The Prospects of the Two-Day Cardiopulmonary Exercise Test (CPET) in ME/CFS Patients: A Meta-Analysis


Abstract
1. Introduction
2. Methods
2.1. Search Strategy, Inclusion and Exclusion Criteria
2.2. Data Extraction and Outcome Measures
2.3. Statistical Analysis
2.4. Assessment of Quality of Studies
3. Results
3.1. Characteristics of Included Studies
3.2. Comparisons of the Four Parameters
3.3. Outcomes of Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Osoba, T.; Pheby, D.; Gray, S.; Nacul, L. The Development of an Epidemiological Definition for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J. Chronic Fatigue Syndr. 2007, 14, 61–84. [Google Scholar]
- American ME and CFS Society. How Many People Have ME/CFS? American ME and CFS Society U.S. (U.S.): 2019. Available online: https://ammes.org/how-many-people-have-mecfs/ (accessed on 30 June 2019).
- Institute of Medicine of the National Academes. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome; Redefining an Illness; Committee on the Diagnostic Criteria for ME/CFS; Institute of Medicine: Washington, DC, USA; The National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Bethesda, M. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) Research. Workshop Report. In State of the Knowledge Workshop; National Institutes of Health (Maryland, U.S.): Bethesda, MD, USA, 2011. [Google Scholar]
- Devasahayam, A.; Lawn, T.; Murphy, M.; White, P.D. Alternative diagnoses to chronic fatigue syndrome in referrals to a specialist service: Service evaluation survey. JRSM Short Rep. 2012, 3, 4. [Google Scholar] [PubMed]
- Carruthers, B.M.; Jain, A.K.; De Meirleir, K.L.; Peterson, D.L.; Klimas, N.G.; Lerner, A.M.; Bested, A.C.; Flor-Henry, P.; Joshi, P.; Powles, A.P.; et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J. Chronic Fatigue Syndr. 2003, 11, 7–115. [Google Scholar]
- Food and Drug Administration (FDA). The Voice of the Patient: Chronic Fatigue Syndrome and Myalgic Encephalomyelitis; Center for Drug Evaluation and Research (CDER): Bethesda, MD, USA, 2013.
- Jason, L.A.; Porter, N.; Hunnell, J.; Brown, A.; Rademaker, A.; Richman, J.A. A natural history study of chronic fatigue syndrome. Rehabil. Psychol. 2011, 56, 32–42. [Google Scholar]
- Jason, L.A.; Sunnquist, M.; Brown, A.; Evans, M.; Vernon, S.D.; Furst, J.D.; Simonis, V. Examining case definition criteria for chronic fatigue syndrome and myalgic encephalomyelitis. Fatigue 2014, 2, 40–56. [Google Scholar]
- Van Ness, J.M.; Snell, C.R.; Stevens, S.R. Diminished Cardiopulmonary Capacity during Post-Exertional Malaise. J. Chronic Fatigue Syndr. 2007, 14, 77–85. [Google Scholar]
- Ella, A. Decoding the 2-Day Cardiopulmonary Exercise Test (CPET) in Chronic Fatigue Syndrome (ME/CFS). Health Rising Finding Answers for ME/CFS and FM. 2019. Available online: https://www.healthrising.org/blog/2019/01/17/decoding-2-day-cpet-chronic-fatigue-syndrome/ (accessed on 15 February 2020).
- McGregor, N.R.; Armstrong, C.W.; Lewis, D.P.; Gooley, P.R. Post-Exertional Malaise Is Associated with Hypermetabolism, Hypoacetylation and Purine Metabolism Deregulation in ME/CFS Cases. Diagn. (BaselSwitz.) 2019, 9, 70. [Google Scholar]
- Albouaini, K.; Egred, M.; Alahmar, A.; Wright, D.J. Cardiopulmonary exercise testing and its application. Postgrad. Med. J. 2007, 83, 675–682. [Google Scholar]
- Stevens, S.; Snell, C.; Stevens, J.; Keller, B.; VanNess, J.M. Cardiopulmonary Exercise Test Methodology for Assessing Exertion Intolerance in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Front. Pediatr. 2018, 6, 242. [Google Scholar]
- Bazelmans, E.; Bleijenberg, G.; Van Der Meer, J.W.; Folgering, H. Is physical deconditioning a perpetuating factor in chronic fatigue syndrome? A controlled study on maximal exercise performance and relations with fatigue, impairment and physical activity. Psychol. Med. 2001, 31, 107–114. [Google Scholar]
- Cook, D.B.; Nagelkirk, P.R.; Peckerman, A.; Poluri, A.; Lamanca, J.J.; Natelson, B.H. Perceived exertion in fatiguing illness: Civilians with chronic fatigue syndrome. Med. Sci. Sports Exerc. 2003, 35, 563–568. [Google Scholar] [PubMed]
- Cook, D.B.; Nagelkirk, P.R.; Peckerman, A.; Poluri, A.; Lamanca, J.J.; Natelson, B.H. Perceived exertion in fatiguing illness: Gulf War veterans with chronic fatigue syndrome. Med. Sci. Sports Exerc. 2003, 35, 569–574. [Google Scholar] [PubMed]
- Moneghetti, K.J.; Skhiri, M.; Contrepois, K.; Kobayashi, Y.; Maecker, H.; Davis, M.; Snyder, M.; Haddad, F.; Montoya, J.G. Value of Circulating Cytokine Profiling During Submaximal Exercise Testing in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Sci. Rep. 2018, 8, 2779. [Google Scholar] [PubMed]
- Vermeulen, R.C.W.; Kurk, R.M.; Visser, F.C.; Sluiter, W.; Scholte, H.R. Patients with chronic fatigue syndrome performed worse than controls in a controlled repeated exercise study despite a normal oxidative phosphorylation capacity. J. Transl. Med. 2010, 8, 93. [Google Scholar]
- Nelson, M.J.; Buckley, J.D.; Thomson, R.L.; Clark, D.; Kwiatek, R.; Davison, K. Diagnostic sensitivity of 2-day cardiopulmonary exercise testing in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J. Transl. Med. 2019, 17, 80. [Google Scholar]
- Myhill, S.; Booth, N.E.; McLaren-Howard, J. Chronic fatigue syndrome and mitochondrial dysfunction. Int. J. Clin. Exp. Med. 2009, 2, 1–16. [Google Scholar]
- Booth, N.E.; Myhill, S.; McLaren-Howard, J. Mitochondrial dysfunction and the pathophysiology of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Int. J. Clin. Exp. Med. 2012, 5, 208–220. [Google Scholar]
- Franklin, J.D.; Atkinson, G.; Atkinson, J.M.; Batterham, A.M. Peak oxygen uptake in chronic fatigue syndrome/myalgic encephalomyelitis: A meta-analysis. Int. J. Clin. Exp. Med. 2019, 40, 77–87. [Google Scholar]
- Jones, D.E.; Hollingsworth, K.G.; Jakovljevic, D.G.; Fattakhova, G.; Pairman, J.; Blamire, A.M.; Trenell, M.I.; Newton, J.L. Loss of capacity to recover from acidosis on repeat exercise in chronic fatigue syndrome: A case-control study. Eur. J. Clin. Investig. 2012, 42, 186–194. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar]
- The Cochrane Collaboration. Review Manager (RevMan); Computer program, Version 5.3; The Cochrane Collaboration: London, UK, 2020. [Google Scholar]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 20 June 2020).
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.P.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International Consensus Criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Snell, C.R.; Stevens, S.R.; Davenport, T.E.; Van Ness, J.M. Discriminative Validity of Metabolic and Workload Measurements for Identifying People with Chronic Fatigue Syndrome. Phys. Ther. 2013, 93, 1484–1492. [Google Scholar] [CrossRef] [PubMed]
- Hodges, L.D.; Nielsen, T.; Baken, D. Physiological measures in participants with chronic fatigue syndrome, multiple sclerosis and healthy controls following repeated exercise: A pilot study. Clin. Physiol. Funct. Imaging 2018, 38, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Spriet, L.L. Anaerobic metabolism during exercise. In Exercise Metabolism, 2nd ed.; Hargreaves, M., Spriet, L.L., Eds.; Human Kinetics: Champaign, IL, USA, 2006; pp. 7–27. [Google Scholar]
- Stephens, C. MEA Summary Review: The role of Mitochondria in ME/CFS; The ME Association: Buckinghamshire, UK, 12 July 2019; Available online: https://meassociation.org.uk/2019/07/mea-summary-review-the-role-of-mitochondria-in-me-cfs-13-july-2019/ (accessed on 10 July 2020).
- Tomas, C.; Brown, A.; Strassheim, V.; Elson, J.L.; Newton, J.; Manning, P. Cellular bioenergetics is impaired in patients with chronic fatigue syndrome. PLoS ONE. 2017, 12, e0186802. [Google Scholar] [CrossRef] [PubMed]
- Billing-Ross, P.; Germain, A.; Ye, K.; Keinan, A.; Gu, Z.; Hanson, M.R. Mitochondrial DNA variants correlate with symptoms in myalgic encephalomyelitis/chronic fatigue syndrome. J. Transl. Med. 2016, 14, 19. [Google Scholar] [CrossRef]
- Tomas, C.; Elson, J.L. The role of mitochondria in ME/CFS: A perspective. Fatigue Biomed. Health Behav. 2019, 7, 52–58. [Google Scholar] [CrossRef]
- Lawson, N.; Hsieh, C.-H.; March, D.; Wang, X. Elevated Energy Production in Chronic Fatigue Syndrome Patients. J. Nat. Sci. 2016, 2, e221. [Google Scholar]
- Rasa, S.; Nora-Krukle, Z.; Henning, N.; Eliassen, E.; Shikova, E.; Harrer, T.; Scheibenbogen, C.; Murovska, M.; Prusty, B.K. Chronic viral infections in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). J. Transl. Med. 2018, 16, 268. [Google Scholar] [CrossRef]
- Morris, G.; Maes, M. Mitochondrial dysfunctions in myalgic encephalomyelitis/chronic fatigue syndrome explained by activated immuno-inflammatory, oxidative and nitrosative stress pathways. Metab. Brain Dis. 2014, 29, 19–36. [Google Scholar] [CrossRef]
- Morris, G.; Stubbs, B.; Köhler, C.A.; Walder, K.; Slyepchenko, A.; Berk, M.; Carvalho, A.F. The putative role of oxidative stress and inflammation in the pathophysiology of sleep dysfunction across neuropsychiatric disorders: Focus on chronic fatigue syndrome, bipolar disorder and multiple sclerosis. Sleep Med. Rev. 2018, 41, 255–265. [Google Scholar] [CrossRef]
- Fluge, Ø.; Mella, O.; Bruland, O.; Risa, K.; Dyrstad, S.E.; Alme, K.; Rekeland, I.G.; Sapkota, D.; Røsland, G.V.; Fosså, A.; et al. Metabolic profiling indicates impaired pyruvate dehydrogenase function in myalgic encephalopathy/chronic fatigue syndrome. JCI Insight 2016, 1, e89376. [Google Scholar] [CrossRef] [PubMed]
- Koufaki, P.; Naish, P.F.; Mercer, T.H. Reproducibility of exercise tolerance in patients with end-stage renal disease. Arch. Phys. Med. Rehabil. 2001, 82, 1421–1424. [Google Scholar] [CrossRef] [PubMed]
- Selig, S.E.; Carey, M.F.; Menzies, D.G.; Patterson, J.; Geerling, R.H.; Williams, A.D.; Bamroongsuk, V.; Toia, D.; Krum, H.; Hare, D.L. Reliability of isokinetic strength and aerobic power testing for patients with chronic heart failure. J. Cardiopulm. Rehabil. 2002, 22, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Hansen, J.E.; Sun, X.G.; Yasunobu, Y.; Garafano, R.P.; Gates, G.; Barst, R.J.; Wasserman, K. Reproducibility of cardiopulmonary exercise measurements in patients with pulmonary arterial hypertension. Chest 2004, 126, 816–824. [Google Scholar] [CrossRef] [PubMed]
- Larson, B.; Davenport, T.E.; Stevens, S.R.; Van Ness, J.M.; Snell, C.R. Reproducibility of measurements obtained during cardiopulmonary exercise testing in individuals with and without fatiguing health conditions: A case series. Cardiopulm. Phys. Ther. J. 2019, 30, 145–152. [Google Scholar] [CrossRef]
- Keller, B.A.; Pryor, J.L.; Giloteaux, L. Inability of myalgic encephalomyelitis/chronic fatigue syndrome patients to reproduce VO2peak indicates functional impairment. J. Transl. Med. 2014, 12, 104. [Google Scholar] [CrossRef] [PubMed]
- van Campen, C.; Rowe, P.; Visser, F. Validity of 2-Day Cardiopulmonary Exercise Testing in Male Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Adv. Phys. Educ. 2020, 10, 68–80. [Google Scholar] [CrossRef][Green Version]
- Naviaux, R.K.; Naviaux, J.C.; Li, K.; Bright, A.T.; Alaynick, W.A.; Wang, L.; Baxter, A.; Nathan, N.; Anderson, W.; Gordon, E. Metabolic features of chronic fatigue syndrome. Proc. Natl. Acad. Sci. USA 2016, 113, E5472–E5480. [Google Scholar] [CrossRef]
- Esfandyarpour, R.; Kashi, A.; Nemat-Gorgani, M.; Wilhelmy, J.; Davis, R.W. A nanoelectronics-blood-based diagnostic biomarker for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Proc. Natl. Acad. Sci. USA 2019, 116, 10250–10257. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ME/CFS + | Control | Newcastle Ottawa Scale § | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| S | C | E | ||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |||
| No. of studies | 5 | 5 | ||||||||
| No. of participants (Female/Male) | 98 (90/8) | 51 (45/6) | ||||||||
| Age (y) # | 42.3 ± 11.6 | 41.3 ± 12.4 | ||||||||
| BMI (kg/m2) # | 25.3 ± 4.8 | 25.6 ± 4.2 | ||||||||
| Selection of participants | ||||||||||
| ME/CFS | Control | |||||||||
| Van Ness (2007) [10] | Physician diagnosis and Fukuda | Healthy sedentary | * | * | * | * | * | * | * | * |
| Vermeulen (2010) [19] | CDC-SI 59.5 ± 13.1 ‡ Fukuda, infectious disease onset | CDC-SI 5.0 ± 4.5 | * | * | * | * | * | * | * | * |
| Snell (2013) [29] | Sedentary ※ Fukuda, Presence of PEM | Sedentary ※ | * | * | * | * | * | * | * | * |
| Hodges (2017) [30] | Fukuda, (CCC and ICC) α De Paul Questionnaire, SF-36 | Healthy | * | * | - | - | * | * | * | * |
| Nelson (2019) [20] | Sedentary † Physician diagnosis Fukuda/(CCC/ICC) α | Sedentary † | * | * | * | * | * | * | * | * |
| # | Study | Participants (Patients/ Controls) | VO2peak | VO2@VT | Workloadpeak | Workload@VT |
|---|---|---|---|---|---|---|
| Test 1/Test 2 (T2-T1) | Test 1/Test 2 (T2-T1) | Test 1/Test 2 (T2-T1) | Test 1/Test 2 (T2-T1) | |||
| (mL kg−1 min−1) | (mL kg−1 min−1) | (Watt) | (Watt) | |||
| 1 | Van Ness (2007) [10] | 6(F) 6(F) | 26.2 ± 4.9/20.5 ± 1.8 (−5.8) 28.4 ± 7.2/28.9 ± 8.0 (+0.5) | 15.0 ± 4.9/11.0 ± 3.4 (−4.0) 17.6 ± 4.9/18.0 ± 5.3 (+0.4) | - - | - - |
| 2 | Vermeulen (2010) [19] | 15(F) 15(F) | 22.3 ± 5.7/20.9 ± 5.5 (−1.3) 31.2 ± 7.0/31.9 ± 7.4 (+0.7) | 12.8 ± 3.0/11.9 ± 2.9 (−0.9) 16.7 ± 4.0/18.0 ± 4.6 (+1.3) | 132.0 ± 30.0/125.0 ± 35.0 (−7.0) 188.0 ± 46.0/196.0 ± 51.0 (+8.0) | 58.6 ± 24.2/54.5 ± 20.9 (−4.1) 82.9 ± 29.1/92.9 ± 31.4 (+10.0) |
| 3 | Snell (2013) [29] | 51(F) 10(F) | 21.5 ± 4.1/20.4 ± 4.5 (−1.1) 25.0 ± 4.4/24.0 ± 4.3 (−1.0) | 12.7 ± 2.9/11.4 ± 2.9 (−1.3) 13.8 ± 2.8/14.1 ± 3.3 (+0.3) | 109.6 ± 28.9/101.6 ± 30.7 (−8.0) 137.2 ± 23.2/140.0 ± 25.0 (+2.8) | 49.5 ± 20.4/22.2 ± 18.1 (−27.3) 58.0 ± 16.7/63.5 ± 19.5 (+5.5) |
| 4 | Hodges (2017) [30] | 9(F)/1(M) 9(F)/1(M) | 25.0 ± 8.9/26.3 ± 7.8 (+1.3) 32.0 ± 10.9/33.1 ± 12.5 (+1.1) | 21.0 ± 4.3/22.2 ± 6.2 (+1.2) 23.6 ± 9.0/28.5 ± 12.5 (+4.9) | 135.0 ± 43.0/126.0 ± 45.0 (−9.0) 164.0 ± 40.0/167.0 ± 41.0 (+3.0) | 105.0 ± 30.0/93.0 ± 37.0 (−12.0) 119.0 ± 28.0/132.0 ± 42.0 (+13.0) |
| 5 | Nelson (2019) [20] | 9(F)/7(M) 5(F)/5(M) | 27.3 ± 9.2/27.4 ± 8.8 (+0.1) 29.9 ± 6.1/30.3 ± 6.2 (+0.4) | 15.9 ± 4.1/15.4 ± 3.4 (−0.5) 16.5 ± 2.0/15.9 ± 1.5 (−0.6) | 154.4 ± 56.0/152.5 ± 51.7 (−1.9) 172.0 ± 35.5/174.0 ± 36.6 (+2.0) | 87.8 ± 29.6/72.5 ± 27.7 (−15.3) 90.5 ± 17.1/88.0 ± 16.7 (−2.5) |
| Total 90(F)/8(M) 45(F)/6(M) | 24.5 ± 6.6/23.1 ± 5.7 (−1.4) 29.3 ± 7.1/29.6 ± 7.7 (+0.3) | 15.5 ± 3.8/14.4 ± 3.8 (−1.1) 17.6 ± 4.5/18.9 ± 5.4 (+1.3) | 132.8 ± 39.5/126.3 ± 40.6 (−6.5) 165.3 ± 36.2/169.3 ± 38.4 (+4.0) | 75.2 ± 26.1/60.6 ± 25.9 (−14.6) 87.6 ± 22.7/94.1 ± 27.4 (+6.5) | ||
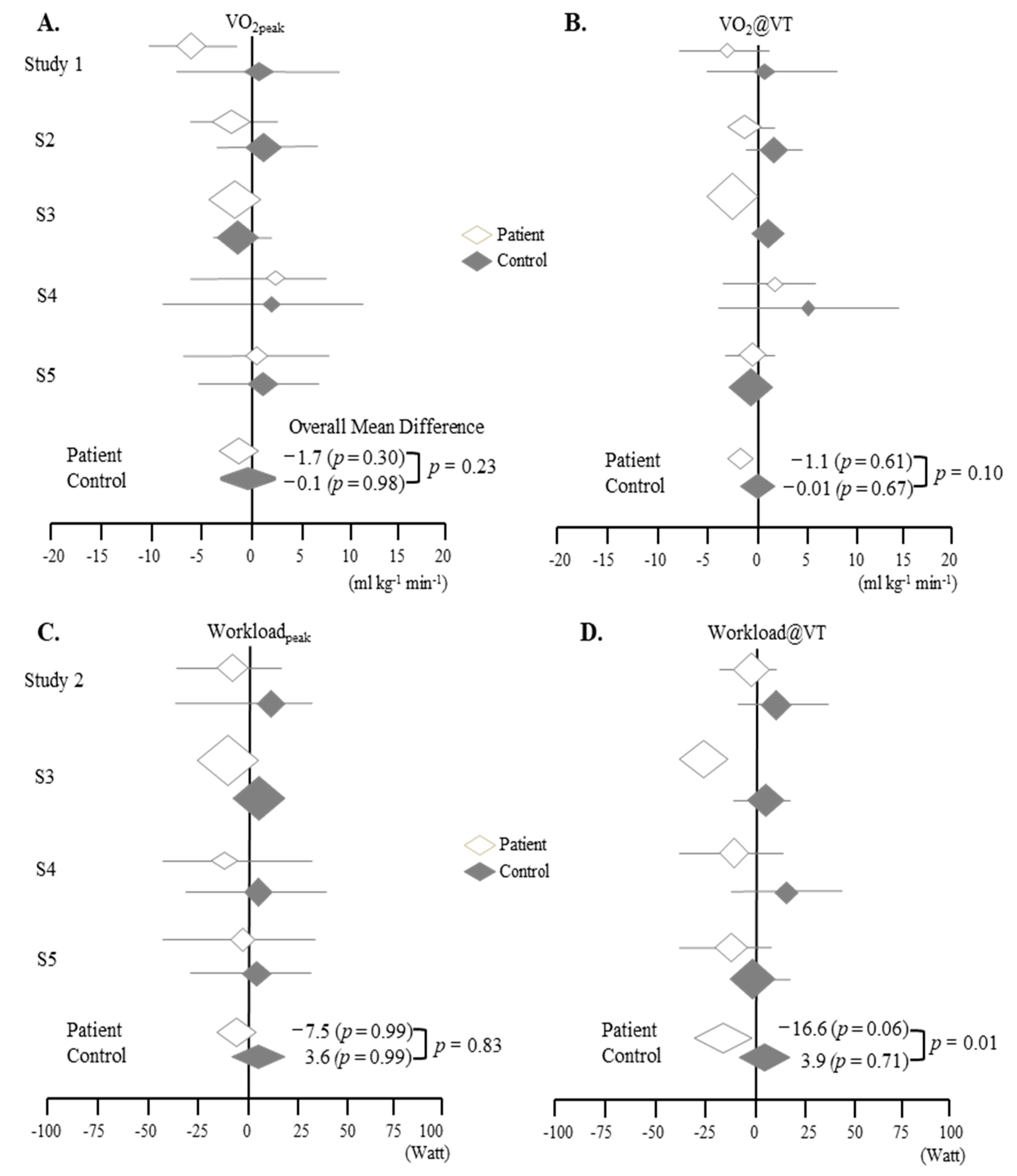
| # | Study | Weight (%) | Mean Difference | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| VO2peak | @VT | WLpeak | @VT | VO2peak | @VT | WLpeak | @VT | |||
| 1 | Van Ness (2007) [10] | P | 16 | 3.5 | - | - | −5.7 (−1.5, −9.9) | −4.0 (0.8, −8.8) | - | - |
| C | 8.2 | 4.3 | - | - | 0.5 (9.1, −8.1) | 0.4 (6.2, −5.4) | - | - | ||
| 2 | Vermeulen (2010) [19] | P | 17.1 | 17.9 | 17.2 | 26.2 | −0.9 (1.2, −3.0) | −1.4 (2.6, −5.4) | −7.0 (16.3, −30.3) | −4.1 (12.1, −20.3) |
| C | 23.0 | 15.0 | 17.0 | 18.4 | 0.7 (5.9, −4.5) | 1.3 (4.4, −1.8) | 8.0 (42.8, −26.8) | 10.0 (31.6, −11.6) | ||
| 3 | Snell (2013) [29] | P | 53.1 | 63.1 | 69.8 | 38.6 | −1.1 (0.6, −2.8) | −1.3 ( −0.2, −2.4) | −8.0 (3.6, −19.6) | −27.3 (−19.8, −34.8) |
| C | 42.0 | 19.8 | 46.0 | 33.8 | −1.0 (2.8, −4.8) | 0.3 (3.0, −2.4) | 2.8 (23.9, −18.3) | 5.5 (21.4, −10.4) | ||
| 4 | Hodges (2017) [30] | P | 5.9 | 3.7 | 6.3 | 13.4 | 1.3 (8.6, −6.0) | 1.2 (5.9, −3.5) | −9.0 (29.6, −47.6) | −12.0 (17.5, −41.5) |
| C | 5.8 | 1.6 | 16.3 | 8.7 | 1.1 (11.4, −9.2) | 4.9 (14.5, −4.7) | 3.0 (38.5, −32.5) | 13.0 (44.3, −18.3) | ||
| 5 | Nelson (2019) [20] | P | 7.9 | 11.7 | 6.7 | 21.7 | 0.1 (6.3, −6.1) | −0.5 (2.1, −3.1) | −1.9 (35.5, −39.3) | −15.3 (4.6, −35.2) |
| C | 21.0 | 59.4 | 20.6 | 39.0 | 0.4 (5.8, −5.0) | −0.6 (1.0, −2.2) | 2.0 (33.6, −29.6) | −2.5 (12.3, −17.3) | ||
| Overall values for P Heterogeneity (I2) p value | 19% 0.30 | 0 0.61 | 0% 0.99 | 60% 0.06 | −1.7 (0.2, −3.5) | −1.1 (−0.2, −2.0) | −7.5 (2.2, −17.2) | −16.6 (−3.6, −29.5) | ||
| Overall values for C Heterogeneity (I2) p value | 0% 0.98 | 0% 0.67 | 0% 0.99 | 0% 0.71 | −0.1 (2.4, −2.5) | −0.01 (1.2, −1.2) | 3.6 (17.9, −10.8) | 3.9 (13.1, −5.4) | ||
| P vs. C p value | 0.23 | 0.10 | 0.83 | 0.01 ** | ||||||
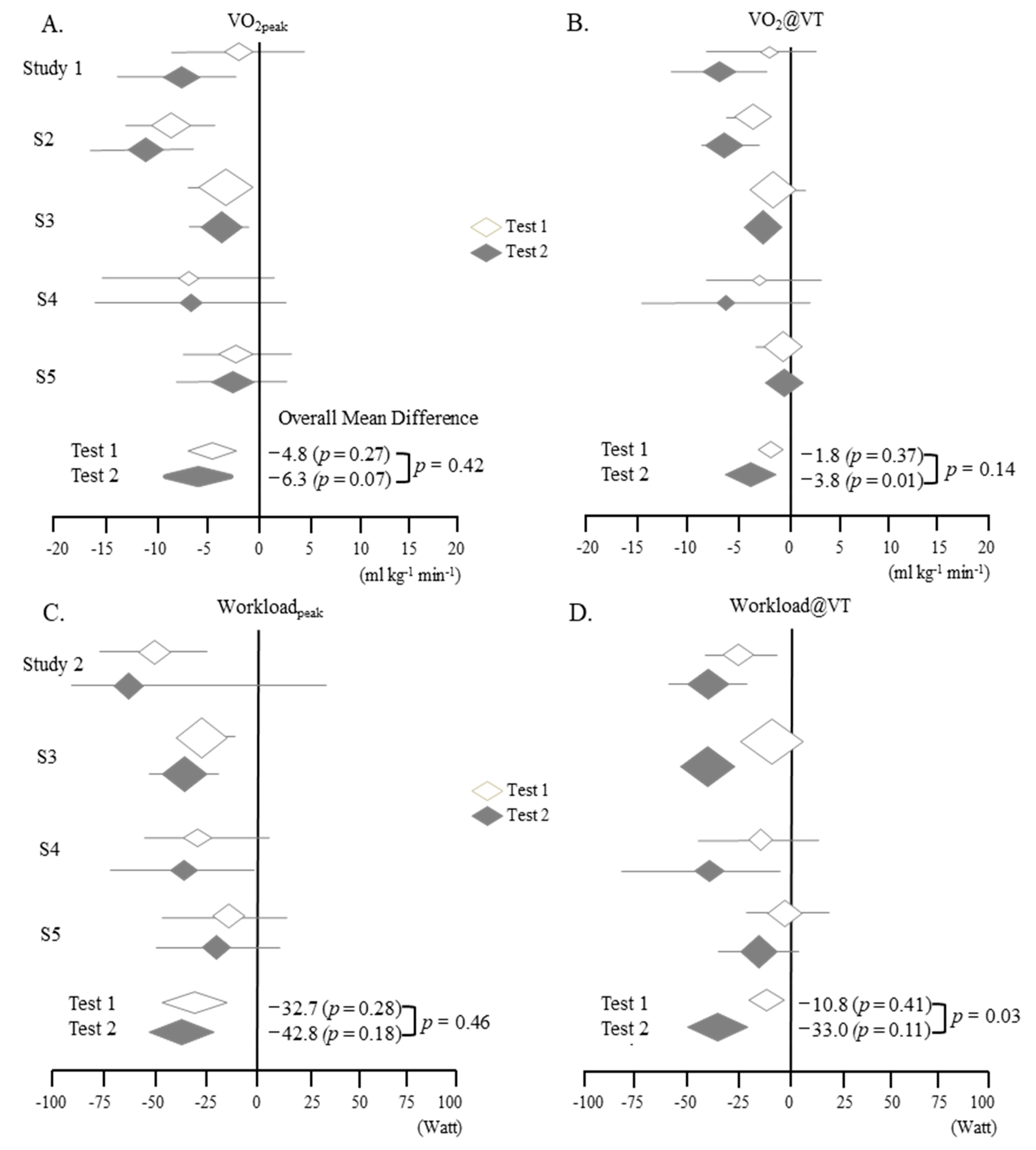
| # | Study | Weight (%) | Mean Difference | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| VO2peak | @VT | WLpeak | @VT | VO2peak | @VT | WLpeak | @VT | |||
| 1 | VanNess (2007) [19] | T1 | 11.9 | 5.4 | - | - | −2.2 (−9.2, 4.8) | −2.6 (−8.1, 2.9) | - | - |
| T2 | 16.4 | 15 | - | - | −8.4 (−14.7, −1.8) | −7.0 (−12.0, −2.0) | - | - | ||
| 2 | Vermeulen (2010) [19] | T1 | 23.4 | 23.9 | 22.8 | 18.7 | −8.9 (−13.37, −4.3) | −3.9 (−6.4, −1.4) | −56.0 (−83.79, −28.2) | −24.3 (−43.5, −5.2) |
| T2 | 23.1 | 23.9 | 22.3 | 25.5 | −11.0 (−15.7, −6.3) | −6.1 (−8.9, −3.4) | −71.0 (−102.3, 39.7) | −38.4 (−57.4, −19.4) | ||
| 3 | Snell (2013) [29] | T1 | 41.0 | 39.3 | 47.2 | 49.5 | −3.5 (−6.5, −0.6) | −1.1 (−3.0, 0.8) | −27.6 (−44.0, −11.2) | −8.5 (−20.3, 3.3) |
| T2 | 31.0 | 26.3 | 40.5 | 34.8 | −3.6 (−6.5, −0.7) | −2.7 (−4.9, −0.5) | −38.4 (−56.0, −20.8) | −41.3 (−54.4, −28.2) | ||
| 4 | Hodges (2017) [30] | T1 | 8.0 | 4.3 | 14.6 | 10.6 | −7.0 (−15.7, 1.7) | −2.6 (−8.8, 3.6) | −29.0 (−65.4, 7.4) | −14.0 (−39.4, 11.4) |
| T2 | 10.5 | 7.4 | 17.2 | 11.6 | −6.8 (−15.9, 2.3) | −6.3 (−15.0, 2.4) | −41.0 (−78.7, −3.3) | −39.0 (−73.7, −4.3) | ||
| 5 | Nelson (2019) [20] | T1 | 15.8 | 27.1 | 15.4 | 21.2 | −2.6 (−8.5, 3.3) | −0.6 (−3.0, 1.8) | −17.6 (−52.8, 17.6) | −2.7 (−20.7, 15.3) |
| T2 | 18.9 | 27.4 | 20.0 | 28.2 | −2.9 (−8.7, 2.9) | −0.5 (−2.4, 1.4) | −21.5 (−55.5, 12.5) | −15.5 (−32.6, 1.6) | ||
| Overall values for T1 Heterogeneity (I2) T1 p value | 22% 0.27 | 7% 0.37 | 21% 0.28 | 0% 0.41 | −4.8 (−7.3, −2.2) | −1.8 (−3.1, −0.5) | −3–32.7 (−47.6, −17.8) | −10.8 (−19.1, −2.5) | ||
| Overall values for T2 Heterogeneity (I2) T2 p value | 53% 0.07 | 72% 0.01** | 38% 0.18 | 50% 0.11 | −6.3 (−9.8, −2.9) | −3.8 (−6.5, −1.1) | −42.8 (−61.0, −24.5) | −33.0 (−46.4, −19.6) | ||
| T1 vs. T2 p value | 0.42 | 0.14 | 0.46 | 0.03 * | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, E.-J.; Kang, E.-B.; Jang, E.-S.; Son, C.-G. The Prospects of the Two-Day Cardiopulmonary Exercise Test (CPET) in ME/CFS Patients: A Meta-Analysis. J. Clin. Med. 2020, 9, 4040. https://doi.org/10.3390/jcm9124040
Lim E-J, Kang E-B, Jang E-S, Son C-G. The Prospects of the Two-Day Cardiopulmonary Exercise Test (CPET) in ME/CFS Patients: A Meta-Analysis. Journal of Clinical Medicine. 2020; 9(12):4040. https://doi.org/10.3390/jcm9124040
Chicago/Turabian StyleLim, Eun-Jin, Eun-Bum Kang, Eun-Su Jang, and Chang-Gue Son. 2020. "The Prospects of the Two-Day Cardiopulmonary Exercise Test (CPET) in ME/CFS Patients: A Meta-Analysis" Journal of Clinical Medicine 9, no. 12: 4040. https://doi.org/10.3390/jcm9124040
APA StyleLim, E.-J., Kang, E.-B., Jang, E.-S., & Son, C.-G. (2020). The Prospects of the Two-Day Cardiopulmonary Exercise Test (CPET) in ME/CFS Patients: A Meta-Analysis. Journal of Clinical Medicine, 9(12), 4040. https://doi.org/10.3390/jcm9124040