The Public Health Burden of Cardiomyopathies: Insights from a Nationwide Inpatient Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. National Inpatient Database
2.2. Population
2.3. Diagnostic Codes and Longitudinal Derivation Rules
2.4. Statistical Analyses
3. Results
3.1. Inpatient Prevalence and Trend of Cardiomyopathies
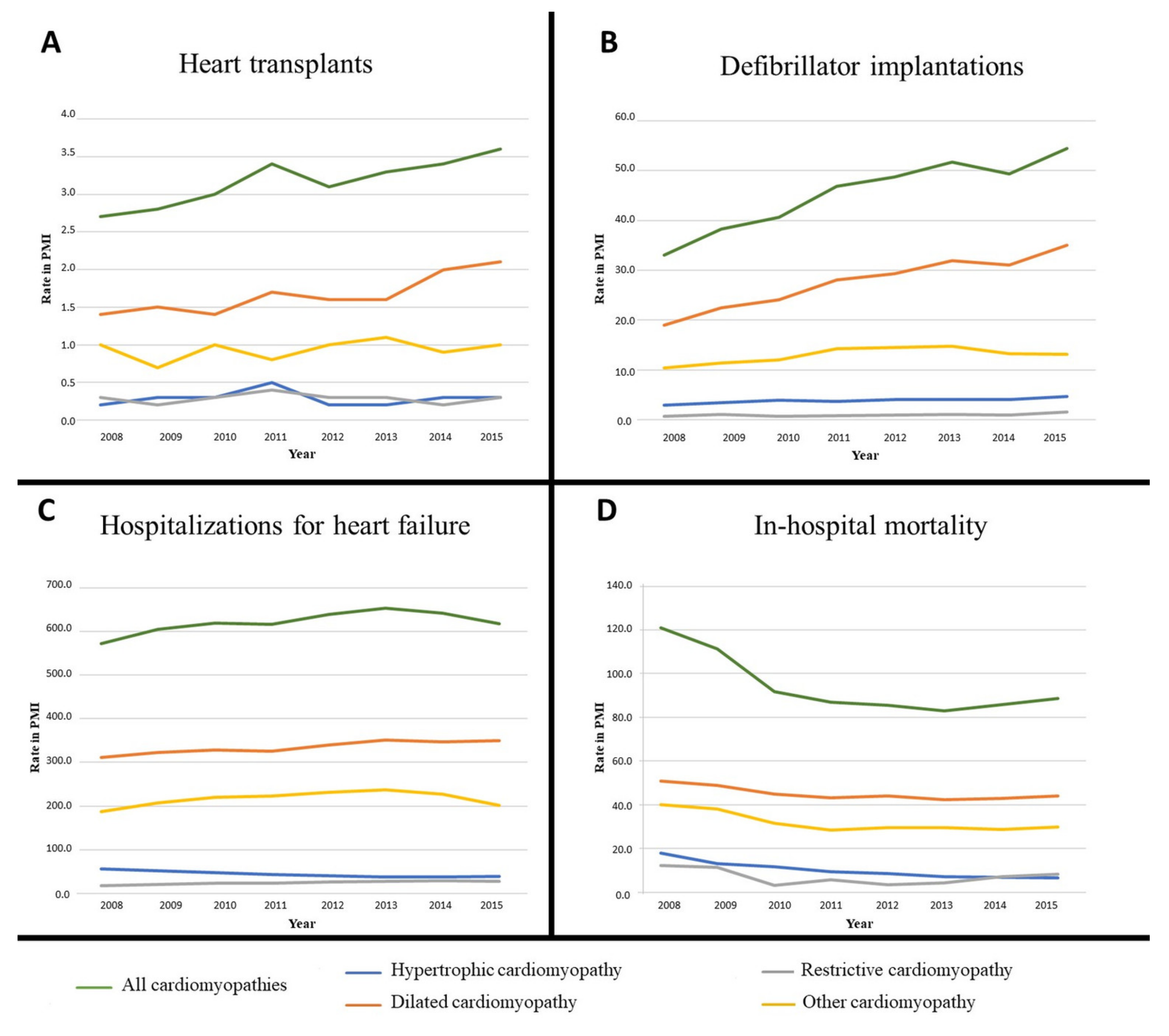
3.2. Cardiomyopathy-Related Cardiovascular Events and Invasive Procedures
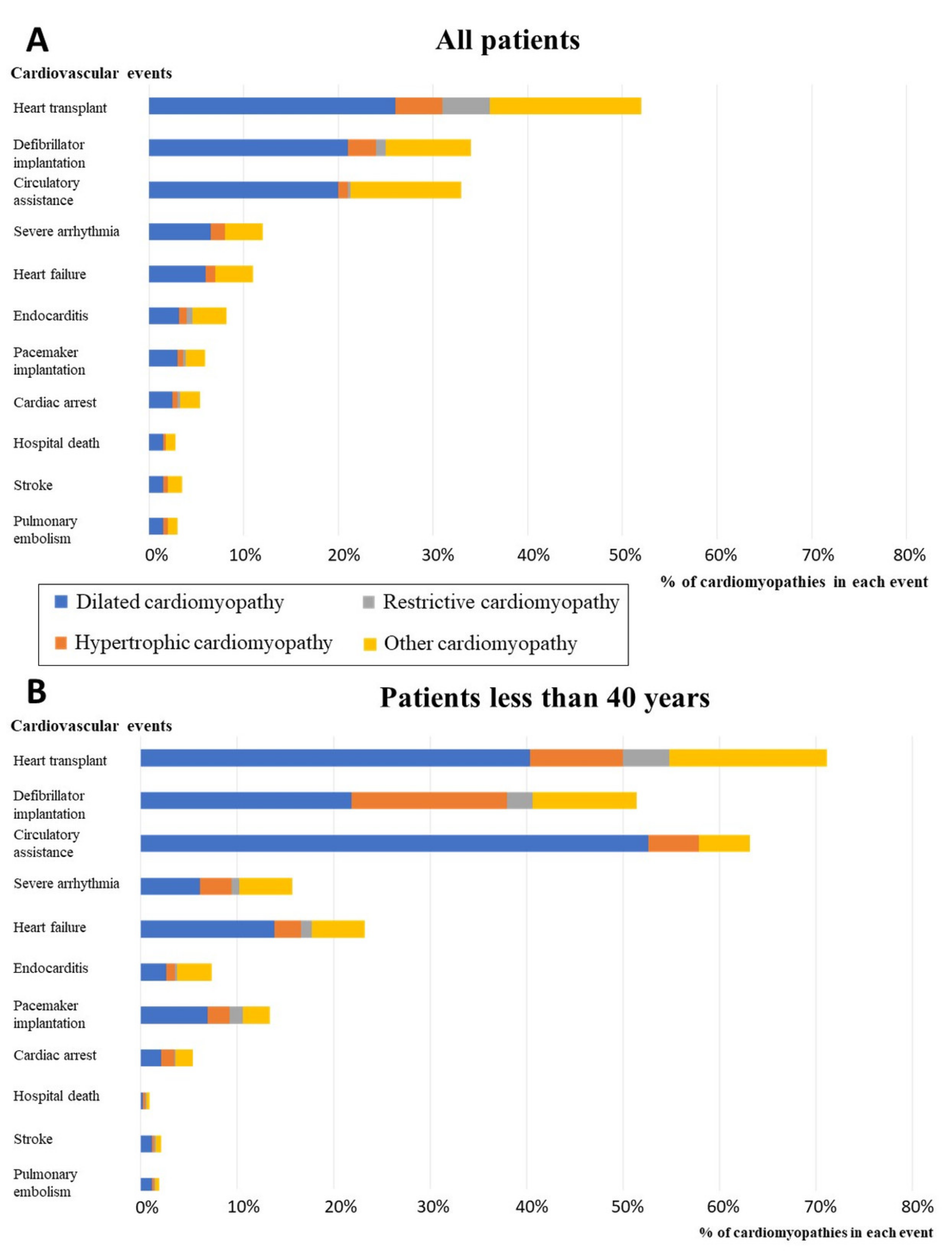
3.3. Proportion of Cardiomyopathies among all Cardiovascular Hospitalizations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Elliott, P.; Andersson, B.; Arbustini, E.; Bilinska, Z.; Cecchi, F.; Charron, P.; Dubourg, O.; Kühl, U.; Maisch, B.; McKenna, W.J.; et al. Classification of the cardiomyopathies: A position statement from the European Society of Cardiology Working Group on myocardial and pericardial diseases. Eur. Heart J. 2008, 29, 270–276. [Google Scholar] [CrossRef]
- Maron, B.J.; Towbin, J.A.; Thiene, G.; Antzelevitch, C.; Corrado, D.; Arnett, D.; Moss, A.J.; Seidman, C.E.; Young, J.B. Contemporary definitions and classification of the cardiomyopathies: An American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee. Circulation 2006, 113, 1807–1816. [Google Scholar] [CrossRef] [PubMed]
- Pinto, Y.M.; Elliott, P.M.; Arbustini, E.; Adler, Y.; Anastasakis, A.; Böhm, M.; Duboc, D.; Gimeno, J.; de Groote, P.; Imazio, M.; et al. Proposal for a revised definition of dilated cardiomyopathy, hypokinetic non-dilated cardiomyopathy, and its implications for clinical practice: A position statement of the ESC working group on myocardial and pericardial diseases. Eur. Heart J. 2016, 37, 1850–1858. [Google Scholar] [CrossRef] [PubMed]
- Miles, C.; Fanton, Z.; Tome, M.; Behr, E.R. Inherited cardiomyopathies. BMJ 2019, 365, l1570. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, R.G.; Semsarian, C.; Macdonald, P. Dilated cardiomyopathy. Lancet 2017, 390, 400–404. [Google Scholar] [CrossRef]
- Mogensen, J.; Arbustini, E. Restrictive cardiomyopathy. Curr. Opin. Cardiol. 2009, 24, 214–220. [Google Scholar] [CrossRef]
- Veselka, J.; Anavekar, N.S.; Charron, P. Hypertrophic obstructive cardiomyopathy. Lancet 2017, 389, 1253–1267. [Google Scholar] [CrossRef]
- Corrado, D.; Link, M.S.; Calkins, H. Arrhythmogenic right ventricular cardiomyopathy. Jarcho JA. N. Engl. J. Med. 2017, 376, 61–72. [Google Scholar] [CrossRef]
- McKenna, W.J.; Maron, B.J.; Thiene, G. Classification, epidemiology, and global burden of cardiomyopathies. Circ. Res. 2017, 121, 722–730. [Google Scholar] [CrossRef]
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef]
- Maron, B.J.; Gardin, J.M.; Flack, J.M.; Gidding, S.S.; Kurosaki, T.T.; Bild, D.E. Prevalence of hypertrophic cardiomyopathy in a general population of young adults: Echocardiographic analysis of 4111 subjects in the CARDIA Study. Circulation 1995, 92, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Codd, M.B.; Sugrue, D.D.; Gersh, B.J.; Melton, L.J. Epidemiology of idiopathic dilated and hypertrophic cardiomyopathy. A population-based study in Olmsted County, Minnesota, 1975–1984. Circulation 1989, 80, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Lorenzini, M.; Anastasiou, Z.; O’Mahony, C.; Guttman, O.P.; Gimeno, J.R.; Monserrat, L.; Anastasakis, A.; Rapezzi, C.; Biagini, E.; Garcia-Pavia, P.; et al. Mortality among Referral Patients With Hypertrophic Cardiomyopathy vs. the General European Population. JAMA Cardiol. 2020, 5, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Bagnall, R.D.; Weintraub, R.G.; Ingles, J.; Duflou, J.; Yeates, L.; Lam, L.L.; Davis, A.M.; Thompson, T.; Connell, V.; Wallace, J.; et al. A Prospective study of sudden cardiac death among children and young adults. N. Engl. J. Med. 2016, 374, 2441–2452. [Google Scholar] [CrossRef]
- Maron, B.J.; Doerer, J.J.; Haas, T.S.; Tierney, D.M.; Mueller, F.O. Sudden deaths in young competitive athletes: Analysis of 1866 deaths in the United States, 1980–2006. Circulation 2009, 119, 1085–1092. [Google Scholar] [CrossRef] [PubMed]
- Charron, P.; Elliott, P.M.; Gimeno, J.R.; Caforio, A.L.; Kaski, J.P.; Tavazzi, L.; Tendera, M.; Maupain, C.; Laroche, C.; Rubis, P.; et al. The Cardiomyopathy Registry of the EURObservational Research Programme of the European Society of Cardiology: Baseline data and contemporary management of adult patients with cardiomyopathies. Eur. Heart J. 2018, 39, 1784–1793. [Google Scholar] [CrossRef] [PubMed]
- Scheller-Kreinsen, D.; Quentin, W.; Busse, R. DRG-Based Hospital Payment Systems and Technological Innovation in 12 European Countries. Value Health 2011, 14, 1166–1172. [Google Scholar] [CrossRef]
- Strang, W.N.; Tuppin, P.; Atinault, A.; Jacquelinet, C. The French organ transplant data system. Stud. Health Technol. Inform. 2005, 116, 77–82. [Google Scholar]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Cantrelle, C.; Legeai, C.; Latouche, A.; Tuppin, P.; Jasseron, C.; Sebbag, L.; Bastien, O.; Dorent, R. Access to Heart Transplantation: A proper analysis of the competing risks of death and transplantation is required to optimize graft allocation. Transplant. Direct 2017, 3, e198. [Google Scholar] [CrossRef]
- Thekkudan, J.; Rogers, C.A.; Thomas, H.L.; van der Meulen, J.H.P.; Bonser, R.S.; Banner, N.R. Trends in adult heart transplantation: A national survey from the United Kingdom Cardiothoracic Transplant Audit 1995–2007. Eur. J. Cardiothorac. Surg. 2010, 37, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Khatiwala, J.R.; Everly, M.J. An update on cardiac transplantation in the United States based on an analysis of the UNOS Registry. Clin. Transpl. 2015, 31, 27–34. [Google Scholar] [PubMed]
- Shore, S.; Grau-Sepulveda, M.V.; Bhatt, D.L.; Heidenreich, P.A.; Eapen, Z.J.; Hernandez, A.F.; Yancy, C.W.; Fonarow, G.C. Characteristics, treatments, and outcomes of hospitalized heart failure patients stratified by etiologies of cardiomyopathy. JACC Heart Failure 2015, 3, 906–916. [Google Scholar] [CrossRef]
- Kirson, N.Y.; Birnbaum, H.G.; Ivanova, J.I.; Waldman, T.; Joish, V.; Williamson, T. Prevalence of pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension in the United States. Curr. Med. Res. Opin. 2011, 27, 1763–1768. [Google Scholar] [CrossRef]
- Priori, S.G.; Blomström-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology. Eur. Heart J. 2015, 36, 2793–2867. [Google Scholar] [PubMed]
- Hershberger, R.E.; Hedges, D.J.; Morales, A. Dilated cardiomyopathy: The complexity of a diverse genetic architecture. Nat. Rev. Cardiol. 2013, 10, 531–547. [Google Scholar] [CrossRef] [PubMed]
- González-López, E.; Gallego-Delgado, M.; Guzzo-Merello, G.; de Haro-del Moral, F.J.; Cobo-Marcos, M.; Robles, C.; Bornstein, B.; Salas, C.; Lara-Pezzi, E.; Alonso-Pulpon, L.; et al. Wild-type transthyretin amyloidosis as a cause of heart failure with preserved ejection fraction. Eur. Heart J. 2015, 36, 2585–2594. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, C.; Jichi, F.; Pavlou, M.; Monserrat, L.; Anastasakis, A.; Rapezzi, C.; Biagini, E.; Gimeno, J.R.; Limongelli, G.; McKenna, W.J.; et al. A novel clinical risk prediction model for sudden cardiac death in hypertrophic cardiomyopathy (HCM Risk-SCD). Eur. Heart J. 2014, 35, 2010–2020. [Google Scholar] [CrossRef] [PubMed]
- Cadrin-Tourigny, J.; Bosman, L.P.; Nozza, A.; Wang, W.; Tadros, R.; Bhonsale, A.; Bourfiss, M.; Fortier, A.; Lie, Ø.H.; Saguner, A.M.; et al. A new prediction model for ventricular arrhythmias in arrhythmogenic right ventricular cardiomyopathy. Eur. Heart J. 2019, 40, 1850–1858. [Google Scholar] [CrossRef]
- Norrish, G.; Ding, T.; Field, E.; Ziółkowska, L.; Olivotto, I.; Limongelli, G.; Anastasakis, A.; Weintraub, R.; Biagini, E.; Ragni, L.; et al. Development of a Novel Risk Prediction Model for Sudden Cardiac Death in Childhood Hypertrophic Cardiomyopathy (HCM Risk-Kids). JAMA Cardiol. 2019, 14. [Google Scholar] [CrossRef]
- Repetti, G.G.; Toepfer, C.N.; Seidman, J.G.; Seidman, C.E. Novel therapies for prevention and early treatment of cardiomyopathies. Circ. Res. 2019, 124, 1536–1550. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, P.; Palm, A.; Branden, E.; Mörner, S. Misclassification of hypertrophic cardiomyopathy: Validation of diagnostic codes. Clin. Epidemiol. 2017, 9, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Aymé, S.; Bellet, B.; Rath, A. Rare diseases in ICD11: Making rare diseases visible in health information systems through appropriate coding. Orphanet. J. Rare Dis. 2015, 10, 35. [Google Scholar] [CrossRef] [PubMed]
- Tuppin, P.; Rudant, J.; Constantinou, P.; Gastaldi-Ménager, C.; Rachas, A.; De Roquefeuil, L.; Maura, G.; Caillol, H.; Tajahmady, A.; Coste, J.; et al. Value of a national administrative database to guide public decisions: From the Système national d’information inter-régimes de l’Assurance Maladie (SNIIRAM) to the Système national des données de santé (SNDS) in France. Rev. Epidemiol. Sante Publique 2017, 65 (Suppl. 4), S149–S167. [Google Scholar] [CrossRef]
- McCormick, N.; Lacaille, D.; Bhole, V.; Avina-Zubieta, J.A. Validity of Heart Failure Diagnoses in Administrative Databases: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e104519. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| CM | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | M ± sd | PC% | AAPC | IC95% | p-Value | %Men | Age (m) | %CM |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DCM | 419.9 | 414.5 | 409.1 | 408.5 | 421 | 435.1 | 446.1 | 472.8 | 428.4 ± 23.6 | +13% | 1.58 | [0.88;2.3] | 0,0000 | 65% | 70 | 53% |
| OCM | 276.6 | 261.3 | 242.6 | 240.3 | 255.4 | 260.3 | 251.1 | 239.6 | 253.4 ± 9.3 | –13% | –1.1 | [–2.77;0.59] | NS | 57% | 69 | 31% |
| HCM | 124.7 | 109.8 | 101.5 | 95.4 | 89.3 | 89.8 | 93.8 | 101.7 | 100.8 ± 7.4 | –18% | –2.8 | [–4.39;–1.19] | 0.0007 | 60% | 70 | 12% |
| RCM | 21.9 | 23.3 | 22.7 | 22.2 | 25.8 | 28.4 | 30.9 | 32.4 | 26 ± 4.1 | +48% | 5.9 | [3.84;8] | 0,0000 | 56% | 74 | 3% |
| All CM | 844.0 | 809.9 | 777.1 | 767.5 | 792.7 | 814.4 | 822.9 | 847.5 | 809.5 ± 27.6 | 0% | 0.2 | [–0.16;0.57] | NS | 62% | 71 | 100% |
| EVENT | CM | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | m ± sd | PC% | AAPC% | CI95% | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Heart Failure | HCM | 56.2 | 52.5 | 47.1 | 42.7 | 40.1 | 37.5 | 38.1 | 39.4 | 44.2 ± 7 | –30% | –4.94 | [–6.17;–3.7] | <0.0001 |
| DCM | 310.9 | 323.4 | 328.4 | 326 | 339.5 | 351.3 | 347.3 | 349.6 | 334.6 ± 14.6 | 12% | 1.71 | [1.11;2.31] | 0.0004 | |
| RCM | 17.2 | 21.1 | 23 | 23.3 | 26.2 | 27.8 | 29.5 | 27.1 | 24.4 ± 4 | 58% | 6.82 | [3.84;9.89] | 0.0013 | |
| OCM | 187.2 | 207.9 | 220.5 | 223.5 | 231.8 | 237 | 227 | 201.7 | 217.1 ± 16.8 | 8% | 0.65 | [–2.15;3.54] | NS | |
| All CM | 571.9 | 605.5 | 619.5 | 616.4 | 638.5 | 654.1 | 642.5 | 618.3 | 620.8 ± 25.5 | 8% | 0.94 | [–0.7;2.6] | NS | |
| Stroke | HCM | 4.8 | 4.6 | 4.6 | 4.2 | 4.1 | 4.5 | 4.9 | 4.3 | 4.5 ± 0.3 | –10% | –0.65 | [–3.09;1.86] | NS |
| DCM | 17.8 | 20.2 | 21.7 | 21.9 | 25 | 24.1 | 24.5 | 24.5 | 22.5 ± 2.5 | 38% | 4.25 | [1.53;7.05] | 0.0021 | |
| RCM | 1.4 | 1.6 | 1.8 | 1.9 | 2.1 | 1.9 | 2.5 | 2.5 | 2 ± 0.4 | 79% | 8.11 | [5.31;10.99] | 0.0003 | |
| OCM | 21.7 | 23.4 | 21 | 20.7 | 21.9 | 22.3 | 22.4 | 19.4 | 21.6 ± 1.2 | –11% | –0.91 | [–3.02;1.25] | NS | |
| All | 45.7 | 49.9 | 49.1 | 48.7 | 53.1 | 52.8 | 54.4 | 50.7 | 50.6 ± 2.8 | 11% | 1.76 | [0.24;3.3] | 0.0299 | |
| Pulmonary Embolim | HCM | 3.3 | 2.9 | 2.8 | 2.8 | 2.6 | 2.3 | 2.6 | 2.5 | 2.7 ± 0.3 | –24% | –3.68 | [–5.92;–1.4] | 0.0078 |
| DCM | 12.7 | 13.4 | 13.6 | 12.9 | 13.3 | 13.3 | 13.5 | 13.4 | 13.3 ± 0.3 | 6% | 0.45 | [–0.39;1.3] | NS | |
| RCM | 0.8 | 1.1 | 1.2 | 1.2 | 1 | 1.2 | 1.3 | 1 | 1.1 ± 0.2 | 25% | 2.67 | [–3.09;8.77] | NS | |
| OCM | 11.1 | 11.6 | 11.7 | 10.9 | 9.9 | 10.5 | 10.1 | 9.8 | 10.7 ± 0.7 | –12% | –2.34 | [–3.84;–0.81] | 0.0098 | |
| All | 27.9 | 29 | 29.2 | 27.8 | 26.8 | 27.3 | 27.5 | 26.8 | 27.8 ± 0.9 | –4% | –0.93 | [–1.85;0] | 0.0496 | |
| Endocarditis | HCM | 0.5 | 0.6 | 0.7 | 0.6 | 0.7 | 0.7 | 0.8 | 0.7 | 0.7 ± 0.1 | 40% | 4.81 | [1.15;8.6] | 0.0178 |
| DCM | 3 | 3.2 | 3.8 | 3.8 | 3.6 | 4.7 | 4.2 | 3.6 | 3.7 ± 0.5 | 20% | 3.91 | [–0.51;8.52] | NS | |
| RCM | 0.2 | 0.3 | 0.3 | 0.4 | 0.4 | 0.4 | 0.3 | 0.4 | 0.3 ± 0.1 | 100% | 7.04 | [–0.61;15.28] | NS | |
| OCM | 2.4 | 2.8 | 3.6 | 4 | 4.8 | 4.5 | 4.3 | 4.2 | 3.8 ± 0.8 | 75% | 8.01 | [5.13;10.97] | <0.0001 | |
| All | 6.3 | 7 | 8.3 | 8.8 | 9.6 | 10.4 | 9.7 | 8.9 | 8.6 ± 1.4 | 41% | 4.71 | [1.68;7.83] | 0.0021 | |
| Cardiac Arrest | HCM | 3.1 | 3 | 3.3 | 2.7 | 2.7 | 2.7 | 2.5 | 2.5 | 2.8 ± 0.3 | –19% | -3.53 | [–5.48;–1.54] | 0.005 |
| DCM | 9.1 | 12.1 | 11.8 | 10.2 | 12 | 12.9 | 12.9 | 13.5 | 11.8 ± 1.5 | 48% | 4.27 | [0.74;7.92] | 0.025 | |
| RCM | 0.8 | 1 | 1.2 | 0.9 | 1.2 | 1.4 | 1.7 | 1.4 | 1.2 ± 0.3 | 75% | 9.11 | [3.34;15.2] | 0.0078 | |
| OCM | 7.4 | 8.8 | 9.3 | 10 | 11 | 11 | 11.1 | 11.6 | 10 ± 1.4 | 57% | 5.82 | [2.99;8.73] | 0,0000 | |
| All | 20.3 | 25 | 25.7 | 23.8 | 26.9 | 27.9 | 28.1 | 28.9 | 25.8 ± 2.8 | 42% | 4.16 | [1.76;6.63] | 0.0053 | |
| In-HospitalDeath | HCM | 18 | 13.1 | 11.7 | 9.4 | 8.5 | 7.1 | 7 | 6.5 | 10.2 ± 3.9 | –64% | –13.42 | [–17.63;–9] | <0.0001 |
| DCM | 50.8 | 48.8 | 45 | 43.2 | 44 | 42.3 | 43 | 44 | 45.1 ± 3 | –13% | –2.26 | [–3.87;–0.63] | 0.0069 | |
| RCM | 12.3 | 11.4 | 3.3 | 5.7 | 3.5 | 4.2 | 7.1 | 8.4 | 7 ± 3.5 | –32% | –10.05 | [–32.58;20.01] | NS | |
| OCM | 40 | 38 | 31.7 | 28.4 | 29.5 | 29.5 | 28.7 | 29.8 | 32 ± 4.5 | –26% | –4.52 | [–7.06;–1.92] | 0.0007 | |
| All | 121 | 111.3 | 91.7 | 86.8 | 85.6 | 83.1 | 85.8 | 88.7 | 94.3 ± 14 | –27% | –4.7 | [–7.09;–2.26] | 0.0002 |
| Procedure | CM | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | m ± sd | PC% | AAPC | CI95% | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pacemaker | HCM | 6.3 | 6.1 | 5.3 | 5.7 | 5 | 4.9 | 5.4 | 5.5 | 5.5 ± 0.5 | –13% | –1.6 | [–6.3;3.33] | NS |
| DCM | 31.3 | 31.8 | 30.7 | 27.8 | 27.6 | 26.8 | 25.8 | 25.9 | 28.5 ± 2.4 | –17% | –3.26 | [–4.25;–2.26] | 0.0002 | |
| RCM | 1.9 | 2.2 | 2.2 | 2.1 | 2.5 | 2.4 | 2.6 | 2.6 | 2.3 ± 0.3 | 37% | 4.21 | [2.2;6.27] | 0.0021 | |
| OCM | 18.1 | 18.1 | 19.1 | 18.2 | 18 | 18.2 | 17.8 | 14.7 | 17.8 ± 1.3 | –19% | –2,00 | [–4.4;0.47] | NS | |
| All | 57.6 | 58.2 | 57.3 | 53.8 | 53.1 | 52.3 | 51.6 | 48.8 | 54.1 ± 3.3 | –15% | –2.41 | [–3.07;–1.75] | 0.0001 | |
| Implantable Cardioverter Defibrillator | HCM | 2.9 | 3.4 | 3.9 | 3.7 | 4 | 4 | 4.1 | 4.7 | 3.8 ± 0.5 | 62% | 5.47 | [2.97;8.02] | 0.0016 |
| DCM | 19 | 22.5 | 24.1 | 28.1 | 29.3 | 31.9 | 31 | 35.1 | 27.6 ± 5.4 | 85% | 8.6 | [5.01;12.31] | <0.0001 | |
| RCM | 0.7 | 1 | 0.7 | 0.8 | 0.9 | 1.1 | 0.9 | 1.6 | 1 ± 0.3 | 129% | 8.35 | [0.4;16.92] | 0.042 | |
| OCM | 10.4 | 11.4 | 12 | 14.2 | 14.5 | 14.7 | 13.2 | 13.1 | 12.9 ± 1.6 | 26% | 3.27 | [0.25;6.38] | 0.0334 | |
| All | 33.1 | 38.3 | 40.7 | 46.9 | 48.7 | 51.7 | 49.3 | 54.5 | 45.4 ± 7.3 | 65% | 6.98 | [3.68;10.38] | <0.0001 | |
| Heart Transplant | HCM | 0.2 | 0.3 | 0.3 | 0.5 | 0.2 | 0.2 | 0.3 | 0.3 | 0.3 ± 0.1 | 50% | 0.84 | [–11.27;14.61] | NS |
| DCM | 1.4 | 1.5 | 1.4 | 1.7 | 1.6 | 1.6 | 2 | 2.1 | 1.7 ± 0.3 | 50% | 5.65 | [2.69;8.7] | 0.0032 | |
| RCM | 0.3 | 0.2 | 0.3 | 0.4 | 0.3 | 0.3 | 0.2 | 0.3 | 0.3 ± 0.1 | 0% | –0.34 | [–9.34;9.55] | NS | |
| OCM | 1 | 0.7 | 1 | 0.8 | 1 | 1.1 | 0.9 | 1 | 0.9 ± 0.1 | 0% | 2.12 | [–3.5;8.08] | NS | |
| All | 2.7 | 2.8 | 3 | 3.4 | 3.1 | 3.3 | 3.4 | 3.6 | 3.2 ± 0.3 | 33% | 3.86 | [2.13;5.61] | 0.0015 | |
| Circulatory Assistance | HCM | 0 | 0 | 0 | 0 | 0 | 0.1 | 0 | 0.1 | 0 ± 0 | – | – | – | – |
| DCM | 0.2 | 0.2 | 0.3 | 0.4 | 0.4 | 0.5 | 0.9 | 0.6 | 0.4 ± 0.2 | 200% | 22.06 | [13.18;31.63] | 0.0007 | |
| RCM | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | – | – | – | – | – | |
| OCM | 0.1 | 0.1 | 0.1 | 0.2 | 0.3 | 0.3 | 0.5 | 0.4 | 0.3 ± 0.2 | 300% | – | – | – | |
| All | 1.2 | 0.9 | 1.2 | 1.5 | 2 | 2.3 | 2.6 | 3.2 | 1.9 ± 0.8 | 167% | 18.71 | [12.42;25.36] | 0.0002 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lannou, S.; Mansencal, N.; Couchoud, C.; Lassalle, M.; Dubourg, O.; Stengel, B.; Jacquelinet, C.; Charron, P. The Public Health Burden of Cardiomyopathies: Insights from a Nationwide Inpatient Study. J. Clin. Med. 2020, 9, 920. https://doi.org/10.3390/jcm9040920
Lannou S, Mansencal N, Couchoud C, Lassalle M, Dubourg O, Stengel B, Jacquelinet C, Charron P. The Public Health Burden of Cardiomyopathies: Insights from a Nationwide Inpatient Study. Journal of Clinical Medicine. 2020; 9(4):920. https://doi.org/10.3390/jcm9040920
Chicago/Turabian StyleLannou, Simon, Nicolas Mansencal, Cécile Couchoud, Mathilde Lassalle, Olivier Dubourg, Bénédicte Stengel, Christian Jacquelinet, and Philippe Charron. 2020. "The Public Health Burden of Cardiomyopathies: Insights from a Nationwide Inpatient Study" Journal of Clinical Medicine 9, no. 4: 920. https://doi.org/10.3390/jcm9040920
APA StyleLannou, S., Mansencal, N., Couchoud, C., Lassalle, M., Dubourg, O., Stengel, B., Jacquelinet, C., & Charron, P. (2020). The Public Health Burden of Cardiomyopathies: Insights from a Nationwide Inpatient Study. Journal of Clinical Medicine, 9(4), 920. https://doi.org/10.3390/jcm9040920