Delta Neutrophil Index for the Prediction of Prognosis in Acute Gastrointestinal Diseases; Diagnostic Test Accuracy Meta-Analysis



Abstract
1. Introduction
2. Methods
2.1. Literature Searching Strategy
2.2. Selection Criteria
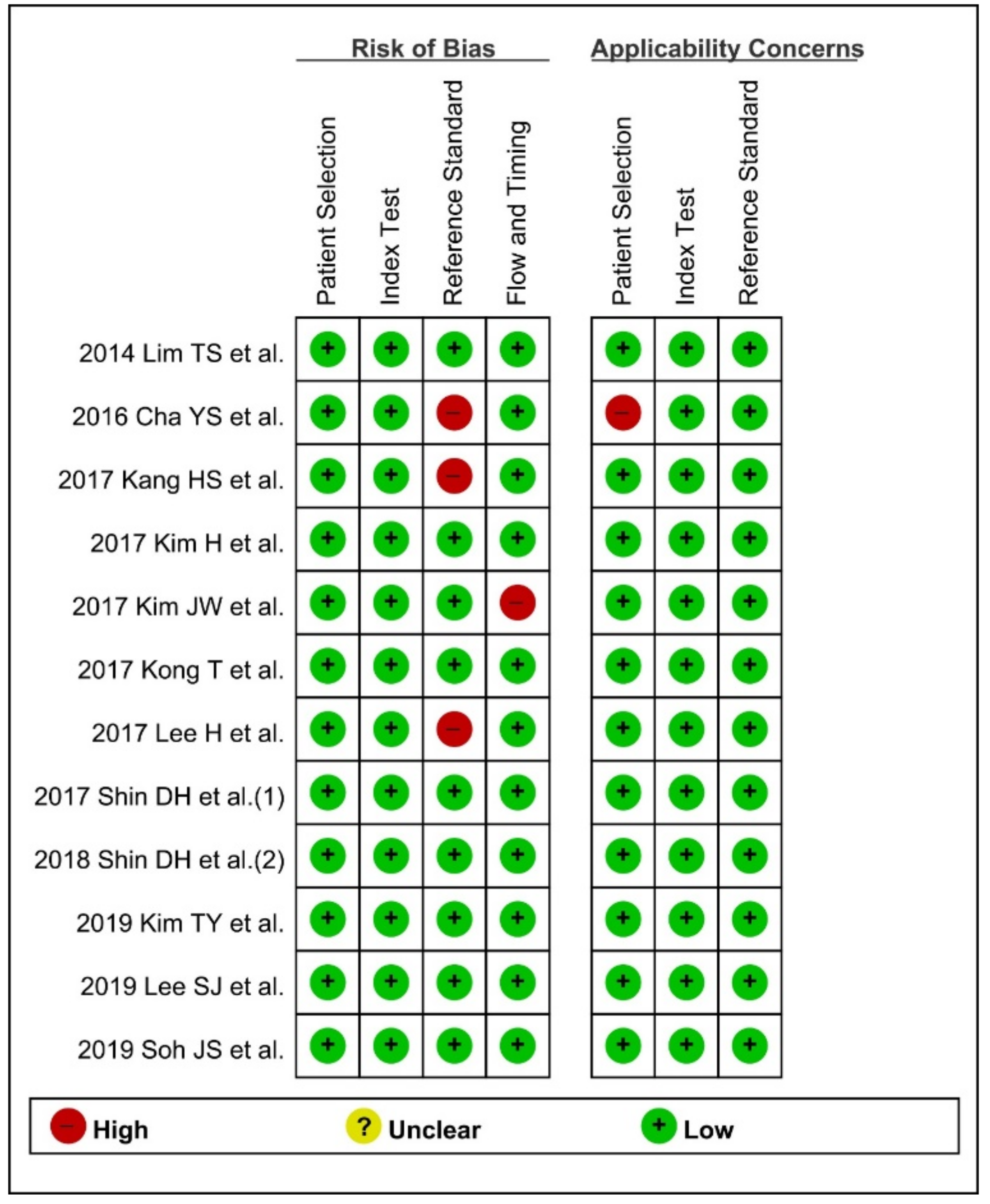
2.3. Methodological Quality Assessment
2.4. Data Extraction, Primary Outcome, and Additional Analyses
2.5. Statistics
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality of the Methodology
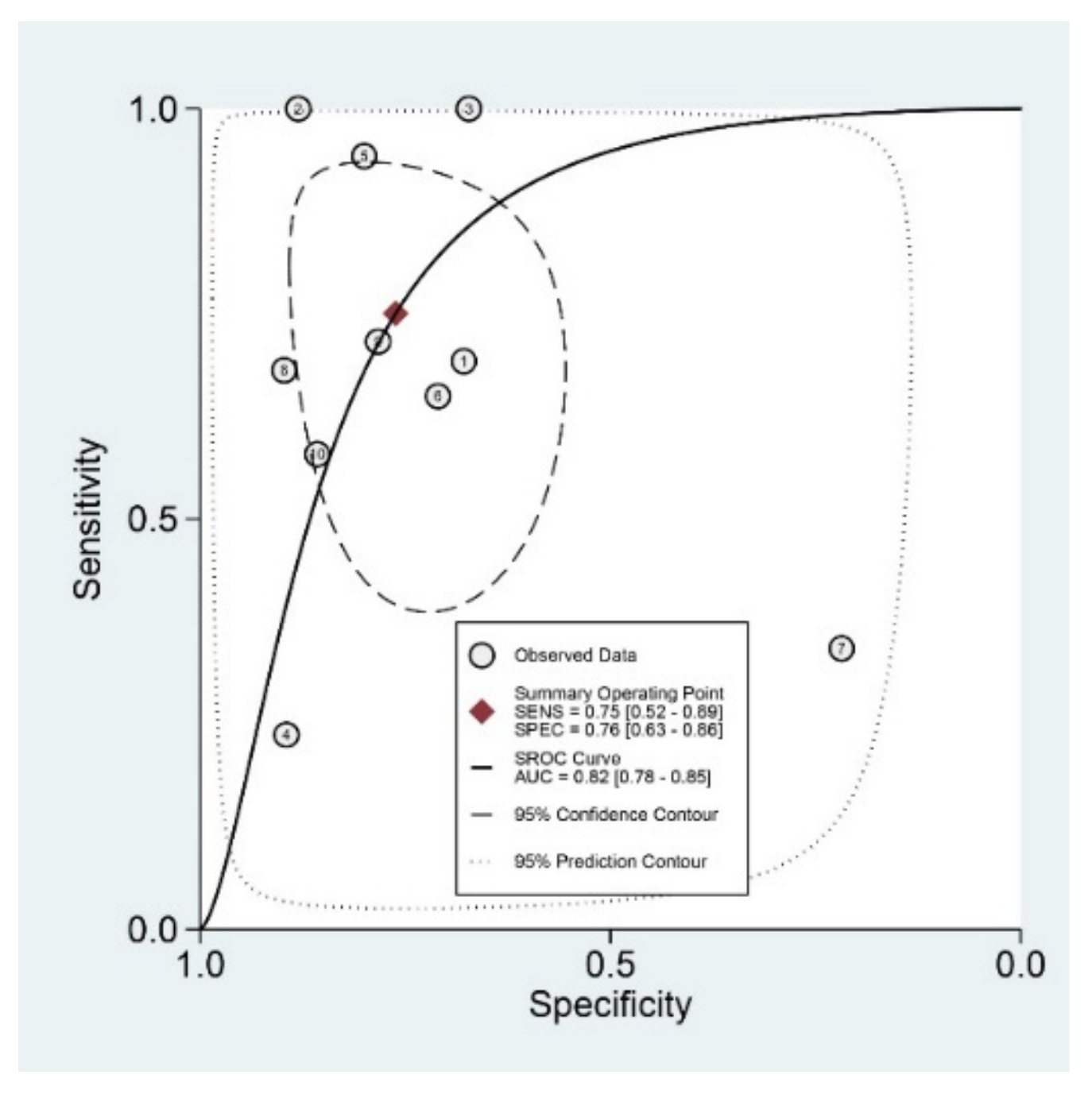
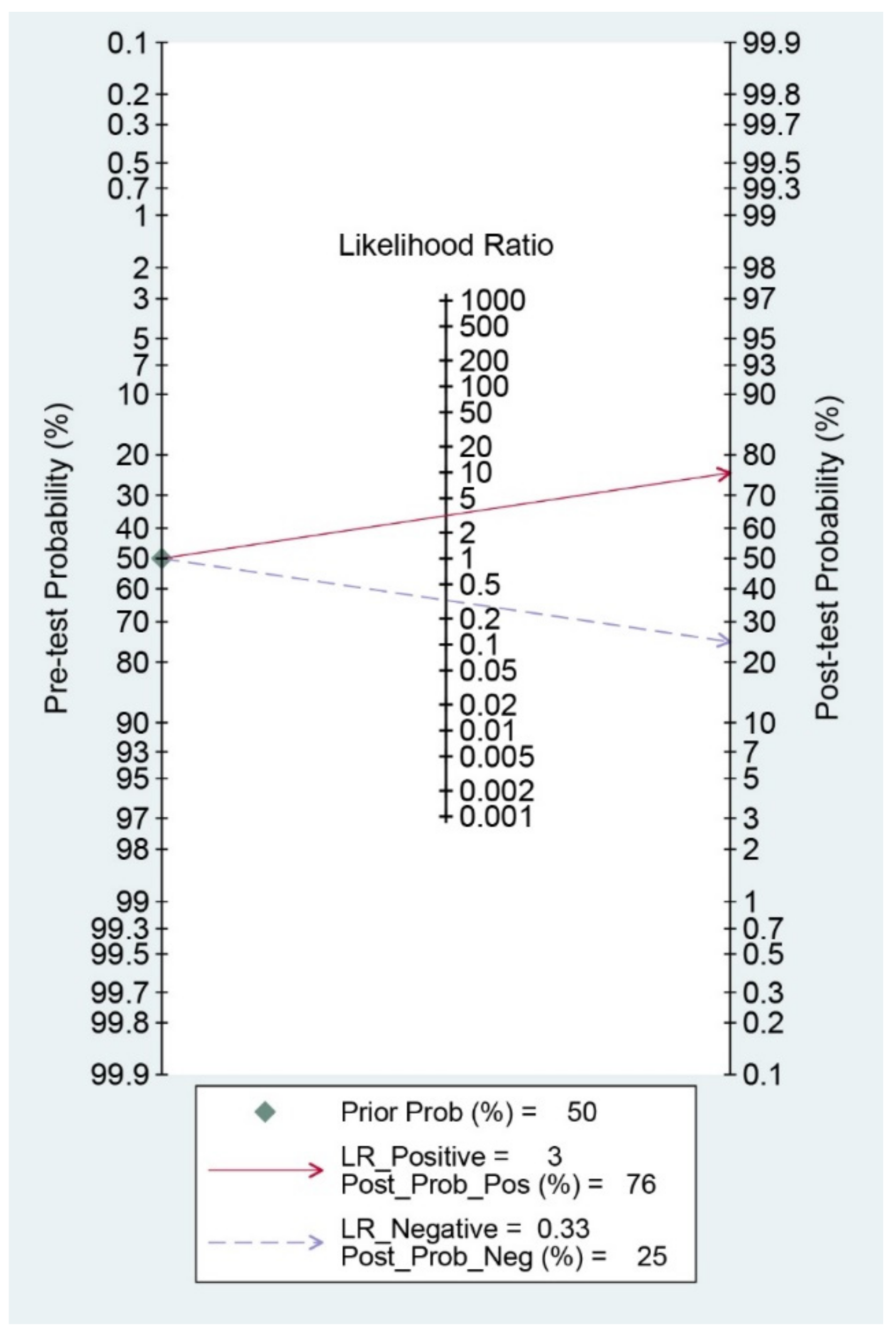
3.4. Diagnostic Indices of DNI for the Prediction of Prognosis of GI Diseases
3.5. Meta-Regression and Subgroup Analysis
3.6. Publication Bias
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Jung, H.K.; Jang, B.; Kim, Y.H.; Park, J.; Park, S.Y.; Nam, M.H.; Choi, M.G. Health care costs of digestive diseases in Korea. Korean J. Gastroenterol. 2011, 58, 323–331. [Google Scholar] [CrossRef]
- Peery, A.F.; Crockett, S.D.; Murphy, C.C.; Lund, J.L.; Dellon, E.S.; Williams, J.L.; Jensen, E.T.; Shaheen, N.J.; Barritt, A.S.; Lieber, S.R.; et al. Burden and Cost of Gastrointestinal, Liver, and Pancreatic Diseases in the United States: Update 2018. Gastroenterology 2019, 156, 254–272.e11. [Google Scholar] [CrossRef]
- Choi, J.H.; Bang, C.S.; Lee, J.J.; Baik, G.H. Delta neutrophil index as a predictor of disease severity, surgical outcomes, and mortality rates in gastrointestinal diseases: Rationale for a meta-analysis of diagnostic test accuracy. Medicine 2019, 98, e17059. [Google Scholar] [CrossRef]
- Barakat, M.T.; Mithal, A.; Huang, R.J.; Sehgal, A.; Sehgal, A.; Singh, G.; Banerjee, S. Recent Trends and the Impact of the Affordable Care Act on Emergency Department Visits and Hospitalizations for Gastrointestinal, Pancreatic, and Liver Diseases. J. Clin. Gastroenterol. 2020, 54, e21–e29. [Google Scholar] [CrossRef]
- Chan, J.S.H.; Chao, A.C.W.; Cheung, V.C.H.; Wong, S.S.K.; Tang, W.; Wu, J.C.Y.; Chan, H.L.Y.; Chan, F.K.L.; Sung, J.J.Y.; Ng, S.C. Gastrointestinal disease burden and mortality: A public hospital-based study from 2005 to 2014. J. Gastroenterol. Hepatol. 2019, 34, 124–131. [Google Scholar] [CrossRef]
- Hernandez, M.C.; Madbak, F.; Parikh, K.; Crandall, M. GI Surgical Emergencies: Scope and Burden of Disease. J. Gastrointest. Surg. 2019, 23, 827–836. [Google Scholar] [CrossRef]
- Kratz, A.; Maloum, K.; O’Malley, C.; Zini, G.; Rocco, V.; Zelmanovic, D.; Kling, G. Enumeration of nucleated red blood cells with the ADVIA 2120 Hematology System: An International Multicenter Clinical Trial. Lab. Hematol. 2006, 12, 63–70. [Google Scholar] [CrossRef]
- Ahn, C.; Kim, W.; Lim, T.H.; Cho, Y.; Choi, K.S.; Jang, B.H. The delta neutrophil index (DNI) as a prognostic marker for mortality in adults with sepsis: A systematic review and meta-analysis. Sci. Rep. 2018, 8, 6621. [Google Scholar] [CrossRef]
- Kim, T.Y.; Kim, S.J.; Kim, Y.S.; Lee, J.W.; Park, E.J.; Lee, S.J.; Lee, K.J.; Cha, Y.S. Delta neutrophil index as an early predictive marker of severe acute pancreatitis in the emergency department. United Eur. Gastroenterol. J. 2019, 7, 488–495. [Google Scholar] [CrossRef]
- Park, J.H.; Byeon, H.J.; Lee, K.H.; Lee, J.W.; Kronbichler, A.; Eisenhut, M.; Shin, J.I. Delta neutrophil index (DNI) as a novel diagnostic and prognostic marker of infection: A systematic review and meta-analysis. Inflamm. Res. 2017, 66, 863–870. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Bang, C.S.; Lee, J.J.; Baik, G.H. Prediction of Chronic Atrophic Gastritis and Gastric Neoplasms by Serum Pepsinogen Assay: A Systematic Review and Meta-Analysis of Diagnostic Test Accuracy. J. Clin. Med. 2019, 8, E657. [Google Scholar] [CrossRef]
- Reitsma, J.B.; Glas, A.S.; Rutjes, A.W.; Scholten, R.J.; Bossuyt, P.M.; Zwinderman, A.H. Bivariate analysis of sensitivity and specificity produces informative summary measures in diagnostic reviews. J. Clin. Epidemiol. 2005, 58, 982–990. [Google Scholar] [CrossRef]
- Rutter, C.M.; Gatsonis, C.A. A hierarchical regression approach to meta-analysis of diagnostic test accuracy evaluations. Stat. Med. 2001, 20, 2865–2884. [Google Scholar] [CrossRef]
- Harbord, R.M.; Whiting, P. Metandi: Meta-analysis of diagnostic accuracy using hierarchical logistic regression. Stata J. 2009, 9, 211–229. [Google Scholar] [CrossRef]
- Lee, S.J.; Park, E.J.; Lee, K.J.; Cha, Y.S. The delta neutrophil index is an early predictive marker of severe acute cholecystitis. Dig. Liver Dis. 2019, 51, 1593–1598. [Google Scholar] [CrossRef]
- Soh, J.S.; Lim, S.W. Delta neutrophil index as a prognostic marker in emergent abdominal surgery. J. Clin. Lab. Anal. 2019, 33, e22895. [Google Scholar] [CrossRef]
- Shin, D.H.; Cho, Y.S.; Kim, Y.S.; Ahn, H.C.; Oh, Y.T.; Park, S.O.; Won, M.H.; Cho, J.H.; Kim, Y.M.; Seo, J.Y.; et al. Delta neutrophil index: A reliable marker to differentiate perforated appendicitis from non-perforated appendicitis in the elderly. J. Clin. Lab. Anal. 2018, 32. [Google Scholar] [CrossRef]
- Lee, H.; Kim, I.K.; Ju, M.K. Which patients with intestinal obstruction need surgery? The delta neutrophil index as an early predictive marker. Ann. Surg. Treat. Res. 2017, 93, 272–276. [Google Scholar] [CrossRef]
- Kang, H.S.; Cha, Y.S.; Park, K.H.; Hwang, S.O. Delta neutrophil index as a promising prognostic marker of emergent surgical intervention for acute diverticulitis in the emergency department. PLoS ONE 2017, 12, e0187629. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Park, J.H.; Kim, D.J.; Choi, W.H.; Cheong, J.C.; Kim, J.Y. The delta neutrophil index is a prognostic factor for postoperative mortality in patients with sepsis caused by peritonitis. PLoS ONE 2017, 12, e0182325. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.H.; Cho, Y.S.; Cho, G.C.; Ahn, H.C.; Park, S.M.; Lim, S.W.; Oh, Y.T.; Cho, J.W.; Park, S.O.; Lee, Y.H. Delta neutrophil index as an early predictor of acute appendicitis and acute complicated appendicitis in adults. World J. Emerg. Surg. 2017, 12, 32. [Google Scholar] [CrossRef] [PubMed]
- Kong, T.; In, S.; Park, Y.S.; Lee, H.S.; Lee, J.W.; You, J.S.; Chung, H.S.; Park, I.; Chung, S.P. Usefulness of the delta neutrophil index to predict 30-day mortality in patients with upper gastrointestinal bleeding. Shock 2017, 48, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kong, T.; Chung, S.P.; Hong, J.H.; Lee, J.W.; Joo, Y.; Ko, D.R.; You, J.S.; Park, I. Usefulness of the delta neutrophil index as a promising prognostic marker of acute cholangitis in emergency departments. Shock 2017, 47, 303–311. [Google Scholar] [CrossRef]
- Cha, Y.S.; Lee, K.H.; Lee, J.W.; Choi, E.H.; Kim, H.I.; Kim, O.H.; Cha, K.C.; Hwang, S.O. The use of delta neutrophil index and myeloperoxidase index as diagnostic predictors of strangulated mechanical bowel obstruction in the emergency department. Medicine 2016, 95, e5481. [Google Scholar] [CrossRef]
- Lim, T.S.; Kim, B.K.; Lee, J.W.; Lee, Y.K.; Chang, S.; Kim, S.U.; Kim, D.Y.; Ahn, S.H.; Han, K.H.; Chon, C.Y.; et al. Use of the delta neutrophil Index as a prognostic factor of mortality in patients with spontaneous bacterial peritonitis: Implications of a simple and useful marker. PLoS ONE 2014, 9, e86884. [Google Scholar] [CrossRef]
- Alves-Filho, J.C.; Spiller, F.; Cunha, F.Q. Neutrophil paralysis in sepsis. Shock 2010, 34, 15–21. [Google Scholar] [CrossRef]
- Ansari-Lari, M.A.; Kickler, T.S.; Borowitz, M.J. Immature granulocyte measurement using the Sysmex XE-2100. Relationship to infection and sepsis. Am. J. Clin. Pathol. 2003, 120, 795–799. [Google Scholar] [CrossRef]
- Biomarkers Definitions Working Group Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [CrossRef]
- Park, S.H.; Bang, C.S.; Kim, D.J. Biomarkers in HCV Infection. Adv. Clin. Chem. 2015, 70, 131–196. [Google Scholar] [CrossRef] [PubMed]
- Ling, M.R.; Chapple, I.L.; Creese, A.J.; Matthews, J.B. Effects of C-reactive protein on the neutrophil respiratory burst in vitro. Innate Immun. 2014, 20, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Meier-Ewert, H.K.; Ridker, P.M.; Rifai, N.; Price, N.; Dinges, D.F.; Mullington, J.M. Absence of diurnal variation of C-reactive protein concentrations in healthy human subjects. Clin. Chem. 2001, 47, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Di Napoli, M.; Schwaninger, M.; Cappelli, R.; Ceccarelli, E.; Di Gianfilippo, G.; Donati, C.; Emsley, H.C.; Forconi, S.; Hopkins, S.J.; Masotti, L.; et al. Evaluation of C-reactive protein measurement for assessing the risk and prognosis in ischemic stroke: A statement for health care professionals from the CRP Pooling Project members. Stroke 2005, 36, 1316–1329. [Google Scholar] [CrossRef]
- Simon, L.; Gauvin, F.; Amre, D.K.; Saint-Louis, P.; Lacroix, J. Serum procalcitonin and C-reactive protein levels as markers of bacterial infection: A systematic review and meta-analysis. Clin. Infect. Dis. 2004, 39, 206–217. [Google Scholar] [CrossRef]
- Rhee, C. Using Procalcitonin to Guide Antibiotic Therapy. Open Forum Infect. Dis. 2016, 4, ofw249. [Google Scholar] [CrossRef]
- Wacker, C.; Prkno, A.; Brunkhorst, F.M.; Schlattmann, P. Procalcitonin as a diagnostic marker for sepsis: A systematic review and meta-analysis. Lancet Infect. Dis. 2013, 13, 426–435. [Google Scholar] [CrossRef]
- Park, S.J.; Park, J.; Lee, M.J.; Seo, J.S.; Ahn, J.Y.; Cho, J.W. Time series analysis of delta neutrophil index as the predictor of sepsis in patients with acute poisoning. Hum. Exp. Toxicol. 2020, 39, 86–94. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Diagnosis | Number of Patients | Number of Controls | Cut-off Value | Age (years, Mean ± SD) | Gender (M/F) | Multivariate Analysis (OR, (95% CI)) | TP | FP | FN | TN |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Kim TY et al. (2019) [9] | Severe acute pancreatitis | 13 | 196 | 1.8% | Median 65 (IQR: 50–78) | 119/90 | 1.122 (1.045–1.205) | 9 | 63 | 4 | 133 |
| Lee SJ et al. (2019) [17] | Severe acute cholecystitis | 28 | 351 | 3.5% | Median 62 (IQR: 52–73) | 214/165 | 1.97 (1.50–2.60) | 28 | 42 | 0 | 309 |
| Soh JS et al. (2019) [18] | 30-day mortality after emergent surgery due to acute peritonitis | 10 (mortality) | 174 (non-mortality) | 0.9% | Mortality: 59.1 ± 20.7, non-mortality: 53.5 ± 18.1 | 118/66 | 10 | 57 | 0 | 117 | |
| Shin DH et al. (2018) [19] | Acute perforated appendicitis (vs. non-perforated appendicitis) | 69 | 39 | 1.4% | Median 72 (IQR: 67–77) | 42/66 | 9.38 (2.51–35) | 47 | 4 | 22 | 35 |
| Lee H et al. (2017) [20] | Need for surgery in patients with intestinal obstruction | 38 | 133 | 4.3% | Median 60 (range: 20–90) | 87/84 | 3.092 (1.072–8.918) (cut-off 4.3% standard) | 9 | 14 | 29 | 119 |
| Kang HS et al. (2017) [21] | Need for surgery in patients with acute colonic diverticulitis | 52 | 80 | 0.7% | Median 56 (IQR: 41–71) | 72/60 | 1.664 (1.203–2.301) | 49 | 16 | 3 | 64 |
| Kim JW et al. (2017) [22] | 30-day mortality after emergent surgery due to acute peritonitis | 44 (mortality) | 116 (non-mortality) | 7.8% (at day 3) | Median 70 (IQR: 59–79) | 96/64 | 1.286 (1.145–1.444) | 34 | 5 | 10 | 111 |
| Shin DH et al. (2017) [23] | Acute complicated appendicitis (vs. non-complicated appendicitis) | 177 | 438 | 0.6% | Median 35 (IQR: 23–48) | 320/295 | 4.10 (2.94–5.80) | 115 | 127 | 62 | 311 |
| Kong T et al. (2017) [24] | 30-day mortality in patients with upper gastrointestinal hemorrhage | 38 (mortality) | 394 (non-mortality) | 1% (at admission) | 63.9 ± 14.4 | 297/135 | HR: 1.09 (1.019–1.166) | 13 | 308 | 25 | 86 |
| Kim H et al. (2017) [25] | Shock requiring vasopressor or inotrope in acute cholangitis | 74 | 387 | 4.3% | 66.22 ± 13.02 | 253/208 | 1.103 (1.045–1.164) | 53 | 84 | 21 | 303 |
| 28-day mortality in acute cholangitis | 17 | 444 | 4.7% | HR: 1.102 (1.053–1.153) | 12 | 111 | 5 | 333 | |||
| Cha YS et al. (2016) [26] | Need for surgery in patients with strangulated mechanical bowel obstruction | 15 | 145 | Median 69 (IQR: 54–76) | 96/64 | ||||||
| Lim TS et al. (2014) [27] | 30-day mortality in patients with spontaneous bacterial peritonitis | 19 | 56 | 5.7% | Median 59 (range: 38–82) | 65/10 | 11 | 8 | 8 | 48 |
| Subgroup | Number of Included Studies | Sensitivity (95% CI) | Specificity (95% CI) | PLR | NLR | DOR | AUC |
|---|---|---|---|---|---|---|---|
| Value of meta-analysis in all the included studies | 10 | 0.75 (0.52–0.89) | 0.76 (0.63–0.86) | 3.1 (1.8–5.6) | 0.33 (0.15–0.74) | 10 (3–35) | 0.82 (0.78–0.85) |
| Age (years, median or mean) | |||||||
| <60 | 4 | 0.85 (0.54–0.96) | 0.75 (0.67–0.81) | 3.4 (2.4–4.6) | 0.20 (0.06–0.74) | 16 (4–74) | 0.81 (0.77–0.84) |
| 60≤ | 6 | 0.67 (0.36–0.88) | 0.76 (0.54–0.90) | 2.8 (1.0–7.5) | 0.43 (0.16–1.15) | 6 (1–42) | 0.78 (0.75–0.82) |
| Quality of methodology of included studies | |||||||
| High-quality | 8 | 0.73 (0.53–0.86) | 0.73 (0.57–0.84) | 2.7 (1.4–5.2) | 0.38 (0.18–0.78) | 7 (2–27) | 0.79 (0.75–0.82) |
| Low-quality | 2 | Null | Null | Null | Null | Null | Null |
| Gender | |||||||
| Male-predominant | 9 | 0.77 (0.50–0.92) | 0.74 (0.60–0.85) | 3.0 (1.6–5.5) | 0.31 (0.12–0.83) | 10 (2–43) | 0.81 (0.78–0.84) |
| Female-predominant | 1 | Null | Null | Null | Null | Null | Null |
| Format of study | |||||||
| Case-control | 8 | 0.81 (0.53–0.94) | 0.81 (0.73–0.87) | 4.2 (2.9–6.2) | 0.24 (0.08–0.67) | 18 (5–65) | 0.86 (0.82–0.88) |
| Cohort | 2 | Null | Null | Null | Null | Null | Null |
| Published year | |||||||
| Before 2018 | 6 | 0.61 (0.37–0.81) | 0.74 (0.53–0.87) | 2.3 (1.0–5.4) | 0.53 (0.26–1.06) | 4 (1–19) | 0.73 (0.69–0.77) |
| After 2018 | 4 | 0.93 (0.47–0.99) | 0.79 (0.66–0.88) | 4.5 (2.5–7.9) | 0.09 (0.01–1.14) | 53 (3–954) | 0.88 (0.85–0.91) |
| Total number of included subjects | |||||||
| <200 | 5 | 0.81 (0.39–0.97) | 0.83 (0.74–0.89) | 4.7 (3.5–6.2) | 0.22 (0.05–0.99) | 20 (4–95) | 0.90 (0.87–0.92) |
| 200≤ | 5 | 0.66 (0.47–0.81) | 0.68 (0.44–0.85) | 2.0 (0.8–5.1) | 0.51 (0.22–1.15) | 4 (1–23) | 0.72 (0.67–0.75) |
| Surgical condition vs. medical condition | |||||||
| Surgical condition | 6 | 0.87 (0.49–0.98) | 0.82 (0.73–0.88) | 4.8 (3.2–7.4) | 0.15 (0.03–0.86) | 31 (5–214) | 0.87 (0.84–0.90) |
| Medical condition | 4 | 0.60 (0.43–0.75) | 0.64 (0.37–0.85) | 1.7 (0.6–4.4) | 0.62 (0.29–1.36) | 3 (0–15) | 0.65 (0.60–0.69) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, H.M.; Bang, C.S.; Lee, J.J.; Baik, G.H. Delta Neutrophil Index for the Prediction of Prognosis in Acute Gastrointestinal Diseases; Diagnostic Test Accuracy Meta-Analysis. J. Clin. Med. 2020, 9, 1133. https://doi.org/10.3390/jcm9041133
Jeong HM, Bang CS, Lee JJ, Baik GH. Delta Neutrophil Index for the Prediction of Prognosis in Acute Gastrointestinal Diseases; Diagnostic Test Accuracy Meta-Analysis. Journal of Clinical Medicine. 2020; 9(4):1133. https://doi.org/10.3390/jcm9041133
Chicago/Turabian StyleJeong, Hae Min, Chang Seok Bang, Jae Jun Lee, and Gwang Ho Baik. 2020. "Delta Neutrophil Index for the Prediction of Prognosis in Acute Gastrointestinal Diseases; Diagnostic Test Accuracy Meta-Analysis" Journal of Clinical Medicine 9, no. 4: 1133. https://doi.org/10.3390/jcm9041133
APA StyleJeong, H. M., Bang, C. S., Lee, J. J., & Baik, G. H. (2020). Delta Neutrophil Index for the Prediction of Prognosis in Acute Gastrointestinal Diseases; Diagnostic Test Accuracy Meta-Analysis. Journal of Clinical Medicine, 9(4), 1133. https://doi.org/10.3390/jcm9041133