Title: Human Serum/Plasma Glycoprotein Analysis by 1H-NMR, an Emerging Method of Inflammatory Assessment

Abstract

1. Background
2. Glycoproteins: A Biochemical Approach
3. Clinical Importance of Glycoproteins
4. Measurement Techniques for Glycoprotein Determination
4.1. Traditionally Used Techniques to Measure Glycated Proteins
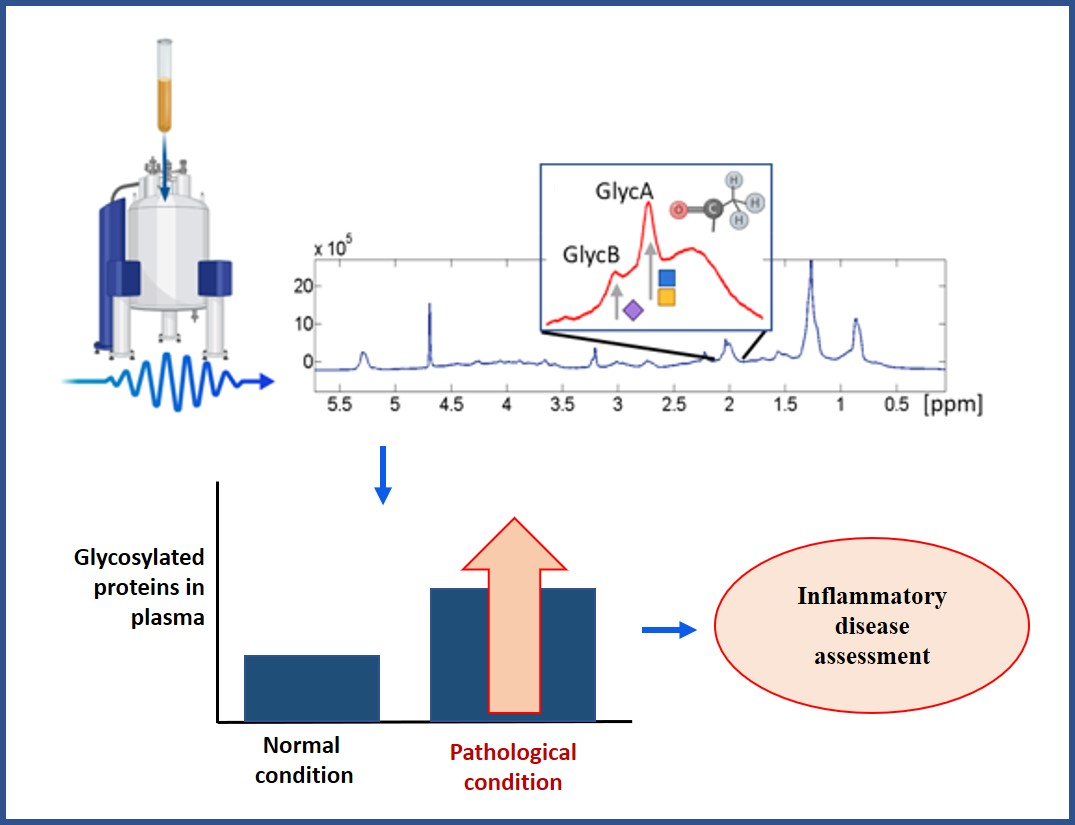
4.2. Serum/Plasma NMR Glycoprotein Analysis
4.2.1. Sample Handling and Preparation
4.2.2. Sample Storage
4.2.3. Processing of NMR Spectra for Glycoprotein Profiling
5. 1H-NMR Glycoprotein Clinical Studies
5.1. Former Studies on 1H-NMR Detection and Identification of Glycoproteins
5.2. Clinical Applications
5.2.1. Diseases
Tumors and Cancer
Metabolic Disorders
Obesity
Diabetes Mellitus
Metabolic Syndrome (MetS)
CVD Risk and All-Cause Mortality Prediction
Apparently Healthy Populations
Prediction of CVD in High-Risk Populations
Life Expectancy Prediction and All-Cause Mortality
Human Immunodeficiency Virus (HIV)-Infection
Chronic Inflammatory Diseases Related to the Immune System
Rheumatoid Arthritis (RA)
Systemic Lupus Erythematosus (SLE)
Psoriasis
Inflammatory Bowel Disease (IBD)
Other Chronic Inflammatory Diseases
Cognitive Function and Psychological Health
5.2.2. Rare Vascular Diseases
Takayasu Arteritis (TA)
Kawasaki Disease
Primary Aldosteronism (PA)
Sickle Cell Disease (SCD)
Human African Trypanosomiasis (HAT)
5.2.3. Treatment Effects and Lifestyle
Tobacco Smoking
Effect of Exercise
Effect of Treatments
Modulators of Inflammatory and Immune Response
Statins
Metformin
Probiotics
5.2.4. Other Conditions
Sodium Intake
Pregnancy
Toxicity
6. Conclusions
6.1. 1H-NMR Glycoproteins as a Diagnostic Tool
6.2. 1H-NMR Glycoproteins as a Therapeutic Tool
6.3. Future Perspectives
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gabay, C.; Kushner, I. Acute-Phase Proteins and Other Systemic Responses to Inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef]
- Bergin, D.A.; Reeves, E.P.; Meleady, P.; Henry, M.; McElvaney, O.J.; Carroll, T.P.; Condron, C.; Chotirmall, S.H.; Clynes, M.; O’Neill, S.J.; et al. α-1 Antitrypsin regulates human neutrophil chemotaxis induced by soluble immune complexes and IL-8. J. Clin. Investig. 2010, 120, 4236–4250. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, C.; Saldova, R.; Wormald, M.R.; Rudd, P.M.; McElvaney, N.G.; Reeves, E.P. The Role and Importance of Glycosylation of Acute Phase Proteins with Focus on Alpha-1 Antitrypsin in Acute and Chronic Inflammatory Conditions. J. Proteome Res. 2014, 13, 3131–3143. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Shang, S.; Li, W.; Qin, X.; Liu, Y. Insights on N-glycosylation of human haptoglobin and its association with cancers. Glycobiology 2016, 26, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Pezer, M.; Rudan, I.; Campbell, H. Mechanisms of disease: The human N-glycome. Biochim. Biophys. Acta—Gen. Subj. 2016, 1860, 1574–1582. [Google Scholar]
- Silva, M.L.S. Cancer serum biomarkers based on aberrant post-translational modifications of glycoproteins: Clinical value and discovery strategies. Biochim. Biophys. Acta—Rev. Cancer 2015, 1856, 165–177. [Google Scholar] [CrossRef]
- Mallol, R.; Rodriguez, M.A.; Brezmes, J.; Masana, L.; Correig, X. Human serum/plasma lipoprotein analysis by NMR: Application to the study of diabetic dyslipidemia. Prog. Nucl. Magn. Reson. Spectrosc. 2013, 70, 1–24. [Google Scholar] [CrossRef]
- Soininen, P.; Kangas, A.J.; Würtz, P.; Suna, T.; Ala-Korpela, M. Quantitative Serum Nuclear Magnetic Resonance Metabolomics in Cardiovascular Epidemiology and Genetics. Circ. Cardiovasc. Genet. 2015, 8, 192–206. [Google Scholar] [CrossRef]
- Seo, J.; Lee, K.-J. Post-translational Modifications and Their Biological Functions: Proteomic Analysis and Systematic Approaches. J. Biochem. Mol. Biol. 2004, 37, 35–44. [Google Scholar] [CrossRef]
- Lodish, H.; Berk, A.; Zipursky, S.L.; Matsudaira, P.; Baltimore, D.; Darnell, J. Glycosylation in the ER and Golgi Complex. In Molecular Cell Biology, 4th ed.; WH Freeman: New York, NY, USA, 2000. [Google Scholar]
- Colley, K.J.; Varki, A.; Kinoshita, T. Cellular Organization of Glycosylation; Cold Spring Harbor Laboratory Press: Cold Spring Harbor, NY, USA, 2015. [Google Scholar]
- Unverzagt, C.; Kajihara, Y. Recent advances in the chemical synthesis of N-linked glycoproteins. Curr. Opin. Chem. Biol. 2018, 46, 130–137. [Google Scholar]
- Ohtsubo, K.; Jamey, D. Marth Glycosylation in Cellular Mechanisms of Health and Disease. Cell 2006, 126, 855–867. [Google Scholar] [CrossRef] [PubMed]
- Lodish, H.; Berk, A.; Zipursky, S.L.; Matsudaira, P.; Baltimore, D.; Darnell, J. Protein Glycosylation in the ER and Golgi Complex, 4th ed.; WH Freeman: New York, NY, USA, 2000. [Google Scholar]
- Vanhooren, V.; Laroy, W.; Libert, C.; Chen, C. N-Glycan profiling in the study of human aging. Biogerontology 2008, 9, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Lakshminarayanan, A.; Richard, M.; Davis, B.G. Studying Glycobiology at the Single-Molecule Level. Nat. Rev. Chem. 2018, 2, 148–159. [Google Scholar] [CrossRef]
- Lyons, J.J.; Milner, J.D.; Rosenzweig, S.D. Glycans Instructing Immunity: The Emerging Role of Altered Glycosylation in Clinical Immunology. Front. Pediatr. 2015, 3, 54. [Google Scholar] [CrossRef] [PubMed]
- Fournier, T.; Medjoubi-N, N.; Porquet, D. Alpha-1-acid glycoprotein. Biochim. Biophys. Acta 2000, 1482, 157–171. [Google Scholar] [CrossRef]
- Dall’Olio, F.; Vanhooren, V.; Chen, C.C.; Slagboom, P.E.; Wuhrer, M.; Franceschi, C. N-glycomic biomarkers of biological aging and longevity: A link with inflammaging. Ageing Res. Rev. 2013, 12, 685–698. [Google Scholar] [CrossRef]
- Pinho, S.S.; Reis, C.A. Glycosylation in cancer: Mechanisms and clinical implications. Nat. Rev. Cancer 2015, 15, 540–555. [Google Scholar] [CrossRef]
- Taniguchi, N.; Korekane, H. Branched N-glycans and their implications for cell adhesion, signaling and clinical applications for cancer biomarkers and in therapeutics. BMB Rep. 2011, 44, 772–781. [Google Scholar] [CrossRef]
- Lefebvre, T.; Dehennaut, V.; Guinez, C.; Olivier, S.; Drougat, L.; Mir, A.-M.; Mortuaire, M.; Vercoutter-Edouart, A.-S.; Michalski, J.-C. Dysregulation of the nutrient/stress sensor O-GlcNAcylation is involved in the etiology of cardiovascular disorders, type-2 diabetes and Alzheimer’s disease. Biochim. Biophys. Acta—Gen. Subj. 2010, 1800, 67–79. [Google Scholar] [CrossRef]
- Myslicki, J.P.; Shearer, J.; Hittel, D.S.; Hughey, C.C.; Belke, D.D. O-GlcNAc modification is associated with insulin sensitivity in the whole blood of healthy young adult males. Diabetol. Metab. Syndr. 2014, 6, 96. [Google Scholar] [CrossRef]
- Bell, J.D.; Brown, J.C.C.; Nicholson, J.K.; Sadler, P.J. Assignment of resonances for ‘acute-phase’ glycoproteins in high resolution proton NMR spectra of human blood plasma. FEBS Lett. 1987, 215, 311–315. [Google Scholar] [CrossRef]
- Lipton, A.; Harvey, H.A.; Delong, S.; Allegra, J.; White, D.; Allegra, M.; Davidson, E.A. Glycoproteins and human cancer:1. Circulating levels in cancer serum. Cancer 1979, 43, 1766–1771. [Google Scholar] [CrossRef]
- Silverman, L.M.; Dermer, G.B.; Tökes, Z.A. Electrophoretic patterns for serum glycoproteins reflect the presence of human breast cancer. Clin. Chem. 1977, 23, 2055–2058. [Google Scholar] [CrossRef]
- Hakomori, S.-I. Aberrant Glycosylation in Cancer Cell Membranes as Focused on Glycolipids: Overview and Perspectives1 Introduction: Glycosylation as a Modulatory Mechanism of Cellular Function and Cell-Social Interaction. Cancer Res. 1985, 45, 2405–2414. [Google Scholar] [PubMed]
- Patel, P.S.; Adhvaryu, S.G.; Balar, D.B. Serum Glycoconjugates in Patients with Anemia and Myeloid Leukemia. Tumori J. 1988, 74, 639–644. [Google Scholar] [CrossRef]
- Rye, P.D.; Walker, R.A. Analysis of glycoproteins released from benign and malignant human breast: Changes in size and fucosylation with malignancy. Eur. J. Cancer Clin. Oncol. 1989, 25, 65–72. [Google Scholar] [CrossRef]
- Moremen, K.W.; Tiemeyer, M.; Nairn, A.V. Vertebrate protein glycosylation: Diversity, synthesis and function. Nat. Rev. Mol. Cell Biol. 2012, 13, 448–462. [Google Scholar] [CrossRef]
- Austrup, F.; Vestweber, D.; Borges, E.; Löhning, M.; Bräuer, R.; Herz, U.; Renz, H.; Hallmann, R.; Scheffold, A.; Radbruch, A.; et al. P- and E-selectin mediate recruitment of T-helper-1 but not T-helper-2 cells into inflamed tissues. Nature 1997, 385, 81–83. [Google Scholar] [CrossRef]
- Bedard, P.W.; Kaila, N. Selectin inhibitors: A patent review. Expert Opin. Ther. Pat. 2010, 20, 781–793. [Google Scholar] [CrossRef]
- Chatterjee, B.P.; Mondal, G.; Chatterjee, U. Glycosylation of Acute Phase Proteins: A Promising Disease Biomarker. Proc. Natl. Acad. Sci. India Sect. B Biol. Sci. 2014, 84, 865–874. [Google Scholar] [CrossRef]
- Baumann, H.; Gauldie, J. The acute phase response. Immunol. Today 1994, 15, 74–80. [Google Scholar] [CrossRef]
- Biou, D.; Konan, D.; Féger, J.; Agneray, J.; Leroy, Y.; Cardon, P.; Fournet, B.; Durand, G. Alterations in the carbohydrate moiety of alpha-1-acid glycoprotein purified from human cirrhotic ascitic fluid. Biochim. Biophys. Acta 1987, 913, 308–312. [Google Scholar] [CrossRef]
- Van Dijk, W.; Koeleman, C.; Van het Hof, B.; Poland, D.; Jakobs, C.; Jaeken, J. Increased alpha3-fucosylation of alpha(1)-acid glycoprotein in patients with congenital disorder of glycosylation type IA (CDG-Ia). FEBS Lett. 2001, 494, 232–235. [Google Scholar] [CrossRef]
- Mackiewicz, A.; Mackiewicz, K. Glycoforms of serum alpha 1-acid glycoprotein as markers of inflammation and cancer. Glycoconj. J. 1995, 12, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Serbource-Goguel, N.; Corbic, M.; Erlinger, S.; Durand, G.; Agneray, J.; Feger, J. Measurement of serum alpha 1-acid glycoprotein and alpha 1-antitrypsin desialylation in liver disease. Hepatology 1982, 3, 356–359. [Google Scholar] [CrossRef]
- Mondal, G.; Chatterjee, U.; Das, H.R.; Chatterjee, B.P. Enhanced expression of α1-acid glycoprotein and fucosylation in hepatitis B patients provides an insight into pathogenesis. Glycoconj. J. 2009, 26, 1225–1234. [Google Scholar] [CrossRef]
- Ishibashi, K.; Nishikawa, A.; Hayashi, N.; Kasahara, A.; Sato, N.; Fujii, S.; Kamada, T.; Taniguchi, N. N-acetylglucosaminyltransferase III in human serum, and liver and hepatoma tissues: Increased activity in liver cirrhosis and hepatoma patients. Clin. Chim. Acta 1989, 185, 325–332. [Google Scholar] [CrossRef]
- Miyoshi, E.; Noda, K.; Yamaguchi, Y.; Inoue, S.; Ikeda, Y.; Wang, W.; Ko, J.H.; Uozumi, N.; Li, W.; Taniguchi, N. The alpha1-6-fucosyltransferase gene and its biological significance. Biochim. Biophys. Acta 1999, 1473, 9–20. [Google Scholar] [CrossRef]
- Mondal, G.; Chatterjee, U.; Chawla, Y.K.; Chatterjee, B.P. Alterations of glycan branching and differential expression of sialic acid on alpha fetoprotein among hepatitis patients. Glycoconj. J. 2011, 28, 1–9. [Google Scholar] [CrossRef]
- Comunale, M.A.; Rodemich-Betesh, L.; Hafner, J.; Wang, M.; Norton, P.; Di Bisceglie, A.M.; Block, T.; Mehta, A. Linkage Specific Fucosylation of Alpha-1-Antitrypsin in Liver Cirrhosis and Cancer Patients: Implications for a Biomarker of Hepatocellular Carcinoma. PLoS ONE 2010, 5, e12419. [Google Scholar] [CrossRef]
- Lee, H.B.; Yoo, O.J.; Ham, J.S.; Lee, M.H. Serum alpha 1-antitrypsin in patients with hepatocellular carcinoma. Clin. Chim. Acta 1992, 206, 225–230. [Google Scholar] [CrossRef]
- Goodarzi, M.T.; Turner, G.A. Decreased branching, increased fucosylation and changed sialylation of alpha-1-proteinase inhibitor in breast and ovarian cancer. Clin. Chim. Acta 1995, 236, 161–171. [Google Scholar] [CrossRef]
- Vaughan, L.; Lorier, M.A.; Carrell, R.W. alpha 1-Antitrypsin microheterogeneity. Isolation and physiological significance of isoforms. Biochim. Biophys. Acta 1982, 701, 339–345. [Google Scholar] [CrossRef]
- Hrycaj, P.; Sobieska, M.; Mackiewicz, S.; Müller, W. Microheterogeneity of alpha 1 acid glycoprotein in rheumatoid arthritis: Dependent on disease duration? Ann. Rheum. Dis. 1993, 52, 138–141. [Google Scholar] [CrossRef]
- Yamashita, K.; Koide, N.; Endo, T.; Iwaki, Y.; Kobata, A. Altered glycosylation of serum transferrin of patients with hepatocellular carcinoma. J. Biol. Chem. 1989, 264, 2415–2423. [Google Scholar]
- Matsumoto, K.; Maeda, Y.; Kato, S.; Yuki, H. Alteration of asparagine-linked glycosylation in serum transferrin of patients with hepatocellular carcinoma. Clin. Chim. Acta 1994, 224, 1–8. [Google Scholar] [CrossRef]
- Vanarsa, K.; Ye, Y.; Han, J.; Xie, C.; Mohan, C.; Wu, T. Inflammation associated anemia and ferritin as disease markers in systemic lupus erythematosus. Arthritis Res. Ther. 2012, 14, R182. [Google Scholar] [CrossRef]
- Mann, A.C.; Record, C.O.; Self, C.H.; Turner, G.A. Monosaccharide composition of haptoglobin in liver diseases and alcohol abuse: Large changes in glycosylation associated with alcoholic liver disease. Clin. Chim. Acta 1994, 227, 69–78. [Google Scholar] [CrossRef]
- Okuyama, N.; Ide, Y.; Nakano, M.; Nakagawa, T.; Yamanaka, K.; Moriwaki, K.; Murata, K.; Ohigashi, H.; Yokoyama, S.; Eguchi, H.; et al. Fucosylated haptoglobin is a novel marker for pancreatic cancer: A detailed analysis of the oligosaccharide structure and a possible mechanism for fucosylation. Int. J. Cancer 2006, 118, 2803–2808. [Google Scholar] [CrossRef]
- Park, S.-Y.; Yoon, S.-J.; Jeong, Y.-T.; Kim, J.-M.; Kim, J.-Y.; Bernert, B.; Ullman, T.; Itzkowitz, S.H.; Kim, J.-H.; Hakomori, S. N-glycosylation status of β-haptoglobin in sera of patients with colon cancer, chronic inflammatory diseases and normal subjects. Int. J. Cancer 2010, 126, 142–155. [Google Scholar] [CrossRef]
- Yoon, S.-J.; Park, S.-Y.; Pang, P.-C.; Gallagher, J.; Gottesman, J.E.; Dell, A.; Kim, J.-H.; Hakomori, S.-I. N-glycosylation status of beta-haptoglobin in sera of patients with prostate cancer vs. benign prostate diseases. Int. J. Oncol. 2010, 36, 193–203. [Google Scholar] [PubMed]
- Dargan, E.; Thompson, S.; Cantwell, B.M.J.; Wilson, R.G.; Turner, G.A. Changes in the fucose content of haptoglobin in breast and ovarian cancer: Association with disease progression. Glycosylation Dis. 1994, 1, 37–43. [Google Scholar] [CrossRef]
- Nakano, M.; Nakagawa, T.; Ito, T.; Kitada, T.; Hijioka, T.; Kasahara, A.; Tajiri, M.; Wada, Y.; Taniguchi, N.; Miyoshi, E. Site-specific analysis of N-glycans on haptoglobin in sera of patients with pancreatic cancer: A novel approach for the development of tumor markers. Int. J. Cancer 2008, 122, 2301–2309. [Google Scholar] [CrossRef] [PubMed]
- Tomana, M.; Schrohenloher, R.E.; Koopman, W.J.; Alarcón, G.S.; Paul, W.A. Abnormal glycosylation of serum IgG from patients with chronic inflammatory diseases. Arthritis Rheum. 1988, 31, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Parekh, R.B.; Roitt, I.M.; Isenberg, D.A.; Dwek, R.A.; Ansell, B.M.; Rademacher, T.W. Galactosylation of IgG associated oligosaccharides: Reduction in patients with adult and juvenile onset rheumatoid arthritis and relation to disease activity. Lancet (London, England) 1988, 1, 966–969. [Google Scholar] [CrossRef]
- Mehta, A.S.; Long, R.E.; Comunale, M.A.; Wang, M.; Rodemich, L.; Krakover, J.; Philip, R.; Marrero, J.A.; Dwek, R.A.; Block, T.M. Increased Levels of Galactose-Deficient Anti-Gal Immunoglobulin G in the Sera of Hepatitis C Virus-Infected Individuals with Fibrosis and Cirrhosis. J. Virol. 2008, 82, 1259–1270. [Google Scholar] [CrossRef]
- Kanoh, Y.; Mashiko, T.; Danbara, M.; Takayama, Y.; Ohtani, S.; Egawa, S.; Baba, S.; Akahoshi, T. Changes in serum IgG oligosaccharide chains with prostate cancer progression. Anticancer Res. 2004, 24, 3135–3139. [Google Scholar]
- Ercan, A.; Cui, J.; Chatterton, D.E.W.; Deane, K.D.; Hazen, M.M.; Brintnell, W.; O’Donnell, C.I.; Derber, L.A.; Weinblatt, M.E.; Shadick, N.A.; et al. Aberrant IgG galactosylation precedes disease onset, correlates with disease activity, and is prevalent in autoantibodies in rheumatoid arthritis. Arthritis Rheum. 2010, 62, 2239–2248. [Google Scholar] [CrossRef]
- Vučković, F.; Krištić, J.; Gudelj, I.; Teruel, M.; Keser, T.; Pezer, M.; Pučić-Baković, M.; Štambuk, J.; Trbojević-Akmačić, I.; Barrios, C.; et al. Association of Systemic Lupus Erythematosus With Decreased Immunosuppressive Potential of the IgG Glycome. Arthritis Rheumatol. 2015, 67, 2978–2989. [Google Scholar] [CrossRef]
- Gudelj, I.; Lauc, G.; Pezer, M. Immunoglobulin G glycosylation in aging and diseases. Cell. Immunol. 2018, 333, 65–79. [Google Scholar] [CrossRef]
- Axford, J.S. Glycosylation and rheumatic disease. Adv. Exp. Med. Biol. 1998, 435, 163–173. [Google Scholar] [PubMed]
- Goodarzi, M.T.; Axford, J.S.; Varanasi, S.S.; Alavi, A.; Cunnane, G.; Fitzgerald, O.; Turner, G.A. Sialyl Lewis(x) expression on IgG in rheumatoid arthritis and other arthritic conditions: A preliminary study. Glycoconj. J. 1998, 15, 1149–1154. [Google Scholar] [CrossRef] [PubMed]
- Barratt, J.; Smith, A.C.; Feehally, J. The pathogenic role of IgA1 O-linked glycosylation in the pathogenesis of IgA nephropathy (Review Article). Nephrology 2007, 12, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Lai, K.N. Pathogenesis of IgA nephropathy. Nat. Rev. Nephrol. 2012, 8, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Pilobello, K.T.; Mahal, L.K. Lectin microarrays for glycoprotein analysis. Methods Mol. Biol. 2007, 385, 193–203. [Google Scholar] [PubMed]
- Gornik, O.; Lauc, G. Glycosylation of Serum Proteins in Inflammatory Diseases. Dis. Markers 2008, 25, 267–278. [Google Scholar] [CrossRef]
- Qi, Y.-J.; Ward, D.G.; Pang, C.; Wang, Q.-M.; Wei, W.; Ma, J.; Zhang, J.; Lou, Q.; Shimwell, N.J.; Martin, A.; et al. Proteomic profiling of N-linked glycoproteins identifies ConA-binding procathepsin D as a novel serum biomarker for hepatocellular carcinoma. Proteomics 2014, 14, 186–195. [Google Scholar] [CrossRef]
- Miura, Y.; Hato, M.; Shinohara, Y.; Kuramoto, H.; Furukawa, J.; Kurogochi, M.; Shimaoka, H.; Tada, M.; Nakanishi, K.; Ozaki, M.; et al. BlotGlycoABCTM, an integrated glycoblotting technique for rapid and large scale clinical glycomics. Mol. Cell. Proteomics 2008, 7, 370–377. [Google Scholar] [CrossRef]
- Gizaw, S.T.; Ohashi, T.; Tanaka, M.; Hinou, H.; Nishimura, S.-I. Glycoblotting method allows for rapid and efficient glycome profiling of human Alzheimer’s disease brain, serum and cerebrospinal fluid towards potential biomarker discovery. Biochim. Biophys. Acta—Gen. Subj. 2016, 1860, 1716–1727. [Google Scholar] [CrossRef]
- Connelly, M.A.; Gruppen, E.G.; Otvos, J.D.; Dullaart, R.P.F. Inflammatory glycoproteins in cardiometabolic disorders, autoimmune diseases and cancer. Clin. Chim. Acta 2016, 459, 177–186. [Google Scholar] [CrossRef]
- Lenz, E.M.; Bright, J.; Wilson, I.D.; Morgan, S.R.; Nash, A.F.P. A 1H NMR-based metabonomic study of urine and plasma samples obtained from healthy human subjects. J. Pharm. Biomed. Anal. 2003, 33, 1103–1115. [Google Scholar] [CrossRef]
- Beckonert, O.; Keun, H.C.; Ebbels, T.M.D.; Bundy, J.; Holmes, E.; Lindon, J.C.; Nicholson, J.K. Metabolic profiling, metabolomic and metabonomic procedures for NMR spectroscopy of urine, plasma, serum and tissue extracts. Nat. Protoc. 2007, 2, 2692–2703. [Google Scholar] [CrossRef] [PubMed]
- Aru, V.; Lam, C.; Khakimov, B.; Hoefsloot, H.C.J.; Zwanenburg, G.; Lind, M.V.; Schäfer, H.; van Duynhoven, J.; Jacobs, D.M.; Smilde, A.K.; et al. Quantification of lipoprotein profiles by nuclear magnetic resonance spectroscopy and multivariate data analysis. TrAC Trends Anal. Chem. 2017, 94, 210–219. [Google Scholar] [CrossRef]
- Torri, G.M.; Torri, J.; Gulian, J.-M.; Vion-Dury, J.; Viout, P.J.; Cozzone, P. Magnetic resonance spectroscopy of serum and acute-phase proteins revisited: A multiparametric statistical analysis of metabolite variations in inflammatory, infectious and miscellaneous diseases. Clin. Chim. Acta 1999, 279, 77–96. [Google Scholar] [CrossRef]
- Jeyarajah, E.J.; Cromwell, W.C.; Otvos, J.D. Lipoprotein Particle Analysis by Nuclear Magnetic Resonance Spectroscopy. Clin. Lab. Med. 2006, 26, 847–870. [Google Scholar] [CrossRef] [PubMed]
- Sears, B.; Deckelbaum, R.J.; Janiak, M.J.; Shipley, G.G.; Small, D.M. Temperature-dependent 13C nuclear magnetic resonance studies of human serum low density lipoproteins. Biochemistry 1976, 15, 4151–4157. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, S.C.; Würtz, P.; Nath, A.P.; Abraham, G.; Havulinna, A.S.; Fearnley, L.G.; Sarin, A.P.; Kangas, A.J.; Soininen, P.; Aalto, K.; et al. The Biomarker GlycA is Associated with Chronic Inflammation and Predicts Long-Term Risk of Severe Infection. Cell Syst. 2015, 1, 293–301. [Google Scholar] [CrossRef]
- Tuck, M.K.; Chan, D.W.; Chia, D.; Godwin, A.K.; Grizzle, W.E.; Krueger, K.E.; Rom, W.; Sanda, M.; Sorbara, L.; Stass, S.; et al. Standard operating procedures for serum and plasma collection: Early detection research network consensus statement standard operating procedure integration working group. J. Proteome Res. 2009, 8, 113–117. [Google Scholar] [CrossRef]
- De Meyer, T.; Sinnaeve, D.; Van Gasse, B.; Tsiporkova, E.; Rietzschel, E.R.; De Buyzere, M.L.; Gillebert, T.C.; Bekaert, S.; Martins, J.C.; Van Criekinge, W. NMR-Based Characterization of Metabolic Alterations in Hypertension Using an Adaptive, Intelligent Binning Algorithm. Anal. Chem. 2008, 80, 3783–3790. [Google Scholar] [CrossRef]
- Fuertes-Martín, R.; Taverner, D.; Vallvé, J.-C.; Paredes, S.; Masana, L.; Correig Blanchar, X.; Amigó Grau, N. Characterization of 1 H NMR Plasma Glycoproteins as a New Strategy To Identify Inflammatory Patterns in Rheumatoid Arthritis. J. Proteome Res. 2018, 17, 3730–3739. [Google Scholar] [CrossRef]
- Otvos, J.D.; Shalaurova, I.; Wolak-Dinsmore, J.; Connelly, M.A.; Mackey, R.H.; Stein, J.H.; Tracy, R.P. GlycA: A Composite Nuclear Magnetic Resonance Biomarker of Systemic Inflammation. Clin. Chem. 2015, 61, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, S.C.; Kettunen, J.; Brozynska, M.; Nath, A.P.; Havulinna, A.S.; Männistö, S.; Perola, M.; Salomaa, V.; Ala-Korpela, M.; Abraham, G.; et al. Elevated alpha-1 antitrypsin is a major component of GlycA-associated risk for future morbidity and mortality. bioRxiv 2018, 309138. [Google Scholar] [CrossRef] [PubMed]
- Röytiö, H.; Mokkala, K.; Vahlberg, T.; Laitinen, K. Dietary intake of fat and fibre according to reference values relates to higher gut microbiota richness in overweight pregnant women. Br. J. Nutr. 2017, 118, 343–352. [Google Scholar] [CrossRef]
- Nicholson, J.K.; Buckingham, M.J.; Sadler, P.J. High resolution 1H NMR studies of vertebrate blood and plasma. Biochem. J. 1983, 211, 605–615. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.K.; O’Flynn, M.P.; Sadler, P.J.; Macleod, A.F.; Juul, S.M.; Sönksen, P.H. Proton-nuclear-magnetic-resonance studies of serum, plasma and urine from fasting normal and diabetic subjects. Biochem. J. 1984, 217, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Kolwijck, E.; Engelke, U.F.; van der Graaf, M.; Heerschap, A.; Blom, H.J.; Hadfoune, M.; Buurman, W.A.; Massuger, L.F.; Wevers, R.A. N-acetyl resonances in in vivo and in vitro NMR spectroscopy of cystic ovarian tumors. NMR Biomed. 2009, 22, 1093–1099. [Google Scholar]
- Hasim, A.; Ma, H.; Mamtimin, B.; Abudula, A.; Niyaz, M.; Zhang, L.; Anwer, J.; Sheyhidin, I. Revealing the metabonomic variation of EC using 1H-NMR spectroscopy and its association with the clinicopathological characteristics. Mol. Biol. Rep. 2012, 39, 8955–8964. [Google Scholar] [CrossRef]
- Jobard, E.; Pontoizeau, C.; Blaise, B.J.; Bachelot, T.; Elena-Herrmann, B.; Trédan, O. A serum nuclear magnetic resonance-based metabolomic signature of advanced metastatic human breast cancer. Cancer Lett. 2014, 343, 33–41. [Google Scholar] [CrossRef]
- Deja, S.; Porebska, I.; Kowal, A.; Zabek, A.; Barg, W.; Pawelczyk, K.; Stanimirova, I.; Daszykowski, M.; Korzeniewska, A.; Jankowska, R.; et al. Metabolomics provide new insights on lung cancer staging and discrimination from chronic obstructive pulmonary disease. J. Pharm. Biomed. Anal. 2014, 100, 369–380. [Google Scholar] [CrossRef]
- Suman, S.; Sharma, R.K.; Kumar, V.; Sinha, N.; Shukla, Y. Metabolic fingerprinting in breast cancer stages through 1H NMR spectroscopy-based metabolomic analysis of plasma. J. Pharm. Biomed. Anal. 2018, 160, 38–45. [Google Scholar] [CrossRef]
- Dullaart, R.P.F.; Gruppen, E.G.; Connelly, M.A.; Otvos, J.D.; Lefrandt, J.D. GlycA, a biomarker of inflammatory glycoproteins, is more closely related to the leptin/adiponectin ratio than to glucose tolerance status. Clin. Biochem. 2015, 48, 811–814. [Google Scholar] [CrossRef] [PubMed]
- Mokkala, K.; Pellonperä, O.; Röytiö, H.; Pussinen, P.; Rönnemaa, T.; Laitinen, K. Increased intestinal permeability, measured by serum zonulin, is associated with metabolic risk markers in overweight pregnant women. Metabolism 2017, 69, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Newgard, C.B.; An, J.; Bain, J.R.; Muehlbauer, M.J.; Stevens, R.D.; Lien, L.F.; Haqq, A.M.; Shah, S.H.; Arlotto, M.; Slentz, C.A.; et al. A branched-chain amino acid-related metabolic signature that differentiates obese and lean humans and contributes to insulin resistance. Cell Metab. 2009, 9, 311–326. [Google Scholar] [CrossRef]
- Lorenzo, C.; Festa, A.; Hanley, A.J.; Rewers, M.J.; Escalante, A.; Haffner, S.M. Novel Protein Glycan–Derived Markers of Systemic Inflammation and C-Reactive Protein in Relation to Glycemia, Insulin Resistance, and Insulin Secretion. Diabetes Care 2017, 40, 375–382. [Google Scholar] [CrossRef]
- Wurtz, P.; Tiainen, M.; Makinen, V.-P.; Kangas, A.J.; Soininen, P.; Saltevo, J.; Keinanen-Kiukaanniemi, S.; Mantyselka, P.; Lehtimaki, T.; Laakso, M.; et al. Circulating Metabolite Predictors of Glycemia in Middle-Aged Men and Women. Diabetes Care 2012, 35, 1749–1756. [Google Scholar] [CrossRef]
- Dungan, K.; Binkley, P.; Osei, K. GlycA is a Novel Marker of Inflammation Among Non-Critically Ill Hospitalized Patients with Type 2 Diabetes. Inflammation 2015, 38, 1357–1363. [Google Scholar] [CrossRef]
- Connelly, M.A.; Gruppen, E.G.; Wolak-Dinsmore, J.; Matyus, S.P.; Riphagen, I.J.; Shalaurova, I.; Bakker, S.J.L.; Otvos, J.D.; Dullaart, R.P.F. GlycA, a marker of acute phase glycoproteins, and the risk of incident type 2 diabetes mellitus: PREVEND study. Clin. Chim. Acta 2016, 452, 10–17. [Google Scholar] [CrossRef]
- Akinkuolie, A.O.; Pradhan, A.D.; Buring, J.E.; Ridker, P.M.; Mora, S. Novel Protein Glycan Side-Chain Biomarker and Risk of Incident Type 2 Diabetes Mellitus. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 1544–1550. [Google Scholar] [CrossRef]
- Fizelova, M.; Jauhiainen, R.; Kangas, A.J.; Soininen, P.; Ala-Korpela, M.; Kuusisto, J.; Laakso, M.; Stančáková, A. Differential Associations of Inflammatory Markers With Insulin Sensitivity and Secretion: The Prospective METSIM Study. J. Clin. Endocrinol. Metab. 2017, 102, 3600–3609. [Google Scholar] [CrossRef]
- Gruppen, E.G.; Connelly, M.A.; Otvos, J.D.; Bakker, S.J.L.; Dullaart, R.P.F. A novel protein glycan biomarker and LCAT activity in metabolic syndrome. Eur. J. Clin. Investig. 2015, 45, 850–859. [Google Scholar] [CrossRef]
- Gruppen, E.G.; Connelly, M.A.; Vart, P.; Otvos, J.D.; Bakker, S.J.; Dullaart, R.P. GlycA, a novel proinflammatory glycoprotein biomarker, and high-sensitivity C-reactive protein are inversely associated with sodium intake after controlling for adiposity: The Prevention of Renal and Vascular End-Stage Disease study. Am. J. Clin. Nutr. 2016, 104, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Chandler, P.D.; Akinkuolie, A.O.; Tobias, D.K.; Lawler, P.R.; Li, C.; Moorthy, M.V.; Wang, L.; Duprez, D.A.; Jacobs, D.R.; Glynn, R.J.; et al. Association of N-Linked glycoprotein acetyls and colorectal cancer incidence and mortality. PLoS ONE 2016, 11, e0165615. [Google Scholar] [CrossRef] [PubMed]
- Duprez, D.A.; Otvos, J.; Sanchez, O.A.; Mackey, R.H.; Tracy, R.; Jacobs, D.R. Comparison of the Predictive Value of GlycA and Other Biomarkers of Inflammation for Total Death, Incident Cardiovascular Events, Noncardiovascular and Noncancer Inflammatory-Related Events, and Total Cancer Events. Clin. Chem. 2016, 62, 1020–1031. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.; Kettunen, J.; Würtz, P.; Haller, T.; Havulinna, A.S.; Kangas, A.J.; Soininen, P.; Esko, T.; Tammesoo, M.-L.; Mägi, R.; et al. Biomarker Profiling by Nuclear Magnetic Resonance Spectroscopy for the Prediction of All-Cause Mortality: An Observational Study of 17,345 Persons. PLoS Med. 2014, 11, e1001606. [Google Scholar] [CrossRef] [PubMed]
- Akinkuolie, A.O.; Buring, J.E.; Ridker, P.M.; Mora, S. A Novel Protein Glycan Biomarker and Future Cardiovascular Disease Events. J. Am. Heart Assoc. 2014, 3, e001221. [Google Scholar] [CrossRef] [PubMed]
- Muhlestein, J.B.; May, H.; Winegar, D.; Rollo, J.; Connelly, M.; Otvos, J.; Anderson, J. GlycA and GlycB, novel NMR biomarkers of inflammation, strongly predict future cardiovascular events, but not the presence of coronary artery disease (CAD), among patients undergoing coronary angiography: The intermountain heart collaborative study. J. Am. Coll. Cardiol. 2014, 63, A1389. [Google Scholar] [CrossRef]
- Connelly, M.A.; Shimizu, C.; Winegar, D.A.; Shalaurova, I.; Pourfarzib, R.; Otvos, J.D.; Kanegaye, J.T.; Tremoulet, A.H.; Burns, J.C. Differences in GlycA and lipoprotein particle parameters may help distinguish acute kawasaki disease from other febrile illnesses in children. BMC Pediatr. 2016, 16, 151. [Google Scholar] [CrossRef]
- Muhlestein, J.B.; May, H.; Winegar, D.; Rollo, J.; Connelly, M.; Otvos, J.; Anderson, J. Differential association of high-density lipoprotein particle subclasses and GlycA, a novel inflammatory marker, in predicting cardiac death among patients undergoing angiography: The intermountain heart collaborative study. J. Am. Coll. Cardiol. 2016, 67, 162. [Google Scholar] [CrossRef]
- Muhlestein, J.B.; May, H.T.; Galenko, O.; Knowlton, K.U.; Otvos, J.D.; Connelly, M.A.; Lappe, D.L.; Anderson, J.L. GlycA and hsCRP are independent and additive predictors of future cardiovascular events among patients undergoing angiography: The intermountain heart collaborative study. Am. Heart J. 2018, 202, 27–32. [Google Scholar] [CrossRef]
- McGarrah, R.W.; Kelly, J.P.; Craig, D.M.; Haynes, C.; Jessee, R.C.; Huffman, K.M.; Kraus, W.E.; Shah, S.H. A Novel Protein Glycan–Derived Inflammation Biomarker Independently Predicts Cardiovascular Disease and Modifies the Association of HDL Subclasses with Mortality. Clin. Chem. 2017, 63, 288–296. [Google Scholar] [CrossRef]
- Otvos, J.D.; Guyton, J.R.; Connelly, M.A.; Akapame, S.; Bittner, V.; Kopecky, S.L.; Lacy, M.; Marcovina, S.M.; Muhlestein, J.B.; Boden, W.E. Relations of GlycA and lipoprotein particle subspecies with cardiovascular events and mortality: A post hoc analysis of the AIM-HIGH trial. J. Clin. Lipidol. 2018, 12, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Gruppen, E.G.; Connelly, M.A.; Sluiter, W.J.; Bakker, S.J.L.; Dullaart, R.P.F. Higher plasma GlycA, a novel pro-inflammatory glycoprotein biomarker, is associated with reduced life expectancy: The PREVEND study. Clin. Chim. Acta 2019, 488, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Kettunen, J.; Ritchie, S.; Anufrieva, O.; Lyytikainen, L.-P.; Hernesniemi, J.; Karhunen, P.J.; Kuukasjarvi, P.; Laurikka, J.; Kahonen, M.; Lehtimaki, T.; et al. The landscape of incident disease risk for the biomarker GlycA and its mortality stratification in angiography patients. bioRxiv 2018, 280677. [Google Scholar]
- Tibuakuu, M.; Fashanu, O.E.; Bs, M.B.; Zhao, D.; Otvos, J.D.; Brown, T.T.; Haberlen, S.A.; Guallar, E.; Budoff, M.J.; Palella, F.J.; et al. GlycA, a Novel Inflammatory Marker, is Associated with Subclinical Coronary Disease in the Multicenter AIDS Cohort Study Short title: GlycA and Coronary Plaque in HIV. UCLA Previously Publ. Work. 2019, 33, 547–557. [Google Scholar]
- Bartlett, D.B.; Connelly, M.A.; AbouAssi, H.; Bateman, L.A.; Tune, K.N.; Huebner, J.L.; Kraus, V.B.; Winegar, D.A.; Otvos, J.D.; Kraus, W.E.; et al. A novel inflammatory biomarker, GlycA, associates with disease activity in rheumatoid arthritis and cardio-metabolic risk in BMI-matched controls. Arthritis Res. Ther. 2016, 18, 86. [Google Scholar] [CrossRef]
- Ormseth, M.J.; Chung, C.P.; Oeser, A.M.; Connelly, M.A.; Sokka, T.; Raggi, P.; Solus, J.F.; Otvos, J.D.; Stein, C.M. Utility of a novel inflammatory marker, GlycA, for assessment of rheumatoid arthritis disease activity and coronary atherosclerosis. Arthritis Res. Ther. 2015, 17, 117. [Google Scholar] [CrossRef]
- Durcan, L.; Winegar, D.A.; Connelly, M.A.; Otvos, J.D.; Magder, L.S.; Petri, M. Longitudinal Evaluation of Lipoprotein Variables in Systemic Lupus Erythematosus Reveals Adverse Changes with Disease Activity and Prednisone and More Favorable Profiles with Hydroxychloroquine Therapy. J. Rheumatol. 2016, 43, 745–750. [Google Scholar] [CrossRef]
- Chung, C.P.; Ormseth, M.J.; Connelly, M.A.; Oeser, A.; Solus, J.F.; Otvos, J.D.; Raggi, P.; Stein, C.M. GlycA, a novel marker of inflammation, is elevated in systemic lupus erythematosus. Lupus 2016, 25, 296–300. [Google Scholar] [CrossRef]
- Dierckx, T.; Goletti, S.; Chiche, L.; Daniel, L.; Lauwerys, B.; Jourde-Chiche, N.; Weyenbergh, J. Van Serum GlycA level is a candidate biomarker for disease activity in systemic lupus erythematosus and for proliferative status of lupus nephritis, independent of renal function impairment. bioRxiv 2018, 493809. [Google Scholar]
- Joshi, A.A.; Lerman, J.B.; Aberra, T.M.; Afshar, M.; Teague, H.L.; Rodante, J.A.; Krishnamoorthy, P.; Ng, Q.; Aridi, T.Z.; Salahuddin, T.; et al. GlycA Is a Novel Biomarker of Inflammation and Subclinical Cardiovascular Disease in Psoriasis. Circ. Res. 2016, 119. [Google Scholar] [CrossRef]
- Dierckx, T.; Verstockt, B.; Vermeire, S.; van Weyenbergh, J. GlycA, a Nuclear Magnetic Resonance Spectroscopy Measure for Protein Glycosylation, is a Viable Biomarker for Disease Activity in IBD. J. Crohn’s Colitis 2018, 13, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Titan, S.M.; Pecoits-Filho, R.; Barreto, S.M.; Lopes, A.A.; Bensenor, I.J.; Lotufo, P.A. GlycA, a marker of protein glycosylation, is related to albuminuria and estimated glomerular filtration rate: The ELSA-Brasil study. BMC Nephrol. 2017, 18, 367. [Google Scholar] [CrossRef] [PubMed]
- Sands, C.J.; Guha, I.N.; Kyriakides, M.; Wright, M.; Beckonert, O.; Holmes, E.; Rosenberg, W.M.; Coen, M. Metabolic Phenotyping for Enhanced Mechanistic Stratification of Chronic Hepatitis C-Induced Liver Fibrosis. Am. J. Gastroenterol. 2015, 110, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Manheim, I.; Doniger, G.M.; Sinnreich, R.; Simon, E.S.; Pinchas-Mizrachi, R.; Otvos, J.D.; Kark, J.D. Increase in the Inflammatory Marker GlycA over 13 Years in Young Adults Is Associated with Poorer Cognitive Function in Midlife. PLoS ONE 2015, 10, e0138036. [Google Scholar] [CrossRef]
- Tukiainen, T.; Tynkkynen, T.; Mäkinen, V.-P.; Jylänki, P.; Kangas, A.; Hokkanen, J.; Vehtari, A.; Gröhn, O.; Hallikainen, M.; Soininen, H.; et al. A multi-metabolite analysis of serum by 1H NMR spectroscopy: Early systemic signs of Alzheimer’s disease. Biochem. Biophys. Res. Commun. 2008, 375, 356–361. [Google Scholar] [CrossRef]
- Jain, A.; Kumar, D.; Guleria, A.; Misra, D.P.; Zanwar, A.; Chaurasia, S.; Kumar, S.; Kumar, U.; Mishra, S.K.; Goel, R.; et al. NMR-Based Serum Metabolomics of Patients with Takayasu Arteritis: Relationship with Disease Activity. J. Proteome Res. 2018, 17, 3317–3324. [Google Scholar] [CrossRef]
- Guleria, A.; Misra, D.P.; Rawat, A.; Dubey, D.; Khetrapal, C.L.; Bacon, P.; Misra, R.; Kumar, D. NMR-Based Serum Metabolomics Discriminates Takayasu Arteritis from Healthy Individuals: A Proof-of-Principle Study. J. Proteome Res. 2015, 14, 3372–3381. [Google Scholar] [CrossRef]
- Berends, A.M.A.; Buitenwerf, E.; Gruppen, E.G.; Sluiter, W.J.; Bakker, S.J.L.; Connelly, M.A.; Kerstens, M.N.; Dullaart, R.P.F. Primary aldosteronism is associated with decreased low-density and high-density lipoprotein particle concentrations and increased GlycA, a pro-inflammatory glycoprotein biomarker. Clin. Endocrinol. (Oxf). 2019, 90, 79–87. [Google Scholar] [CrossRef]
- Weisman, J.K.; Meeks, D.; Mendelsohn, L.; Remaley, A.T.; Sampson, M.; Allen, D.T.; Nichols, J.; Shet, A.S.; Thein, S.L. GlycA is not a useful biomarker of inflammation in sickle cell disease. Int. J. Lab. Hematol. 2018, 40, 704–709. [Google Scholar] [CrossRef]
- Lamour, S.D.; Gomez-Romero, M.; Vorkas, P.A.; Alibu, V.P.; Saric, J.; Holmes, E.; Sternberg, J.M. Discovery of Infection Associated Metabolic Markers in Human African Trypanosomiasis. PLoS Negl. Trop. Dis. 2015, 9, e0004200. [Google Scholar] [CrossRef][Green Version]
- Kianoush, S.; Bittencourt, M.S.; Lotufo, P.A.; Bensenor, I.M.; Jones, S.R.; DeFilippis, A.P.; Toth, P.P.; Otvos, J.D.; Tibuakuu, M.; Hall, M.E.; et al. Association Between Smoking and Serum GlycA and High-Sensitivity C-Reactive Protein Levels: The Multi-Ethnic Study of Atherosclerosis (MESA) and Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). J. Am. Heart Assoc. 2017, 6, e006545. [Google Scholar] [CrossRef] [PubMed]
- Kujala, U.M.; Mäkinen, V.-P.; Heinonen, I.; Soininen, P.; Kangas, A.J.; Leskinen, T.H.; Rahkila, P.; Würtz, P.; Kovanen, V.; Cheng, S.; et al. Long-term Leisure-time Physical Activity and Serum Metabolome. Circulation 2013, 127, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, D.B.; Slentz, C.A.; Connelly, M.A.; Piner, L.W.; Willis, L.H.; Bateman, L.A.; Granville, E.O.; Bales, C.W.; Huffman, K.M.; Kraus, W.E. Association of the Composite Inflammatory Biomarker GlycA, with Exercise-Induced Changes in Body Habitus in Men and Women with Prediabetes. Oxid. Med. Cell. Longev. 2017, 2017, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Barber, J.L.; Kraus, W.E.; Church, T.S.; Hagberg, J.M.; Thompson, P.D.; Bartlett, D.B.; Beets, M.W.; Earnest, C.P.; Huffman, K.M.; Landers-Ramos, R.Q.; et al. Effects of regular endurance exercise on GlycA: Combined analysis of 14 exercise interventions. Atherosclerosis 2018, 277, 1–6. [Google Scholar] [CrossRef]
- Kelesidis, T.; Tran, T.T.T.; Stein, J.H.; Brown, T.T.; Moser, C.; Ribaudo, H.J.; Dube, M.P.; Murphy, R.; Yang, O.O.; Currier, J.S.; et al. Changes in Inflammation and Immune Activation With Atazanavir-, Raltegravir-, Darunavir-Based Initial Antiviral Therapy: ACTG 5260s. Clin. Infect. Dis. 2015, 61, 651–660. [Google Scholar] [CrossRef]
- Huo, T.; Cai, S.; Lu, X.; Sha, Y.; Yu, M.; Li, F. Metabonomic study of biochemical changes in the serum of type 2 diabetes mellitus patients after the treatment of metformin hydrochloride. J. Pharm. Biomed. Anal. 2009, 49, 976–982. [Google Scholar] [CrossRef]
- Gruppen, E.G.; Connelly, M.A.; Dullaart, R.P.F. Higher circulating GlycA, a pro-inflammatory glycoprotein biomarker, relates to lipoprotein-associated phospholipase A2 mass in nondiabetic subjects but not in diabetic or metabolic syndrome subjects. J. Clin. Lipidol. 2016, 10, 512–518. [Google Scholar] [CrossRef]
- Pinto, J.; Barros, A.S.; Domingues, M.R.M.; Goodfellow, B.J.; Galhano, E.; Pita, C.; Almeida, M.D.C.; Carreira, I.M.; Gil, A.M. Following Healthy Pregnancy by NMR Metabolomics of Plasma and Correlation to Urine. J. Proteome Res. 2015, 14, 1263–1274. [Google Scholar] [CrossRef]
- Houttu, N.; Mokkala, K.; Laitinen, K. Overweight and obesity status in pregnant women are related to intestinal microbiota and serum metabolic and inflammatory profiles. Clin. Nutr. 2018, 37, 1955–1966. [Google Scholar] [CrossRef]
- Huo, T.; Chen, X.; Lu, X.; Qu, L.; Liu, Y.; Cai, S. An effective assessment of valproate sodium-induced hepatotoxicity with UPLC–MS and 1HNMR-based metabonomics approach. J. Chromatogr. B 2014, 969, 109–116. [Google Scholar] [CrossRef]
- Boguszewicz, Ł.; Hajduk, A.; Mrochem-Kwarciak, J.; Skorupa, A.; Ciszek, M.; Heyda, A.; Składowski, K.; Sokół, M. 1H NMR based metabolomic approach to monitoring of the head and neck cancer treatment toxicity. Metabolomics 2016, 12, 102. [Google Scholar] [CrossRef]
- Stowell, S.R.; Ju, T.; Cummings, R.D. Protein Glycosylation in Cancer. Annu. Rev. Pathol. Mech. Dis. 2015, 10, 473–510. [Google Scholar] [CrossRef] [PubMed]
- Kriat, M.; Vion-Dury, J.; Fayre, R.; Maraninchi, D.; Harlé, J.R.; Confort-Gouny, S.; Sciaky, M.; Fontanarava, E.; Viout, P.; Cozzone, P.J. Variations of plasma sialic acid and N-acetylglucosamine levels in cancer, inflammatory diseases and bone marrow transplantation: A proton NMR spectroscopy study. Biochimie 1991, 73, 99–104. [Google Scholar] [CrossRef]
- Tiziani, S.; Lopes, V.; Günther, U.L. Early Stage Diagnosis of Oral Cancer Using 1 H NMR-Based Metabolomics 1,2. Neoplasia 2009, 11, 269–276. [Google Scholar] [CrossRef]
- Lécuyer, L.; Victor Bala, A.; Deschasaux, M.; Bouchemal, N.; Nawfal Triba, M.; Vasson, M.-P.; Rossary, A.; Demidem, A.; Galan, P.; Hercberg, S.; et al. NMR metabolomic signatures reveal predictive plasma metabolites associated with long-term risk of developing breast cancer. Int. J. Epidemiol. 2018, 47, 484–494. [Google Scholar] [CrossRef]
- Boss, E.A.; Moolenaar, S.H.; Massuger, L.F.A.G.; Boonstra, H.; Engelke, U.F.H.; De Jong, J.G.N.; Wevers, R.A. High-resolution proton nuclear magnetic resonance spectroscopy of ovarian cyst fluid. NMR Biomed. 2000, 13, 297. [Google Scholar] [CrossRef]
- Hasim, A.; Ali, M.; Mamtimin, B.; Ma, J.; Li, G.; Abudula, A. Metabonomic signature analysis of cervical carcinoma and precancerous lesions in women by 1H NMR spectroscopy. Exp. Ther. Med. 2012, 3, 945–951. [Google Scholar] [CrossRef][Green Version]
- Fages, A.; Duarte-Salles, T.; Stepien, M.; Ferrari, P.; Fedirko, V.; Pontoizeau, C.; Trichopoulou, A.; Aleksandrova, K.; Tjønneland, A.; Olsen, A.; et al. Metabolomic profiles of hepatocellular carcinoma in a European prospective cohort. BMC Med. 2015, 13, 242. [Google Scholar] [CrossRef]
- Li, P.; Tao, J.; Wei, D.; Yang, X.; Lu, Z.; Deng, X.; Cheng, Y.; Gu, J.; Yang, X.; Wang, Z.; et al. Serum metabolomic analysis of human upper urinary tract urothelial carcinoma. Tumor Biol. 2015, 36, 7531–7537. [Google Scholar] [CrossRef]
- Kelimu, A.; Xie, R.; Zhang, K.; Zhuang, Z.; Mamtimin, B.; Sheyhidin, I. Metabonomic signature analysis in plasma samples of glioma patients based on 1 H-nuclear magnetic resonance spectroscopy. Neurol. India 2016, 64, 246. [Google Scholar]
- López-Jaramillo, P.; Gómez-Arbeláez, D.; López-López, J.; López-López, C.; Martínez-Ortega, J.; Gómez-Rodríguez, A.; Triana-Cubillos, S. The role of leptin/adiponectin ratio in metabolic syndrome and diabetes. Horm. Mol. Biol. Clin. Investig. 2014, 18, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Finucane, F.M.; Luan, J.; Wareham, N.J.; Sharp, S.J.; O’Rahilly, S.; Balkau, B.; Flyvbjerg, A.; Walker, M.; Højlund, K.; Nolan, J.J.; et al. Correlation of the leptin:adiponectin ratio with measures of insulin resistance in non-diabetic individuals. Diabetologia 2009, 52, 2345–2349. [Google Scholar] [CrossRef] [PubMed]
- Dullaart, R.P.F.; Gruppen, E.G.; Connelly, M.A.; Lefrandt, J.D. A pro-inflammatory glycoprotein biomarker is associated with lower bilirubin in metabolic syndrome. Clin. Biochem. 2015, 48, 1045–1047. [Google Scholar] [CrossRef] [PubMed]
- Bogl, L.H.; Kaye, S.M.; Rämö, J.T.; Kangas, A.J.; Soininen, P.; Hakkarainen, A.; Lundbom, J.; Lundbom, N.; Ortega-Alonso, A.; Rissanen, A.; et al. Abdominal obesity and circulating metabolites: A twin study approach. Metabolism 2016, 65, 111–121. [Google Scholar] [CrossRef]
- Wang, T.J.; Larson, M.G.; Vasan, R.S.; Cheng, S.; Rhee, E.P.; McCabe, E.; Lewis, G.D.; Fox, C.S.; Jacques, P.F.; Fernandez, C.; et al. Metabolite profiles and the risk of developing diabetes. Nat. Med. 2011, 17, 448–453. [Google Scholar] [CrossRef]
- Manmadhan, A.; Lin, B.-X.; Zhong, J.; Parikh, M.; Berger, J.S.; Fisher, E.A.; Heffron, S.P. Elevated GlycA in severe obesity is normalized by bariatric surgery. Diabetes, Obes. Metab. 2019, 21, 178–182. [Google Scholar] [CrossRef]
- Jago, R.; Drews, K.L.; Otvos, J.D.; Willi, S.M.; Buse, J.B. Novel measures of inflammation and insulin resistance are related to obesity and fitness in a diverse sample of 11–14 year olds: The HEALTHY Study. Int. J. Obes. 2016, 40, 1157–1163. [Google Scholar] [CrossRef]
- Olson, M.L.; Rentería-Mexía, A.; Connelly, M.A.; Vega-López, S.; Soltero, E.G.; Konopken, Y.P.; Williams, A.N.; Castro, F.G.; Keller, C.S.; Yang, H.P.; et al. Decreased GlycA after lifestyle intervention among obese, prediabetic adolescent Latinos. J. Clin. Lipidol. 2019, 13, 186–193. [Google Scholar] [CrossRef]
- Tabish, S.A. Is Diabetes Becoming the Biggest Epidemic of the Twenty-first Century? Int. J. Health Sci. (Qassim) 2007, 1, 5–8. [Google Scholar]
- Duncan, B.B.; Schmidt, M.I.; Pankow, J.S.; Ballantyne, C.M.; Couper, D.; Vigo, A.; Hoogeveen, R.; Folsom, A.R.; Heiss, G. Atherosclerosis Risk in Communities Study Low-grade systemic inflammation and the development of type 2 diabetes: The atherosclerosis risk in communities study. Diabetes 2003, 52, 1799–1805. [Google Scholar] [CrossRef]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef]
- Karstoft, K.; Pedersen, B.K. Exercise and type 2 diabetes: Focus on metabolism and inflammation. Immunol. Cell Biol. 2016, 94, 146–150. [Google Scholar] [CrossRef]
- Pradhan, A.D.; Manson, J.E.; Rifai, N.; Buring, J.E.; Ridker, P.M. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA 2001, 286, 327–334. [Google Scholar] [CrossRef]
- Badawi, A.; Klip, A.; Haddad, P.; Cole, D.E.; Bailo, B.G.; El-Sohemy, A.; Karmali, M. Type 2 diabetes mellitus and inflammation: Prospects for biomarkers of risk and nutritional intervention. Diabetes. Metab. Syndr. Obes. 2010, 3, 173–186. [Google Scholar] [CrossRef]
- Rawat, A.; Misra, G.; Saxena, M.; Tripathi, S.; Dubey, D.; Saxena, S.; Aggarwal, A.; Gupta, V.; Khan, M.Y.; Prakash, A. 1H NMR based serum metabolic profiling reveals differentiating biomarkers in patients with diabetes and diabetes-related complication. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 290–298. [Google Scholar] [CrossRef]
- Sutherland, J.P.; McKinley, B.; Eckel, R.H. The Metabolic Syndrome and Inflammation. Metab. Syndr. Relat. Disord. 2004, 2, 82–104. [Google Scholar] [CrossRef]
- Esser, N.; Legrand-Poels, S.; Piette, J.; Scheen, A.J.; Paquot, N. Inflammation as a link between obesity, metabolic syndrome and type 2 diabetes. Diabetes Res. Clin. Pract. 2014, 105, 141–150. [Google Scholar] [CrossRef]
- Gruppen, E.G.; Riphagen, I.J.; Connelly, M.A.; Otvos, J.D.; Bakker, S.J.L.; Dullaart, R.P.F. GlycA, a Pro-Inflammatory Glycoprotein Biomarker, and Incident Cardiovascular Disease: Relationship with C-Reactive Protein and Renal Function. PLoS ONE 2015, 10, e0139057. [Google Scholar] [CrossRef]
- Ridker, P.M.; Hennekens, C.H.; Buring, J.E.; Rifai, N. C-Reactive Protein and Other Markers of Inflammation in the Prediction of Cardiovascular Disease in Women. N. Engl. J. Med. 2000, 342, 836–843. [Google Scholar] [CrossRef]
- Bassuk, S.S.; Rifai, N.; Ridker, P.M. High-sensitivity C-reactive protein: Clinical importance. Curr. Probl. Cardiol. 2004, 29, 439–493. [Google Scholar]
- Harris, T.B.; Ferrucci, L.; Tracy, R.P.; Corti, M.C.; Wacholder, S.; Ettinger, W.H.; Heimovitz, H.; Cohen, H.J.; Wallace, R. Associations of elevated interleukin-6 and C-reactive protein levels with mortality in the elderly. Am. J. Med. 1999, 106, 506–512. [Google Scholar] [CrossRef]
- Lawler, P.R.; Akinkuolie, A.O.; Chandler, P.D.; Moorthy, M.V.; Vandenburgh, M.J.; Schaumberg, D.A.; Lee, I.-M.; Glynn, R.J.; Ridker, P.M.; Buring, J.E.; et al. Circulating N-Linked Glycoprotein Acetyls and Longitudinal Mortality Risk Novelty and Significance. Circ. Res. 2016, 118, 1106–1115. [Google Scholar] [CrossRef] [PubMed]
- Benson, E.-M.A.; Tibuakuu, M.; Zhao, D.; Akinkuolie, A.O.; Otvos, J.D.; Duprez, D.A.; Jacobs, D.R.; Mora, S.; Michos, E.D. Associations of ideal cardiovascular health with GlycA, a novel inflammatory marker: The Multi-Ethnic Study of Atherosclerosis. Clin. Cardiol. 2018, 41, 1439–1445. [Google Scholar] [CrossRef] [PubMed]
- Holmes, M.V.; Millwood, I.Y.; Kartsonaki, C.; Hill, M.R.; Bennett, D.A.; Boxall, R.; Guo, Y.; Xu, X.; Bian, Z.; Hu, R.; et al. Lipids, Lipoproteins, and Metabolites and Risk of Myocardial Infarction and Stroke. J. Am. Coll. Cardiol. 2018, 71, 620–632. [Google Scholar] [CrossRef]
- McGarrah, R.; Craig, D.; Haynes, C.; Dowdy, Z.E.; Shah, S.; Kraus, W. GlycA, a novel biomarker of systemic inflammation, improves cardiovascular risk prediction in a high-risk coronary catheterization cohort. J. Am. Coll. Cardiol. 2015, 65, A1606. [Google Scholar] [CrossRef][Green Version]
- Correia, G.D.S.; Wooi Ng, K.; Wijeyesekera, A.; Gala-Peralta, S.; Williams, R.; MacCarthy-Morrogh, S.; Jiménez, B.; Inwald, D.; Macrae, D.; Frost, G.; et al. Metabolic Profiling of Children Undergoing Surgery for Congenital Heart Disease. Crit. Care Med. 2015, 43, 1467–1476. [Google Scholar] [CrossRef]
- Freiberg, M.S.; Chang, C.-C.H.; Kuller, L.H.; Skanderson, M.; Lowy, E.; Kraemer, K.L.; Butt, A.A.; Bidwell Goetz, M.; Leaf, D.; Oursler, K.A.; et al. HIV Infection and the Risk of Acute Myocardial Infarction. JAMA Intern. Med. 2013, 173, 614. [Google Scholar] [CrossRef]
- Triant, V.A.; Lee, H.; Hadigan, C.; Grinspoon, S.K. Increased Acute Myocardial Infarction Rates and Cardiovascular Risk Factors among Patients with Human Immunodeficiency Virus Disease. J. Clin. Endocrinol. Metab. 2007, 92, 2506–2512. [Google Scholar] [CrossRef]
- Mehta, N.N.; Yu, Y.; Saboury, B.; Foroughi, N.; Krishnamoorthy, P.; Raper, A.; Baer, A.; Antigua, J.; Van Voorhees, A.S.; Torigian, D.A.; et al. Systemic and Vascular Inflammation in Patients With Moderate to Severe Psoriasis as Measured by [18F]-Fluorodeoxyglucose Positron Emission Tomography—Computed Tomography (FDG-PET/CT). Arch. Dermatol. 2011, 147, 1031. [Google Scholar] [CrossRef]
- Mehta, N.N.; Azfar, R.S.; Shin, D.B.; Neimann, A.L.; Troxel, A.B.; Gelfand, J.M. Patients with severe psoriasis are at increased risk of cardiovascular mortality: Cohort study using the General Practice Research Database. Eur. Heart J. 2010, 31, 1000–1006. [Google Scholar] [CrossRef]
- Kaplan, G.G. The global burden of IBD: From 2015 to 2025. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-Z.; Li, Y.-Y. Inflammatory bowel disease: Pathogenesis. World J. Gastroenterol. 2014, 20, 91. [Google Scholar] [CrossRef] [PubMed]
- Austin, V.; Crack, P.J.; Bozinovski, S.; Miller, A.A.; Vlahos, R. COPD and stroke: Are systemic inflammation and oxidative stress the missing links? Clin. Sci. (Lond). 2016, 130, 1039–1050. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Upur, H.; Wu, Y.; Mamtimin, B.; Yang, J.; Ga, Y.; You, L. Metabolomic changes in patients with chronic obstructive pulmonary disease with abnormal Savda syndrome. Exp. Ther. Med. 2015, 9, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Ablimit, A.; Kühnel, H.; Strasser, A.; Upur, H. Abnormal Savda syndrome: Long-term consequences of emotional and physical stress on endocrine and immune activities in an animal model. Chin. J. Integr. Med. 2013, 19, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Gupta, J.; Mitra, N.; Kanetsky, P.A.; Devaney, J.; Wing, M.R.; Reilly, M.; Shah, V.O.; Balakrishnan, V.S.; Guzman, N.J.; Girndt, M.; et al. Association between Albuminuria, Kidney Function, and Inflammatory Biomarker Profile in CKD in CRIC. Clin. J. Am. Soc. Nephrol. 2012, 7, 1938–1946. [Google Scholar] [CrossRef]
- Upadhyay, A.; Larson, M.G.; Guo, C.-Y.; Vasan, R.S.; Lipinska, I.; O’Donnell, C.J.; Kathiresan, S.; Meigs, J.B.; Keaney, J.F.; Rong, J.; et al. Inflammation, kidney function and albuminuria in the Framingham Offspring cohort. Nephrol. Dial. Transplant. 2011, 26, 920–926. [Google Scholar] [CrossRef]
- Lee, B.T.; Ahmed, F.A.; Hamm, L.L.; Teran, F.J.; Chen, C.-S.; Liu, Y.; Shah, K.; Rifai, N.; Batuman, V.; Simon, E.E.; et al. Association of C-reactive protein, tumor necrosis factor-alpha, and interleukin-6 with chronic kidney disease. BMC Nephrol. 2015, 16, 77. [Google Scholar] [CrossRef]
- Tian, J.; Xia, X.; Wu, Y.; Zhao, L.; Xiang, H.; Du, G.; Zhang, X.; Qin, X. Discovery, screening and evaluation of a plasma biomarker panel for subjects with psychological suboptimal health state using 1H-NMR-based metabolomics profiles. Sci. Rep. 2016, 6, 33820. [Google Scholar] [CrossRef]
- Tombetti, E.; Mason, J.C. Takayasu arteritis: Advanced understanding is leading to new horizons. Rheumatology 2019, 58, 206–219. [Google Scholar] [CrossRef]
- Gordon, J.B.; Kahn, A.M.; Burns, J.C. When Children With Kawasaki Disease Grow Up. J. Am. Coll. Cardiol. 2009, 54, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Vilela, L.A.P.; Almeida, M.Q. Diagnosis and management of primary aldosteronism. Arch. Endocrinol. Metab. 2017, 61, 305–312. [Google Scholar] [CrossRef]
- Brown, N.J. Contribution of aldosterone to cardiovascular and renal inflammation and fibrosis. Nat. Rev. Nephrol. 2013, 9, 459–469. [Google Scholar] [CrossRef]
- Platt, O.S. Sickle cell anemia as an inflammatory disease. J. Clin. Investig. 2000, 106, 337–338. [Google Scholar] [CrossRef]
- Vermeire, S.; Van Assche, G.; Rutgeerts, P. Laboratory markers in IBD: Useful, magic, or unnecessary toys? Gut 2006, 55, 426–431. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Liu, K.; Tian, L.; Greenland, P. Narrative review: Assessment of C-reactive protein in risk prediction for cardiovascular disease. Ann. Intern. Med. 2006, 145, 35–42. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Glycoprotein | Glycation Change | Related Diseases | References |
|---|---|---|---|
| Alpha 1-Acid Glycoprotein (AGP) | Highly branched N-linked glycan | Cirrhosis and HCC, congenital disorders, RA, SLE | [35,36] |
| Increased sialylation | Cancer | [37] | |
| Decreased sialylation | Cirrhosis and HCC | [35,38] | |
| Increased fucosylation | liver cancer | [39] | |
| Alpha-Fetoprotein | Elevated bisecting N-acetylglucosamine, decrease in sialylation and increase in fucosylation | Cirrhosis, hepatitis and HCC | [40,41,42] |
| Alpha -1-antitrypsin (ATT) | Increased fucosylation alpha | Hepatitis C, HCC | [43,44] |
| Decrease in branching, predominance of alpha 2–6 linked sialic acid and less alpha 2–3 linked sialic acid | Breast and ovarian cancer | [45] | |
| Oligosaccharide branching and increased sialic acid content | Acute general inflammation | [46] | |
| Increased glycan branching | RA | [47] | |
| Transferrin | Increased branching and fucosylation of N-glycans. Increasing peripheral N-acetylglucosamine residues | Ovarian, breast and colon cancer, HCC, Cirrhosis, hepatitis | [48,49] |
| Increased fucosylation and sialic acid-linked to galactose | Liver disease | [50] | |
| Haptoglobin (Hp) | Increased fucose and N-acetylglucosamine | Alcoholic liver disease | [51] |
| Increased fucosylation | Various types of cancer and RA | [52,53,54,55] | |
| O-glycans ad fucosylation | Prostate cancer | [56] | |
| Inmunoglobulin G (IgG) | Decreased galactose | RA, SLE, IBD, ovarian cancer, prostate cancer | [57,58,59,60,61,62,63] |
| Increased N-acetylglucosamine residues (controversy) | RA | [64,65] | |
| Inmunoglobulin A (Ig A) | Reduced galactosylation of O-linked glycosylation | Nephropathy | [66,67] |
| Clinical Study Topic | Main Findings | References | |
|---|---|---|---|
| Tumors and cancer | OC, CSCC, BC, LC, CRC | Increased circulating N-acetyl glycoproteins levels and increased GlcNAc-branching of N-glycans. | [24,89,90,91,92,93] |
| Metabolic diseases | Obesity | Association between GlycA and the leptin/adiponectin ratio | [94] |
| Correlation between GlycA and TG and lipids | [95] | ||
| Correlation GlycA and branched chain amino acids | [96] | ||
| Strong relationship of CRP, GlycA, and GlycB and insulin resistance | [97] | ||
| Diabetes Mellitus | α1-acid glycoprotein as a predictor of future glycemia | [98] | |
| Associations of GlycA with higher IL-6 and CRP | [99] | ||
| Associations of GlycA with future T2DM | [100,101] | ||
| GlycA had a more robust correlation with CRP, plasma glucose, and measures of adiposity and insulin resistance than GlycB | [97,102] | ||
| MetS | Increased levels of glycosylated acute-phase proteins (GlycA) associated with MetS | [94,103,104] | |
| Cardiovascular risk | Healthy individuals | GlycA/alpha1-acid glycoproteins or baseline circulating glycoprotein N-acetyl methyl groups are associated with CVD and longitudinal risk of all-cause mortality. | [101,105,106,107,108,109,110] |
| High-risk individuals | GlycA and GlycB strongly associated with future major adverse CVE | [109] | |
| GlycA and hsCRP was statistically significant for the outcome of death | [111,112] | ||
| GlycA, and small and medium-size HDL particles proved to be independent predictors of cardiac death. | [113,114] | ||
| Life expectancy | Higher GlycA levels had lower life expectancy. | [115] | |
| All-cause mortality | Positive association between α1-antitrypsin and increased risk of liver diseases, heart failure, and COPD, and significant association between α1-acid glycoprotein and heart failure and chronic lower respiratory diseases | [85] | |
| GlycA related to increased risk of alcoholic liver disease, chronic renal failure, glomerular diseases, COPD, inflammatory polyarthropathies, and hypertension | [116] | ||
| HIV-infection | Higher GlycA levels in HIV-infected patients | [117] | |
| Chronic inflammatory diseases | RA | GlycA is higher in RA patients than in controls. | [83,118,119] |
| SLE | GlycA levels increased with each unit increase in SELDAI. | [120,121] | |
| GlycA has been shown to be a good marker of systemic inflammation in lupus-nephritis. | [122] | ||
| Psoriasis | GlycA is increased in psoriasis. | [123] | |
| IBD | GlycA in populations with ulcerative colitis and Chron’s disease better reflects inflammatory status than other classical markers. | [124] | |
| CKD | GlycA was independently associated with albuminuria and inversely related to eGFR. | [125] | |
| CHC | Increased severity of fibrosis has been associated with higher NAC plasma levels. | [126] | |
| Cognitive function and psychological health | Global cognitive function | GlycA is inversely related to global cognition, information processing speed and memory domains. | [127] |
| AD | Elevated circulating glycoproteins were associated with the risk for AD and MCI. | [128] | |
| Rare vascular diseases | Takayasu arteritis | N-Acetyl glycoproteins are significantly up-regulated in TA patients | [129,130] |
| Kawasaki disease | High levels of GlycA were confirmed in paediatric population with acute KD disease | [110] | |
| Primary aldosteronism | GlycA levels significantly increased in PA population. | [131] | |
| Sickle cell disease | GlycA levels are decreased in SCL. | [132] | |
| Human African Trypanosomiasis | Significant increase of N-acetyl glycoprotein in HAT patients. | [133] | |
| Clicical Study Topic | Main Findings | References | |
|---|---|---|---|
| Tobacco smoking | Similar significant associations between different measures of smoking behaviour and higher GlycA and hsCRP levels. | [134] | |
| Effect of exercise | Regular exercise significantly reduced plasma GlycA. | [135,136,137] | |
| Effect of treatments | Anti-TNF and monoclonal antibodies | Decrease in GlycA levels. | [122,123] |
| Antirretroviral treatment | GlycA was the only marker of inflammation, among hsCRP, IL-6 and D-dimer, that decreased. | [138] | |
| Statins | Do not affect GlycA levels. | [114] | |
| Metformin | Lower NAC serum levels in T2DM patients treated in metformin than in untreated patients. | [139] | |
| Probiotics | Greater gut microbiota richness is negatively linked with low-grade inflammation marker GlycA. | [86] | |
| Clinical Study Topic | Main Findings | References | |
|---|---|---|---|
| Sodium intake | Lower GlycA and hsCRP concentrations were both associated with higher 24-h sodium excretion. | [140] | |
| Pregnancy | Gradual increase in N-acetyl glycoproteins during pregnancy. | [141] | |
| Multiple nutrient intake correlates with GlycA including fibre, LC-PUFA and w-3 LC-PUFA and several vitamins and minerals. | [86] | ||
| GlycA and hsCRP were statistically significantly higher in obese than in overweight pregnant women. | [142] | ||
| Toxicity | Sodium valproate | N-acetyl moieties of glycoprotein significantly increased (p < 0.01) in valproate sodium induced hepatotoxicity | [143] |
| Oncologic toxicity | The high acute radiation sequelae were associated with increased signals of N-acetyl glycoproteins | [144] | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fuertes-Martín, R.; Correig, X.; Vallvé, J.-C.; Amigó, N. Title: Human Serum/Plasma Glycoprotein Analysis by 1H-NMR, an Emerging Method of Inflammatory Assessment. J. Clin. Med. 2020, 9, 354. https://doi.org/10.3390/jcm9020354
Fuertes-Martín R, Correig X, Vallvé J-C, Amigó N. Title: Human Serum/Plasma Glycoprotein Analysis by 1H-NMR, an Emerging Method of Inflammatory Assessment. Journal of Clinical Medicine. 2020; 9(2):354. https://doi.org/10.3390/jcm9020354
Chicago/Turabian StyleFuertes-Martín, Rocío, Xavier Correig, Joan-Carles Vallvé, and Núria Amigó. 2020. "Title: Human Serum/Plasma Glycoprotein Analysis by 1H-NMR, an Emerging Method of Inflammatory Assessment" Journal of Clinical Medicine 9, no. 2: 354. https://doi.org/10.3390/jcm9020354
APA StyleFuertes-Martín, R., Correig, X., Vallvé, J.-C., & Amigó, N. (2020). Title: Human Serum/Plasma Glycoprotein Analysis by 1H-NMR, an Emerging Method of Inflammatory Assessment. Journal of Clinical Medicine, 9(2), 354. https://doi.org/10.3390/jcm9020354