Clarithromycin Versus Metronidazole in First-Line Helicobacter Pylori Triple Eradication Therapy Based on Resistance to Antimicrobial Agents: Meta-Analysis

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
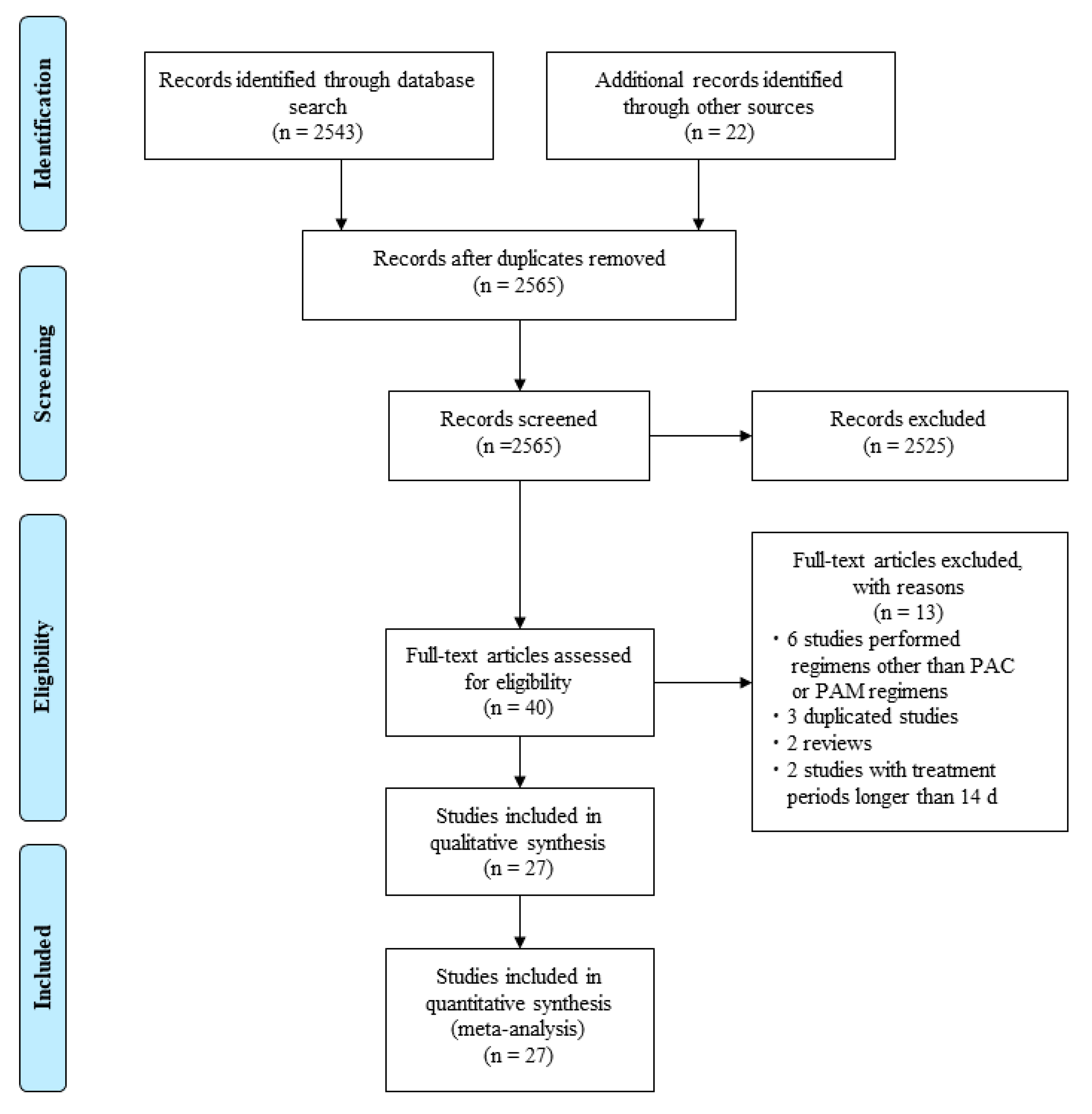
2.1. Search Strategy and Inclusion Criteria
- RCTs published up to December 2018;
- Studies comparing eradication rates of PAC therapy with those of PAM therapy for H. pylori infection;
- Studies performed as first-line treatment;
- Studies that detected H. pylori infection by one or more tests (urea breath test, histology, rapid urease test, stool monoclonal antigen or culture);
- Studies checking eradication outcome ≥ 4 weeks after eradication therapy; and
- Studies written in English.
- Studies performed with regimens other than PAC or PAM regimens, and
- Studies with treatment periods > 14 days.
2.2. Statistical Analysis
3. Results
3.1. Literature Search and Data Extraction
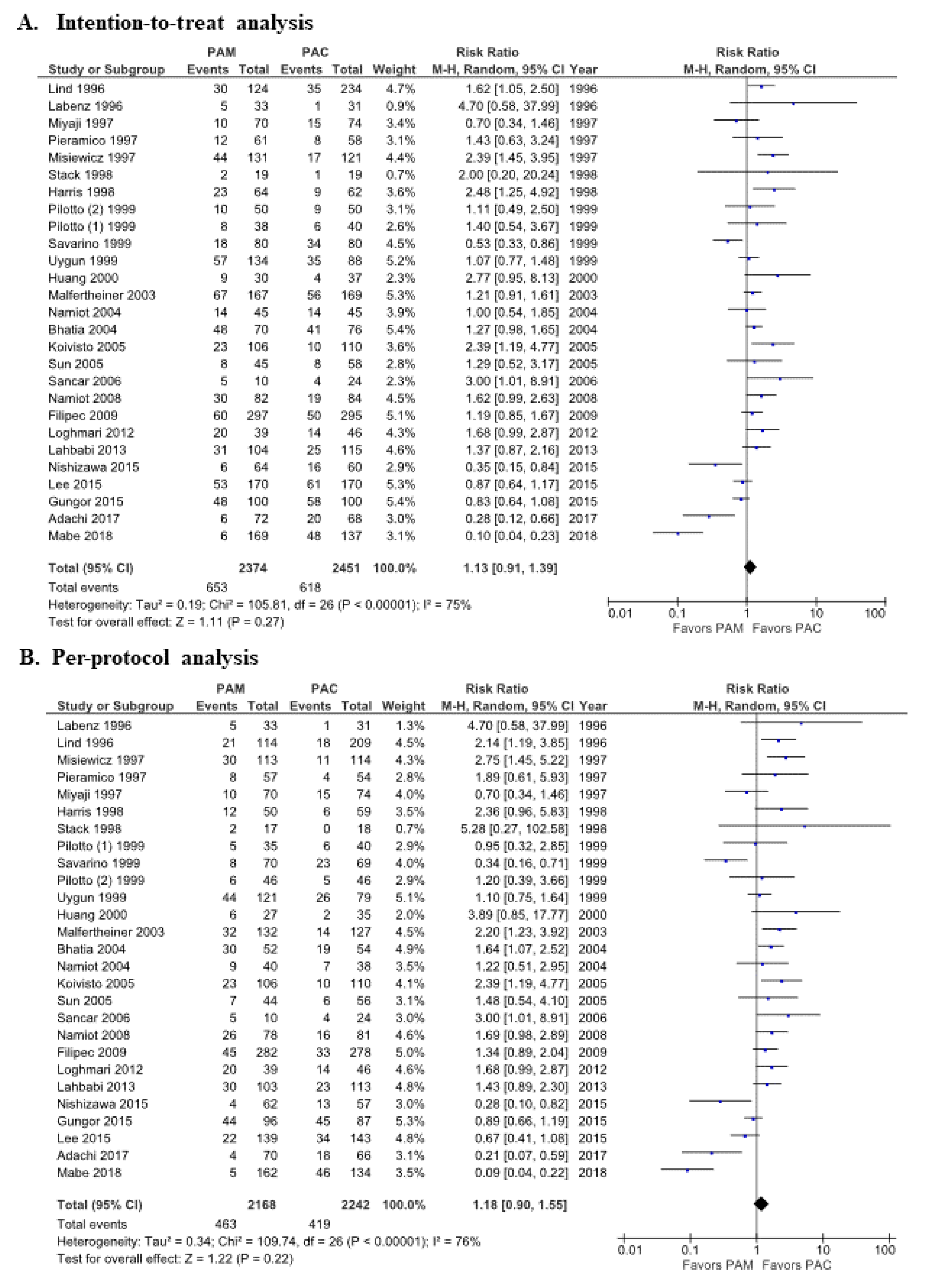
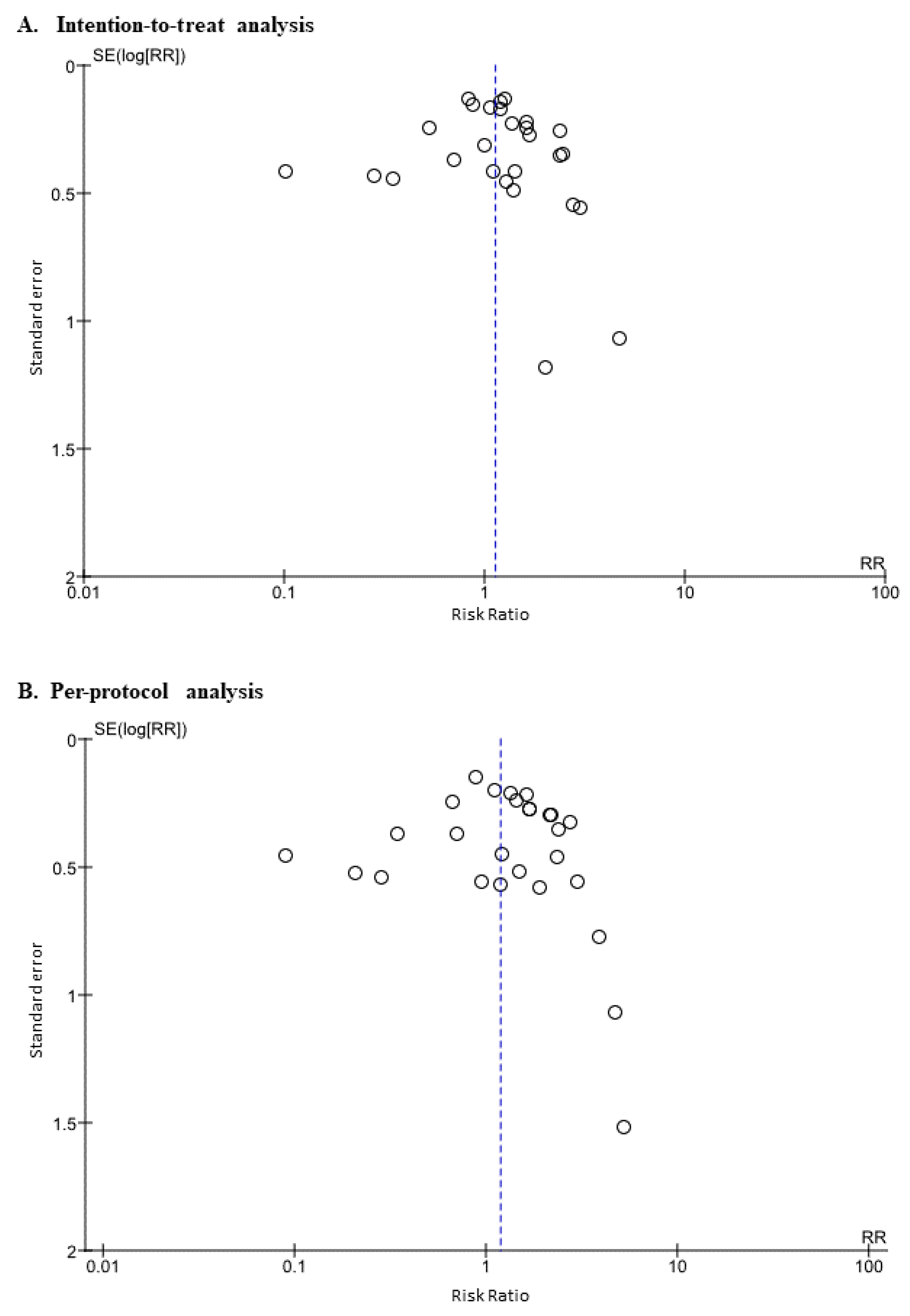
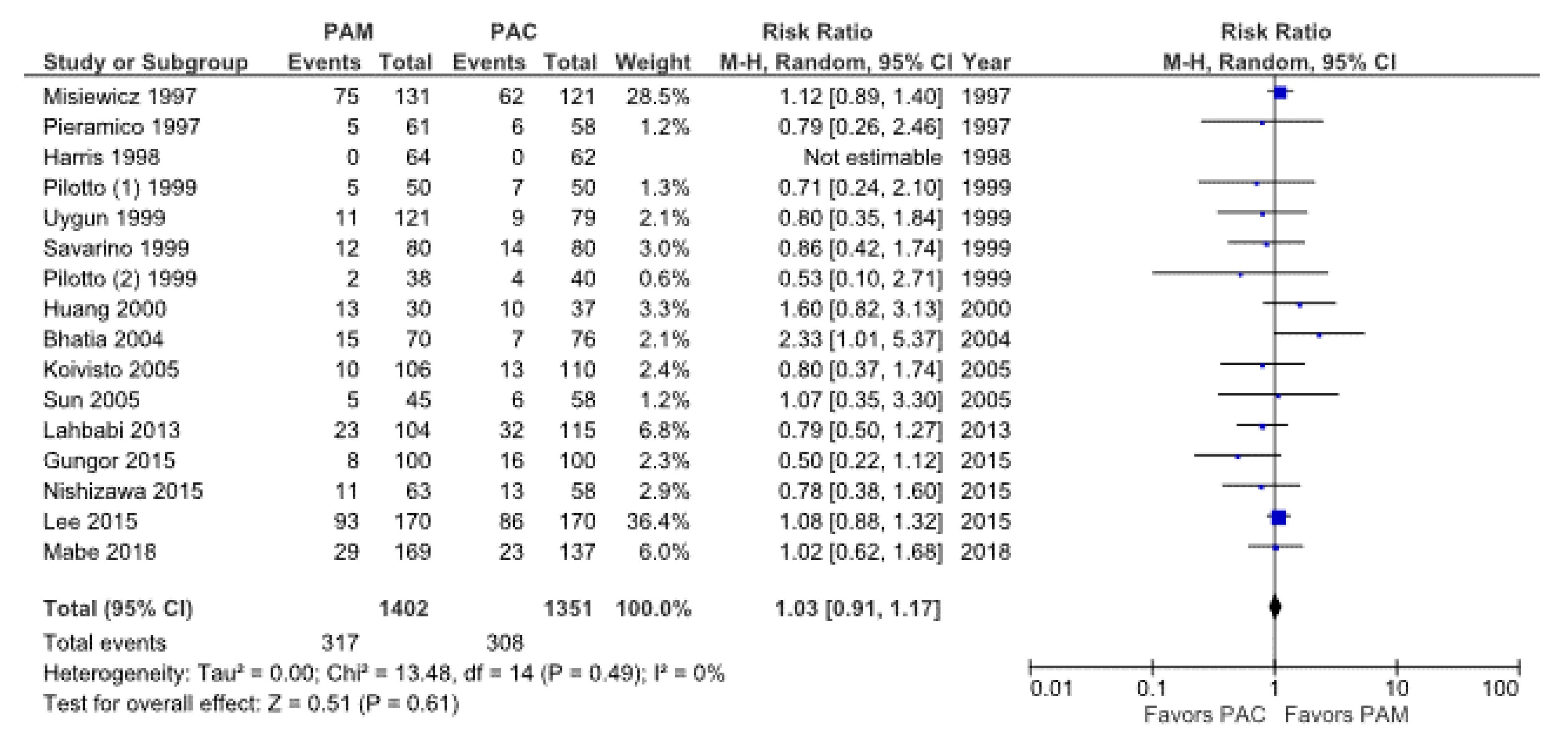
3.2. Meta-Analysis for Eradication Rate of PAC vs. PAM Therapy
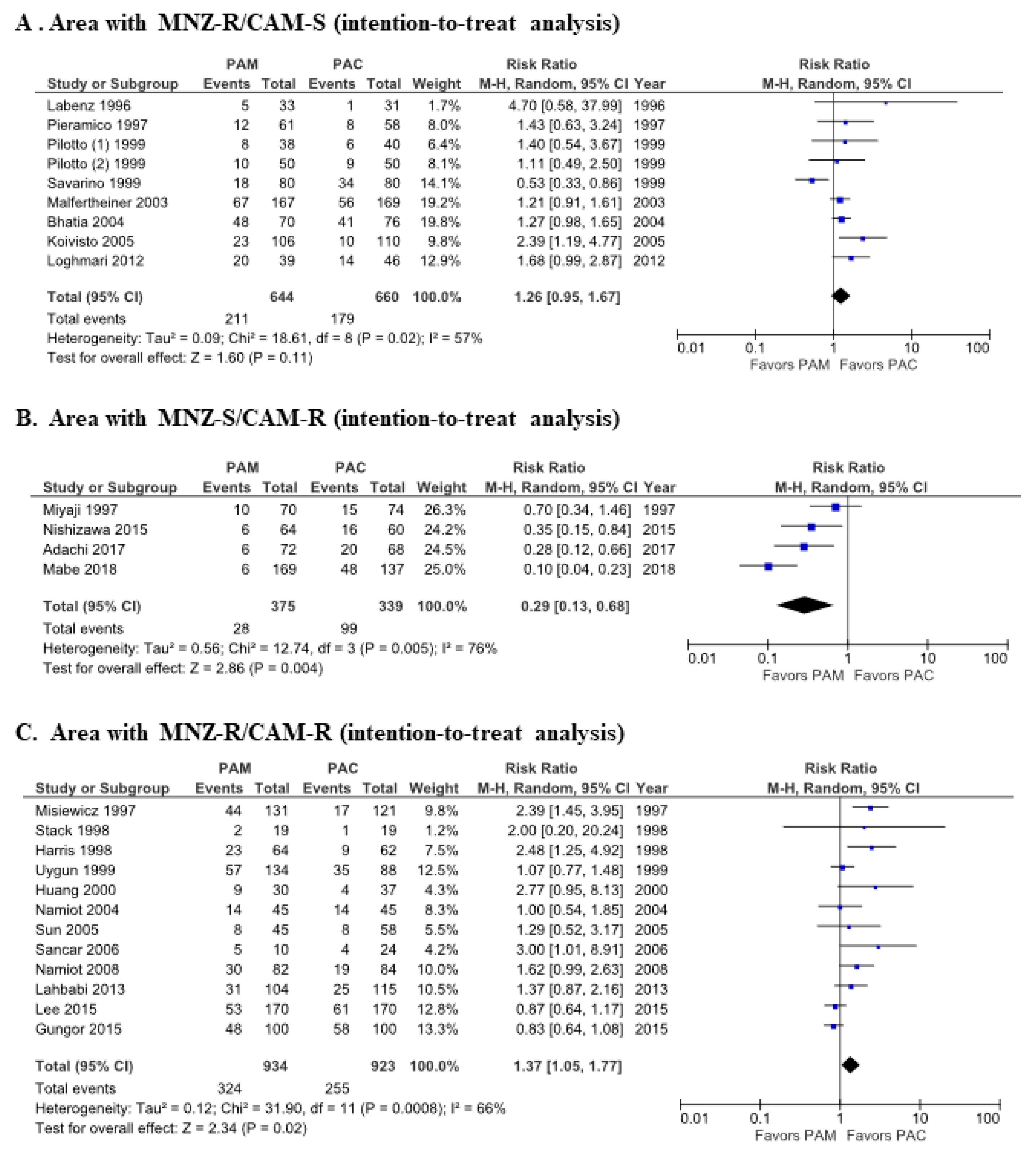
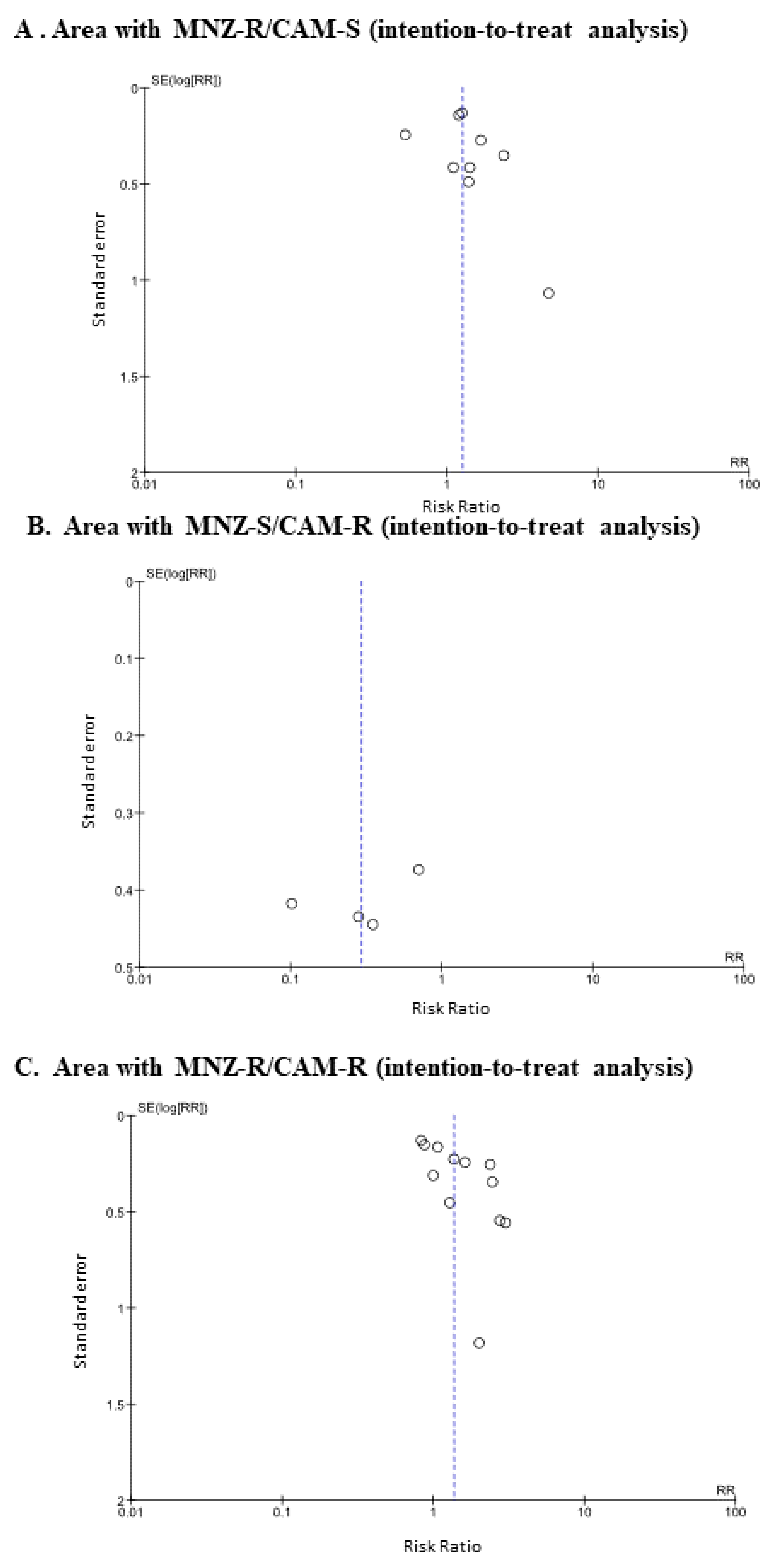
3.3. Subgroup Analysis of Eradication Rates by Different Geographical Areas Based on Rates of CAM and MNZ Resistance
3.4. Meta-Analysis of the Incidence Rates of Adverse Events from PAC Therapy vs PAM Therapy
4. Discussion
4.1. Importance of H. pylori Antimicrobial Agent Resistance
4.2. Alternatives to Triple Therapy
4.3. Efficacy of Vonoprazan-Containing Triple Therapy
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef]
- Wotherspoon, A.C.; Doglioni, C.; de Boni, M.; Spencer, J.; Isaacson, P.G. Antibiotic treatment for low-grade gastric MALT lymphoma. Lancet 1994, 343, 1503. [Google Scholar] [CrossRef]
- Sugimoto, M.; Kajimura, M.; Shirai, N.; Furuta, T.; Kanaoka, S.; Ikuma, M.; Sato, Y.; Hishida, A. Outcome of radiotherapy for gastric mucosa-associated lymphoid tissue lymphoma refractory to Helicobacter pylori eradication therapy. Intern. Med. 2006, 45, 405–409. [Google Scholar] [CrossRef]
- Take, S.; Mizuno, M.; Ishiki, K.; Nagahara, Y.; Yoshida, T.; Yokota, K.; Oguma, K.; Okada, H.; Shiratori, Y. The effect of eradicating helicobacter pylori on the development of gastric cancer in patients with peptic ulcer disease. Am. J. Gastroenterol. 2005, 100, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Tebbe, B.; Geilen, C.C.; Schulzke, J.D.; Bojarski, C.; Radenhausen, M.; Orfanos, C.E. Helicobacter pylori infection and chronic urticaria. J. Am. Acad. Dermatol. 1996, 34, 685–686. [Google Scholar] [CrossRef]
- Annibale, B.; Marignani, M.; Monarca, B.; Antonelli, G.; Marcheggiano, A.; Martino, G.; Mandelli, F.; Caprilli, R.; Delle Fave, G. Reversal of iron deficiency anemia after Helicobacter pylori eradication in patients with asymptomatic gastritis. Ann. Intern. Med. 1999, 131, 668–672. [Google Scholar] [CrossRef] [PubMed]
- Asaka, M.; Sugiyama, T.; Kato, M.; Satoh, K.; Kuwayama, H.; Fukuda, Y.; Fujioka, T.; Takemoto, T.; Kimura, K.; Shimoyama, T.; et al. A multicenter, double-blind study on triple therapy with lansoprazole, amoxicillin and clarithromycin for eradication of Helicobacter pylori in Japanese peptic ulcer patients. Helicobacter 2001, 6, 254–261. [Google Scholar] [CrossRef]
- Graham, D.Y.; Fischbach, L. Helicobacter pylori treatment in the era of increasing antibiotic resistance. Gut 2010, 59, 1143–1153. [Google Scholar] [CrossRef]
- Thung, I.; Aramin, H.; Vavinskaya, V.; Gupta, S.; Park, J.Y.; Crowe, S.E.; Valasek, M.A. Review article: The global emergence of Helicobacter pylori antibiotic resistance. Aliment. Pharmacol. Ther. 2016, 43, 514–533. [Google Scholar] [CrossRef]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382. [Google Scholar] [CrossRef]
- Kobayashi, I.; Murakami, K.; Kato, M.; Kato, S.; Azuma, T.; Takahashi, S.; Uemura, N.; Katsuyama, T.; Fukuda, Y.; Haruma, K.; et al. Changing antimicrobial susceptibility epidemiology of Helicobacter pylori strains in Japan between 2002 and 2005. J. Clin. Microbiol. 2007, 45, 4006–4010. [Google Scholar] [CrossRef] [PubMed]
- Fischbach, L.; Evans, E.L. Meta-analysis: The effect of antibiotic resistance status on the efficacy of triple and quadruple first-line therapies for Helicobacter pylori. Aliment. Pharmacol. Ther. 2007, 26, 343–357. [Google Scholar] [CrossRef] [PubMed]
- Megraud, F. Helicobacter pylori and antibiotic resistance. Gut 2007, 56, 1502. [Google Scholar] [CrossRef]
- Murakami, K.; Sato, R.; Okimoto, T.; Nasu, M.; Fujioka, T.; Kodama, M.; Kagawa, J.; Sato, S.; Abe, H.; Arita, T. Eradication rates of clarithromycin-resistant Helicobacter pylori using either rabeprazole or lansoprazole plus amoxicillin and clarithromycin. Aliment. Pharmacol. Ther. 2002, 16, 1933–1938. [Google Scholar] [CrossRef]
- Furuta, T.; Shirai, N.; Takashima, M.; Xiao, F.; Hanai, H.; Nakagawa, K.; Sugimura, H.; Ohashi, K.; Ishizaki, T. Effects of genotypic differences in CYP2C19 status on cure rates for Helicobacter pylori infection by dual therapy with rabeprazole plus amoxicillin. Pharmacogenetics 2001, 11, 341–348. [Google Scholar] [CrossRef]
- Fallone, C.A.; Chiba, N.; van Zanten, S.V.; Fischbach, L.; Gisbert, J.P.; Hunt, R.H.; Jones, N.L.; Render, C.; Leontiadis, G.I.; Moayyedi, P.; et al. The Toronto Consensus for the Treatment of Helicobacter pylori Infection in Adults. Gastroenterology 2016, 151, 51–69. [Google Scholar] [CrossRef]
- Adachi, T.; Matsui, S.; Watanabe, T.; Okamoto, K.; Okamoto, A.; Kono, M.; Yamada, M.; Nagai, T.; Komeda, Y.; Minaga, K.; et al. Comparative Study of Clarithromycin- versus Metronidazole-Based Triple Therapy as First-Line Eradication for Helicobacter pylori. Oncology 2017, 93 (Suppl. 1), 15–19. [Google Scholar] [CrossRef]
- Mabe, K.; Okuda, M.; Kikuchi, S.; Amagai, K.; Yoshimura, R.; Kato, M.; Sakamoto, N.; Asaka, M. Randomized controlled trial: PPI-based triple therapy containing metronidazole versus clarithromycin as first-line treatment for Helicobacter pylori in adolescents and young adults in Japan. J. Infect. Chemother. 2018, 24, 538–543. [Google Scholar] [CrossRef]
- Shiota, S.; Yamaoka, Y. Strategy for the treatment of Helicobacter pylori infection. Curr. Pharm. Des. 2014, 20, 4489–4500. [Google Scholar] [CrossRef]
- Mantel, N.; Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar]
- Berlin, J.A.; Laird, N.M.; Sacks, H.S.; Chalmers, T.C. A comparison of statistical methods for combining event rates from clinical trials. Stat. Med. 1989, 8, 141–151. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 2015, 45, 139–145. [Google Scholar] [CrossRef]
- Koivisto, T.T.; Rautelin, H.I.; Voutilainen, M.E.; Heikkinen, M.T.; Koskenpato, J.P.; Farkkila, M.A. First-line eradication therapy for Helicobacter pylori in primary health care based on antibiotic resistance: Results of three eradication regimens. Aliment. Pharmacol. Ther. 2005, 21, 773–782. [Google Scholar] [CrossRef] [PubMed]
- Bouihat, N.; Burucoa, C.; Benkirane, A.; Seddik, H.; Sentissi, S.; Al Bouzidi, A.; Elouennas, M.; Benouda, A. Helicobacter pylori Primary Antibiotic Resistance in 2015 in Morocco: A Phenotypic and Genotypic Prospective and Multicenter Study. Microb. Drug. Resist. 2017, 23, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Ben Mansour, K.; Burucoa, C.; Zribi, M.; Masmoudi, A.; Karoui, S.; Kallel, L.; Chouaib, S.; Matri, S.; Fekih, M.; Zarrouk, S.; et al. Primary resistance to clarithromycin, metronidazole and amoxicillin of Helicobacter pylori isolated from Tunisian patients with peptic ulcers and gastritis: A prospective multicentre study. Ann. Clin. Microbiol. Antimicrob. 2010, 9, 22. [Google Scholar] [CrossRef] [PubMed]
- Binkowska, A.; Biernat, M.M.; Laczmanski, L.; Gosciniak, G. Molecular Patterns of Resistance Among Helicobacter pylori Strains in South-Western Poland. Front. Microbiol. 2018, 9, 3154. [Google Scholar] [CrossRef] [PubMed]
- Lind, T.; Veldhuyzen van Zanten, S.; Unge, P.; Spiller, R.; Bayerdorffer, E.; O’Morain, C.; Bardhan, K.D.; Bradette, M.; Chiba, N.; Wrangstadh, M.; et al. Eradication of Helicobacter pylori using one-week triple therapies combining omeprazole with two antimicrobials: The MACH I Study. Helicobacter 1996, 1, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Labenz, J.; Tillenburg, B.; Peitz, U.; Kohl, H.; Becker, T.; Stolte, M.; Borsch, G. Ulcer healing through the elimination of Helicobacter pylori: Is a week of therapy enough? Dtsch. Med. Wochenschr. 1996, 121, 3–7. [Google Scholar] [CrossRef]
- Misiewicz, J.J.; Harris, A.W.; Bardhan, K.D.; Levi, S.; O’Morain, C.; Cooper, B.T.; Kerr, G.D.; Dixon, M.F.; Langworthy, H.; Piper, D. One week triple therapy for Helicobacter pylori: A multicentre comparative study. Lansoprazole Helicobacter Study Group. Gut 1997, 41, 735–739. [Google Scholar] [CrossRef]
- Miyaji, H.; Azuma, T.; Ito, S.; Suto, H.; Ito, Y.; Yamazaki, Y.; Sato, F.; Hirai, M.; Kuriyama, M.; Kato, T.; et al. Susceptibility of Helicobacter pylori isolates to metronidazole, clarithromycin and amoxycillin in vitro and in clinical treatment in Japan. Aliment. Pharmacol. Ther. 1997, 11, 1131–1136. [Google Scholar] [CrossRef]
- Pieramico, O.; Zanetti, M.V.; Innerhofer, M.; Malfertheiner, P. Omeprazole-based dual and triple therapy for the treatment of Helicobacter pylori infection in peptic ulcer disease: A randomized trial. Helicobacter 1997, 2, 92–97. [Google Scholar] [CrossRef]
- Stack, W.A.; Knifton, A.; Thirlwell, D.; Cockayne, A.; Jenkins, D.; Hawkey, C.J.; Atherton, J.C. Safety and efficacy of rabeprazole in combination with four antibiotic regimens for the eradication of Helicobacter pylori in patients with chronic gastritis with or without peptic ulceration. Am. J. Gastroenterol. 1998, 93, 1909–1913. [Google Scholar] [CrossRef]
- Harris, A.W.; Misiewicz, J.J.; Bardhan, K.D.; Levi, S.; O’Morain, C.; Cooper, B.T.; Kerr, G.D.; Dixon, M.F.; Langworthy, H.; Piper, D. Incidence of duodenal ulcer healing after 1 week of proton pump inhibitor triple therapy for eradication of Helicobacter pylori. The Lansoprazole Helicobacter Study Group. Aliment. Pharmacol. Ther. 1998, 12, 741–745. [Google Scholar] [CrossRef]
- Pilotto, A.; Franceschi, M.; Leandro, G.; Bozzola, L.; Fortunato, A.; Rassu, M.; Meli, S.; Soffiati, G.; Scagnelli, M.; Di Mario, F.; et al. Efficacy of 7 day lansoprazole-based triple therapy for Helicobacter pylori infection in elderly patients. J. Gastroenterol. Hepatol. 1999, 14, 468–475. [Google Scholar] [CrossRef]
- Pilotto, A.; Leandro, G.; Franceschi, M.; Rassu, M.; Bozzola, L.; Furlan, F.; Di Mario, F.; Valerio, G. The effect of antibiotic resistance on the outcome of three 1-week triple therapies against Helicobacter pylori. Aliment. Pharmacol. Ther. 1999, 13, 667–673. [Google Scholar] [CrossRef]
- Savarino, V.; Zentilin, P.; Bisso, G.; Pivari, M.; Mele, M.R.; Mela, G.S.; Mansi, C.; Vigneri, S.; Termini, R.; Celle, G. Head-to-head comparison of 1-week triple regimens combining ranitidine or omeprazole with two antibiotics to eradicate Helicobacter pylori. Aliment. Pharmacol. Ther. 1999, 13, 643–649. [Google Scholar] [CrossRef]
- Uygun, A.; Ates, Y.; Erdil, A.; Kadayifci, A.; Cetin, C.; Gulsen, M.; Karaeren, N.; Dagalp, K. Efficacy of omeprazole plus two antimicrobials for the eradication of Helicobacter pylori in a Turkish population. Clin. Ther. 1999, 21, 1539–1548. [Google Scholar] [CrossRef]
- Huang, A.H.; Sheu, B.S.; Yang, H.B.; Huang, C.C.; Wu, J.J.; Lin, X.Z. Impact of Helicobacter pylori antimicrobial resistance on the outcome of 1-week lansoprazole-based triple therapy. J. Formos. Med. Assoc. 2000, 99, 704–709. [Google Scholar]
- Malfertheiner, P.; Kirchner, T.; Kist, M.; Leodolter, A.; Peitz, U.; Strobel, S.; Bohuschke, M.; Gatz, G. Helicobacter pylori eradication and gastric ulcer healing-comparison of three pantoprazole-based triple therapies. Aliment. Pharmacol. Ther. 2003, 17, 1125–1135. [Google Scholar] [CrossRef]
- Bhatia, V.; Ahuja, V.; Das, B.; Bal, C.; Sharma, M.P. Use of imidazole-based eradication regimens for Helicobacter pylori should be abandoned in North India regardless of in vitro antibiotic sensitivity. J. Gastroenterol. Hepatol. 2004, 19, 619–625. [Google Scholar] [CrossRef]
- Namiot, Z.; Namiot, D.B.; Kemona, A.; Stasiewicz, J. Effect of antibacterial therapy and salivary secretion on the efficacy of Helicobacter pylori eradication in duodenal ulcer patients. Oral Surg. Oral Med. Oral Pathol. 2004, 97, 714–717. [Google Scholar] [CrossRef]
- Sun, W.H.; Ou, X.L.; Cao, D.Z.; Yu, Q.; Yu, T.; Hu, J.M.; Zhu, F.; Sun, Y.L.; Fu, X.L.; Su, H. Efficacy of omeprazole and amoxicillin with either clarithromycin or metronidazole on eradication of Helicobacter pylori in Chinese peptic ulcer patients. World J. Gastroenterol. 2005, 11, 2477–2481. [Google Scholar] [CrossRef]
- Sancar, M.; Izzettin, F.V.; Apikoglu-Rabus, S.; Besisik, F.; Tozun, N.; Dulger, G. Pharmacoeconomic comparison of Helicobacter pylori eradication regimens. Pharm. World Sci. 2006, 28, 207–214. [Google Scholar] [CrossRef]
- Namiot, D.B.; Leszczynska, K.; Namiot, Z.; Kurylonek, A.J.; Kemona, A. Smoking and drinking habits are important predictors of Helicobacter pylori eradication. Adv. Med. Sci. 2008, 53, 310–315. [Google Scholar] [CrossRef]
- Filipec Kanizaj, T.; Katicic, M.; Skurla, B.; Ticak, M.; Plecko, V.; Kalenic, S. Helicobacter pylori eradication therapy success regarding different treatment period based on clarithromycin or metronidazole triple-therapy regimens. Helicobacter 2009, 14, 29–35. [Google Scholar] [CrossRef]
- Loghmari, H.; Bdioui, F.; Bouhlel, W.; Melki, W.; Hellara, O.; Ben Chaabane, N.; Safer, L.; Zakhama, A.; Saffar, H. Clarithromycin versus metronidazole in first-line Helicobacter pylori eradication. Prospective randomized study of 85 Tunisian adults. Tunis. Med. 2012, 90, 31–35. [Google Scholar]
- Lahbabi, M.; Alaoui, S.; El Rhazi, K.; El Abkari, M.; Nejjari, C.; Amarti, A.; Bennani, B.; Mahmoud, M.; Ibrahimi, A.; Benajah, D.A. Sequential therapy versus standard triple-drug therapy for Helicobacter pylori eradication: Result of the HPFEZ randomised study. Clin. Res. Hepatol. Gastroenterol. 2013, 37, 416–421. [Google Scholar] [CrossRef]
- Nishizawa, T.; Maekawa, T.; Watanabe, N.; Harada, N.; Hosoda, Y.; Yoshinaga, M.; Yoshio, T.; Ohta, H.; Inoue, S.; Toyokawa, T.; et al. Clarithromycin Versus Metronidazole as First-line Helicobacter pylori Eradication: A Multicenter, Prospective, Randomized Controlled Study in Japan. J. Clin. Gastroenterol. 2015, 49, 468–471. [Google Scholar] [CrossRef]
- Lee, H.J.; Kim, J.I.; Lee, J.S.; Jun, E.J.; Oh, J.H.; Cheung, D.Y.; Chung, W.C.; Kim, B.W.; Kim, S.S. Concomitant therapy achieved the best eradication rate for Helicobacter pylori among various treatment strategies. World J. Gastroenterol. 2015, 21, 351–359. [Google Scholar] [CrossRef]
- Gungor, G.; Baglicakoglu, M.; Kayacetin, E.; Biyik, M.; Ucar, R.; Goktepe, H.; Ataseven, H.; Demir, A. Current Status of Five Different Regimens for Empiric First-Line Helicobacter pylori Eradication in Turkey. Digestion 2015, 92, 55–59. [Google Scholar] [CrossRef]
- Graham, D.Y.; Dore, M.P. Helicobacter pylori therapy: A paradigm shift. Expert Rev. Anti-Infect. Ther. 2016, 14, 577–585. [Google Scholar] [CrossRef]
- Cosme, A.; Montes, M.; Martos, M.; Gil, I.; Mendarte, U.; Salicio, Y.; Pineiro, L.; Recasens, M.T.; Ibarra, B.; Sarasqueta, C.; et al. Usefulness of antimicrobial susceptibility in the eradication of Helicobacter pylori. Clin. Microbiol. Infect. 2013, 19, 379–383. [Google Scholar] [CrossRef]
- Megraud, F.; Benejat, L.; Ontsira Ngoyi, E.N.; Lehours, P. Molecular Approaches to Identify Helicobacter pylori Antimicrobial Resistance. Gastroenterol. Clin. N. Am. 2015, 44, 577–596. [Google Scholar] [CrossRef]
- Nakamura, A.; Furuta, T.; Shirai, N.; Sugimoto, M.; Kajimura, M.; Soya, Y.; Hishida, A. Determination of mutations of the 23S rRNA gene of Helicobacter pylori by allele specific primer-polymerase chain reaction method. J. Gastroenterol. Hepatol. 2007, 22, 1057–1063. [Google Scholar] [CrossRef]
- Kawai, T.; Yamagishi, T.; Yagi, K.; Kataoka, M.; Kawakami, K.; Sofuni, A.; Itoi, T.; Sakai, Y.; Moriyasu, F.; Osaka, Y.; et al. Tailored eradication therapy based on fecal Helicobacter pylori clarithromycin sensitivities. J. Gastroenterol. Hepatol. 2008, 23 (Suppl. 2), S171–S174. [Google Scholar] [CrossRef]
- Sugimoto, M.; Uotani, T.; Sahara, S.; Ichikawa, H.; Yamade, M.; Sugimoto, K.; Furuta, T. Efficacy of tailored Helicobacter pylori eradication treatment based on clarithromycin susceptibility and maintenance of acid secretion. Helicobacter 2014, 19, 312–318. [Google Scholar] [CrossRef]
- Kim, J.S.; Lee, K.S.; Kim, Y.I.; Tamai, Y.; Nakahata, R.; Takami, H. A randomized crossover comparative study of aspirin, cilostazol and clopidogrel in normal controls: Analysis with quantitative bleeding time and platelet aggregation test. J. Clin. Neurosci. 2004, 11, 600–602. [Google Scholar] [CrossRef]
- Morse, A.L.; Goodman, K.J.; Munday, R.; Chang, H.J.; Morse, J.W.; Keelan, M.; Geary, J.; Sander, V. A randomized controlled trial comparing sequential with triple therapy for Helicobacter pylori in an Aboriginal community in the Canadian North. Can. J. Gastroenterol. 2013, 27, 701–706. [Google Scholar] [CrossRef][Green Version]
- Otth, L.; Wilson, M.; Fernandez, H.; Otth, C.; Toledo, C.; Carcamo, V.; Rivera, P.; Ruiz, L. Isolation of Helicobacter pylori in gastric mucosa and susceptibility to five antimicrobial drugs in Southern chile. Braz. J. Microbiol. 2011, 42, 442–447. [Google Scholar] [CrossRef]
- Borody, T.J.; Cole, P.; Noonan, S.; Morgan, A.; Lenne, J.; Hyland, L.; Brandl, S.; Borody, E.G.; George, L.L. Recurrence of duodenal ulcer and Campylobacter pylori infection after eradication. Med. J. Aust. 1989, 151, 431–435. [Google Scholar] [CrossRef]
- Graham, D.Y.; Lee, S.Y. How to Effectively Use Bismuth Quadruple Therapy: The Good, the Bad, and the Ugly. Clin. Gastroenterol. 2015, 44, 537–563. [Google Scholar] [CrossRef]
- Gene, E.; Calvet, X.; Azagra, R.; Gisbert, J.P. Triple vs. quadruple therapy for treating Helicobacter pylori infection: A meta-analysis. Aliment. Pharmacol. Ther. 2003, 17, 1137–1143. [Google Scholar] [CrossRef]
- Luther, J.; Higgins, P.D.; Schoenfeld, P.S.; Moayyedi, P.; Vakil, N.; Chey, W.D. Empiric quadruple vs. triple therapy for primary treatment of Helicobacter pylori infection: Systematic review and meta-analysis of efficacy and tolerability. Am. J. Gastroenterol. 2010, 105, 65–73. [Google Scholar] [CrossRef]
- Venerito, M.; Krieger, T.; Ecker, T.; Leandro, G.; Malfertheiner, P. Meta-analysis of bismuth quadruple therapy versus clarithromycin triple therapy for empiric primary treatment of Helicobacter pylori infection. Digestion 2013, 88, 33–45. [Google Scholar] [CrossRef]
- Martin-Bouyer, G.; Foulon, G.; Guerbois, H.; Barin, C. Epidemiological study of encephalopathies following bismuth administration per os. Characteristics of intoxicated subjects: Comparison with a control group. Clin. Toxicol. 1981, 18, 1277–1283. [Google Scholar] [CrossRef]
- Graham, D.Y.; Lee, Y.C.; Wu, M.S. Rational Helicobacter pylori therapy: Evidence-based medicine rather than medicine-based evidence. Clin. Gastroenterol. Hepatol. 2014, 12, 177–186. [Google Scholar] [CrossRef]
- Chen, M.J.; Chen, C.C.; Chen, Y.N.; Chen, C.C.; Fang, Y.J.; Lin, J.T.; Wu, M.S.; Liou, J.M. Systematic Review with Meta-Analysis: Concomitant Therapy vs. Triple Therapy for the First-Line Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2018, 113, 1444–1457. [Google Scholar] [CrossRef]
- Molina-Infante, J.; Romano, M.; Fernandez-Bermejo, M.; Federico, A.; Gravina, A.G.; Pozzati, L.; Garcia-Abadia, E.; Vinagre-Rodriguez, G.; Martinez-Alcala, C.; Hernandez-Alonso, M.; et al. Optimized nonbismuth quadruple therapies cure most patients with Helicobacter pylori infection in populations with high rates of antibiotic resistance. Gastroenterology 2013, 145, 121–128. [Google Scholar] [CrossRef]
- Liou, J.M.; Fang, Y.J.; Chen, C.C.; Bair, M.J.; Chang, C.Y.; Lee, Y.C.; Chen, M.J.; Chen, C.C.; Tseng, C.H.; Hsu, Y.C.; et al. Concomitant, bismuth quadruple, and 14-day triple therapy in the first-line treatment of Helicobacter pylori: A multicentre, open-label, randomised trial. Lancet 2016, 388, 2355–2365. [Google Scholar] [CrossRef]
- Labenz, J.; Stolte, M.; Blum, A.L.; Jorias, I.; Leverkus, F.; Sollbohmer, M.; Bertrams, J.; Borsch, G. Intragastric acidity as a predictor of the success of Helicobacter pylori eradication: A study in peptic ulcer patients with omeprazole and amoxicillin. Gut 1995, 37, 39–43. [Google Scholar] [CrossRef]
- Sugimoto, M.; Furuta, T.; Shirai, N.; Kodaira, C.; Nishino, M.; Ikuma, M.; Ishizaki, T.; Hishida, A. Evidence that the degree and duration of acid suppression are related to Helicobacter pylori eradication by triple therapy. Helicobacter 2007, 12, 317–323. [Google Scholar] [CrossRef]
- Yang, J.C.; Wang, H.L.; Chern, H.D.; Shun, C.T.; Lin, B.R.; Lin, C.J.; Wang, T.H. Role of omeprazole dosage and cytochrome P450 2C19 genotype in patients receiving omeprazole-amoxicillin dual therapy for Helicobacter pylori eradication. Pharmacotherapy 2011, 31, 227–238. [Google Scholar] [CrossRef]
- Parsons, M.E.; Keeling, D.J. Novel approaches to the pharmacological blockade of gastric acid secretion. Expert Opin. Investig. Drugs 2005, 14, 411–421. [Google Scholar] [CrossRef]
- Jenkins, H.; Sakurai, Y.; Nishimura, A.; Okamoto, H.; Hibberd, M.; Jenkins, R.; Yoneyama, T.; Ashida, K.; Ogama, Y.; Warrington, S. Randomised clinical trial: Safety, tolerability, pharmacokinetics and pharmacodynamics of repeated doses of TAK-438 (vonoprazan), a novel potassium-competitive acid blocker, in healthy male subjects. Aliment. Pharmacol. Ther. 2015, 41, 636–648. [Google Scholar] [CrossRef]
- Kagami, T.; Sahara, S.; Ichikawa, H.; Uotani, T.; Yamade, M.; Sugimoto, M.; Hamaya, Y.; Iwaizumi, M.; Osawa, S.; Sugimoto, K.; et al. Potent acid inhibition by vonoprazan in comparison with esomeprazole, with reference to CYP2C19 genotype. Aliment. Pharmacol. Ther. 2016, 43, 1048–1059. [Google Scholar] [CrossRef]
- Murakami, K.; Sakurai, Y.; Shiino, M.; Funao, N.; Nishimura, A.; Asaka, M. Vonoprazan, a novel potassium-competitive acid blocker, as a component of first-line and second-line triple therapy for Helicobacter pylori eradication: A phase III, randomised, double-blind study. Gut 2016, 65, 1439–1446. [Google Scholar] [CrossRef]
- Maruyama, M.; Tanaka, N.; Kubota, D.; Miyajima, M.; Kimura, T.; Tokutake, K.; Imai, R.; Fujisawa, T.; Mori, H.; Matsuda, Y.; et al. Vonoprazan-Based Regimen Is More Useful than PPI-Based One as a First-Line Helicobacter pylori Eradication: A Randomized Controlled Trial. Can. J. Gastroenterol. Hepatol. 2017, 2017, 4385161. [Google Scholar] [CrossRef]
- Sue, S.; Ogushi, M.; Arima, I.; Kuwashima, H.; Nakao, S.; Naito, M.; Komatsu, K.; Kaneko, H.; Tamura, T.; Sasaki, T.; et al. Vonoprazan-vs proton-pump inhibitor-based first-line 7-day triple therapy for clarithromycin-susceptible Helicobacter pylori: A multicenter, prospective, randomized trial. Helicobacter 2018, 23, e12456. [Google Scholar] [CrossRef]
- Jung, Y.S.; Kim, E.H.; Park, C.H. Systematic review with meta-analysis: The efficacy of vonoprazan-based triple therapy on Helicobacter pylori eradication. Aliment. Pharmacol. Ther. 2017, 46, 106–114. [Google Scholar] [CrossRef]
- Li, M.; Oshima, T.; Horikawa, T.; Tozawa, K.; Tomita, T.; Fukui, H.; Watari, J.; Miwa, H. Systematic review with meta-analysis: Vonoprazan, a potent acid blocker, is superior to proton-pump inhibitors for eradication of clarithromycin-resistant strains of Helicobacter pylori. Helicobacter 2018, 23, e12495. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Year | Country | Patient Number | Age (mean) | Sex (M/F) | Regimen of PAC Therapy (Dosing Dose a Day) | Duration | Eradication Rate of PAC (ITT/PP) | Regimen of PAM Therapy (Dosing Dose a Day) | Duration | Eradication Rate of PAM (ITT/PP) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Labenz et al. [28] | 1996 | Germany | 64 | NA | NA | OPZ (20), AMPC (1000), CAM (500) | 7 days | 96.8%/96.8% | OPZ (20), AMPC (1000), MNZ (500) | 7 days | 84.8%/84.8% |
| Lind et al. [27] | 1996 | Multiple | 391 | NA | NA | OPZ (20), AMPC (1000), CAM (500) | 7 days | 85.0%/91.4% | OPZ (20), AMPC (1000), MNZ (400) | 7 days | 75.8%/81.6% |
| Misiewicz et al. [29] | 1997 | UK | 252 | 48 | 176/76 | LPZ (30), AMPC (1000), CAM (250) | 7 days | 86.0%/90.4% | LPZ (30), AMPC (1000), MNZ (400)* | 7 days | 66.4%/73.5% |
| Miyaji et al. [30] | 1997 | Japan | 144 | 52 | NA | PPIs AMPC (500), CAM (200) | 7 days | 79.7%/79.7% | PPIs AMPC (500), MNZ (250) | 7 days | 85.7%/85.7% |
| Pieramico et al. [31] | 1997 | Italy | 119 | 53 | 61/58 | OPZ (20), AMPC (1000), CAM (500) | 7 days | 86.2%/92.6% | OPZ (20), AMPC (1000), MNZ (500) | 7 days | 80.3%/86.0% |
| Stack et al. [32] | 1997 | UK | 38 | 52 | 28/10 | RPZ (20), AMPC (1000), CAM (500) | 7 days | 94.7%/100.0% | RPZ (20), AMPC (1000), MNZ (400) | 7 days | 89.5%/88.2% |
| Harris et al. [33] | 1998 | UK | 126 | 47 | 88/38 | PPIs AMPC (1000), CAM (250) | 7 days | 85.5%/89.8% | PPIs AMPC (500), MNZ (400) | 7 days | 64.1%/76.0% |
| Pilotto et al. [34] | 1999 | Italy | 100 | 77 | 43/57 | LPZ (30), AMPC (1000), CAM (250) | 7 days | 82.0%/89.1% | LPZ (30), AMPC (1000), MNZ (250) | 7 days | 80.0%/87.0% |
| Pilotto et al. [35] | 1999 | Italy | 78 | 71 | 28/50 | PAN (40), AMPC (1000), CAM (250) | 7 days | 85.0%/85.0% | PAN (40), AMPC (1000), MNZ (250) | 7 days | 78.9%/85.7% |
| Savarino et al. [36] | 1999 | Italy | 160 | 49 | 86/74 | OPZ (20), AMPC (1000), CAM (250) | 7 days | 57.5%/66.7% | OPZ (20), AMPC (1000), MNZ (500) | 7 days | 77.5%/88.6% |
| Uygun et al. [37] | 1999 | Turkey | 222 | 39 | 119/103 | OPZ (20), AMPC (1000), CAM (500) | 7 days | 60.2%/67.1% | OPZ (20), AMPC (1000), MNZ (500)/TNZ (500) | 7 days | 57.5%/63.6% |
| Huang et al. [38] | 2000 | Taiwan | 67 | 42 | 37/30 | LPZ (30), AMPC (1000), CAM (500) | 7 days | 89.2%/94.3% | LPZ (30), AMPC (1000), MNZ (500) | 7 days | 70.0%/77.8% |
| Malfertheiner et al. [39] | 2003 | Germany | 336 | 57 | 184/152 | PAN (40), AMPC (1000), CAM (500) | 7 days | 66.9%/89.0% | PA (40), AMPC (1000), MNZ (500) | 7 days | 59.9%/75.8% |
| Bhatia et al. [40] | 2004 | India | 146 | 39 | 113/33 | LPZ (30), AMPC (1000), CAM (500) | 14 days | 46.1%/64.8% | LPZ (30), AMPC (1000), TNZ (500) | 14 days | 31.4%/42.3% |
| Namiot et al. [41] | 2004 | Poland | 90 | 42 | 68/22 | OPZ (20), AMPC (1000), CAM (250) | 7 days | 68.9%/81.6% | OPZ( 20), AMPC (1000), TNZ (500) | 7 days | 68.9%/77.5% |
| Koivisto et al. [23] | 2005 | Finland | 216 | 56 | 103/113 | LPZ (30), AMPC (1000), CAM (500) | 7 days | 90.9%/90.9% | LPZ (30), AMPC (1000), MNZ (400)* | 7 days | 78.3%/78.3% |
| Sun et al. [42] | 2005 | China | 103 | 51 | 85/18 | OPZ (20), AMPC (1000), CAM (500) | 7 days | 86.2%/89.3% | OPZ (20), AMPC (1000), MNZ (500) | 7 days | 82.2%/84.1% |
| Sancar et al. [43] | 2006 | Turkey | 35 | 43 | 18/17 | LPZ (30)/OPZ (20), AMPC (1000), CAM (500) | 7, 14 days | 83.3%/83.3% | LPZ (30)/OPZ (20), AMPC (1000), MNZ (500) | 7, 14 days | 50.0%/50.0% |
| Namiot et al. [44] | 2008 | Poland | 159 | 50 | 106/53 | OPZ( 20), AMPC (1000), CAM (250) | 7 days | 77.4%/80.2% | OPZ (20), AMPC (1000), MNZ (250) | 7 days | 63.4%/66.7% |
| Filipec et al. [45] | 2009 | Croatia | 592 | 52 | 335/257 | PAN (40), AMPC (1000), CAM (500) | 7, 10, 14 days | 83.1%/88.1% | PAN (40), AMPC (1000), MNZ (500) | 7, 10, 14 days | 79.8%/84.0% |
| Loghmari et al. [46] | 2012 | Tunisia | 85 | 40 | 44/41 | OPZ (20), AMPC (1000), CAM (500) | 7 days | 69.6%/69.6% | OPZ (20), AMPC (1000), MNZ (500) | 7 days | 48.7%/48.7% |
| Lahbabi et al. [47] | 2013 | Morocco | 219 | 47 | 105/114 | PPIs AMPC (1000), CAM (500) | 7 days | 78.3%/79.6% | PPIs AMPC (1000), MNZ (500) | 7 days | 70.2%/70.9% |
| Nishizawa et al. [48] | 2015 | Japan | 219 | 47 | 105/114 | PAN (40), AMPC (1000), CAM (500) | 14 days | 42.0%/48.3% | PAN (40), AMPC (1000), MNZ (500) | 14 days | 52.0%/54.2% |
| Lee et al. [49] | 2015 | Korea | 340 | 57 | 209/131 | RPZ (20), AMPC (1000), CAM (500) | 7 days | 64.1%/76.2% | RPZ (20), AMPC (1000), MNZ (750) | 7 days | 68.8%/84.2% |
| Gungor et al. [50] | 2015 | Turkey | 124 | 61 | 51/73 | RPZ (10), AMPC (750), CAM (400) | 7 days | 73.3%/77.2% | RPZ (10), AMPC (750), MNZ (250) | 7 days | 90.6%/93.5% |
| Adachi et al. [17] | 2017 | Japan | 140 | 64 | 68/72 | EPZ (20), AMPC (750), CAM (400) | 7 days | 70.6%/72.7% | EPZ (20), AMPC (750), MNZ (500) | 7 days | 91.7%/94.3% |
| Mabe et al. [18] | 2018 | Japan | 306 | 26 | 157/149 | LPZ (30), AMPC (750), CAM (200) | 7 days | 65.0%/65.7% | LPZ (30), AMPC (750), MNZ (250) | 7 days | 96.4%/96.9% |
| Authors | PAC | PAM | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Events | Diarrhea | Skin Rash | Dysgeusia | Nausea | N | Events | Diarrhea | Skin Rash | Dysgeusia | Nausea | |
| Lind et al. [27] | 234 | NA | 29 | NA | 18 | 2 | 124 | NA | 24 | NA | 11 | 2 |
| Misiewicz et al. [29] | 121 | 51.2% | 22 | NA | 2 | NA | 131 | 57.3% | 19 | NA | 13 | NA |
| Pieramico et al. [31] | 58 | 10.3% | 2 | 0 | 1 | 0 | 61 | 8.2% | 1 | 0 | 0 | 1 |
| Stack et al. [32] | 19 | NA | 9 | NA | 8 | NA | 19 | NA | 11 | NA | 3 | NA |
| Harris et al. [33] | 62 | 0.0% | 0 | 0 | 0 | 0 | 64 | 0.0% | 0 | 0 | 0 | 0 |
| Pilotto et al. [34] | 50 | 14.0% | NA | NA | NA | NA | 50 | 10.0% | NA | NA | NA | NA |
| Pilotto et al. [35] | 40 | 10.0% | NA | NA | NA | NA | 38 | 5.3% | NA | NA | NA | NA |
| Savarino et al. [36] | 80 | 17.5% | 3 | 1 | 4 | 3 | 80 | 15.0% | 1 | 2 | 2 | 3 |
| Uygun et al. [37] | 79 | 11.4% | 3 | 0 | 5 | 0 | 121 | 9.1% | 1 | 2 | 0 | 7 |
| Huang et al. [38] | 37 | 27.0% | 3 | 0 | 1 | 3 | 30 | 43.3% | 2 | 0 | 4 | 3 |
| Bhatia et al. [40] | 76 | 9.2% | NA | NA | NA | NA | 70 | 21.4% | NA | NA | NA | NA |
| Koivisto et al. [23] | 110 | 11.8% | NA | NA | NA | NA | 106 | 9.4% | NA | NA | NA | NA |
| Sun et al. [42] | 58 | 10.3% | 1 | 1 | 0 | 1 | 45 | 11.1% | 1 | 1 | 2 | 1 |
| Filipec et al. [45] | 295 | NA | 13 | NA | 15 | 12 | 297 | NA | 11 | NA | 22 | 26 |
| Lahbabi et al. [47] | 115 | 27.8% | 11 | 1 | 11 | NA | 104 | 22.1% | 9 | 1 | 6 | NA |
| Nishizawa et al. [48] | 100 | 16.0% | 11 | 1 | 7 | 0 | 100 | 8.0% | 9 | 1 | 6 | 0 |
| Lee et al. [49] | 170 | 50.6% | 24 | 0 | 28 | 12 | 170 | 54.7% | 2 | 0 | 10 | 32 |
| Gungor et al. [50] | 58 | 22.4% | 5 | 5 | 1 | 2 | 63 | 17.5% | 6 | 3 | 0 | 0 |
| Mabe et al. [18] | 137 | 16.8% | 8 | 4 | 4 | 2 | 169 | 17.2% | 12 | 4 | 4 | 3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murata, M.; Sugimoto, M.; Mizuno, H.; Kanno, T.; Satoh, K. Clarithromycin Versus Metronidazole in First-Line Helicobacter Pylori Triple Eradication Therapy Based on Resistance to Antimicrobial Agents: Meta-Analysis. J. Clin. Med. 2020, 9, 543. https://doi.org/10.3390/jcm9020543
Murata M, Sugimoto M, Mizuno H, Kanno T, Satoh K. Clarithromycin Versus Metronidazole in First-Line Helicobacter Pylori Triple Eradication Therapy Based on Resistance to Antimicrobial Agents: Meta-Analysis. Journal of Clinical Medicine. 2020; 9(2):543. https://doi.org/10.3390/jcm9020543
Chicago/Turabian StyleMurata, Masaki, Mitsushige Sugimoto, Hitomi Mizuno, Takeshi Kanno, and Kiichi Satoh. 2020. "Clarithromycin Versus Metronidazole in First-Line Helicobacter Pylori Triple Eradication Therapy Based on Resistance to Antimicrobial Agents: Meta-Analysis" Journal of Clinical Medicine 9, no. 2: 543. https://doi.org/10.3390/jcm9020543
APA StyleMurata, M., Sugimoto, M., Mizuno, H., Kanno, T., & Satoh, K. (2020). Clarithromycin Versus Metronidazole in First-Line Helicobacter Pylori Triple Eradication Therapy Based on Resistance to Antimicrobial Agents: Meta-Analysis. Journal of Clinical Medicine, 9(2), 543. https://doi.org/10.3390/jcm9020543