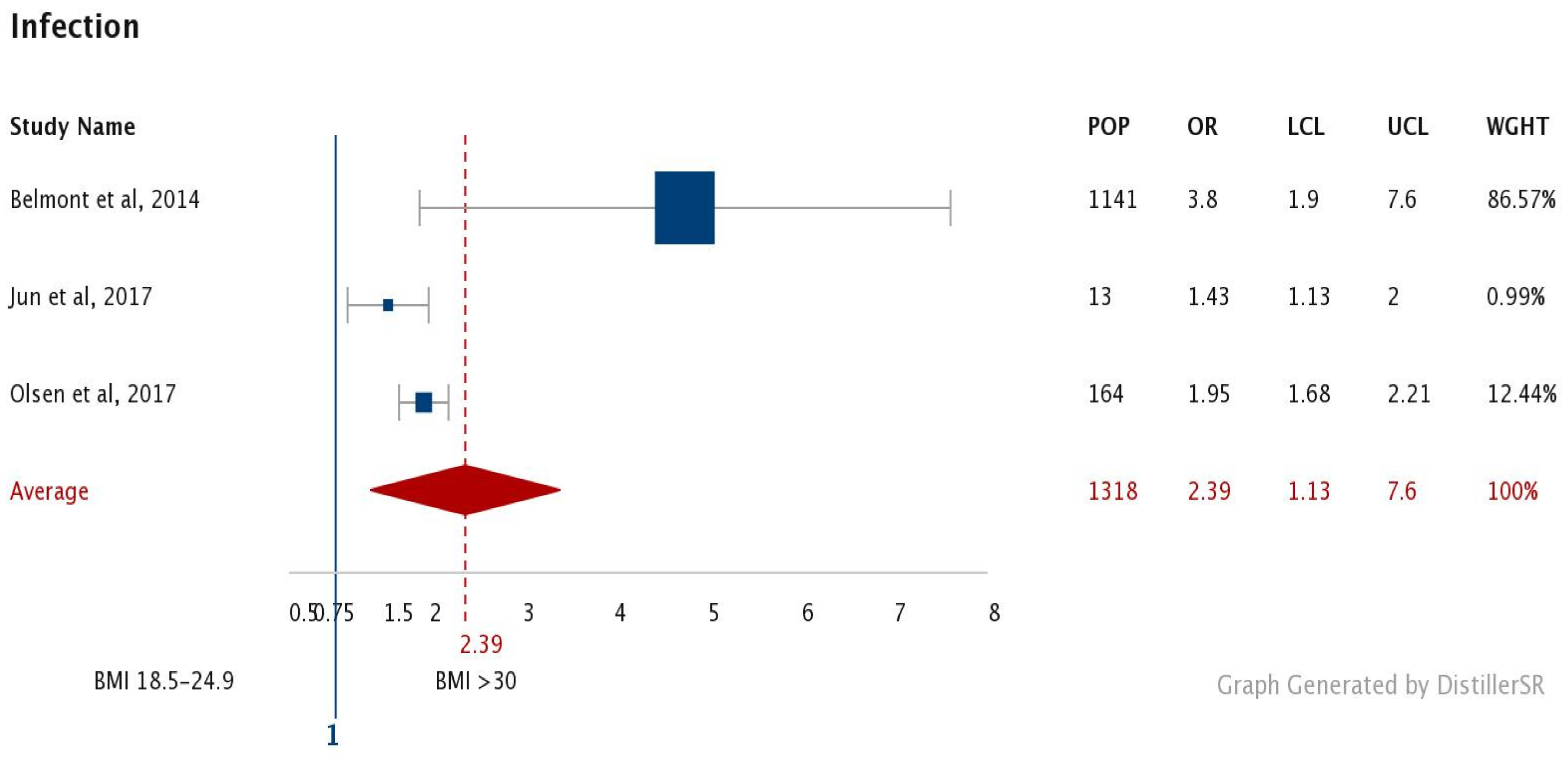
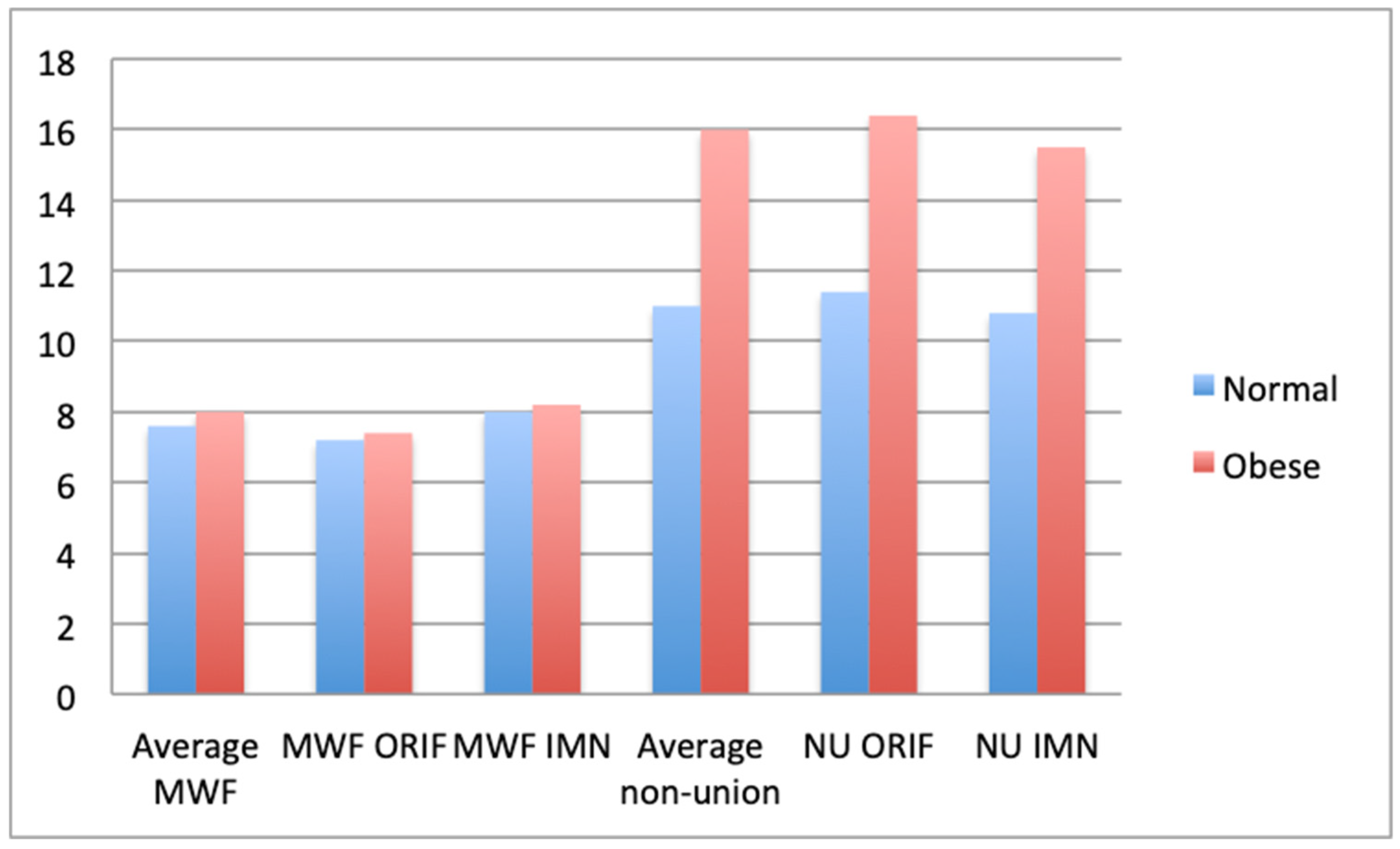
3. Results
4. Discussion
5. Conclusion
Author Contributions
Funding
Conflicts of Interest
References
- Ezzati, M. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar]
- Brooks, A.; Mahoney, F.; Hodgetts, J. Major Trauma; Churchill Livingston: Edinburgh, UK, 2007. [Google Scholar]
- WHO. Obesity and Overweight. 2018. Available online: http://www.who.int/mediacentre/factsheets/fs11/en/ (accessed on 3 March 2018).
- WHO. Obesity. 2019. Available online: https://www.who.int/topics/obesity/en/ (accessed on 2 December 2019).
- Chesser, T.J.; Hammett, R.B.; Norton, S.A. Orthopaedic trauma in the obese patient. Injury 2010, 41, 247–252. [Google Scholar] [CrossRef]
- Lazar, M.A.; Plocher, E.K.; Egol, K.A. Obesity and its relationship with pelvic and lower- extremity orthopedic trauma. Am. J. Orthop. (Chatham, NJ) 2010, 39, 175–182. [Google Scholar]
- Neville, A.L.; Brown, C.V.R.; Weng, J.; Demetriades, D.; Velmahos, G.C. Obesity is an independent risk factor of mortality in severely injured blunt trauma patients. Arch Surg. 2004, 139, 983–987. [Google Scholar] [CrossRef]
- Brown, C.V.R.; Velmahos, G.C. The consequences of obesity on trauma, emergency surgery, and surgical critical care. World J. Emerg. Surg. 2006, 1, 1–5. [Google Scholar] [CrossRef][Green Version]
- Whiting, P.S.; White-Dzuro, G.A.; Avilucea, F.R.; Dodd, A.C.; Lakomkin, N.; Obremskey, W.T.; Collinge, C.A.; Sethi, M.K. Body mass index predicts perioperative complications following orthopaedic trauma surgery: An ACS-NSQIP analysis. Eur. J. Trauma Emerg. Surg. Gery Off. Publ. Eur. Trauma Soc. 2017, 43, 255–264. [Google Scholar] [CrossRef]
- Parratte, S.; Pesenti, S.; Argenson, J.N. Obesity in orthopedics and trauma surgery. Orthop. Traumatol. Surg. Res. 2014, 100, 91–97. [Google Scholar] [CrossRef]
- Pelosi, P.; Croci, M.; Ravagnan, I.; Vicardi, P.; Gattinoni, L. Total respiratory system, lung, and chest wall mechanics in sedated-paralyzed postoperative morbidly obese patients. Chest 1996, 109, 144–151. [Google Scholar] [CrossRef]
- Hoffmann, M.; Lefering, R.; Gruber-Rathmann, M.; Rueger, J.; Lehmann, W. Trauma Registry of the German Society for Trauma Surgery, The impact of BMI on polytrauma outcome. Injury 2012, 43, 184–188. [Google Scholar] [CrossRef]
- Huschak, G.; Busch, T.; Kaisers, U.X. Obesity in anesthesia and intensive care. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 247–260. [Google Scholar] [CrossRef]
- Geoffroy, M.C.; Li, L.; Power, C. Depressive symptoms and body mass index: Co-morbidity and direction of association in a British birth cohort followed over 50 years. Psychol. Med. 2014, 44, 2641–2652. [Google Scholar] [CrossRef] [PubMed]
- Orri, M.; Boleslawski, E.; Regimbeau, J.M.; Bary, C.; Hassler, C.; Gregoire, E.; Bachellier, P.; Scatton, O.; Mabrut, J.Y.; Adham, M.; et al. Influence of Depression on Recovery After Major Noncardiac Surgery: A Prospective Cohort Study. Ann. Surg. 2015, 262, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Shaparin, N.; Widyn, J.; Nair, S.; Kho, I.; Geller, D.; Delphin, E. Does the obesity paradox apply to early postoperative complications after hip surgery? A retrospective chart review. J. Clin. Anesth. 2016, 32, 84–91. [Google Scholar] [CrossRef]
- Compston, J. Obesity and Bone. Curr. Osteoporos. Rep. 2013, 11, 30–35. [Google Scholar] [CrossRef]
- Tang, X.; Liu, G.; Kang, J.; Hou, Y.; Jiang, F.; Yuan, W.; Shi, J. Obesity and Risk of Hip Fracture in Adults: A Meta-Analysis of Prospective Cohort Studies. PLoS ONE 2013, 8, e55077. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Stroup, D.F., Berlin, J.A., Morton, S.C., Olkin, I., Williamson, G.D., Rennie, D., Moher, D., Becker, B.J., Sipe, T.A., Thacker, S.B., Eds.; Meta-Analysis of Observational Studies in Epidemiology; Wiley-Blackwell: Oxford, UK, 2008. [Google Scholar]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Vist, G.E.; Falck-Ytter, Y.; Schunemann, H.J. What is “quality of evidence” and why is it important to clinicians? BMJ (Clin. Res. Ed.) 2008, 336, 995–998. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ (Clin. Res. Ed.) 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; Debeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Ahmad, J.; Jones, K. The Effect of Obesity on Surgical Treatment of Achilles Tendon Ruptures. J. Am. Acad. Orthop. Surg. 2017, 25, 773–779. [Google Scholar] [CrossRef]
- Cavo, M.J.; Fox, J.P.; Markert, R.; Laughlin, R.T.; Laughlin, R.T. Association Between Diabetes, Obesity, and Short-Term Outcomes Among Patients Surgically Treated for Ankle Fracture. J. Bone Jt. Surg. Am. 2015, 97, 987–994. [Google Scholar] [CrossRef]
- Arroyo, W.; Nelson, K.J.; Belmont, P.J., Jr.; Bader, J.O.; Schoenfeld, A.J. Pelvic trauma: What are the predictors of mortality and cardiac, venous thrombo-embolic and infectious complications following injury? Injury 2013, 44, 1745–1749. [Google Scholar] [CrossRef]
- Baldwin, K.D.; Matuszewski, P.E.; Namdari, S.; Esterhai, J.L.; Mehta, S. Does morbid obesity negatively affect the hospital course of patients undergoing treatment of closed, lower- extremity diaphyseal long-bone fractures? Orthopedics 2011, 34, 18. [Google Scholar]
- Batsis, J.A.; Huddleston, J.M.; Melton, L.J.; Huddleston, P.M.; Lopez-Jimenez, F.; Larson, D.R.; Gullerud, R.E.; McMahon, M.M. Body mass index and risk of adverse cardiac events in elderly patients with hip fracture: A population-based study. J. Am. Geriatr. Soc. 2010, 57, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Huddleston, J.M.; Melton, L.J.; Huddleston, P.M.; Larson, D.R.; Gullerud, R.E.; McMahon, M.M. Body mass index (BMI) and risk of noncardiac postoperative medical complications in elderly hip fracture patients: A population-based study. J. Hosp. Med. 2009, 4, 1–9. [Google Scholar] [CrossRef]
- Belmont, P.J., Jr.; Garcia, E.J.; Romano, D.; Bader, J.O.; Nelson, K.J.; Schoenfeld, A.J. Risk factors for complications and in-hospital mortality following hip fractures: A study using the National Trauma Data Bank. Arch. Orthop. Trauma Surg. 2014, 134, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Burrus, M.T.; Werner, B.C.; Yarboro, S.R. Obesity is associated with increased postoperative complications after operative management of tibial shaft fractures. Injury 2016, 47, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Childs, B.R.; Nahm, N.J.; Dolenc, A.J.; Vallier, H.A. Obesity is Associated with More Complications and Longer Hospital Stays After Orthopaedic Trauma. J. Orthop. Trauma 2015, 29, 504–509. [Google Scholar] [CrossRef]
- Dincel, Y.M.; Oner, A.; Arikan, Y.; Caglar, S.; Ozcafer, R.; Gulec, M.A. Effect of BMI on outcomes of surgical treatment for tibial plateau fractures: A comparative retrospective case series study. Chin. J. Traumatol. 2018, 21, 104–108. [Google Scholar] [CrossRef]
- Dodd, A.C.; Lakomkin, N.; Attum, B.; Bulka, C.; Karhade, A.V.; Douleh, D.G.; Mir, H.; Jahangir, A.A.; Obremskey, W.T.; Sethi, M.K. Predictors of Adverse Events for Ankle Fractures: An Analysis of 6800 Patients. J. Foot Ankle Surg. 2016, 55, 762–766. [Google Scholar] [CrossRef]
- Graves, M.L.; Porter, S.E.; Fagan, B.C. Is obesity protective against wound healing complications in pilon Surgery? Soft tissue envelope and pilon fractures in the obese. Orthopedics 2010, 33, 555. [Google Scholar] [CrossRef]
- Johnson, J.P.; Kleiner, J.; Klinge, S.A.; McClure, P.K.; Hayda, R.A.; Born, C.T. Increased incidence of vascular injury in obese patients with knee dislocations. J. Orthop. Trauma 2018, 32, 82–87. [Google Scholar] [CrossRef]
- Su, J.; Cao, X. Risk factors of wound infection after open reduction and internal fixation of calcaneal fractures. Medicine 2017, 96, e8411. [Google Scholar] [CrossRef]
- Koerner, J.D.; Patel, N.M.; Yoon, R.S.; Gage, M.J.; Donegan, D.J.; Liporace, F.A. Femoral malrotation after intramedullary nailing in obese versus non- obese patients. Injury 2014, 45, 1095–1098. [Google Scholar] [CrossRef] [PubMed]
- Kusnezov, N.; Bader, J.; Blair, J.A. Predictors of Inpatient Mortality and Systemic Complications in Acetabular Fractures Requiring Operative Treatment. Orthopedics 2017, 40, e223–e228. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, R.; Mack, C.D.; Kaufman, R.P. Severity of injury and outcomes among obese trauma patients with fractures of the femur and tibia: A crash injury research and engineering network study. J. Orthop. Trauma 2009, 23, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.; Matsumoto, N.; Cho, B.; Hong, J.; Yamashita, M.; Hashizume, M.; Yi, B.J. Individual risk factors for deep infection and compromised fracture healing after intramedullary nailing of tibial shaft fractures: A single centre experience of 480 patients. Injury 2016, 46, 740–745. [Google Scholar]
- Morris, B.J.; Richards, J.E.; Guillamondegui, O.D.; Sweeney, K.R.; Mir, H.R.; Obremskey, W.T.; Kregor, P.J. Obesity Increases Early Complications After High-Energy Pelvic and Acetabular Fractures. Orthopedics 2015, 38, 881–887. [Google Scholar] [CrossRef]
- Olsen, L.L.; Møller, A.M.; Brorson, S.; Hasselager, R.B.; Sort, R. The impact of lifestyle risk factors on the rate of infection after surgery for a fracture of the ankle. Bone Jt. J. 2017, 99, 225–230. [Google Scholar] [CrossRef]
- Porter, S.E.; Graves, M.L.; Qin, Z.; Russell, G.V. Operative experience of pelvic fractures in the obese. Obes. Surg. 2008, 18, 702–708. [Google Scholar] [CrossRef]
- Sems, S.A.; Johnson, M.; Cole, P.A.; Byrd, C.T.; Templeman, D.C. Elevated body mass index increases early complications of surgical treatment of pelvic ring injuries. J. Orthop. Trauma 2010, 24, 309–314. [Google Scholar] [CrossRef]
- Shubiya, N.; Colby HFrost Jason DCampbell Matthew LDavis Daniel, C. Jupiter. Incidence of Acute Deep Vein Thrombosis and Pulmonary Embolism in Foot and Ankle Trauma: Analysis of the National Trauma Data Bank. J. Foot Ankle Surg. 2012, 51, 63–68. [Google Scholar] [CrossRef]
- Stavem, K.; Naumann, M.G.; Sigurdsen, U.; Utvåg, S.E. The association of body mass index with complications and functional outcomes after surgery for closed ankle fractures. Bone Jt. J. 2017, 99, 1389–1398. [Google Scholar] [CrossRef]
- Weinlein, J.C.; Deaderick, S.; Murphy, R.F. Morbid obesity increases the risk for systemic complications in patients with femoral shaft fractures. J. Orthop. Trauma 2015, 29, e91–e95. [Google Scholar] [CrossRef]
- Lean, M.E.J. Pathophysiology of Obesity. Proc. Nutr. Soc. 2000, 59, 331–336. [Google Scholar] [CrossRef]
- Werner, B.C.; Griffin, J.W.; Yang, S.; Brockmeier, S.F.; Gwathmey, F.W. Obesity is associated with increased postoperative complications after operative management of proximal humerus fractures. J. Shoulder Elb. Surg. 2015, 24, 593–600. [Google Scholar] [CrossRef]
- Heymsfield, S.B.; Wadden, T.A. Mechanisms, Pathophysiology and Management of Obesity. N. Engl. J. Med. 2017, 376, 254–266. [Google Scholar] [CrossRef]
- Tchkonia, T.; Thomou, T.; Zhu, Y.; Karagiannides, I.; Pothoulakis, C.; Jensen, M.D.; Kirkland, J.L. Mechanisms and metabolic implications of regional differences among fat depots. Cell Metab. 2013, 17, 644–656. [Google Scholar] [CrossRef]
- Pi-Sunyer, X. The medical risks of obesity. Postgrad. Med. 2009, 121, 21–33. [Google Scholar] [CrossRef]
- Ha, H.; Han, C.; Kim, B. Can Obesity Cause Depression? A Pseudo-panel Analysis. J. Prev. Med. Public Health 2017, 50, 262–267. [Google Scholar] [CrossRef]
- Sardesai, N.R.; Miller, M.A.; Jauregui, J.J.; Griffith, C.K.; Henn, R.F.; Nascone, J.W. Operative management of acetabulum fractures in the obese patient: Challenges and solutions. Orthop. Res. Rev. 2017, 9, 75–81. [Google Scholar] [CrossRef]
- Bozzio, A.E.; Gala, R.J.; Villasenor, M.A.; Hao, J.; Mauffrey, C. Orthopedic trauma surgery in the morbidly obese patient. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 421. [Google Scholar] [CrossRef]
- Yasin, M.M.; Saqib, R. Trauma healthcare treatment costs in the National Health Service. Bull. R. Coll. Surg. Engl. 2015, 97, 28–31. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Author | Title | Year | Normal BMI | Under weight BMI | Obese BMI | GRADE |
|---|---|---|---|---|---|---|---|
| 1 | Ahmad et al. [23] | The Effect of Obesity on Surgical Treatment of Achilles Tendon Ruptures | 2017 | 44 | 0 | 32 | Low |
| 2 | Arroyo et al. [25] | Pelvic trauma: What are the predictors of mortality and cardiac, venous thrombo-embolic and infectious complications following injury? | 2013 | 40,183 | 0 | 1114 | Mod |
| 3 | Baldwin et al. [26] | Does morbid obesity negatively affect the hospital course of patients undergoing treatment of closed, lower-extremity diaphyseal long-bone fractures? | 2011 | 19,795 | 0 | 331 | Low |
| 4 | Batsis et al. [27] | Body mass index (BMI) and risk of noncardiac postoperative medical complications in elderly hip fracture patients: a population-based study | 2010 | 640 | 184 | 105 | Low |
| 5 | Batsis et al. [28] | Body mass index and risk of adverse cardiac events in elderly patients with hip fracture: a population-based study | 2009 | 640 | 184 | 105 | Low |
| 6 | Belmont et al. [29] | Risk factors for complications and in-hospital mortality following hip fractures: a study using the National Trauma Data Bank | 2014 | 43,278 | 0 | 1141 | Low |
| 7 | Burrus et al. [30] | Obesity is associated with increased postoperative complications after operative management of tibial shaft fractures | 2016 | 12,727 | 0 | 1091 | Mod |
| 8 | Cavo et al. [24] | Association Between Diabetes, Obesity, and Short-Term Outcomes Among Patients Surgically Treated for Ankle Fracture | 2015 | 116,411 | 0 | 7424 | High |
| 9 | Childs et al. [31] | Obesity Is Associated With More Complications and Longer Hospital Stays After Orthopaedic Trauma | 2015 | 107 | 0 | 121 | Low |
| 10 | Dincel et al. [32] | Effect of BMI on outcomes of surgical treatment for tibial plateau fractures: A comparative retrospective case study | 2018 | 22 | 0 | 16 | Very Low |
| 11 | Dodd et al. [33] | Predictors of Adverse Events for Ankle Fractures: An Analysis of 6800 Patients | 2016 | 1242 | 232 | 3073 | High |
| 12 | Graves et al. [34] | Is obesity protective against wound healing complications in pilon surgery? Soft tissue envelope and pilon fractures in the obese. | 2010 | 83 | 0 | 31 | Low |
| 13 | Johnson et al. [35] | Increased incidence of vascular injury in obese patients with knee dislocations. | 2018 | 19,087 | 0 | 2265 | Mod |
| 14 | Jun et al. [36] | Risk factors of wound infection after open reduction and internal fixation of calcaneal fractures. | 2017 | 286 | 0 | 13 | Very Low |
| 15 | Koerner et al. [37] | Femoral malrotation after intramedullary nailing in obese versus non-obese patients. | 2014 | 111 | 0 | 95 | Low |
| 16 | Kusnezov et al. [38] | Predictors of inpatient mortality and systemic complications in acetabular fractures requiring operative treatment. | 2017 | 6763 | 0 | 678 | Mod |
| 17 | Maheswari et al. [39] | Severity of injury and outcomes among obese trauma patients with fractures of the femur and tibia: A crash injury research and engineering network study. | 2009 | 204 | 0 | 461 | Low |
| 18 | Metes makers et al. [40] | Individual risk factors for deep infection and compromised fracture healing after intramedullary nailing of tibial shaft fractures: a single centre experience of 480 patients. | 2015 | 430 | 0 | 50 | Very Low |
| 19 | Morris et al. [41] | Obesity Increases Early Complications After High-Energy Pelvic and Acetabular Fractures | 2015 | 175 | 0 | 69 | Low |
| 20 | Olsen et al. [42] | The impact of lifestyle risk factors on the rate of infection after surgery for a fracture of the ankle | 2017 | 879 | 0 | 164 | Mod |
| 21 | Porter et al. [43] | Operative experience of pelvic fractures in the obese. | 2008 | 102 | 0 | 186 | Mod |
| 22 | Sems et al. [44] | Elevated body mass index increases early complications of surgical treatment of pelvic ring injuries. | 2010 | 134 | 0 | 48 | Low |
| 23 | Shubiya et al. [45] | Incidence of Acute Deep Vein Thrombosis and Pulmonary Embolism in Foot and Ankle Trauma: Analysis of the National Trauma Data Bank | 2012 | 72,896 | 0 | 2768 | High |
| 24 | Stavem et al. [46] | The association of body mass index with complications and functional outcomes after surgery for closed ankle fractures. | 2017 | 272 | 0 | 239 | Mod |
| 25 | Weinlein et al. [47] | Morbid obesity increases the risk of systemic complications in patients with femoral shaft fractures. | 2015 | 184 | 114 | Mod | |
| 26 | Werner et al. [48] | Obesity is associated with increased postoperative complications after operative management of proximal humerus fractures. | 2015 | 16525 | 0 | 3794 | High |
| Complication | Prevalence in BMI <30 (Normal) | Prevalence in BMI >30 (abnormal) |
|---|---|---|
| Non-Union | 11.1% | 16.2% |
| Infection/Wound Problems | 5.6% | 12.7% |
| Metalwork Failure | 7.7% | 8.2% |
| Mortality | 3.4% | 4.9% |
| Cardiac | 2.3% | 3.7% |
| DVT | 1.3% | 3.2% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinder, F.; Giannoudis, P.V.; Boddice, T.; Howard, A. The Effect of an Abnormal BMI on Orthopaedic Trauma Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 1302. https://doi.org/10.3390/jcm9051302
Kinder F, Giannoudis PV, Boddice T, Howard A. The Effect of an Abnormal BMI on Orthopaedic Trauma Patients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2020; 9(5):1302. https://doi.org/10.3390/jcm9051302
Chicago/Turabian StyleKinder, Florence, Peter V. Giannoudis, Tim Boddice, and Anthony Howard. 2020. "The Effect of an Abnormal BMI on Orthopaedic Trauma Patients: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 9, no. 5: 1302. https://doi.org/10.3390/jcm9051302
APA StyleKinder, F., Giannoudis, P. V., Boddice, T., & Howard, A. (2020). The Effect of an Abnormal BMI on Orthopaedic Trauma Patients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 9(5), 1302. https://doi.org/10.3390/jcm9051302