Effects of Self-Care for Older PErsons (SCOPE) on Functional and Physiological Measures: A Cluster Randomized Controlled Trial


Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Subject Recruitment
2.3. SCOPE Intervention
2.4. Control Group
3. Outcome Measures
3.1. Primary Outcome Measure
3.2. Secondary Outcome Measures
3.2.1. Functional Measurements
3.2.2. Physiological Measurements
4. Statistical Analyses
4.1. Sample Size Calculation
- m = number of participants in each cluster
- kmax = the maximum number of clusters that can be assigned in each arm
- k(m=1) = the number of clusters in each arm that would be required if m = 1
- µ1 = population mean in treatment arm 1
- µ2 = population mean in treatment arm 2
- µ1 − µ2 = the difference in means between the two arms to detect
- σ2 = population variance
- ρ = intra cluster correlation coefficient
- tα/2 = critical value for α = 0.05
- tβ = critical value for β = 0.2
4.2. Primary Composite Measure
4.3. Secondary Measures
5. Results
5.1. Baseline Demographics and Characteristics
5.2. Effects of SCOPE on Primary Outcome
5.3. Effects of SCOPE on Secondary Outcomes: Functional and Physiological Measures
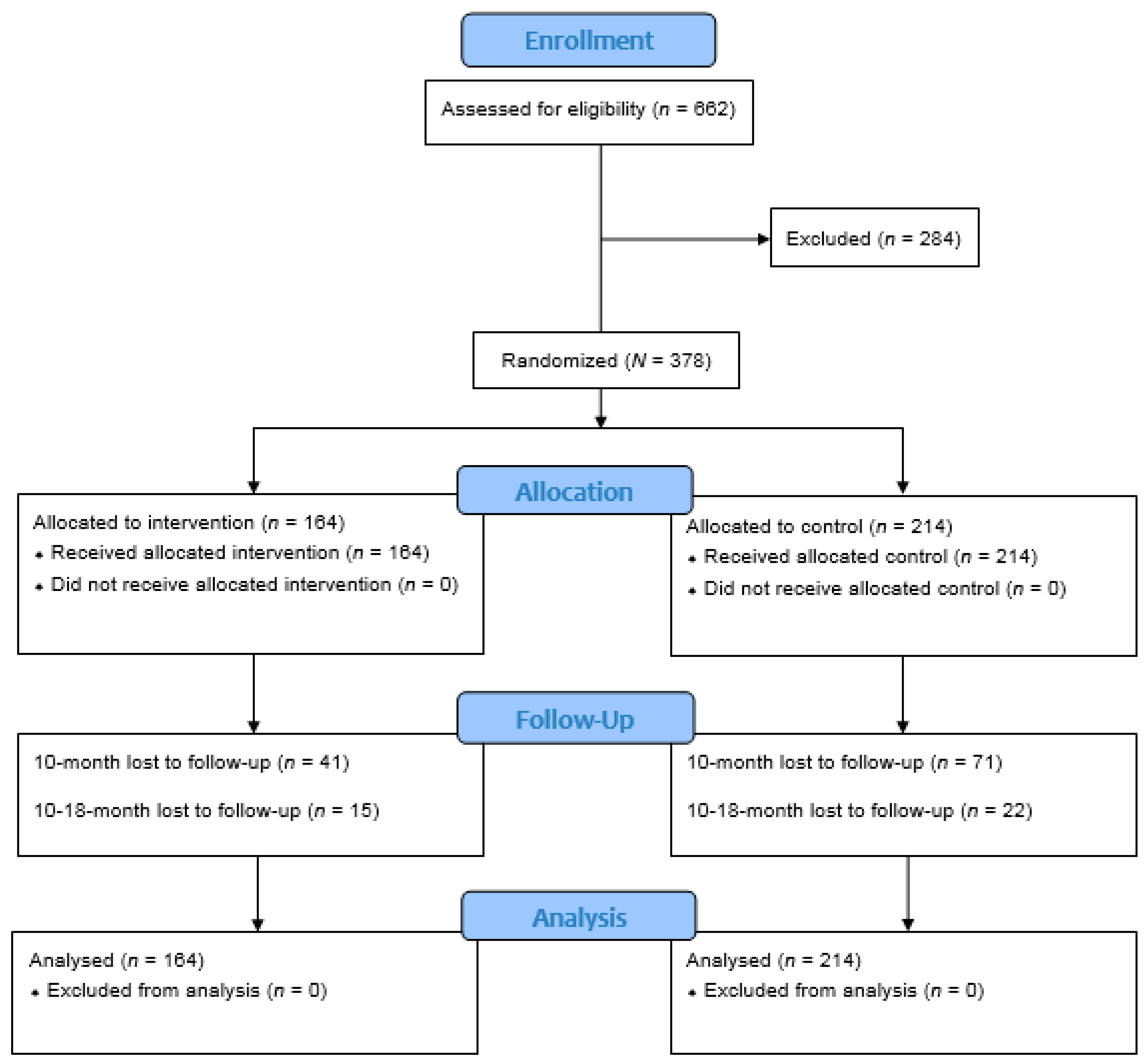
5.4. Loss-to-Follow-up
6. Discussion
7. Conclusions and Implications
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lorig, K.R.; Sobel, D.S.; Stewart, A.L.; Brown, B.W., Jr.; Bandura, A.; Ritter, P.; Gonzalez, V.M.; Laurent, D.D.; Holman, H.R. Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalization: A randomized trial. Med. Care 1999, 37, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.R.; Ritter, P.; Stewart, A.L.; Sobel, D.S.; Brown, B.W., Jr.; Bandura, A.; Gonzalez, V.M.; Laurent, D.D.; Holman, H.R. Chronic disease self-management program: 2-year health status and health care utilization outcomes. Med. Care 2001, 39, 1217–1223. [Google Scholar] [CrossRef] [PubMed]
- Jones, H.; Edwards, L.; Vallis, T.M.; Ruggiero, L.; Rossi, S.R.; Rossi, J.S.; Greene, G.; Prochaska, J.O.; Zinman, B. Changes in diabetes self-care behaviors make a difference in glycemic control: The Diabetes Stages of Change (DiSC) study. Diabetes Care 2003, 26, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Norris, S.L.; Lau, J.; Smith, S.J.; Schmid, C.H.; Engelgau, M.M. Self-management education for adults with type 2 diabetes: A meta-analysis of the effect on glycemic control. Diabetes Care 2002, 25, 1159–1171. [Google Scholar] [CrossRef]
- Iso, H.; Shimamoto, T.; Yokota, K.; Sankai, T.; Jacobs, D.R.; Komachi, Y. Community-based education classes for hypertension control: A 1.5-year randomized controlled trial. Hypertension 1996, 27, 968–974. [Google Scholar] [CrossRef]
- Chodosh, J.; Morton, S.C.; Mojica, W.; Maglione, M.; Suttorp, M.J.; Hilton, L.; Rhodes, S.; Shekelle, P. Meta-analysis: Chronic disease self-management programs for older adults. Ann. Intern. Med. 2005, 143, 427–438. [Google Scholar] [CrossRef]
- Worth, H.; Dhein, Y. Does patient education modify behaviour in the management of COPD? Patient Educ. Couns. 2004, 52, 267–270. [Google Scholar] [CrossRef]
- Lorig, K.R.; Sobel, D.S.; Ritter, P.L.; Laurent, D.; Hobbs, M. Effect of a self-management program on patients with chronic disease. Eff. Clin. Pract. ECP 2001, 4, 256–262. [Google Scholar]
- Bandura, A. Social Foundations of Thought and Action; Prentice Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Huang, O.S.; Tay, W.T.; Tai, E.S.; Wang, J.J.; Saw, S.-M.; Jeganathan, V.S.; Sandar, M.; Wong, T.Y. Lack of awareness amongst community patients with diabetes and diabetic retinopathy: The Singapore Malay eye study. Ann. Acad. Med. Singap. 2009, 38, 1048–1055. [Google Scholar]
- DeFriese, G.H.; Ory, M.G. Self Care in Later Life: Research, Program, and Policy Issues; Springer Publishing Company: New York, NY, USA, 1998. [Google Scholar]
- Dale, B.; Söderhamn, U.; Söderhamn, O. Self-care ability among home-dwelling older people in rural areas in southern Norway. Scand. J. Caring Sci. 2012, 26, 113–122. [Google Scholar] [CrossRef]
- Badzek, L.; Hines, S.C.; Moss, A.H. Inadequate self-care knowledge among elderly hemodialysis patients: Assessing its prevalence and potential causes. Nephrol. Nurs. J. 1998, 25, 293. [Google Scholar]
- Rockwell, J.M.; Riegel, B. Predictors of self-care in persons with heart failure. Heart Lung 2001, 30, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy mechanism in human agency. Am. Psychol. 1982, 37, 122. [Google Scholar] [CrossRef]
- Bandura, A.; Freeman, W.; Lightsey, R. Self-Efficacy: The Exercise of Control; Springer: New York, NY, USA, 1999. [Google Scholar]
- Israel, B.A.; Checkoway, B.; Schulz, A.; Zimmerman, M. Health education and community empowerment: Conceptualizing and measuring perceptions of individual, organizational, and community control. Health Educ. Q. 1994, 21, 149–170. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.; Matchar, D.B.; Tsao, M.A.; Harding, S.; Chiu, C.-T.; Tay, B.; Raman, P.; Pietryla, Z.; Klein, M.K.; Haldane, V.E. Self-Care for Older People (SCOPE): A cluster randomized controlled trial of self-care training and health outcomes in low-income elderly in Singapore. Contemp. Clin. Trials 2015, 41, 313–324. [Google Scholar] [CrossRef]
- International Expert Committee. International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care 2009, 32, 1327–1334. [Google Scholar] [CrossRef]
- WHO. Use of Glycated Haemoglobin (HbA1c) in Diagnosis of Diabetes Mellitus: Abbreviated Report of a WHO Consultation; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Jackson, H.; Hubbard, R. Detecting chronic obstructive pulmonary disease using peak flow rate: Cross sectional survey. BMJ 2003, 327, 653–654. [Google Scholar] [CrossRef]
- National Institutes of Health. Guidelines for the Diagnosis and Management of Asthma. In Expert Panel Report 2: Guidelines for the Diagnosis and Management of Asthma; National Institutes of Health: Bethesda, MD, USA, 1998. [Google Scholar]
- Malhotra, R.; Malhotra, C.; Chan, A.; Østbye, T. Life-course socioeconomic status and obesity among older Singaporean Chinese men and women. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2012, 68, 117–127. [Google Scholar] [CrossRef]
- Health SMo. National Health Survey 2004; Ministry of Health of Singapore: Singapore, 2005.
- Donner, A.; Klar, N. Sample size estimation for cluster randomization designs. In Design and Analysis of Cluster Randomization Trials in Health Research; Wiley: Hoboken, NJ, USA, 2010. [Google Scholar]
- Chen, S.-Y.; Feng, Z.; Yi, X. A general introduction to adjustment for multiple comparisons. J. Thorac. Dis. 2017, 9, 1725. [Google Scholar] [CrossRef] [PubMed]
- Sedgwick, P. Multiple hypothesis testing and Bonferroni’s correction. Bmj 2014, 349, g6284. [Google Scholar] [CrossRef]
- Althouse, A.D. Adjust for multiple comparisons? It’s not that simple. Ann. Thorac. Surg. 2016, 101, 1644–1645. [Google Scholar] [CrossRef] [PubMed]
- Verbeke, G.; Molenberghs, G. Linear Mixed Models for Longitudinal Data; Springer Science & Business Media: Medford, MA, USA, 2009. [Google Scholar]
- Katz, S. Assessing self-maintenance: Activities of daily living, mobility, and instrumental activities of daily living. J. Am. Geriatr. Soc. 1983, 31, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.; Kourlaba, G.; Zeimbekis, A.; Toutouzas, P.; Polychronopoulos, E. The J-shape association of alcohol consumption on blood pressure levels, in elderly people from Mediterranean Islands (MEDIS epidemiological study). J. Hum. Hypertens. 2007, 21, 585. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Sherlock, P.; Beard, J.; Minicuci, N.; Ebrahim, S.; Chatterji, S. Hypertension among older adults in low-and middle-income countries: Prevalence, awareness and control. Int. J. Epidemiol. 2014, 43, 116–128. [Google Scholar] [CrossRef]
- Lorig, K.; Ritter, P.L.; Plant, K. A disease-specific self-help program compared with a generalized chronic disease self-help program for arthritis patients. Arthritis Care Res. Off. J. Am. Coll. Rheumatol. 2005, 53, 950–957. [Google Scholar] [CrossRef]
- Breitenstein, S.M.; Gross, D.; Garvey, C.A.; Hill, C.; Fogg, L.; Resnick, B. Implementation fidelity in community-based interventions. Res. Nurs. Health 2010, 33, 164–173. [Google Scholar] [CrossRef]
- Bohannon, R.W. Sit-to-stand test for measuring performance of lower extremity muscles. Percept. Motor Skills 1995, 80, 163–166. [Google Scholar] [CrossRef]
- Jones, C.J.; Rikli, R.E.; Beam, W.C. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res. Q. Exerc. Sport 1999, 70, 113–119. [Google Scholar] [CrossRef]
- Moreland, J.D.; Richardson, J.A.; Goldsmith, C.H.; Clase, C.M. Muscle weakness and falls in older adults: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2004, 52, 1121–1129. [Google Scholar] [CrossRef]
- Al-Thihli, K.; Sinclair, G.; Sirrs, S.; Mezei, M.; Nelson, J.; Vallance, H. Performance of serum and dried blood spot acylcarnitine profiles for detection of fatty acid β-oxidation disorders in adult patients with rhabdomyolysis. J. Inherit. Metab. Dis. 2014, 37, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, N.; Nakatani, T.; Morita, N.; Saeki, K.; Kurumatani, N. Home-based walking improves cardiopulmonary function and health-related QOL in community-dwelling adults. Int. J. Sports Med. 2007, 28, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Brubaker, P.H.; Kitzman, D.W. Chronotropic incompetence: Causes, consequences, and management. Circulation 2011, 123, 1010–1020. [Google Scholar] [CrossRef] [PubMed]
- Hollmann, W.; Strüder, H.K.; Tagarakis, C.V.; King, G. Physical activity and the elderly. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 730–739. [Google Scholar] [CrossRef]
- Son, S.M.; Kim, M.J. The effect of nutrition education program for various chronic disease in elderly visiting public health center. Korean J. Community Nutr. 2001, 6, 668–677. [Google Scholar]
- Baik, H.; Russell, R. Vitamin B12 deficiency in the elderly. Annu. Rev. Nutr. 1999, 19, 357–377. [Google Scholar] [CrossRef]
- Kwok, T.; Cheng, G.; Woo, J.; Lai, W.; Pang, C. Independent effect of vitamin B12 deficiency on hematological status in older Chinese vegetarian women. Am. J. Hematol. 2002, 70, 186–190. [Google Scholar] [CrossRef]
- Rose, M.A.; Arenson, C.; Harrod, P.; Salkey, R.; Santana, A.; Diamond, J. Evaluation of the chronic disease self-management program with low-income, urban, African American older adults. J. Community Health Nurs. 2008, 25, 193–202. [Google Scholar] [CrossRef]
- Collard, C.; Robinson-Dooley, V.; Patrick, F.; Farabaugh, K. Efficacy of Chronic Disease Self-Management among Low-Income Black Males with Behavioral Health Disorders: Pilot Study. J. Ga. Public Health Assoc. 2016, 6, 4. [Google Scholar]
- Jerant, A.; Moore-Hill, M.; Franks, P. Home-based, peer-led chronic illness self-management training: Findings from a 1-year randomized controlled trial. Ann. Fam. Med. 2009, 7, 319–327. [Google Scholar] [CrossRef]


{kind=link}
| Demographics Characteristics | Intervention (n = 164) mean ± SD n (%) | Control (n = 214) mean ± SD n (%) | p-Value |
|---|---|---|---|
| Age (in years) | 72.22 ± 7.79 | 72.16 ± 8.24 | 0.942 |
| Age group (in years) | |||
| 55–60 | 12 (7.3) | 15 (7) | 0.611 |
| 61–65 | 23 (14.0) | 37 (17.3) | |
| 66–70 | 31 (18.9) | 39 (18.3) | |
| 71–75 | 42 (25.6) | 47 (22.1) | |
| 76–80 | 35 (21.3) | 35 (16.4) | |
| 81–85 | 14 (8.5) | 28 (13.1) | |
| ≥85 | 7 (4.3) | 12 (5.6) | |
| Gender | |||
| Female | 104 (63.3) | 147 (68.7) | 0.282 |
| Male | 60 (36.6) | 67 (31.3) | |
| Ethnicity | 0.032 * | ||
| Chinese | 144 (87.8) | 170 (79.4) | |
| Non-Chinese | 20 (12.2) | 44 (20.6) | |
| Education | 0.260 | ||
| No formal education and primary school education only | 30 (18.3) | 30 (14) | |
| Secondary school education and above | 134 (81.7) | 184 (86) | |
| Marital Status | <0.001 *** | ||
| Married | 72 (43.9) | 137 (64) | |
| Not married | 92 (56.1) | 77 (36) | |
| Working Status | 0.400 | ||
| Holding full-time or part-time job | 18 (11) | 18 (8.4) | |
| Not working/retiree/housewife | 146 (89) | 196 (91.6) | |
| Housing Type | 0.802 | ||
| 1–3 room public housing | 149 (90.9) | 196 (91.6) | |
| ≥4 room public housing /private housing | 15 (9.1) | 18 (8.4) | |
| BMI (kg/m2) | 24.13 ± 4.73 | 24.52 ± 4.98 | 0.447 |
| Number of morbidities | 2.46 ± 1.58 | 2.31 ± 1.62 | 0.386 |
| Composite Measures | Time-Points | Intervention Group | Control Group | Estimate (SE) | 95% CI of the Estimates | t | p−Value |
|---|---|---|---|---|---|---|---|
| Cases with at Least One Improvement/Total Number of Cases (% of Cases with at Least One Improvement) | Cases with at Least One Improvement/Total Number of Cases (% of Cases with at Least One Improvement) | ||||||
| Original dataset | 10-month | 36/123 (29.3%) | 40/143 (28%) | −0.067 | −0.577 to 0.442 | −2.06 | 0.795 |
| 18-month | 30/108 (27.8%) | 29/121 (24%) | −0.214 | −0.782 to 0.354 | −0.74 | 0.459 | |
| Missing values replaced with 1 | 10-month | 77/164 (46%) | 111/214 (51.9%) | 0.191 | −0.341 to 0.7237 | 0.75 | 0.463 |
| 18-month | 86/164 (52.4%) | 122/214 (57%) | 0.179 | −0.354 to 0.712 | 0.70 | 0.493 | |
| Missing values replaced with 0 | 10-month | 36/164 (22%) | 40/214 (18.7%) | −0.255 | −1.027 to 0.518 | −0.70 | 0.495 |
| 18-month | 30/164 (18.3%) | 29/214 (13.6%) | −0.413 | −1.215 to 0.389 | −1.07 | 0.296 |
| Measures | Time-Points | Intervention | 95% CI | Control | 95% CI | Estimate | 95% CI of the Estimates | t | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| (Units) | Mean ± SE (N) | Mean ± SE (N) | (SE) | ||||||
| Time to completing chair-stand test (seconds) | Baseline | 12.37 (0.34) | 11.70 to 13.04 | 11.93 (0.32) | 11.30 to 12.57 | Reference | Reference | Reference | Reference |
| 10-month | 10.27 (0.36) | 9.57 to 10.98 | 12.29 (0.35) | 11.61 to 12.98 | 2.45 (0.41) | 1.65 to 3.25 | 5.99 | <0.001 | |
| 18-month | 10.04 (0.37) | 9.21 to 10.77 | 12.16 (0.36) | 11.45 to 12.87 | 2.55 (0.46) | 1.64 to 3.45 | 5.53 | <0.001 | |
| Oxygen desaturation after chair-stand test (%) | Baseline | −0.23 (0.15) | −0.52 to 0.06 | 0.08 (0.14) | −0.19 to 0.35 | Reference | Reference | Reference | Reference |
| 10-month | −0.06 (0.16) | −0.36 to 0.25 | −0.41 (0.15) | −0.71 to −0.12 | −0.66 (0.21) | −1.08 to −0.25 | 0.28 | 0.002 | |
| 18-month | −0.04 (0.16) | −0.36 to 0.28 | −0.47 (0.16) | −0.78 to −0.17 | −0.74 (0.22) | −1.17 to −0.32 | 0.24 | 0.001 | |
| Difference in heart rate after chair-stand test (BPM) | Baseline | 10.80 (0.72) | 9.38 to 12.22 | 10.79 (0.68) | 9.45 to 12.14 | Reference | Reference | Reference | Reference |
| 10-month | 12.38 (0.77) | 10.87 to 13.89 | 9.72 (0.75) | 8.25 to 11.18 | −2.66 (0.96) | −4.54 to −0.78 | 0.006 | 0.006 | |
| 18-month | 10.31 (0.79) | 8.75 to 11.86 | 10.91 (0.77) | 9.39 to 12.42 | 0.60 (1.03) | −1.41 to 2.62 | 0.558 | 0.558 |
| Measures | Time-Points | Intervention | 95% CI | Control | 95% CI | Estimate | 95% CI of the Estimates | t | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| (Units) | Mean ± SE (N) | Mean ± SE (N) | (SE) | ||||||
| Vitamin B12 (pmol/L) | Baseline | 291.57 (12.52) | 266.99 to 316.15 | 289.49 (11.97) | 265.97 to 313.00 | Reference | Reference | Reference | Reference |
| 10-month | 336.46 (13.14) | 310.66 to 362.26 | 321.99 (12.76) | 296.93 to 347.05 | −12.39 (13.53) | −38.96 to 14.19 | −0.915 | 0.360 | |
| 18-month | 397.22 (13.49) | 370.74 to 423.71 | 329.31 (13.13) | 3030.52 to 355.10 | −65.83 (15.73) | −96.71 to −34.96 | −4.185 | <0.001 | |
| Hemoglobin concentration (g/dL) | Baseline | 13.26 (0.07) | 13.13 to 13.40 | 13.30 (0.07) | 13.17 to 13.43 | Reference | Reference | Reference | Reference |
| 10-month | 13.50 (0.07) | 13.40 to 13.64 | 13.26 (0.07) | 13.13 to 13.40 | −0.27 (0.07) | −0.41 to −0.12 | −3.63 | <0.001 | |
| 18-month | 13.28 (0.07) | 13.14 to 13.42 | 13.29 (0.07) | 13.15 to 13.43 | −0.03 (0.09) | −0.19 to 0.14 | −0.19 | 0.758 | |
| MCV (fl) | Baseline | 90.04 (0.25) | 89.55 to 90.53 | 89.94 (0.24) | 89.47 to 90.41 | Reference | Reference | Reference | Reference |
| 10-month | 89.86 (0.26) | 89.35 to 90.38 | 90.69 (0.25) | 90.19 to 91.19 | 0.93 (0.27) | 0.39 to 1.47 | 3.39 | 0.001 | |
| 18-month | 89.27 (0.27) | 88.74 to 89.80 | 89.77 (0.26) | 89.26 to 90.29 | 0.60 (0.32) | −0.20 to 1.23 | 1.90 | 0.058 | |
| HDL Cholesterol (mmol/L) | Baseline | 1.52 (0.01) | 1.50 to 1.55 | 1.52 (0.01) | 1.50 to 1.54 | Reference | Reference | Reference | Reference |
| 10-month | 1.49 (0.01) | 1.46 to 1.52 | 1.56 (0.01) | 1.54 to 1.59 | 0.08 (0.02) | 0.05 to 0.11 | 4.53 | <0.001 | |
| 18-month | 1.51 (0.01) | 1.48 to 1.54 | 1.51 (0.01) | 1.48 to 1.53 | 0.01 (0.02) | −0.03 to 0.04 | 0.04 | 0.969 | |
| Total Cholesterol/HDL Cholesterol (mmol/L) | Baseline | 3.48 (0.04) | 3.40 to 3.56 | 3.50 (0.04) | 3.43 to 3.57 | Reference | Reference | Reference | Reference |
| 10-month | 3.54 (0.04) | 3.46 to 3.62 | 3.40 (0.04) | 3.32 to 3.48 | −0.15 (0.05) | −0.25 to −0.06 | −3.29 | 0.001 | |
| 18-month | 3.46 (0.04) | 3.38 to 3.54 | 3.46 (0.04) | 3.38 to 3.54 | −0.02 (0.05) | −0.41 to −0.69 | 0.69 | 0.08 | |
| Creatinine (umol/L) | Baseline | 75.98 (0.96) | 74.10 to 77.86 | 76.26 (0.91) | 74.48 to 78.05 | Reference | Reference | Reference | Reference |
| 10-month | 80.95 (1.02) | 78.95 to 82.95 | 85.15 (0.99) | 83.22 to 87.09 | 3.92 (1.27) | 1.42 to 6.43 | 3.08 | 0.002 | |
| 18-month | 77.30 (1.04) | 75.25 to 79.35 | 77.16 (1.01) | 75.17 to 79.15 | −0.42 (1.36) | −3.08 to 2.25 | −0.31 | 0.756 | |
| Waist circumference (cm) | Baseline | 94.34 (11.94) | 70.89 to 117.79 | 95.94 (11.30) | 73.75 to 118.13 | Reference | Reference | Reference | Reference |
| 10-month | 94.81 (12.78) | 69.72 to 119.89 | 132.22 (12.35) | 107.97 to 156.47 | 35.82 (17.16) | 2.12 to 69.52 | 2.087 | 0.037 | |
| 18-month | 117.55 (13.03) | 91.98 to 143.12 | 123.21 (12.71) | 98.27 to 148.15 | 4.06 (17.42) | −30.12 to 38.25 | 0.233 | 0.816 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ng, T.K.S.; Matchar, D.B.; Sultana, R.; Chan, A. Effects of Self-Care for Older PErsons (SCOPE) on Functional and Physiological Measures: A Cluster Randomized Controlled Trial. J. Clin. Med. 2020, 9, 885. https://doi.org/10.3390/jcm9030885
Ng TKS, Matchar DB, Sultana R, Chan A. Effects of Self-Care for Older PErsons (SCOPE) on Functional and Physiological Measures: A Cluster Randomized Controlled Trial. Journal of Clinical Medicine. 2020; 9(3):885. https://doi.org/10.3390/jcm9030885
Chicago/Turabian StyleNg, Ted Kheng Siang, David Bruce Matchar, Rehena Sultana, and Angelique Chan. 2020. "Effects of Self-Care for Older PErsons (SCOPE) on Functional and Physiological Measures: A Cluster Randomized Controlled Trial" Journal of Clinical Medicine 9, no. 3: 885. https://doi.org/10.3390/jcm9030885
APA StyleNg, T. K. S., Matchar, D. B., Sultana, R., & Chan, A. (2020). Effects of Self-Care for Older PErsons (SCOPE) on Functional and Physiological Measures: A Cluster Randomized Controlled Trial. Journal of Clinical Medicine, 9(3), 885. https://doi.org/10.3390/jcm9030885