Biphasic Temporal Relationship between Cancers and Systemic Sclerosis: A Clinical Series from Montpellier University Hospital and Review of the Literature

 ,
, 
Abstract
1. Introduction
2. Material and Methods
3. Results
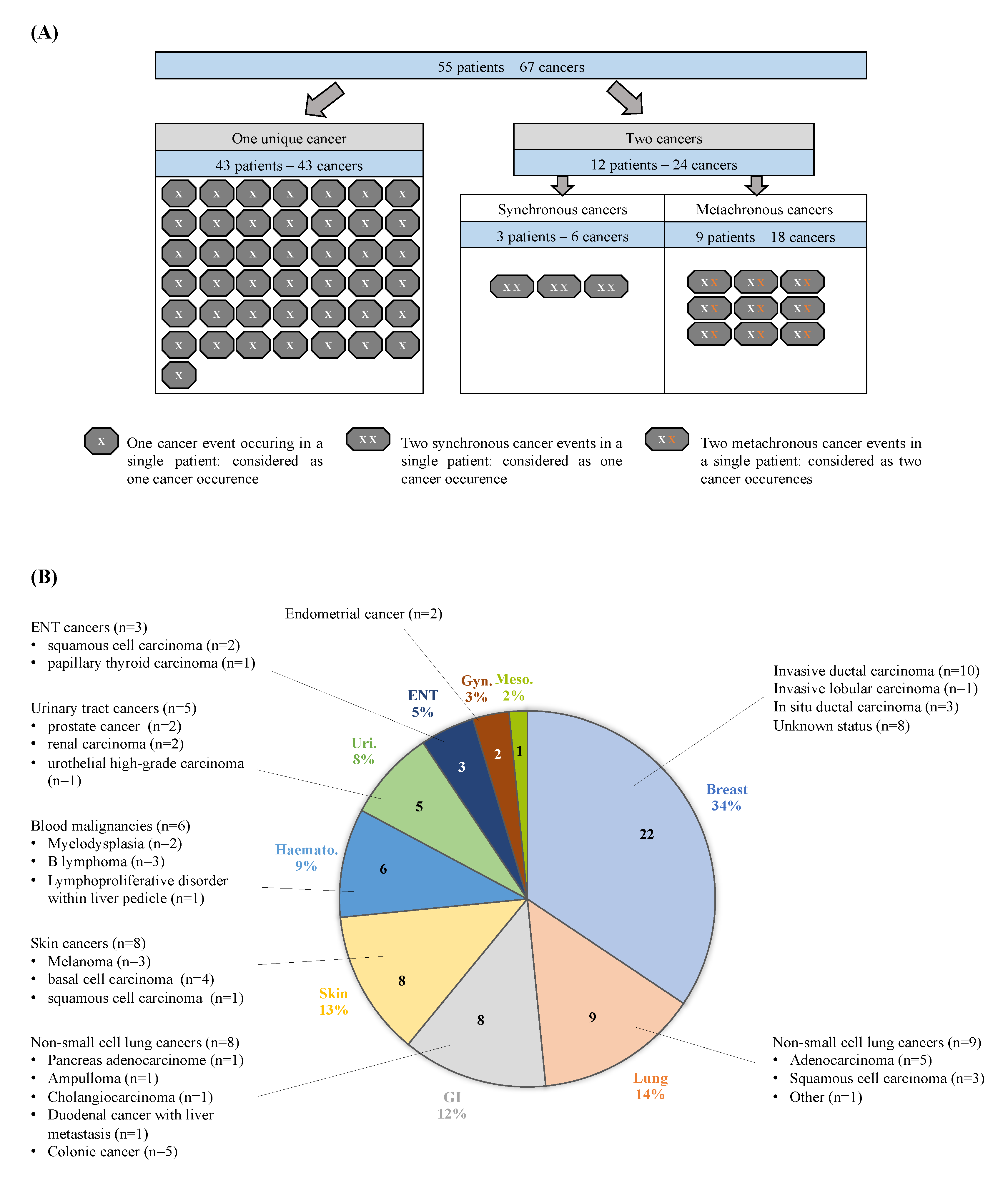
3.1. General Characteristics of Systemic Sclerosis (SSc) Patients with Cancer
3.2. Characteristics of Cancer
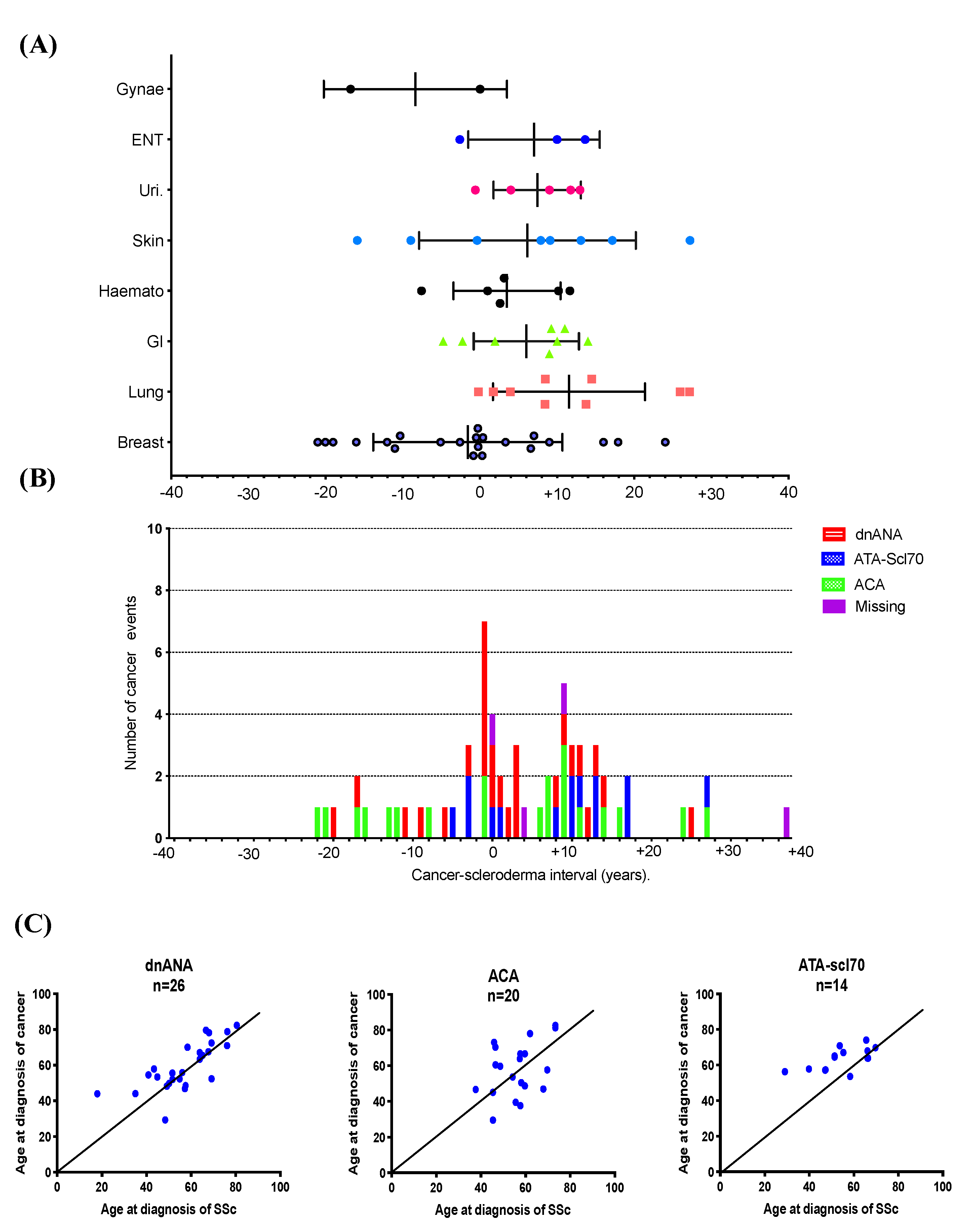
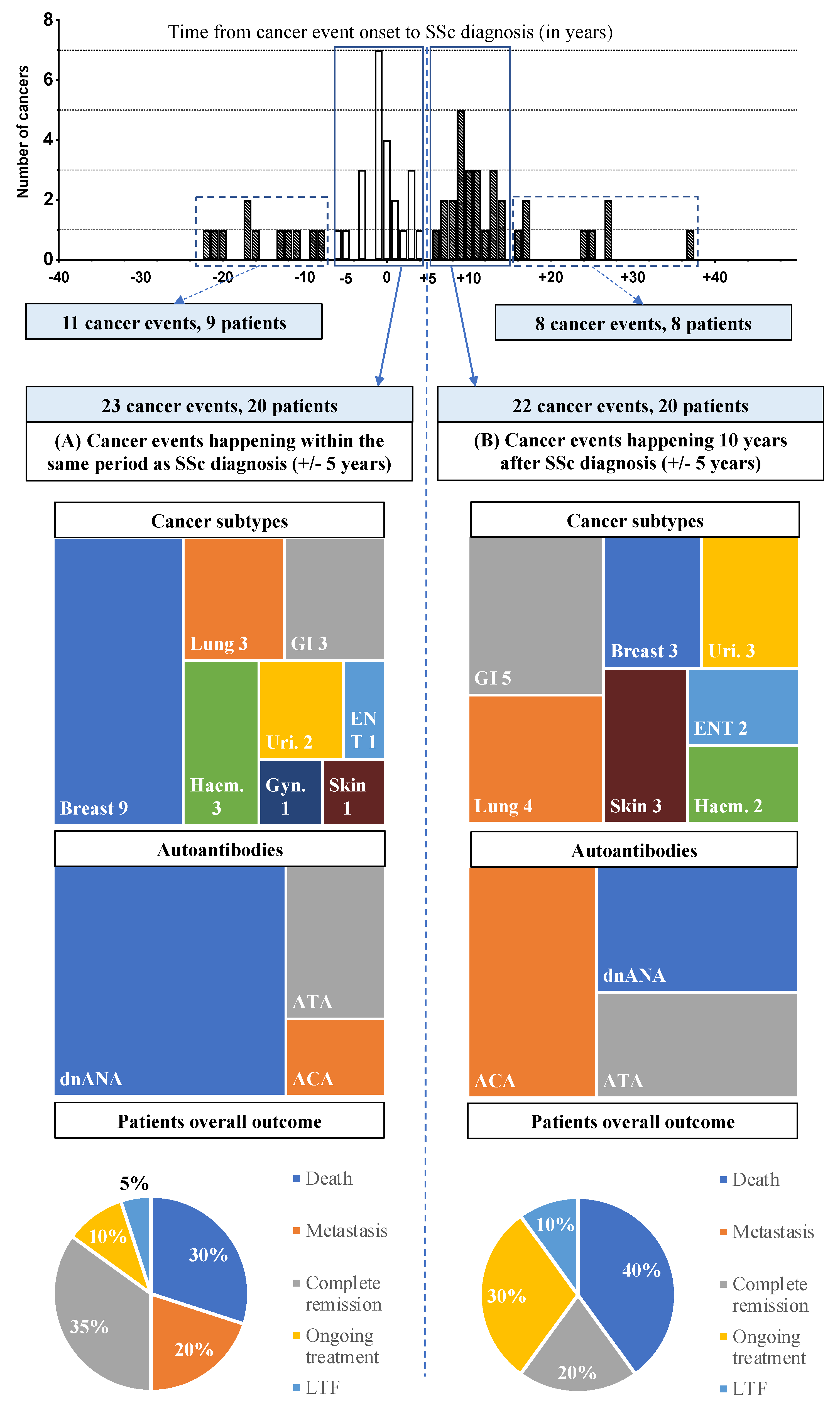
3.3. Temporal Relationship between SSc and Cancer Diagnoses: Two Peaks of Occurrence
3.3.1. First Peak: Close Temporal Relationship between SSc and Cancer Diagnosis (±5 years)
3.3.2. Second Peak: Delayed Temporal Relationship between SSc and Cancer Diagnosis (10 Years ± 5 Years)
3.3.3. Cancer Diagnoses Widely Spaced Apart from SSc Diagnosis
4. Discussion
4.1. Comparison of Cancer Distribution with Epidemiological Data from Literature
4.2. First Peak: the Close Temporal Relationship between SSc and Cancer
4.3. Second Peak: Late-Onset Cancers May Result from Multiple Intertwined Factors
4.4. Cancer-Screening Strategy: Current Recommendations and Additional Suggestions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Maria, A.T.J.; Partouche, L.; Goulabchand, R.; Rivière, S.; Rozier, P.; Bourgier, C.; Le Quellec, A.; Morel, J.; Noël, D.; Guilpain, P. Intriguing Relationships Between Cancer and Systemic Sclerosis: Role of the Immune System and Other Contributors. Front. Immunol. 2018, 9, 3112. [Google Scholar] [CrossRef] [PubMed]
- Bonifazi, M.; Tramacere, I.; Pomponio, G.; Gabrielli, B.; Avvedimento, E.V.; La Vecchia, C.; Negri, E.; Gabrielli, A. Systemic sclerosis (scleroderma) and cancer risk: Systematic review and meta-analysis of observational studies. Rheumatology (Oxf.) 2013, 52, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Moinzadeh, P.; Fonseca, C.; Hellmich, M.; Shah, A.A.; Chighizola, C.; Denton, C.P.; Ong, V.H. Association of anti-RNA polymerase III autoantibodies and cancer in scleroderma. Arthritis Res. Ther. 2014, 16, R53. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.A.; Xu, G.; Rosen, A.; Hummers, L.K.; Wigley, F.M.; Elledge, S.J.; Casciola-Rosen, L. Brief Report: Anti-RNPC-3 Antibodies As a Marker of Cancer-Associated Scleroderma. Arthritis Rheumatol. (Hoboken N.J.) 2017, 69, 1306–1312. [Google Scholar] [CrossRef] [PubMed]
- Igusa, T.; Hummers, L.K.; Visvanathan, K.; Richardson, C.; Wigley, F.M.; Casciola-Rosen, L.; Rosen, A.; Shah, A.A. Autoantibodies and scleroderma phenotype define subgroups at high-risk and low-risk for cancer. Ann. Rheum. Dis. 2018, 77, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. 2013, 65, 2737–2747. [Google Scholar] [CrossRef]
- LeRoy, E.C.; Medsger, T.A. Criteria for the classification of early systemic sclerosis. J. Rheumatol. 2001, 28, 1573–1576. [Google Scholar]
- Shah, A.A.; Hummers, L.K.; Casciola-Rosen, L.; Visvanathan, K.; Rosen, A.; Wigley, F.M. Examination of autoantibody status and clinical features associated with cancer risk and cancer-associated scleroderma. Arthritis Rheumatol. (Hoboken N.J.) 2015, 67, 1053–1061. [Google Scholar] [CrossRef]
- Morrisroe, K.; Hansen, D.; Huq, M.; Stevens, W.; Sahhar, J.; Ngian, G.-S.; Ferdowsi, N.; Hill, C.; Roddy, J.; Walker, J.; et al. Incidence, risk factors and outcomes of cancer in systemic sclerosis. Arthritis Care Res. (Hoboken) 2019. [Google Scholar] [CrossRef]
- Catano, J.; Guedon, A.; Riviere, S.; Carrat, F.; Mahevas, T.; Fain, O.; Mekinian, A. Survenue de cancers au cours de la sclérodermie systémique: Facteurs de risque, impact sur la survie et revue de la littérature. La Revue de Médecine Interne 2019, 40, 637–644. [Google Scholar] [CrossRef]
- Colaci, M.; Giuggioli, D.; Vacchi, C.; Lumetti, F.; Iachetta, F.; Marcheselli, L.; Federico, M.; Ferri, C. Breast cancer in systemic sclerosis: Results of a cross-linkage of an Italian Rheumatologic Center and a population-based Cancer Registry and review of the literature. Autoimmun. Rev. 2014, 13, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Olesen, A.B.; Svaerke, C.; Farkas, D.K.; Sørensen, H.T. Systemic sclerosis and the risk of cancer: A nationwide population-based cohort study. Br. J. Dermatol. 2010, 163, 800–806. [Google Scholar] [CrossRef] [PubMed]
- Onishi, A.; Sugiyama, D.; Kumagai, S.; Morinobu, A. Cancer incidence in systemic sclerosis: Meta-analysis of population-based cohort studies. Arthritis Rheum. 2013, 65, 1913–1921. [Google Scholar] [CrossRef] [PubMed]
- Siau, K.; Laversuch, C.J.; Creamer, P.; O’Rourke, K.P. Malignancy in scleroderma patients from south west England: A population-based cohort study. Rheumatol. Int. 2011, 31, 641–645. [Google Scholar] [CrossRef]
- Hashimoto, A.; Arinuma, Y.; Nagai, T.; Tanaka, S.; Matsui, T.; Tohma, S.; Endo, H.; Hirohata, S. Incidence and the risk factor of malignancy in Japanese patients with systemic sclerosis. Intern. Med. 2012, 51, 1683–1688. [Google Scholar] [CrossRef]
- Hill, C.L.; Nguyen, A.-M.; Roder, D.; Roberts-Thomson, P. Risk of cancer in patients with scleroderma: A population based cohort study. Ann. Rheum. Dis. 2003, 62, 728–731. [Google Scholar] [CrossRef]
- Kang, K.Y.; Yim, H.W.; Kim, I.-J.; Yoon, J.U.; Ju, J.H.; Kim, H.-Y.; Park, S.-H. Incidence of cancer among patients with systemic sclerosis in Korea: Results from a single centre. Scand. J. Rheumatol. 2009, 38, 299–303. [Google Scholar] [CrossRef]
- Kuo, C.-F.; Luo, S.-F.; Yu, K.-H.; Chou, I.-J.; Tseng, W.-Y.; Chang, H.-C.; Fang, Y.-F.; Chiou, M.-J.; See, L.-C. Cancer risk among patients with systemic sclerosis: A nationwide population study in Taiwan. Scand. J. Rheumatol. 2012, 41, 44–49. [Google Scholar] [CrossRef]
- Sargin, G.; Senturk, T.; Cildag, S. Systemic sclerosis and malignancy. Int. J. Rheum. Dis 2018, 21, 1093–1099. [Google Scholar] [CrossRef]
- Derk, C.T.; Rasheed, M.; Artlett, C.M.; Jimenez, S.A. A cohort study of cancer incidence in systemic sclerosis. J. Rheumatol. 2006, 33, 1113–1116. [Google Scholar]
- Bernal-Bello, D.; de Tena, J.G.; Guillén-Del Castillo, A.; Selva-O’Callaghan, A.; Callejas-Moraga, E.L.; Marín-Sánchez, A.M.; Fonollosa-Pla, V.; Simeón-Aznar, C.P. Novel risk factors related to cancer in scleroderma. Autoimmun. Rev. 2017, 16, 461–468. [Google Scholar] [CrossRef]
- Launay, D.; Le Berre, R.; Hatron, P.-Y.; Peyrat, J.-P.; Hachulla, E.; Devulder, B.; Hebbar, M. Association between systemic sclerosis and breast cancer: Eight new cases and review of the literature. Clin. Rheumatol. 2004, 23, 516–522. [Google Scholar] [CrossRef]
- Liu, C.; Hou, Y.; Xu, D.; Li, L.; Zhang, Y.; Cheng, L.; Yan, S.; Zhang, F.; Li, Y. Analysis of anti-RNA polymerase III antibodies in Chinese Han systemic sclerosis patients. Clin. Rheumatol. 2019, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Nikpour, M.; Hissaria, P.; Byron, J.; Sahhar, J.; Micallef, M.; Paspaliaris, W.; Roddy, J.; Nash, P.; Sturgess, A.; Proudman, S.; et al. Prevalence, correlates and clinical usefulness of antibodies to RNA polymerase III in systemic sclerosis: A cross-sectional analysis of data from an Australian cohort. Arthritis Res. Ther. 2011, 13, R211. [Google Scholar] [CrossRef] [PubMed]
- Lazzaroni, M.-G.; Cavazzana, I.; Colombo, E.; Dobrota, R.; Hernandez, J.; Hesselstrand, R.; Varju, C.; Nagy, G.; Smith, V.; Caramaschi, P.; et al. Malignancies in Patients with Anti-RNA Polymerase III Antibodies and Systemic Sclerosis: Analysis of the EULAR Scleroderma Trials and Research Cohort and Possible Recommendations for Screening. J. Rheumatol. 2017, 44, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Patterson, K.A.; Roberts-Thomson, P.J.; Lester, S.; Tan, J.A.; Hakendorf, P.; Rischmueller, M.; Zochling, J.; Sahhar, J.; Nash, P.; Roddy, J.; et al. Interpretation of an Extended Autoantibody Profile in a Well-Characterized Australian Systemic Sclerosis (Scleroderma) Cohort Using Principal Components Analysis. Arthritis Rheumatol. 2015, 67, 3234–3244. [Google Scholar] [CrossRef]
- Xu, G.J.; Shah, A.A.; Li, M.Z.; Xu, Q.; Rosen, A.; Casciola-Rosen, L.; Elledge, S.J. Systematic autoantigen analysis identifies a distinct subtype of scleroderma with coincident cancer. Proc. Natl. Acad. Sci. USA 2016, 113, E7526–E7534. [Google Scholar] [CrossRef]
- Shah, A.A.; Rosen, A.; Hummers, L.; Wigley, F.; Casciola-Rosen, L. Close temporal relationship between onset of cancer and scleroderma in patients with RNA polymerase I/III antibodies. Arthritis Rheum. 2010, 62, 2787–2795. [Google Scholar] [CrossRef]
- Joseph, C.G.; Darrah, E.; Shah, A.A.; Skora, A.D.; Casciola-Rosen, L.A.; Wigley, F.M.; Boin, F.; Fava, A.; Thoburn, C.; Kinde, I.; et al. Association of the autoimmune disease scleroderma with an immunologic response to cancer. Science 2014, 343, 152–157. [Google Scholar] [CrossRef]
- Shah, A.A.; Rosen, A. Cancer and systemic sclerosis: Novel insights into pathogenesis and clinical implications. Curr. Opin. Rheumatol. 2011, 23, 530–535. [Google Scholar] [CrossRef]
- Shah, A.A.; Laiho, M.; Rosen, A.; Casciola-Rosen, L. Protective Effect against Cancer of Antibodies to the Large Subunits of Both RNA Polymerases I and III in Scleroderma. Arthritis Rheumatol. (Hoboken N.J.) 2019, 71, 1571–1579. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; McGonagle, D.; Bragazzi, N.L.; Tiosano, S.; Comaneshter, D.; Shoenfeld, Y.; Cohen, A.D.; Amital, H. Autoantibody status in systemic sclerosis patients defines both cancer risk and survival with ANA negativity in cases with concomitant cancer having a worse survival. Oncoimmunology 2019, 8, e1588084. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, R.D.; Old, L.J.; Smyth, M.J. Cancer immunoediting: Integrating immunity’s roles in cancer suppression and promotion. Science 2011, 331, 1565–1570. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.A.; Casciola-Rosen, L. Cancer and scleroderma: A paraneoplastic disease with implications for malignancy screening. Curr. Opin. Rheumatol. 2015, 27, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Howard, M.D.; Su, J.C.; Chong, A.H. Skin Cancer Following Solid Organ Transplantation: A Review of Risk Factors and Models of Care. Am. J. Clin. Dermatol. 2018, 19, 585–597. [Google Scholar] [CrossRef]
- Wright, C.M.; Moorin, R.E.; Chowdhury, E.K.; Stricker, B.H.; Reid, C.M.; Saunders, C.M.; Hughes, J.D. Calcium channel blockers and breast cancer incidence: An updated systematic review and meta-analysis of the evidence. Cancer Epidemiol. 2017, 50, 113–124. [Google Scholar] [CrossRef]
- Hussain, S.P.; He, P.; Subleski, J.; Hofseth, L.J.; Trivers, G.E.; Mechanic, L.; Hofseth, A.B.; Bernard, M.; Schwank, J.; Nguyen, G.; et al. Nitric Oxide Is a Key Component in Inflammation-Accelerated Tumorigenesis. Cancer Res. 2008, 68, 7130–7136. [Google Scholar] [CrossRef]
- Pesic, M.; Greten, F.R. Inflammation and cancer: Tissue regeneration gone awry. Curr. Opin. Cell Biol. 2016, 43, 55–61. [Google Scholar] [CrossRef]
- Zeineddine, N.; Khoury, L.E.; Mosak, J. Systemic Sclerosis and Malignancy: A Review of Current Data. J. Clin. Med. Res. 2016, 8, 625–632. [Google Scholar] [CrossRef]
- Boozalis, E.; Shah, A.A.; Wigley, F.; Kang, S.; Kwatra, S.G. Morphea and systemic sclerosis are associated with an increased risk for melanoma and nonmelanoma skin cancer. J. Am. Acad. Dermatol. 2019, 80, 1449–1451. [Google Scholar] [CrossRef]
- Sosa, V.; Moliné, T.; Somoza, R.; Paciucci, R.; Kondoh, H.; LLeonart, M.E. Oxidative stress and cancer: An overview. Ageing Res. Rev. 2013, 12, 376–390. [Google Scholar] [CrossRef] [PubMed]
- Didier, K.; Robbins, A.; Antonicelli, F.; Pham, B.N.; Giusti, D.; Servettaz, A. Actualités dans la physiopathologie de la sclérodermie systémique: Vers de nouvelles opportunités thérapeutiques. La Revue de Médecine Interne 2019, 40, 654–663, S0248866319305259. [Google Scholar] [CrossRef] [PubMed]
- Bottrell, A.; Meng, Y.H.; Najy, A.J.; Hurst, N.; Kim, S.; Kim, C.J.; Kim, E.-S.; Moon, A.; Kim, E.J.; Park, S.Y.; et al. An oncogenic activity of PDGF-C and its splice variant in human breast cancer. Growth Factors 2019, 37, 131–145. [Google Scholar] [CrossRef] [PubMed]
- Üçüncü, M.; Serilmez, M.; Sarı, M.; Bademler, S.; Karabulut, S. The Diagnostic Significance of PDGF, EphA7, CCR5, and CCL5 Levels in Colorectal Cancer. Biomolecules 2019, 9, 464. [Google Scholar] [CrossRef] [PubMed]
- Kishi, M.; Aono, Y.; Sato, S.; Koyama, K.; Azuma, M.; Abe, S.; Kawano, H.; Kishi, J.; Toyoda, Y.; Okazaki, H.; et al. Blockade of platelet-derived growth factor receptor-β, not receptor-α ameliorates bleomycin-induced pulmonary fibrosis in mice. PLoS ONE 2018, 13, e0209786. [Google Scholar] [CrossRef]
- Donin, N.; Filson, C.; Drakaki, A.; Tan, H.-J.; Castillo, A.; Kwan, L.; Litwin, M.; Chamie, K. Risk of second primary malignancies among cancer survivors in the United States, 1992 through 2008. Cancer 2016, 122, 3075–3086. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| SSc Patients with Cancer, n | 55 | |
| Median Age at SSc onset (IQR), years | 56 | (47–66) |
| Median Follow-up Time (IQR), years | 11 | (4–15) |
| Sex | ||
| Female, n (%) | 42 | 76.4 |
| Male, n (%) | 13 | 23.6 |
| Tobacco Use, n (%) | 19 | 34.5 |
| SSc Subtypes | ||
| lcSSc, n (%) | 32 | 58.2 |
| dcSSc, n (%) | 20 | 36.4 |
| Sine Scleroderma, n (%) | 3 | 5.5 |
| Organ Involvement | ||
| Lung Fibrosis, n (%) | 18 | 32.7 |
| PAH, n (%) | 8 | 14.5 |
| SRC, n (%) | 2 | 3.6 |
| SSc-Cardiomyopathy, n (%) | 3 | 5.5 |
| GERD, n (%) | 44 | 80.0 |
| Digital Ulcer, n (%) | 21 | 38.2 |
| SSc Autoantibody Status | ||
| ANA, n (%) | 52 | 94.5 |
| ACA, n (%) | 16 | 29.1 |
| ATA, n (%) | 12 | 21.8 |
| Double-Negative SSc Patients, n (%) | 24 | 43.6 |
| Use of Immunosuppressive Drugs Prior to Cancer | ||
| Corticosteroid | 19 | 34.5 |
| Hydroxychloroquine | 5 | 9.1 |
| Methotrexate | 12 | 21.8 |
| Leflunomide | 1 | 1.8 |
| Mycophenolate Mofetil | 2 | 3.6 |
| Azathioprine | 7 | 12.7 |
| Cyclophosphamide | 7 | 12.7 |
| Biotherapy | 1 | 1.8 |
| Evolution | ||
| Lost to Follow-up, n (%) | 7 | 12.7 |
| Death, n (%) | 19 | 34.5 |
| SSc-Related Death Cases | 2 | 3.6 |
| Malignancy-Related Death Cases | 16 | 29.1 |
| Other Cause of Death | 1 | 1.8 |
| Characteristics | Cancer Subtypes | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Breast (n = 22) | Lung (n = 9) | GI (n = 8) | Skin (n = 8) | Haemato. (n = 6) | Urinary (n = 5) | ENT (n = 3) | Gyn. (n = 2) | Meso. (n = 1) | |||||||
| Sex | |||||||||||||||
| Female, % | 22 | 100.0 | 2 | 22.2 | 6 | 75.0 | 7 | 87.5 | 4 | 66.7 | 2 | 40.0 | 2 | 2 | 1 |
| Male, % | 0 | 0 | 7 | 77.8 | 2 | 25.0 | 1 | 12.5 | 2 | 33.3 | 3 | 60.0 | 1 | 0 | 0 |
| Median Age at Cancer Diagnosis (years, IQR) | 55 | IQR: 47–65 | 56 | IQR: 56–65 | 60 | IQR: 56–72 | 65 | IQR: 49–74 | 68 | IQR: 64–76 | 66 | IQR: 54–67 | 55 | 71 | 76 |
| Median Age at SSc onset (years, IQR) | 59 | IQR: 50–66 | 51 | IQR: 43–56 | 58 | IQR: 48–68 | 53 | IQR: 49–61 | 63 | IQR: 59–67 | 55 | IQR: 54–62 | 47 | 69 | 39 |
| Tobacco Use, % | 5 | 27.8 | 6 | 75.0 | 3 | 50.0 | 2 | 25.0 | 1 | 20.0 | 4 | 80.0 | 2 | 0 | NA |
| SSc Subsets | |||||||||||||||
| lcSSc, % | 14 | 63.6 | 3 | 33.3 | 5 | 62.5 | 4 | 50.0 | 6 | 100.0 | 4 | 80.0 | 2 | 0 | 0 |
| dcSSc, % | 6 | 27.3 | 6 | 66.7 | 3 | 37.5 | 4 | 50.0 | 0 | 0.0 | 1 | 20.0 | 1 | 1 | 1 |
| Sine Scleroderma, % | 2 | 9.1 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 1 | 0 |
| SSc Autoantibody Status | |||||||||||||||
| ANA, % | 22 | 100.0 | 9 | 100.0 | 8 | 100.0 | 7 | 87.5 | 5 | 83.3 | 4 | 80.0 | 3 | 2 | NA |
| ACA, % | 10 | 45.5 | 0 | 0.0 | 4 | 50.0 | 3 | 37.5 | 1 | 16.7 | 2 | 40.0 | 0 | 0 | NA |
| ATA, % | 2 | 9.1 | 4 | 44.4 | 3 | 37.5 | 2 | 25.0 | 0 | 0.0 | 1 | 20.0 | 1 | 1 | NA |
| dnANA, % | 10 | 45.5 | 5 | 55.6 | 1 | 12.5 | 2 | 25.0 | 4 | 66.7 | 1 | 20.0 | 2 | 1 | NA |
| Metastatic Stage at Cancer Diagnosis (n, %) | 0 | 0 | 2 | 22 | 3 | 43 | 0 | 0 | NC | 0 | 0 | 1 | 0 | 0 | |
| IS Treatment Prior to Cancer | 1/6 | 3/8 | 3/6 | 2/5 | 3/5 | 2/4 | 1/2 | ||||||||
| Overall Outcome | |||||||||||||||
| Death, % | 5 | 22.7 | 5 | 55.6 | 7 | 87.5 | 3 | 37.5 | 2 | 33.3 | |||||
| Metastasis, % | 2 | 9.1 | |||||||||||||
| Complete Remission, % | 11 | 50.0 | 1 | 11.1 | 1 | 12.5 | 5 | 62.5 | 1 | 16.7 | 3 | 60.0 | 2 | 2 | |
| Ongoing Treatment, % | 3 | 13.6 | 2 | 33.3 | 2 | 40.0 | |||||||||
| Lost to Follow-up, % | 1 | 4.5 | 3 | 33.3 | 1 | 16.7 | 1 | 1 | |||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Partouche, L.; Goulabchand, R.; Maria, A.T.J.; Rivière, S.; Jorgensen, C.; Rigau, V.; Bourgier, C.; Bessis, D.; Le Quellec, A.; Quere, I.; et al. Biphasic Temporal Relationship between Cancers and Systemic Sclerosis: A Clinical Series from Montpellier University Hospital and Review of the Literature. J. Clin. Med. 2020, 9, 853. https://doi.org/10.3390/jcm9030853
Partouche L, Goulabchand R, Maria ATJ, Rivière S, Jorgensen C, Rigau V, Bourgier C, Bessis D, Le Quellec A, Quere I, et al. Biphasic Temporal Relationship between Cancers and Systemic Sclerosis: A Clinical Series from Montpellier University Hospital and Review of the Literature. Journal of Clinical Medicine. 2020; 9(3):853. https://doi.org/10.3390/jcm9030853
Chicago/Turabian StylePartouche, Léo, Radjiv Goulabchand, Alexandre Thibault Jacques Maria, Sophie Rivière, Christian Jorgensen, Valérie Rigau, Céline Bourgier, Didier Bessis, Alain Le Quellec, Isabelle Quere, and et al. 2020. "Biphasic Temporal Relationship between Cancers and Systemic Sclerosis: A Clinical Series from Montpellier University Hospital and Review of the Literature" Journal of Clinical Medicine 9, no. 3: 853. https://doi.org/10.3390/jcm9030853
APA StylePartouche, L., Goulabchand, R., Maria, A. T. J., Rivière, S., Jorgensen, C., Rigau, V., Bourgier, C., Bessis, D., Le Quellec, A., Quere, I., Morel, J., & Guilpain, P. (2020). Biphasic Temporal Relationship between Cancers and Systemic Sclerosis: A Clinical Series from Montpellier University Hospital and Review of the Literature. Journal of Clinical Medicine, 9(3), 853. https://doi.org/10.3390/jcm9030853