A Population-Based Study of Diabetes during Pregnancy in Spain (2009–2015): Trends in Incidence, Obstetric Interventions, and Pregnancy Outcomes

 ,
, 
 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design, Setting, and Participants
2.2. Main Outcomes Measures
2.3. Statistical Methods
2.4. Ethical Aspects
3. Results
3.1. Incidence of Deliveries, Obstetric Interventions and Obstetric Outcomes among Women with Existing and Gestational Diabetes
3.1.1. Time Trends in the Incidence and Demographic Characteristics of Deliveries in Women with Existing and Gestational Diabetes
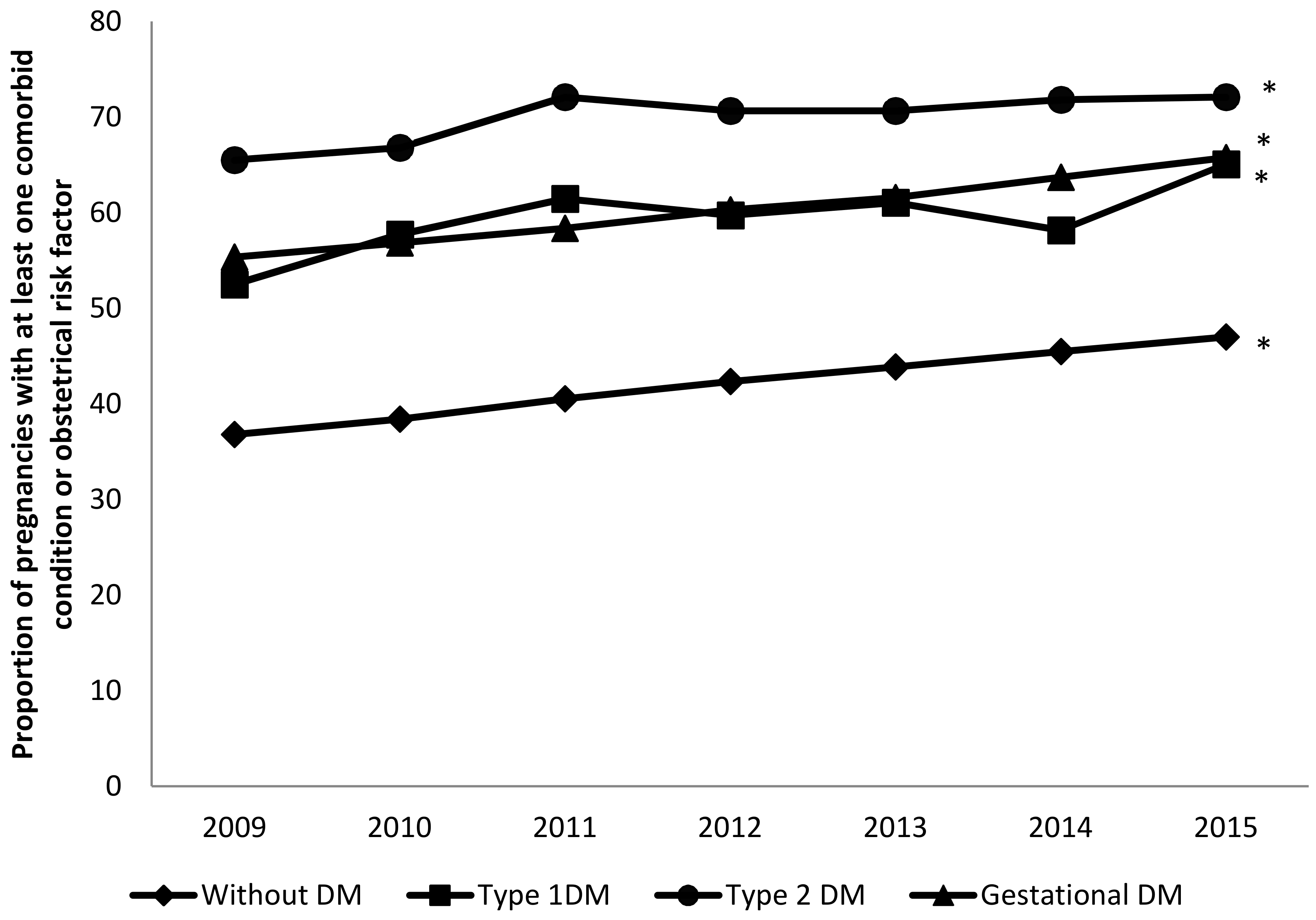
3.1.2. Comorbidities and Obstetrical Risk Factors of Deliveries in Women with Existing and Gestational Diabetes
3.1.3. Impact of Diabetes Mellitus Types on Obstetrical Interventions and Maternal and Neonatal Health Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Battarbee, A.N.; Venkatesh, K.K.; Aliaga, S.; Boggess, K.A. The association of pregestational and gestational diabetes with severe neonatal morbidity and mortality. J. Perinatol. 2019, 40, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Stogianni, A.; Lendahls, L.; Landin-Olsson, M.; Thunander, M. Obstetric and perinatal outcomes in pregnancies complicated by diabetes, and control pregnancies, in Kronoberg, Sweden. BMC Pregnancy Childbirth 2019, 19, 159. [Google Scholar] [CrossRef] [PubMed]
- De Andrés, A.L.; Jiménez-García, R.; Carrasco-Garrido, P. Trends in pregestational diabetes among women delivering in Spain, 2001–2008. Int. J. Gynaecol. Obstet. 2012, 117, 182–183. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, L.; Casas, J.P.; Hingorani, A.D.; Williams, D. Type 2 diabetes mellitus after gestational diabetes: A systematic review and meta-analysis. Lancet 2009, 373, 1773–1779. [Google Scholar] [CrossRef]
- Tinker, S.C.; Gilboa, S.M.; Moore, C.A.; Waller, D.K.; Simeone, R.M.; Kim, S.Y.; Denise, J.; Jamieson, D.J.; Lorenzo, D.; Botto, L.D.; et al. Specific birth defects in pregnancies of women with diabetes: National Birth Defects Prevention Study, 1997–2011. Am. J. Obstet. Gynecol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Ladfors, L.; Shaat, N.; Wiberg, N.; Katasarou, A.; Berntorp, K.; Kristensen, K. Fetal overgrowth in women with type 1 and type 2 diabetes mellitus. PLoS ONE 2017, 12, e0187917. [Google Scholar] [CrossRef]
- Abouzeid, M.; Versace, V.L.; Janus, E.D.; Davey, M.A.; Philpot, B.; Oats, J.; Dunbar, J.A. A population-based observational study of diabetes during pregnancy in Victoria, Australia, 1999–2008. BMJ Open 2014, 4, e005394. [Google Scholar] [CrossRef]
- Bardenheier, B.H.; Imperatore, G.; Devlin, H.M.; Kim, S.Y.; Cho, P.; Geiss, L.S. Trends in pre-pregnancy diabetes among deliveries in 19 U.S. states, 2000–2010. Am. J. Prev. Med. 2015, 48, 154–161. [Google Scholar] [CrossRef]
- Bardenheier, B.H.; Imperatore, G.; Gilboa, S.M.; Geiss, L.S.; Saydah, S.H.; Devlin, H.M.; Kim, S.Y.; Gregg, E.W. Trends in gestational diabetes among hospital deliveries in 19 U.S. states, 2000–2010. Am. J. Prev. Med. 2015, 49, 12–19. [Google Scholar] [CrossRef]
- Mackin, S.T.; Nelson, S.M.; Kerssens, J.J.; Wood, R.; Wild, S.; Colhoun, H.M.; Leese, G.P.; Philip, S.; Lindsay, R.S. Diabetes and pregnancy: National trends over a 15 year period. Diabetologia 2018, 61, 1081–1088. [Google Scholar] [CrossRef]
- Collier, A.; Abraham, E.C.; Armstrong, J.; Godwin, J.; Monteath, K.; Lindsay, R. Reported prevalence of gestational diabetes in Scotland: The relationship with obesity, age, socioeconomic status, smoking and macrosomia, and how many are we missing? J. Diabetes Investig. 2017, 8, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Lopez-de-Andres, A.; Carrasco-Garrido, P.; Gil-de-Miguel, A.; Hernandez-Barrera, V.; Jiménez-García, R. Trends in deliveries in women with gestational diabetes in Spain, 2001–2008. Diabetes Res. Clin. Pract. 2011, 91, e27–e29. [Google Scholar] [CrossRef] [PubMed]
- Coton, S.J.; Nazareth, I.; Petersen, I. A cohort study of trends in the prevalence of pregestational diabetes in pregnancy recorded in UK general practice between 1995 and 2012. BMJ Open 2016, 6, e009494. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, A.; Sabr, Y.; Hutcheon, J.A.; Donovan, L.; Lyons, J.; Burrows, J.; Joseph, K.S. Trends in Obstetric Intervention and Pregnancy Outcomes of Canadian Women with Diabetes in Pregnancy from 2004 to 2015. J. Endocr. Soc. 2017, 1, 1540–1549. [Google Scholar] [CrossRef] [PubMed]
- Fadl, H.E.; Simmons, D. Trends in diabetes in pregnancy in Sweden 1998–2012. BMJ Open Diabetes Res. Care 2016, 4, e000221. [Google Scholar] [CrossRef]
- Deputy, N.P.; Kim, S.Y.; Conrey, E.J.; Bullard, K.M. Prevalence and Changes in Preexisting Diabetes and Gestational Diabetes Among Women Who Had a Live Birth—United States, 2012–2016. MMWR 2018, 67, 1201–1207. [Google Scholar] [CrossRef]
- Kuklina, E.V.; Whiteman, M.K.; Hillis, S.D.; Jamieson, D.J.; Meikle, S.F.; Posner, S.F.; Marchbanks, P.A. An enhanced method for identifying obstetric deliveries: Implications for estimating maternal morbidity. Matern. Child Health J. 2008, 12, 469–477. [Google Scholar] [CrossRef]
- Spanish Group of Diabetes and Pregnancy. Care of pregnancies complicated by diabetes. Clinical practice guidelines: 2014 update. Av. Diabetol. 2015, 31, 45–59. [Google Scholar] [CrossRef]
- Ministerio de Sanidad Servicios Social e Igualdad. Estrategia en Diabetes del Sistema Nacional de Salud 2012. Available online: https://www.mscbs.gob.es/organizacion/sns/planCalidadSNS/pdf/excelencia/cuidadospaliativos-diabetes/DIABETES/Estrategia_en_diabetes_del_SNS_Accesible.pdf (accessed on 12 February 2020).
- Bateman, B.T.; Mhyre, J.M.; Hernandez-Diaz, S.; Huybrechts, K.F.; Fischer, M.A.; Creanga, A.A.; Callaghan, W.M.; Gagne, J.J. Development of a comorbidity index for use in obstetric patients. Obstet. Gynecol. 2013, 122, 957–965. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Severe Maternal Morbidity in the United States. November 2017. Available online: www.cdc.gov/reproductivehealth/maternalinfanthealth/severematernalmorbidity.html (accessed on 7 October 2019).
- Bartlett, J. Estimating Risk Ratios from Observational Data in Stata. Available online: https://thestatsgeek.com/2015/03/09/estimating-risk-ratios-from-observational-data-in-stata/ (accessed on 12 February 2020).
- Bliddal, M.; Möller, S.; Vinter, C.A.; Rubin, K.H.; Gagne, J.J.; Pottegård, A. Validation of a comorbidity index for use in obstetric patients: A nationwide cohort study. Acta Obstet. Gynecol. Scand. 2019. [Google Scholar] [CrossRef]
- Metcalfe, A.; Lix, L.M.; Johnson, J.A.; Currie, G.; Lyon, A.W.; Bernier, F.; Tough, S.C. Validation of an obstetric comorbidity index in an external population. BJOG 2015, 122, 1748–1755. [Google Scholar] [CrossRef] [PubMed]
- Somerville, N.J.; Nielsen, T.C.; Harvey, E.; Easter, S.R.; Bateman, B.; Diop, H.; Manning, S.E. Obstetric Comorbidity and Severe Maternal Morbidity among Massachusetts Delivery Hospitalizations, 1998–2013. Matern. Child Health J. 2019, 23, 1152–1158. [Google Scholar] [CrossRef] [PubMed]
- Timur, B.B.; Timur, H.; Tokmak, A.; Isik, H.; Eyi, E.G.Y. The Influence of Maternal Obesity on Pregnancy Complications and Neonatal Outcomes in Diabetic and Nondiabetic Women. Geburtshilfe Frauenheilkd. 2018, 78, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Hackshaw, A.; Rodeck, C.; Boniface, S. Maternal smoking in pregnancy and birth defects: A systematic review based on 173 687 malformed cases and 11.7 million controls. Hum. Reprod. Update 2011, 17, 589–604. [Google Scholar] [CrossRef]
- Borsari, L.; Malagoli, C.; Werler, M.M.; Rothman, K.J.; Malavolti, M.; Rodolfi, R.; De Girolamo, G.; Nicolini, F.; Vinceti, M. Joint Effect of Maternal Tobacco Smoking and Pregestational Diabetes on Preterm Births and Congenital Anomalies: A Population-Based Study in Northern Italy. J. Diabetes Res. 2018, 2018, 2782741. [Google Scholar] [CrossRef]
- Ringholm, L.; Damm, P.; Mathiesen, E.R. Improving pregnancy outcomes in women with diabetes mellitus: Modern management. Nat. Rev. Endocrinol. 2019, 15, 406–416. [Google Scholar] [CrossRef]
- Persson, M.; Norman, M.; Hanson, U. Obstetric and perinatal outcomes in type 1 diabetic pregnancies: A large, population-based study. Diabetes Care 2009, 32, 2005–2009. [Google Scholar] [CrossRef]
- Persson, M.; Pasupathy, D.; Hanson, U.; Westgren, M.; Norman, M. Pre-pregnancy body mass index and the risk of adverse outcome in type 1 diabetic pregnancies: A population-based cohort study. BMJ Open 2012, 2, e000601. [Google Scholar] [CrossRef]
- Ehrenberg, H.M.; Huston-Presley, L.; Catalano, P.M. The influence of obesity and gestational diabetes mellitus on accretion and the distribution of adipose tissue in pregnancy. Am. J. Obstet. Gynecol. 2003, 189, 944–948. [Google Scholar] [CrossRef]
- Basterra-Gortari, F.J.; Bes-Rastrollo, M.; Ruiz-Canela, M.; Gea, A.; Martinez-Gonzalez, M.Á. Trends of Obesity Prevalence among Spanish Adults with Diabetes, 1987–2012. Med. Clin. 2017, 148, 250–256. [Google Scholar] [CrossRef]
- Borsari, L.; Malagoli, C.; Ballotari, P.; De Girolamo, G.; Bonora, K.; Violi, F.; Capelli, O.; Rodolfi, R.; Nicolini, F.; Vinceti, M. Validity of hospital discharge records to identify pregestational diabetes in an Italian population. Diabetes Res. Clin. Pract. 2017, 123, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Devlin, H.M.; Desai, J.; Walaszek, A. Reviewing performance of birth certificate and hospital discharge data to identify births complicated by maternal diabetes. Matern. Child Health J. 2009, 13, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.C.; Ford, J.B.; Cameron, C.A.; Roberts, C.L. The accuracy of population health data for monitoring trends and outcomes among women with diabetes in pregnancy. Diabetes Res. Clin. Pract. 2008, 81, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Bowker, S.L.; Savu, A.; Donovan, L.E.; Johnson, J.A.; Kaul, P. Validation of administrative and clinical case definitions for gestational diabetes mellitus against laboratory results. Diabet. Med. 2017, 34, 781–785. [Google Scholar] [CrossRef]
- Havard, A.; Jorm, L.R.; Lujic, S. Risk adjustment for smoking identified through tobacco use diagnoses in hospital data: A validation study. PLoS ONE 2014, 9, e95029. [Google Scholar] [CrossRef]


{kind=link}
| 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | p | ||
|---|---|---|---|---|---|---|---|---|---|
| Without DM | N | 373,235 | 357,622 | 347,589 | 333,999 | 310,116 | 308,120 | 309,866 | |
| Rate per 10,000 deliveries | 9522.2 | 9455.37 | 9443.42 | 9427.25 | 9384.65 | 9364.95 | 9405.12 | <0.001 | |
| Maternal age, mean (SD) | 30.5 (5.56) | 30.68 (5.55) | 31 (5.51) | 31.17 (5.54) | 31.35 (5.56) | 31.49 (5.57) | 31.67 (5.6) | <0.001 | |
| Type 1 DM | N | 705 | 771 | 789 | 859 | 811 | 865 | 761 | |
| Rate per 10,000 deliveries | 17.98 | 20.38 | 21.43 | 24.24 | 24.54 | 26.29 | 23.09 | <0.001 | |
| Maternal age, mean (SD) | 31.52 (5.03) | 31.7 (5.24) | 31.89 (5.19) | 31.81 (5.43) | 32.15 (5.13) | 32.32 (5.06) | 32.53 (5.2) | 0.001 | |
| Type 2 DM | N | 571 | 545 | 591 | 586 | 668 | 692 | 738 | |
| Rate per 10,000 deliveries | 14.56 | 14.41 | 16.05 | 16.54 | 20.21 | 21.03 | 22.4 | <0.001 | |
| Maternal age, mean (SD) | 33.58 (5.78) | 33.9 (5.52) | 34.26 (5.28) | 34.38 (5.19) | 34.21 (5.62) | 34.22 (5.26) | 34.47 (5.3) | 0.073 | |
| Gestational DM | N | 17,452 | 19,283 | 19,106 | 18,847 | 18,855 | 19,337 | 18,100 | |
| Rate per 10,000 deliveries | 445.24 | 509.83 | 519.07 | 531.96 | 570.58 | 587.72 | 549.37 | <0.001 | |
| Maternal age, mean (SD) | 33.19 (5.07) | 33.29 (5.01) | 33.46 (4.96) | 33.67 (4.99) | 33.88 (5.02) | 34.06 (4.95) | 34.16 (5.04) | <0.001 |
| Without DM (n = 2,340,547) | Type 1 DM (n = 5561) | Type 2 DM (n = 4391) | Gestational DM (n = 130,980) | p | |
|---|---|---|---|---|---|
| Maternal age, mean (SD) | 31.1 (5.57) | 32 (5.19) | 34.17 (5.42) | 33.67 (5.02) | <0.001 |
| 15–24 years, n (%) | 313,139 (13.38) | 489 (8.79) | 174 (3.96) | 5784 (4.42) | <0.001 |
| 25–34 years, n (%) | 1,358,332 (58.03) | 3192 (57.4) | 2060 (46.91) | 65,494 (50) | <0.001 |
| 35–39 years, n (%) | 553,578 (23.65) | 1570 (28.23) | 1486 (33.84) | 44,693 (34.12) | <0.001 |
| 40–44 years, n (%) | 109,299 (4.67) | 297 (5.34) | 588 (13.39) | 13,843 (10.57) | <0.001 |
| ≥45 years, n (%) | 6199 (0.26) | 13 (0.23) | 83 (1.89) | 1166 (0.89) | 0.454 |
| Pulmonary hypertension, n (%) | 112 (0) | <5 | <5 | 8 (0.01) | <0.001 |
| Placenta previa, n (%) | 11,817 (0.5) | 35 (0.63) | 27 (0.61) | 822 (0.63) | <0.001 |
| Sickle cell disease, n (%) | 7174 (0.31) | 28 (0.5) | 16 (0.36) | 485 (0.37) | <0.001 |
| Gestational hypertension, n (%) | 24,462 (1.05) | 231 (4.15) | 144 (3.28) | 3221 (2.46) | <0.001 |
| Mild preeclampsia or unspecified preeclampsia, n (%) | 21,877 (0.93) | 349 (6.28) | 198 (4.51) | 2431 (1.86) | <0.001 |
| Severe preeclampsia/eclampsia, n (%) | 10,215 (0.44) | 123 (2.21) | 74 (1.69) | 851 (0.65) | <0.001 |
| Chronic renal disease, n (%) | 4029 (0.17) | 161 (2.9) | 62 (1.41) | 268 (0.2) | <0.001 |
| Preexisting hypertension, n (%) | 18,759 (0.8) | 268 (4.82) | 460 (10.48) | 3041 (2.32) | <0.001 |
| Chronic ischemic heart disease, n (%) | 149 (0.01) | <5 | <5 | 16 (0.01) | <0.001 |
| Congenital heart disease, n (%) | 1823 (0.08) | 12 (0.22) | <5 | 118 (0.09) | 0.001 |
| Systemic lupus erythematosus, n (%) | 1822 (0.08) | 3 (0.05) | <5 | 81 (0.06) | 0.166 |
| Human immunodeficiency virus, n (%) | 2043 (0.09) | <5 | 9 (0.2) | 104 (0.08) | 0.012 |
| Multiple gestation, n (%) | 50,342 (2.15) | 101 (1.82) | 98 (2.23) | 4475 (3.42) | <0.001 |
| Drug abuse, n (%) | 4468 (0.19) | 13 (0.23) | 6 (0.14) | 181 (0.14) | <0.001 |
| Alcohol abuse, n (%) | 764 (0.03) | <5 | <5 | 31 (0.02) | 0.035 |
| Tobacco use, n (%) | 114,001 (4.87) | 334 (6.01) | 249 (5.67) | 7466 (5.7) | <0.001 |
| Cardiac valvular disease, n (%) | 2219 (0.09) | 5 (0.09) | 8 (0.18) | 160 (0.12) | 0.005 |
| Chronic congestive heart failure, n (%) | <5 | <5 | <5 | <5 | 0.981 |
| Asthma, n (%) | 35,711 (1.53) | 67 (1.2) | 99 (2.25) | 2319 (1.77) | <0.001 |
| Obesity, n (%) | 38,657 (1.65) | 164 (2.95) | 474 (10.79) | 6896 (5.26) | <0.001 |
| Previous cesarean delivery, n (%) | 192,441 (8.22) | 1033 (18.58) | 809 (18.42) | 15,144 (11.56) | <0.001 |
| Obstetric Comorbidity Index | 978,769 (41.82) | 3306 (59.45) | 3079 (70.12) | 78,960 (60.28) | <0.001 |
| Without DM | Type 1 DM | Type 2 DM | Gestational DM | |
|---|---|---|---|---|
| Labor induction. n (%) | 357,116 (15.26) | 1645 (29.58) | 1335 (30.4) | 29,535 (22.55) |
| Crude RR (95% CI) | 1.94 (1.85–2.03) | 1.99 (1.89–2.10) | 1.48 (1.46–1.49) | |
| Adjusted RR (95% CI) | 1.91 (1.82–2.00) | 1.94 (1.84–2.05) | 1.45 (1.44–1.47) | |
| Cesarean delivery n (%) | 505,715 (21.61) | 3162 (56.86) | 2084 (47.46) | 37,828 (28.88) |
| Crude RR (95% CI) | 2.63 (2.54–2.72) | 2.20 (2.10–2.29) | 1.34 (1.32–1.35) | |
| Adjusted RR (95% CI) | 2.34 (2.26–2.43) | 1.83 (1.75–1.91) | 1.18 (1.17–1.20) | |
| Forceps/vacuum extraction n (%) | 288,088 (12.31) | 650 (11.69) | 463 (10.54) | 15,523 (11.85) |
| Crude RR (95% CI) | 0.94 (0.88–1.02) | 0.86 (0.78–0.94) | 0.96 (0.95–0.98) | |
| Adjusted RR (95% CI) | 0.96 (0.89–1.04) | 0.88 (0.80–0.96) | 0.98 (0.96–0.99) | |
| Episiotomy n (%) | 498,487 (21.3) | 690 (12.41) | 562 (12.8) | 25,113 (19.17) |
| Crude RR (95% CI) | 0.58 (0.54–0.63) | 0.60 (0.55–0.65) | 0.90 (0.88–0.91) | |
| Adjusted RR (95% CI) | 0.61 (0.57–0.66) | 0.65 (0.60–0.71) | 0.95 (0.94–0.96) | |
| Severe Maternal morbidity n (%) | 32,744 (1.4) | 170 (3.06) | 90 (2.05) | 2103 (1.61) |
| Crude RR (95% CI) | 2.18 (1.88–2.54) | 1.46 (1.19–1.80) | 1.15 (1.10–1.20) | |
| Adjusted RR (95% CI) | 1.97 (1.70–2.29) | 1.25 (1.02–1.54) | 1.03 (0.99–1.08) | |
| Prolonged maternal length of stay n (%) | 245,451 (10.49) | 1883 (33.86) | 1097 (24.98) | 14,662 (11.19) |
| Crude RR (95% CI) | 3.22 (3.09–3.38) | 2.38 (2.24–2.53) | 1.07 (1.05–1.08) | |
| Adjusted RR (95% CI) | 3.09 (2.95–3.23) | 2.22 (2.09–2.35) | 1.02 (0.99–1.03) | |
| Preterm birth n (%) | 140,101 (5.99) | 1221 (21.96) | 660 (15.03) | 10,298 (7.86) |
| Crude RR (95% CI) | 3.66 (3.47–3.88) | 2.51 (2.33–2.71) | 1.31 (1.29–1.34) | |
| Adjusted RR (95% CI) | 3.32 (3.14–3.51) | 2.15 (1.99–2.32) | 1.18 (1.16–1.21) | |
| Fetal overgrowth n (%) | 28,226 (1.21) | 572 (10.29) | 322 (7.33) | 4419 (3.37) |
| Crude RR (95% CI) | 8.53 (7.85–9.26) | 6.08 (5.45–6.79) | 2.80 (2.71–2.89) | |
| Adjusted RR (95% CI) | 8.05 (7.41–8.75) | 5.55 (4.97–6.20) | 2.63 (2.55–2.72) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-de-Andrés, A.; Perez-Farinos, N.; Hernández-Barrera, V.; Palomar-Gallego, M.A.; Carabantes-Alarcón, D.; Zamorano-León, J.J.; De Miguel-Diez, J.; Jimenez-Garcia, R. A Population-Based Study of Diabetes during Pregnancy in Spain (2009–2015): Trends in Incidence, Obstetric Interventions, and Pregnancy Outcomes. J. Clin. Med. 2020, 9, 582. https://doi.org/10.3390/jcm9020582
López-de-Andrés A, Perez-Farinos N, Hernández-Barrera V, Palomar-Gallego MA, Carabantes-Alarcón D, Zamorano-León JJ, De Miguel-Diez J, Jimenez-Garcia R. A Population-Based Study of Diabetes during Pregnancy in Spain (2009–2015): Trends in Incidence, Obstetric Interventions, and Pregnancy Outcomes. Journal of Clinical Medicine. 2020; 9(2):582. https://doi.org/10.3390/jcm9020582
Chicago/Turabian StyleLópez-de-Andrés, Ana, Napoleón Perez-Farinos, Valentín Hernández-Barrera, María A. Palomar-Gallego, David Carabantes-Alarcón, José J. Zamorano-León, Javier De Miguel-Diez, and Rodrigo Jimenez-Garcia. 2020. "A Population-Based Study of Diabetes during Pregnancy in Spain (2009–2015): Trends in Incidence, Obstetric Interventions, and Pregnancy Outcomes" Journal of Clinical Medicine 9, no. 2: 582. https://doi.org/10.3390/jcm9020582
APA StyleLópez-de-Andrés, A., Perez-Farinos, N., Hernández-Barrera, V., Palomar-Gallego, M. A., Carabantes-Alarcón, D., Zamorano-León, J. J., De Miguel-Diez, J., & Jimenez-Garcia, R. (2020). A Population-Based Study of Diabetes during Pregnancy in Spain (2009–2015): Trends in Incidence, Obstetric Interventions, and Pregnancy Outcomes. Journal of Clinical Medicine, 9(2), 582. https://doi.org/10.3390/jcm9020582