Long-Term Follow-Up of Patients with Catecholaminergic Polymorphic Ventricular Arrhythmia

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Definitions
2.2. Genetic Screening
2.3. Statistics
3. Results
3.1. Demographics, Clinical Profile and Follow-Up Data
3.2. Symptoms Per Family
3.3. Genetic Screening
3.4. Detailed Description of CPVT Families
3.4.1. Family 1
3.4.2. Family 2
3.4.3. Family 3
3.4.4. Family 4
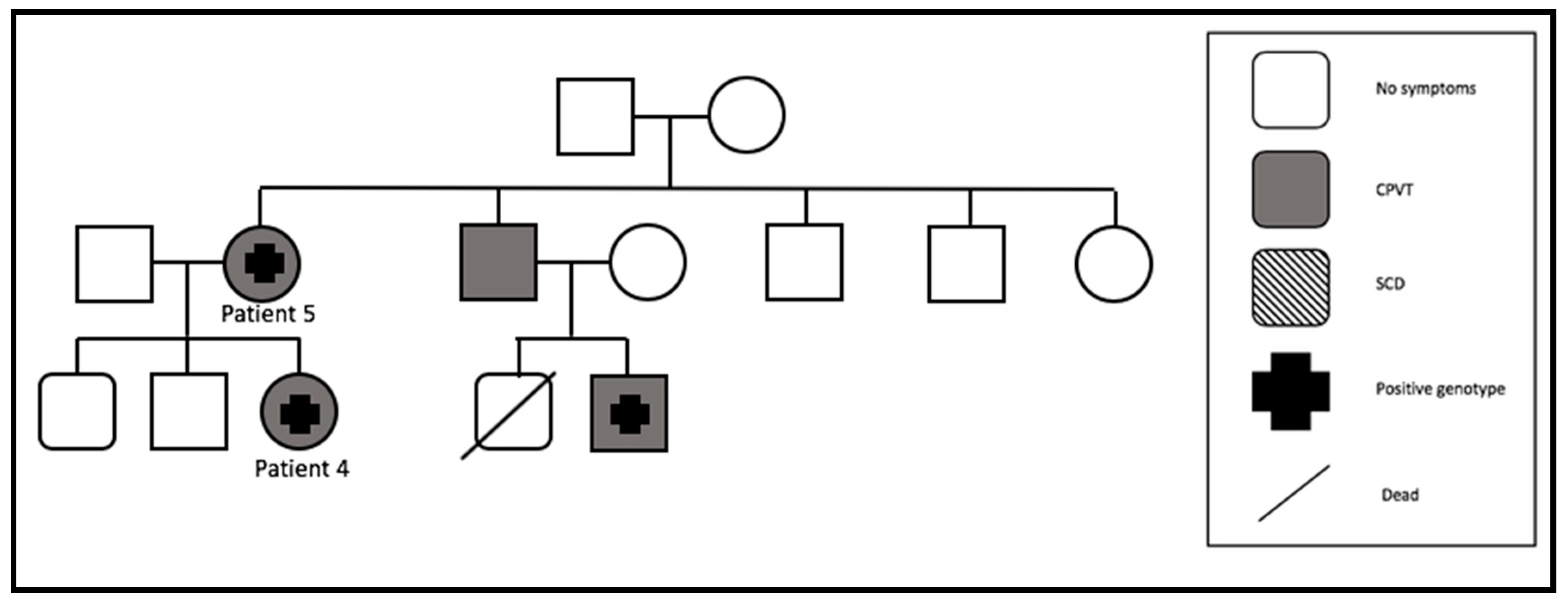
3.4.5. Family 5
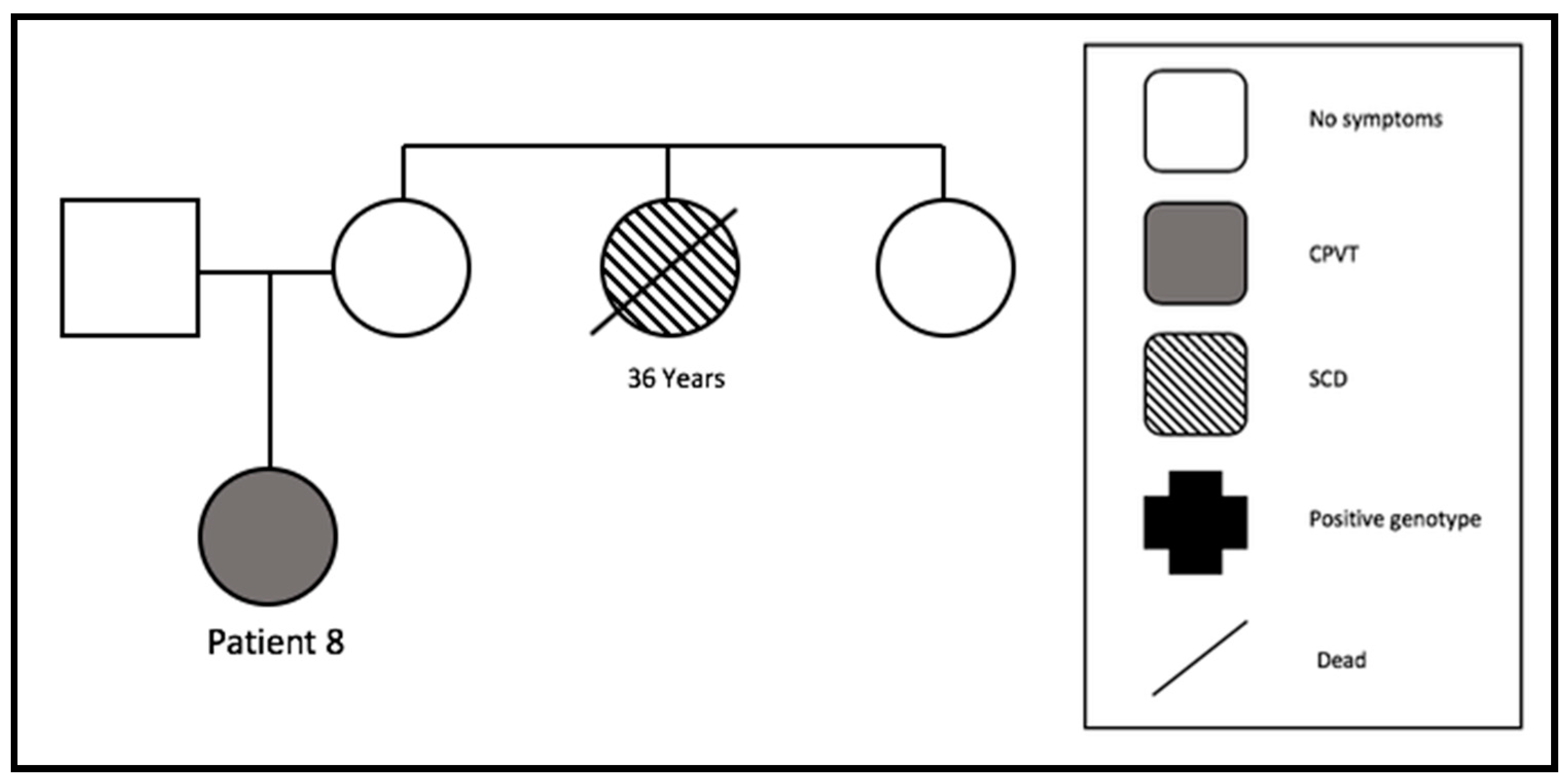
3.4.6. Family 6
3.4.7. Family 7
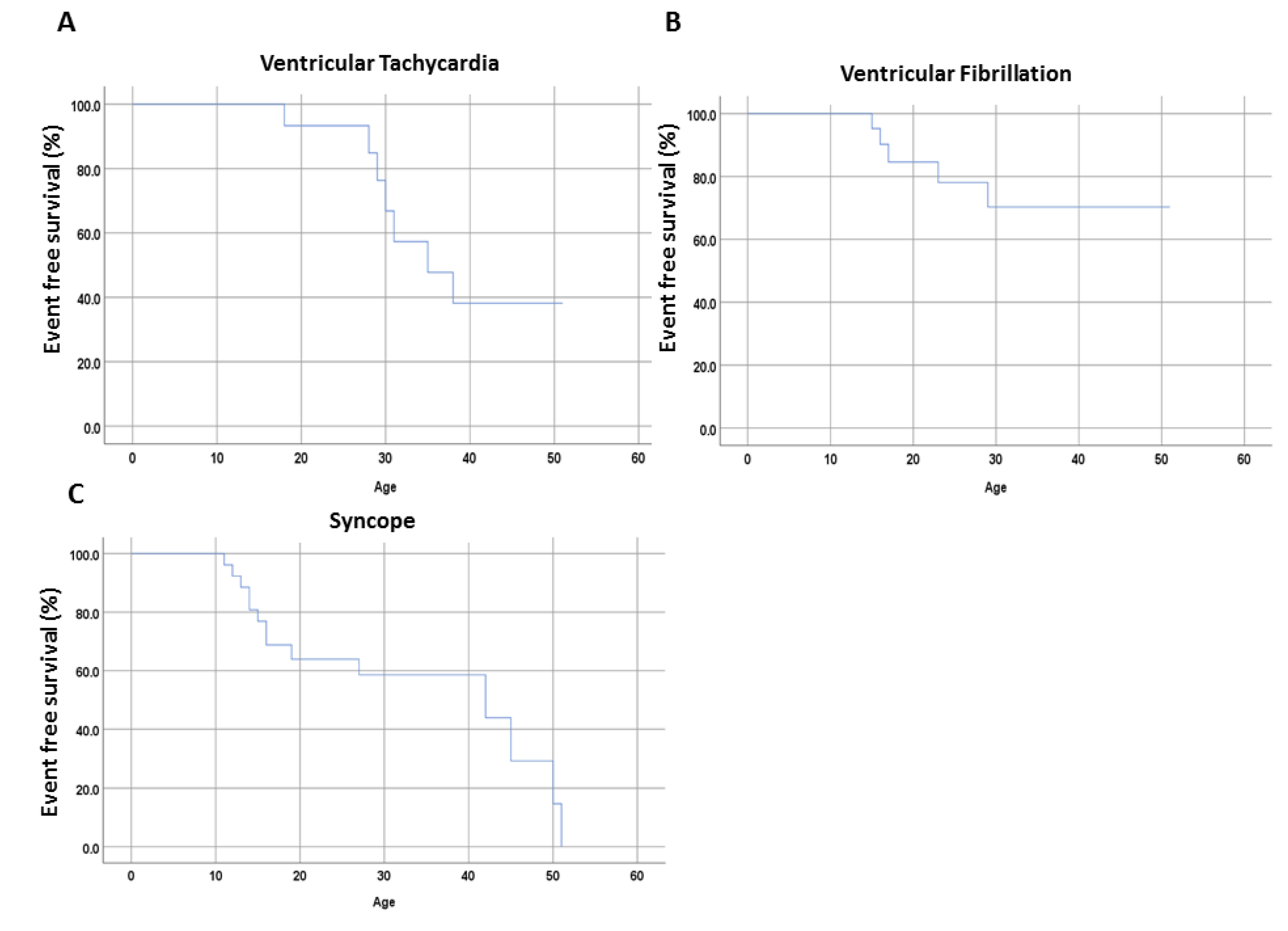
3.5. Long-Term Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Leenhardt, A.; Lucet, V.; Denjoy, I.; Grau, F.; Ngoc, D.D.; Coumel, P. Catecholaminergic polymorphic ventricular tachycardia in children. A 7-year follow-up of 21 patients. Circulation 1995, 91, 1512–1519. [Google Scholar] [CrossRef] [PubMed]
- Priori, S.G.; Napolitano, C.; Memmi, M.; Colombi, B.; Drago, F.; Gasparini, M.; DeSimone, L.; Coltorti, F.; Bloise, R.; Keegan, R.; et al. Clinical and molecular characterization of patients with catecholaminergic polymorphic ventricular tachycardia. Circulation 2002, 106, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Denjoy, I.; Extramiana, F.; Maltret, A.; Buisson, N.R.; Lupoglazoff, J.M.; Klug, D.; Hayashi, M.; Takatsuki, S.; Villain, E.; et al. Incidence and risk factors of arrhythmic events in catecholaminergic polymorphic ventricular tachycardia. Circulation 2009, 119, 2426–2434. [Google Scholar] [CrossRef] [PubMed]
- Priori, S.G.; Napolitano, C.; Tiso, N.; Memmi, M.; Vignati, G.; Bloise, R.; Sorrentino, V.; Danieli, G.A. Mutations in the cardiac ryanodine receptor gene (hRyR2) underlie catecholaminergic polymorphic ventricular tachycardia. Circulation 2001, 103, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Laitinen, P.J.; Swan, H.; Kontula, K. Molecular genetics of exercise-induced polymorphic ventricular tachycardia: Identification of three novel cardiac ryanodine receptor mutations and two common calsequestrin 2 amino-acid polymorphisms. Eur. J. Hum. Genet. 2003, 11, 888–891. [Google Scholar] [CrossRef][Green Version]
- Lahat, H.; Pras, E.; Olender, T.; Avidan, N.; Ben-Asher, E.; Man, O.; Levy-Nissenbaum, E.; Khoury, A.; Lorber, A.; Goldman, B.; et al. A missense mutation in a highly conserved region of CASQ2 is associated with autosomal recessive catecholamine-induced polymorphic ventricular tachycardia in Bedouin families from Israel. Am. J. Hum. Genet. 2001, 69, 1378–1384. [Google Scholar] [CrossRef]
- Roston, T.M.; Vinocur, J.M.; Maginot, K.R.; Mohammed, S.; Salerno, J.C.; Etheridge, S.P.; Cohen, M.; Hamilton, R.M.; Pflaumer, A.; Kanter, R.J.; et al. Catecholaminergic polymorphic ventricular tachycardia in children: Analysis of therapeutic strategies and outcomes from an international multicenter registry. Circ. Arrhythmia Electrophysiol. 2015, 8, 633–642. [Google Scholar] [CrossRef]
- Van der Werf, C.; Kannankeril, P.J.; Sacher, F.; Krahn, A.D.; Viskin, S.; Leenhardt, A.; Shimizu, W.; Sumitomo, N.; Fish, F.A.; Bhuiyan, Z.A.; et al. Flecainide therapy reduces exercise-induced ventricular arrhythmias in patients with catecholaminergic polymorphic ventricular tachycardia. J. Am. Coll. Cardiol. 2011, 57, 2244–2254. [Google Scholar] [CrossRef]
- Roses-Noguer, F.; Jarman, J.W.; Clague, J.R.; Till, J. Outcomes of defibrillator therapy in catecholaminergic polymorphic ventricular tachycardia. Heart Rhythm. 2014, 11, 58–66. [Google Scholar] [CrossRef]
- Miyake, C.Y.; Webster, G.; Czosek, R.J.; Kantoch, M.J.; Dubin, A.M.; Avasarala, K.; Atallah, J. Efficacy of implantable cardioverter defibrillators in young patients with catecholaminergic polymorphic ventricular tachycardia: Success depends on substrate. Circ. Arrhythmia Electrophysiol. 2013, 6, 579–587. [Google Scholar] [CrossRef] [PubMed]
- De Ferrari, G.M.; Dusi, V.; Spazzolini, C.; Bos, J.M.; Abrams, D.J.; Berul, C.I.; Crotti, L.; Davis, A.M.; Eldar, M.; Kharlap, M.; et al. Clinical Management of Catecholaminergic Polymorphic Ventricular Tachycardia: The Role of Left Cardiac Sympathetic Denervation. Circulation 2015, 131, 2185–2193. [Google Scholar] [CrossRef] [PubMed]
- Priori, S.G.; Blomstrom-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur. Heart J. 2015, 36, 2793–2867. [Google Scholar] [PubMed]
- Wanguemert, F.; Bosch Calero, C.; Perez, C.; Campuzano, O.; Beltran-Alvarez, P.; Scornik, F.S.; Iglesias, A.; Berne, P.; Allegue, C.; Hernandez, P.M.R.; et al. Clinical and molecular characterization of a cardiac ryanodine receptor founder mutation causing catecholaminergic polymorphic ventricular tachycardia. Heart Rhythm. 2015, 12, 1636–1643. [Google Scholar] [CrossRef] [PubMed]
- Leite, L.R.; Ponzi Pereira, K.R.; Alessi, S.R.; de Paola, A.A. Catecholaminergic polymorphic ventricular tachycardia. An important diagnosis in children with syncope and normal heart. Arq. Bras. Cardiol. 2001, 76, 63–74. [Google Scholar] [CrossRef]
- Swan, H.; Amarouch, M.Y.; Leinonen, J.; Marjamaa, A.; Kucera, J.P.; Laitinen-Forsblom, P.J.; Lahtinen, A.M.; Palotie, A.; Kontula, A.; Toivonen, L.; et al. Gain-of-function mutation of the SCN5A gene causes exercise-induced polymorphic ventricular arrhythmias. Circ. Cardiovasc. Genet. 2014, 7, 771–781. [Google Scholar] [CrossRef]
- Roux-Buisson, N.; Cacheux, M.; Fourest-Lieuvin, A.; Fauconnier, J.; Brocard, J.; Denjoy, I.; Durand, P.; Guicheney, P.; Kyndt, F.; Leenhardt, A.; et al. Absence of triadin, a protein of the calcium release complex, is responsible for cardiac arrhythmia with sudden death in human. Hum. Mol. Genet. 2012, 21, 2759–2767. [Google Scholar] [CrossRef]
- Nyegaard, M.; Overgaard, M.T.; Sondergaard, M.T.; Vranas, M.; Behr, E.R.; Hildebrandt, L.L.; Lund, J.; Hedley, P.L.; Camm, A.J.; Wettrell, G.; et al. Mutations in calmodulin cause ventricular tachycardia and sudden cardiac death. Am. J. Hum. Genet. 2012, 91, 703–712. [Google Scholar] [CrossRef]
- Xie, L.; Hou, C.; Jiang, X.; Zhao, J.; Li, Y.; Xiao, T. A compound heterozygosity of Tecrl gene confirmed in a catecholaminergic polymorphic ventricular tachycardia family. Eur. J. Med. Genet. 2019, 62, 103631. [Google Scholar] [CrossRef]
- Van der Werf, C.; Zwinderman, A.H.; Wilde, A.A. Therapeutic approach for patients with catecholaminergic polymorphic ventricular tachycardia: State of the art and future developments. Europace 2012, 14, 175–183. [Google Scholar] [CrossRef]
- Roston, T.M.; Jones, K.; Hawkins, N.M.; Bos, J.M.; Schwartz, P.J.; Perry, F.; Ackerman, M.J.; Laksman, Z.W.M.; Kaul, P.; Lieve, K.V.V.; et al. Implantable cardioverter-defibrillator use in catecholaminergic polymorphic ventricular tachycardia: A systematic review. Heart Rhythm. 2018, 15, 1791–1799. [Google Scholar] [CrossRef]
- Van der Werf, C.; Lieve, K.V.; Bos, J.M.; Lane, C.M.; Denjoy, I.; Roses-Noguer, F.; Aiba, T.; Wada, Y.; Ingles, J.; Leren, I.S.; et al. Implantable cardioverter-defibrillators in previously undiagnosed patients with catecholaminergic polymorphic ventricular tachycardia resuscitated from sudden cardiac arrest. Eur. Heart J. 2019, 40, 2953–2961. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N = 9 |
|---|---|
| Demographics | |
| Age at first symptoms, mean ± SD | 20.4 ± 10.3 |
| Age at diagnosis, mean ± SD | 26.4 ± 12 |
| Male, n (%) | 2 (22.2) |
| Symptoms at admission, n (%) | |
| Syncope | 4 (44.4) |
| Aborted cardiac arrest | 4 (44.4) |
| Atrial arrhythmias | 3 (33.3) |
| Family history of SCD | 5 (55.6) |
| Epilepsy | 0 (0) |
| ECG at admission | |
| Sinus rhythm | 9 (100) |
| Exercise stress test, n (%) | |
| Induction of VT or VF | 1 (11.1) |
| Induction of VES | 8 (88.9) |
| Genetic screening, n (%) | |
| RYR2 | 5 (55.6) |
| CASQ2 | 0 (0) |
| Not identified | 3 (33.3) |
| Not screened | 1 (11.1) |
| Treatment, n (%) | |
| Beta-blocker | 7 (77.8) |
| Flecainide and Beta-blocker | 4 (44.4) |
| LCSD | 0 (0) |
| ICD Implantation, n (%) | |
| Yes | 7 (77.8) |
| No | 1 (11.1) |
| Event recorder | 1 (11.1) |
| Patient Number | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| Sex | female | male | female | female | female | female | female | female | male |
| Age at diagnosis (years) | 23 | 55 | 16 | 13 | 20 | 31 | 33 | 18 | 29 |
| Family number | 1 | 2 | 2 | 3 | 3 | 4 | 5 | 6 | 7 |
| Gene mutation (mutation sequence) | not screened | RYR2 (D2216G) | RYR2 (D2216G) | RYR2 (L2432F) | RYR2 (L2432F) | RYR2 (M4002V) | 0 | 0 | 0 |
| Initial medical treatment | Metoprolol 50 mg/day | no medical treatment | Bisoprolol 2.5 mg/day | Bisoprolol 2.5 mg/day | no medical treatment | Metoprolol 200 mg/day | Propafenone 450 mg/day | Metoprolol 150 mg/day | Propanolol (dosage not available) |
| Changed medical treatment | refused | no medical treatment | Metoprolol 25 mg/day | Bisoprolol 5 mg/day | no medical treatment | Metoprolol 200 mg/day + Flecainide 200 mg/day | Metoprolol 100 mg/day | Metoprolol 150 mg/day | refused |
| Current medical treatment | refused | no medical treatment | Metoprolol 100 mg/day | Bisoprolol 5 mg/day + Flecainide 200 mg/day | no medical treatment | Metoprolol 200 mg/day + Flecainide 200 mg/day | Metoprolol 100 mg/day + Flecainide 100 mg/day | refused | refused |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veith, M.; El-Battrawy, I.; Roterberg, G.; Raschwitz, L.; Lang, S.; Wolpert, C.; Schimpf, R.; Zhou, X.; Akin, I.; Borggrefe, M. Long-Term Follow-Up of Patients with Catecholaminergic Polymorphic Ventricular Arrhythmia. J. Clin. Med. 2020, 9, 903. https://doi.org/10.3390/jcm9040903
Veith M, El-Battrawy I, Roterberg G, Raschwitz L, Lang S, Wolpert C, Schimpf R, Zhou X, Akin I, Borggrefe M. Long-Term Follow-Up of Patients with Catecholaminergic Polymorphic Ventricular Arrhythmia. Journal of Clinical Medicine. 2020; 9(4):903. https://doi.org/10.3390/jcm9040903
Chicago/Turabian StyleVeith, Michael, Ibrahim El-Battrawy, Gretje Roterberg, Laura Raschwitz, Siegfried Lang, Christian Wolpert, Rainer Schimpf, Xiaobo Zhou, Ibrahim Akin, and Martin Borggrefe. 2020. "Long-Term Follow-Up of Patients with Catecholaminergic Polymorphic Ventricular Arrhythmia" Journal of Clinical Medicine 9, no. 4: 903. https://doi.org/10.3390/jcm9040903
APA StyleVeith, M., El-Battrawy, I., Roterberg, G., Raschwitz, L., Lang, S., Wolpert, C., Schimpf, R., Zhou, X., Akin, I., & Borggrefe, M. (2020). Long-Term Follow-Up of Patients with Catecholaminergic Polymorphic Ventricular Arrhythmia. Journal of Clinical Medicine, 9(4), 903. https://doi.org/10.3390/jcm9040903