Body Mass Index and Calprotectin Blood Level Correlation in Healthy Children: An Individual Patient Data Meta-Analysis

 ,
, 
 , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Eligibility Criteria
2.3. Search Strategy and Selection Criteria
2.4. Data Extraction, Evaluation, and Synthesis
2.5. Data Extraction
2.6. Risk of Bias and Assessment of Study Quality
2.7. Statistical Considerations
3. Results
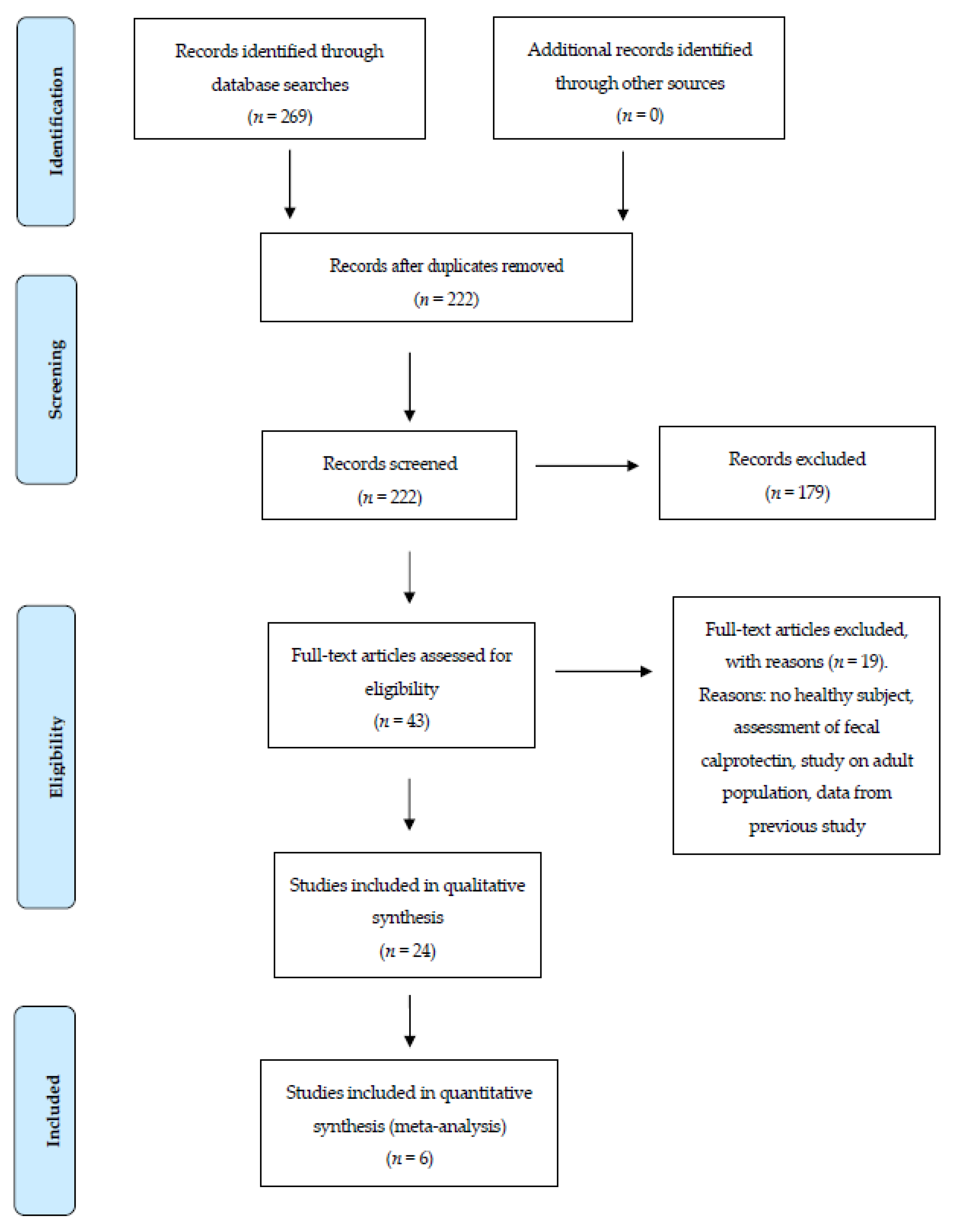
3.1. Studies Selection
3.2. Study Characteristics
3.3. Subject Characteristics
3.4. Meta-Analysis and Sensitivity Analysis
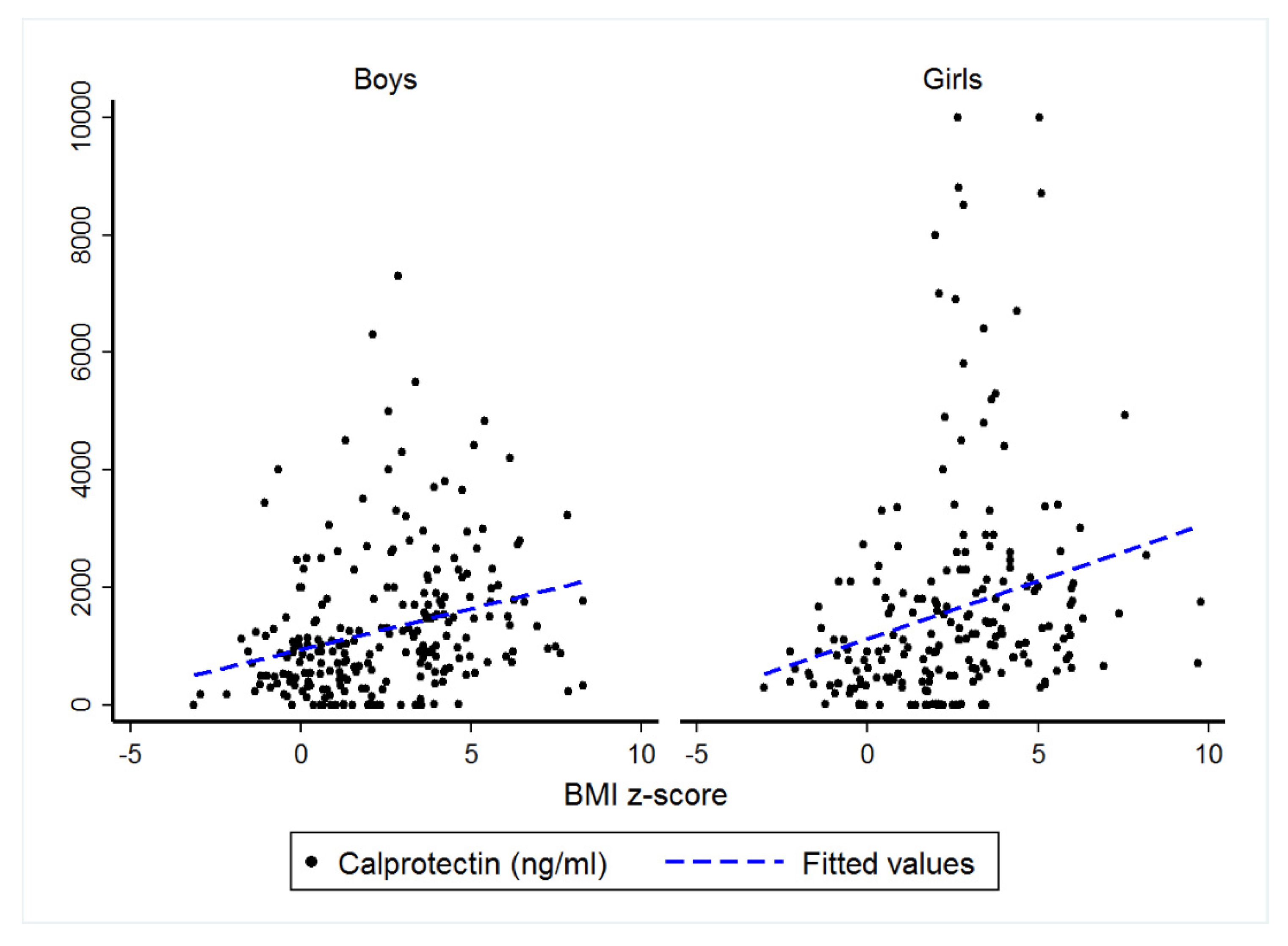
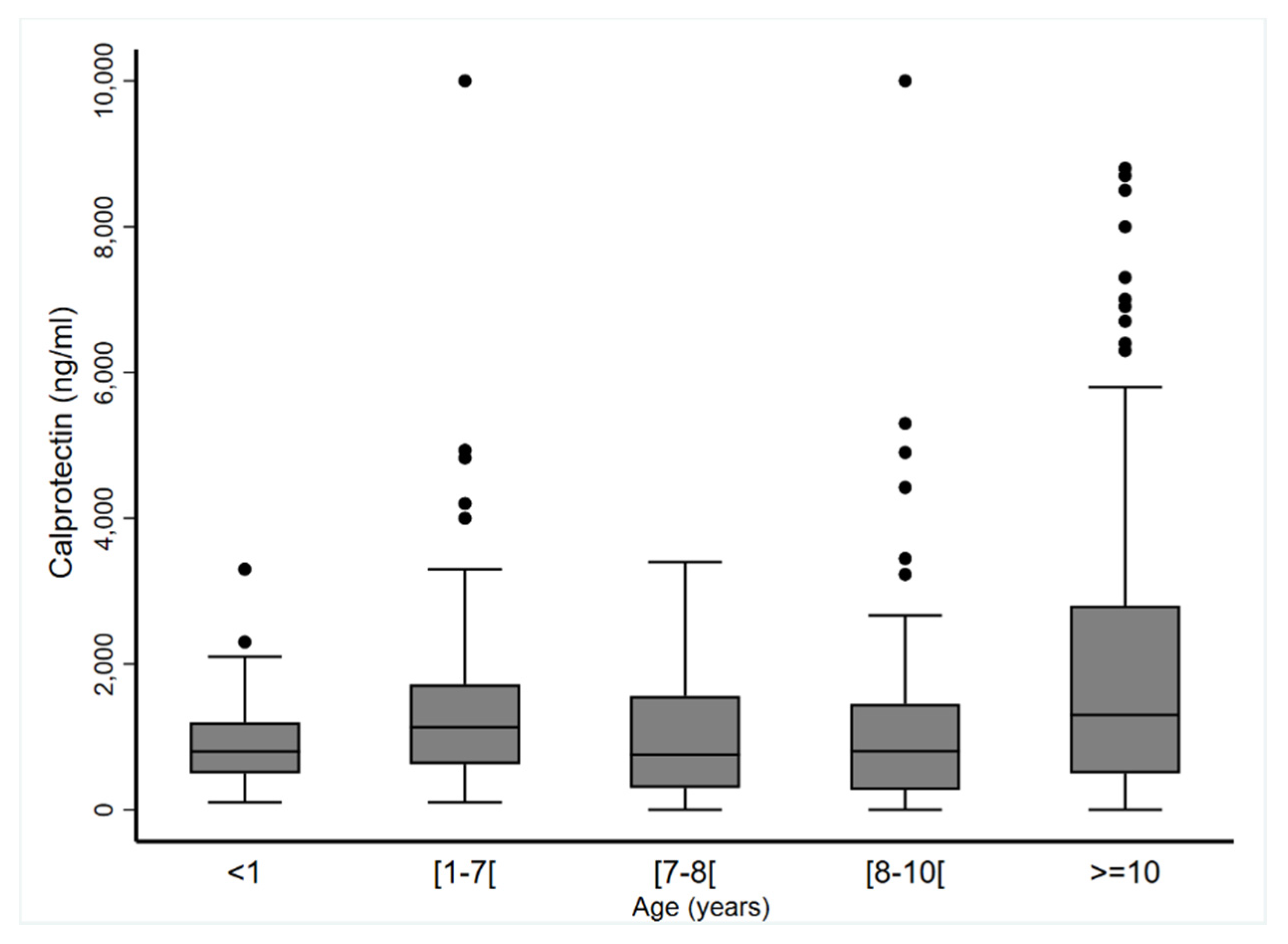
3.5. Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BMI | body mass index |
| CP | calprotectin |
| CRP | C-reactive protein |
| ICC | intraclass correlation coefficient |
| ELISA | enzyme linked immunosorbent assay |
| MRP8/14 | myeloid related protein 8/14 |
| NOS | Newcastle–Ottawa scale |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| SD | standard deviation |
| TLR-4 | toll-like receptor 4 |
References
- Stríz, I.; Trebichavský, I. Calprotectin-a pleiotropic molecule in acute and chronic inflammation. Physiol. Res. 2004, 53, 245–253. [Google Scholar] [PubMed]
- Ehrchen, J.M.; Sunderkötter, C.; Foell, D.; Vogl, T.; Roth, J. The endogenous Toll-like receptor 4 agonist S100A8/S100A9 (calprotectin) as innate amplifier of infection, autoimmunity, and cancer. J. Leukoc. Biol. 2009, 86, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Vaos, G.; Kostakis, I.D.; Zavras, N.; Chatzemichael, A. The role of calprotectin in pediatric disease. BioMed Res. Int. 2013, 2013, 542363. [Google Scholar] [CrossRef] [PubMed]
- Choi, I.Y.; Gerlag, D.M.; Herenius, M.J.; Thurlings, R.M.; Wijbrandts, C.A.; Foell, D.; Vogl, T.; Roth, J.; Tak, P.P.; Holzinger, D. MRP8/14 serum levels as a strong predictor of response to biological treatments in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2015, 74, 499–505. [Google Scholar] [CrossRef]
- Catalán, V.; Gómez-Ambrosi, J.; Rodríguez, A.; Ramírez, B.; Rotellar, F.; Valentí, V.; Silva, C.; Gil, M.J.; Fernández-Real, J.M.; Salvador, J.; et al. Increased levels of calprotectin in obesity are related to macrophage content: Impact on inflammation and effect of weight loss. Mol. Med. 2011, 17, 1157–1167. [Google Scholar] [CrossRef]
- Calcaterra, V.; De Amici, M.; Leonard, M.M.; De Silvestri, A.; Pelizzo, G.; Buttari, N.; Michev, A.; Leggio, M.; Larizza, D.; Cena, H. Serum Calprotectin Level in Children: Marker of Obesity and its Metabolic Complications. Ann. Nutr. Metab. 2018, 73, 177–183. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, 336–341. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality if Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohrica/programs/clinical_epidemiology/oxfordasp (accessed on 19 October 2009).
- Kim, J.; Bhattacharjee, R.; Snow, A.B.; Capdevila, O.S.; Kheirandish-Gozal, L.; Gozal, D. Myeloid-related protein 8/14 levels in children with obstructive sleep apnoea. Eur. Respir. J. 2010, 35, 843–850. [Google Scholar] [CrossRef]
- Kim, J.; Lee, S.; Bhattacharjee, R.; Khalyfa, A.; Kheirandish-Gozal, L.; Gozal, D. Leukocyte telomere length and plasma catestatin and myeloid-related protein 8/14 concentrations in children with obstructive sleep apnea. Chest 2010, 138, 91–99. [Google Scholar] [CrossRef]
- Terrin, G.; Passariello, A.; Manguso, F.; Salvia, G.; Rapacciuolo, L.; Messina, F.; Raimondi, F.; Canani, R.B. Serum calprotectin: An antimicrobial peptide as a new marker for the diagnosis of sepsis in very low birth weight newborns. Clin. Dev. Immunol. 2011, 2011, 291085. [Google Scholar] [CrossRef]
- Cobanoglu, N.; Dalkan, C.; Galip, N.; Tekguc, H.; Uncu, M.; Bahceciler, N.N. Is calprotectin a marker of tobacco smoke related inflammation: A pilot study in children. Inhal. Toxicol. 2012, 24, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Schellekens, D.H.S.M.; Hulsewé, K.W.E.; van Acker, B.A.C.; van Bijnen, A.A.; de Jaegere, T.M.H.; Sastrowijoto, S.H.; Buurman, W.A.; Derikx, J.P.M. Evaluation of the diagnostic accuracy of plasma markers for early diagnosis in patients suspected for acute appendicitis. Acad. Emerg. Med. 2013, 20, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Kane, H.; Lynch, L. Innate Immune Control of Adipose Tissue Homeostasis. Trends Immunol. 2019, 40, 857–872. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Nikolajczyk, B.S. Tissue Immune Cells Fuel Obesity-Associated Inflammation in Adipose Tissue and Beyond. Front. Immunol. 2019, 10, 1587. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Bey, A.; Segura-Jiménez, V.; Fernández-Santos, J.D.R.; Esteban-Cornejo, I.; Gómez-Martínez, S.; Veiga, O.L.; Marcos, A.; Ortega, F.B.; Castro-Piñero, J. The influence of cardiorespiratory fitness on clustered cardiovascular disease risk factors and the mediator role of body mass index in youth: The UP&DOWN Study. Pediatr. Diabetes 2019, 20, 32–40. [Google Scholar]
- Calcaterra, V.; Vinci, F.; Casari, G.; Pelizzo, G.; de Silvestri, A.; De Amici, M.; Albertini, R.; Regalbuto, C.; Montalbano, C.; Larizza, D.; et al. Evaluation of Allostatic Load as a Marker of Chronic Stress in Children and the Importance of Excess Weight. Front. Pediatr. 2019, 7, 335. [Google Scholar] [CrossRef] [PubMed]
- Harford, K.A.; Reynolds, C.M.; McGillicuddy, F.C.; Roche, H.M. Fats, inflammation and insulin resistance: Insights to the role of macrophage and T-cell accumulation in adipose tissue. Proc. Nutr. Soc. 2011, 70, 408–417. [Google Scholar] [CrossRef]
- Rhee, H.; Love, T.; Harrington, D. Blood Neutrophil Count is Associated with Body Mass Index in Adolescents with Asthma. JSM Allergy Asthma 2018, 3, 1019. [Google Scholar]
- Todendi, P.F.; Possuelo, L.G.; Klinger, E.I.; Reuter, C.P.; Burgos, M.S.; Moura, D.J.; Fiegenbaum, M.; de M. Valim, A.R. Low-grade inflammation markers in children and adolescents: Influence of anthropometric characteristics and CRP and IL6 polymorphisms. Cytokine 2016, 88, 177–183. [Google Scholar] [CrossRef]
- Shah, R.D.; Xue, C.; Zhang, H.; Tuteja, S.; Li, M.; Reilly, M.P.; Ferguson, J.F. Expression of Calgranulin Genes S100A8, S100A9 and S100A12 Is Modulated by n-3 PUFA during Inflammation in Adipose Tissue and Mononuclear Cells. PLoS ONE 2017, 12, e0169614. [Google Scholar] [CrossRef]
- Levitova, A.; Hulejova, H.; Spiritovic, M.; Pavelka, K.; Senolt, L.; Husakova, M. Clinical improvement and reduction in serum calprotectin levels after an intensive exercise programme for patients with ankylosing spondylitis and non-radiographic axial spondyloarthritis. Arthritis Res. Ther. 2016, 18, 275. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study/Year | Population and Condition | Age | Matrix | Test Kit | Sample Condition and Storage | Lower Detection Limit | Calprotectin Values |
|---|---|---|---|---|---|---|---|
| Kim et al. 2010 [9] | Mod./sev. OSA (n = 34); Mild OSA (n = 106); Controls (n = 115) | Mod./sev. OSA: 7.20 ± 1.96 yr.; Mild OSA: 7.65 ± 1.55 yr.; Controls: 7.81 ± 1.44 yr. | Plasma | ELISA (R&D Systems, Minneapolis, USA) | Fasting blood sample centrifuged and frozen at −80 °C | 0.4 µg·mL−1 | Mean ± SD in µg·mL−1 Mod./sev. OSA: 1.73 ± 0.92; Mild OSA: 1.27 ± 0.87; Controls: 1.02 ± 0.85 |
| Kim et al. 2010 [10] | Mod./sev. OSA (n = 26); Mild OSA (n = 85); Controls (n = 102) | Mod./sev. OSA: 7.19 ± 1.83 yr.; Mild OSA: 7.79 ± 1.57 yr.; Controls: 7.71 ± 1.29 yr. | Plasma | ELISA (ALPCO Diagnostics, Salem, USA) | Fasting blood sample centrifuged and frozen at −80 °C | 0.4 µg·mL−1 | Mean ± SD in µg·mL−1 Mod./sev. OSA: 1.82 ± 0.97; Mild OSA: 1.28 ± 0.91; Controls: 1.00 ± 0.84 |
| Terrin et al. 2011 [11] | Low body weight newborns: Septic group (n = 62); Non septic group (n = 29); Controls (n = 110) | Septic group: 8.7 d (95% CI: 7.2–10.1); Non septic group: 6.8 d (95% CI: 5.5–8.0); Controls: 6.9 d (95% CI: 6.1–7.7) | Serum | ELISA (Calprest, Eurospital, Trieste, Italy) | Collected in EDTA tube, centrifuged for 10 min at 10,000 rpm, stored at −20 °C | 1.6 ng·mL−1 | Mean (95% CI) in µg·mL−1 Septic: 3.1 (2.9–3.4); Non septic: 1.1 (0.9–1.2); Controls: 0.91 (0.8–1.0) |
| Cobanoglu et al. 2012 [12] | Group 1 (n = 51): not exposed Group 2 (n = 46): exposed to second-hand smoke at home | Group 1: 8.6 ± 1.6 yr.; Group 2: 8.4 ± 1.3 yr. | Serum | ELISA (Cusabio Biotech, China) | Coagulate for 30 min, centrifuged for 15 min at 10,000 rpm, frozen at −20 °C | 2 ng·mL−1 | Median (min–max) in ng·mL−1 Group 1: 0.00 (0.00–17.82); Group 2: 2.25 (0.00–106.87) |
| Schellekens et al. 2013 [13] | Acute abdominal complaints suspected for appendicitis (n = 233); Controls (n =52) | 33 yr. (min–max: 5–79) | Plasma | ELISA (Hbt, Uden, the Netherlands) | Collected in EDTA tube, centrifuged for 12 min at 2100 rpm, frozen at −20 °C | 10 ng·mL−1 | Median (IQR) in ng·mL−1 AA: 320.9 (193.4–492.4); Controls: 219.9 (104.3–323.0) |
| Calcaterra et al. 2018 [6] | Normal weight (n = 39); Overweight (n = 36); Obesity (n = 56) | NW: 12.3 ± 5.1 yr.; OW: 11.4 ± 4.0 yr.; Ob: 11.4 ± 3.0 yr. | Serum | ELISA (Calprest, Eurospital, Trieste, Italy) | ND | 0.3 µg·mL−1 | Median (IQR) in µg·mL−1 NW: 1.1 (0.9–2.1); OW: 1.85 (1.1–4.7); Ob: 2.65 (1.6–4.2) |
| Study | Year | Country | Sample Type | Number of Participants | Girls/Boys | CP Values in Blood (ng·mL−1) | Age (Years) | BMI z-Score |
|---|---|---|---|---|---|---|---|---|
| Kim J et al. ‡ [9,10] | 2010 | United States | Plasma | 252 | 106/146 | 1194.7 ± 856.3 | 7.6 ± 1.5 | 2.82 ± 2.59 |
| Terrin G et al. [11] | 2011 | Italy | Serum | 139 | 58/81 | 952.5 ± 543.5 | 0.018 ± 0.010 | NK |
| Cobanoglu et al. [12] | 2012 | Cyprus | Serum | 51 | 25/26 | 1.72 ± 3.39 | 8.4 ± 1.3 | 1.82 ± 1.56 |
| Schellekens D et al. [13] | 2013 | Netherlands | Plasma | 4 | 0/4 | 193.6 ± 97.4 | 15.0 ± 2.6 | NK |
| Calcaterra et al. [6] | 2018 | Italy | Serum | 122 | 65/57 | 2680.3 ± 2169.8 | 11.1 ± 3.2 | 2.36 ± 1.69 |
| Merlin et al. ‡‡ | 2018 | France | Plasma | 26 | 16/10 | 419.9 ± 264.5 | 10.7 ± 3.3 | 0.09 ± 1.47 |
| Authors | n | Mean | SD | Q1 | MED | Q3 | P5 | P95 | MIN | MAX | CV |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Kim et al. [9,10] | 252 | 1194.73 | 856.63 | 550.00 | 963.50 | 1566.50 | 250.00 | 2789.00 | 100.00 | 4930.00 | 0.72 |
| Terrin et al. [11] | 139 | 952.52 | 543.52 | 500.00 | 800.00 | 1200.00 | 200.00 | 2000.00 | 100.00 | 3300.00 | 0.57 |
| Cobanoglu et al. [12] | 51 | 1.73 | 3.40 | 0.00 | 0.00 | 1.90 | 0.00 | 6.80 | 0.00 | 17.80 | 1.97 |
| Schellekens et al. [13] | 3 | 193.63 | 97.41 | 113.10 | 165.90 | 301.90 | 113.10 | 301.90 | 113.10 | 301.90 | 0.50 |
| Calcaterra et al. [6] | 122 | 2680.33 | 2169.88 | 1100.00 | 1950.00 | 3400.00 | 600.00 | 7300.00 | 400.00 | 10,000.00 | 0.81 |
| Merlin et al. | 26 | 419.91 | 264.47 | 303.30 | 336.80 | 460.70 | 177.30 | 883.90 | 140.80 | 1415.60 | 0.63 |
| Meta-Analysis | 593 | 880.75 | 255.36 | 482 | 900 | 1700 |
| Univariate Analysis 1 Correlation Coefficient | Multivariable Analysis 2 Coefficient Correlation | |
|---|---|---|
| Boys | 0.39 | 0.118 (0.076; 0.159), p < 0.001 |
| Girls | 0.48 | 0.116 (0.072; 0.160), p < 0.001 |
| Year(s) | <1 | (≥1–<7) | (≥7–<8) | (≥8–<10) | ≥10 | p |
|---|---|---|---|---|---|---|
| Boys | ||||||
| n | 81 | 68 | 48 | 64 | 62 | 0.25 |
| Mean ± SD | 849.4 ± 455.3 | 1356.7 ± 949.8 | 802.9 ± 850.5 | 977.2 ± 937.3 | 1752.8 ± 1666.1 | |
| Median (min–max) | 800 (100–2300) | 1165 (100–4824) | 498.8 (0–2789) | 812 (0–4420) | 1150 (0–7300) | |
| Girls | ||||||
| n | 58 | 48 | 43 | 52 | 69 | 0.97 |
| Mean ± SD | 1096.5 ± 622.9 | 1395.3 ± 1556.0 | 1169.1 ± 936.5 | 1216.7 ± 1658.5 | 2277.1 ± 2400.3 | |
| Median (min–max) | 1100 (100–3300) | 1060 (189–10,000) | 978 (0–3400) | 803.5 (0–10,000) | 1400 (0–8800) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grand, A.; Rochette, E.; Dutheil, F.; Gozal, D.; Calcaterra, V.; Berni Canani, R.; Cobanoglu, N.; Derikx, J.P.M.; Terrin, G.; Pereira, B.; et al. Body Mass Index and Calprotectin Blood Level Correlation in Healthy Children: An Individual Patient Data Meta-Analysis. J. Clin. Med. 2020, 9, 857. https://doi.org/10.3390/jcm9030857
Grand A, Rochette E, Dutheil F, Gozal D, Calcaterra V, Berni Canani R, Cobanoglu N, Derikx JPM, Terrin G, Pereira B, et al. Body Mass Index and Calprotectin Blood Level Correlation in Healthy Children: An Individual Patient Data Meta-Analysis. Journal of Clinical Medicine. 2020; 9(3):857. https://doi.org/10.3390/jcm9030857
Chicago/Turabian StyleGrand, Anais, Emmanuelle Rochette, Frederic Dutheil, David Gozal, Valeria Calcaterra, Roberto Berni Canani, Nazan Cobanoglu, Joep P. M. Derikx, Gianluca Terrin, Bruno Pereira, and et al. 2020. "Body Mass Index and Calprotectin Blood Level Correlation in Healthy Children: An Individual Patient Data Meta-Analysis" Journal of Clinical Medicine 9, no. 3: 857. https://doi.org/10.3390/jcm9030857
APA StyleGrand, A., Rochette, E., Dutheil, F., Gozal, D., Calcaterra, V., Berni Canani, R., Cobanoglu, N., Derikx, J. P. M., Terrin, G., Pereira, B., & Merlin, E. (2020). Body Mass Index and Calprotectin Blood Level Correlation in Healthy Children: An Individual Patient Data Meta-Analysis. Journal of Clinical Medicine, 9(3), 857. https://doi.org/10.3390/jcm9030857