Antihypertensive Treatment in Kidney Transplant Recipients—A Current Single Center Experience

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Blood Pressure Monitoring and Antihypertensive Medication
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Clinical Characteristics of Patients and the Use of Antihypertensive Agents
3.3. Blood Pressure and Renal Allograft Function
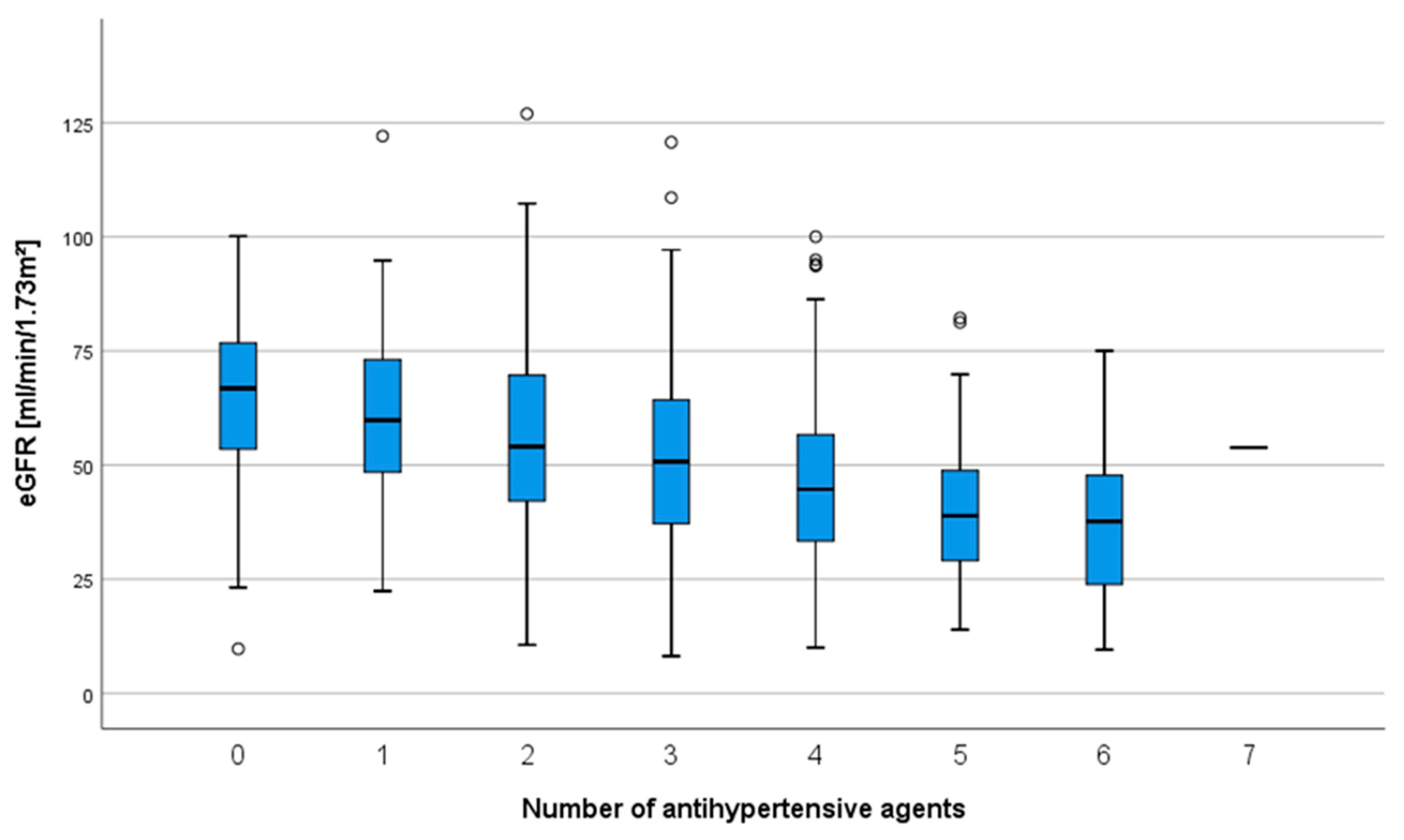
3.4. Renal Allograft Function and Number of Antihypertensive Agents
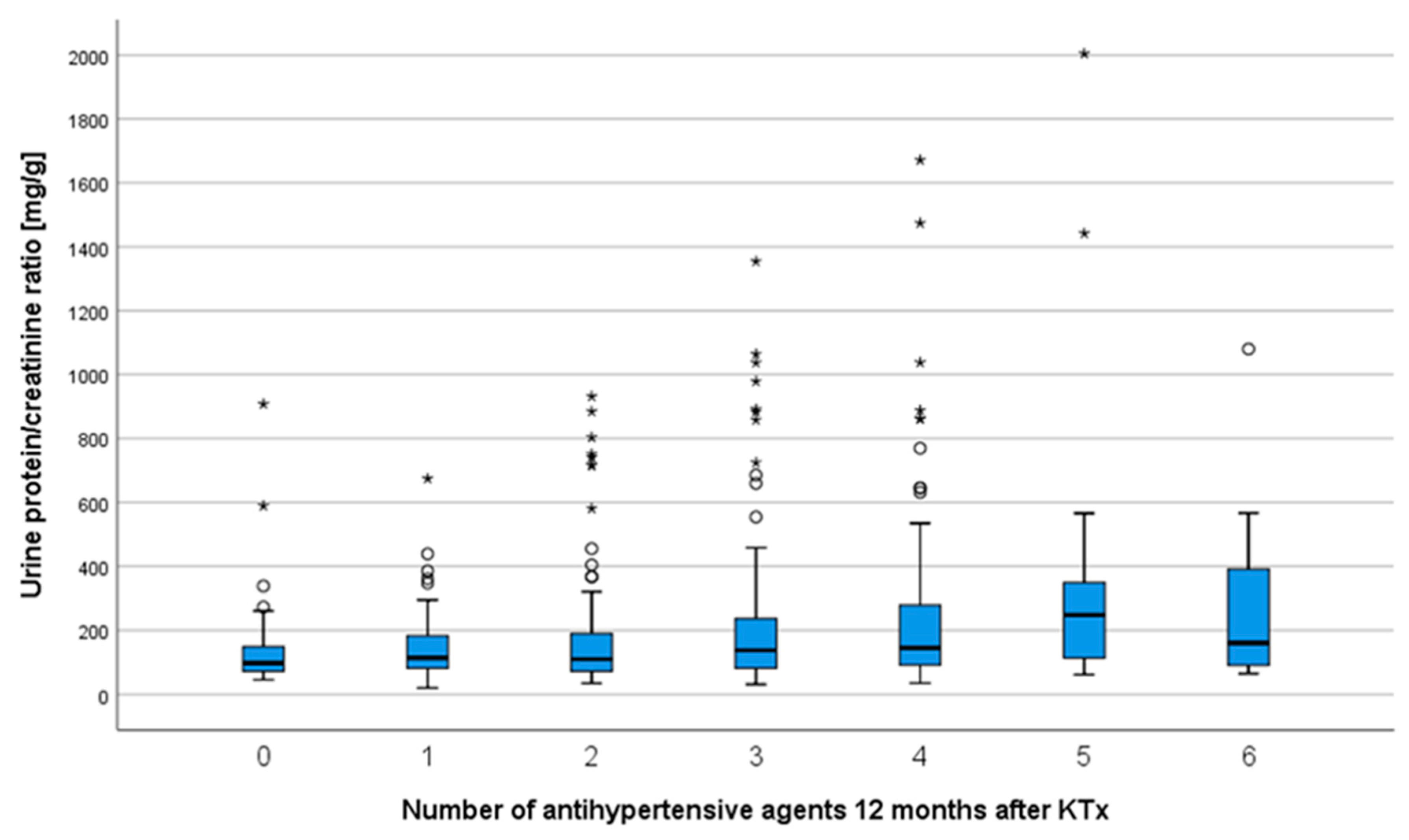
3.5. Antihypertensive Agents and Renal Allograft Function
3.6. Antihypertensive Agents and Allograft Survival
3.7. The Number of Antihypertensive Drugs as Indicator for Death-Censored Kidney Allograft Failure
3.8. The Development of Kidney Function as a Function of the Number of Antihypertensive Drugs
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Matas, A.J.; Gillingham, K.J.; Humar, A.; Kandaswamy, R.; Sutherland, D.E.R.; Payne, W.D.; Dunn, T.B.; Najarian, J.S. 2202 kidney transplant recipients with 10 years of graft function: What happens next? Am. J. Transplant. 2008, 8, 2410–2419. [Google Scholar] [CrossRef]
- Weir, M.R.; Burgess, E.D.; Cooper, J.E.; Fenves, A.Z.; Goldsmith, D.; McKay, D.; Mehrotra, A.; Mitsnefes, M.M.; Sica, D.A.; Taler, S.J. Assessment and management of hypertension in transplant patients. J. Am. Soc. Nephrol. 2015, 26, 1248–1260. [Google Scholar] [CrossRef]
- Opelz, G.; Wujciak, T.; Ritz, E. Association of chronic kidney graft failure with recipient blood pressure. Collab. Transpl. Study Kidney Int. 1998, 53, 217–222. [Google Scholar] [CrossRef]
- Wright, J.T.; Williamson, J.D.; Whelton, P.K.; Snyder, J.K.; Sink, K.M.; Rocco, M.V.; Reboussin, D.M.; Rahman, M.; Oparil, S.; Lewis, C.E.; et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N. Engl. J. Med. 2015, 373, 2103–2116. [Google Scholar] [CrossRef]
- Malhotra, R.; Katz, R.; Weiner, D.E.; Levey, A.S.; Cheung, A.K.; Bostom, A.G.; Ix, J.H. Blood Pressure, Chronic Kidney Disease Progression, and Kidney Allograft Failure in Kidney Transplant Recipients: A Secondary Analysis of the FAVORIT Trial. Am. J. Hypertens. 2019, 32, 816–823. [Google Scholar] [CrossRef]
- Chatzikyrkou, C.; Menne, J.; Gwinner, W.; Schmidt, B.M.; Lehner, F.; Blume, C.; Schwarz, A.; Haller, H.; Schiffer, M. Pathogenesis and management of hypertension after kidney transplantation. J. Hypertens. 2011, 29, 2283–2294. [Google Scholar] [CrossRef]
- Miller, L.W. Cardiovascular toxicities of immunosuppressive agents. Am. J. Transpl. 2002, 2, 807–818. [Google Scholar] [CrossRef]
- Agarwal, R.; Alborzi, P.; Satyan, S.; Light, R.P. Dry-weight reduction in hypertensive hemodialysis patients (DRIP): A randomized, controlled trial. Hypertension 2009, 53, 500–507. [Google Scholar] [CrossRef]
- Hamrahian, S.M.; Falkner, B. Hypertension in Chronic Kidney Disease. Adv. Exp. Med. Biol. 2017, 956, 307–325. [Google Scholar] [CrossRef]
- Bruno, S.; Remuzzi, G.; Ruggenenti, P. Transplant renal artery stenosis. J. Am. Soc. Nephrol. 2004, 15, 134–141. [Google Scholar] [CrossRef]
- Hricik, D.E. Metabolic syndrome in kidney transplantation: Management of risk factors. Clin. J. Am. Soc. Nephrol. 2011, 6, 1781–1785. [Google Scholar] [CrossRef]
- Aziz, F.; Clark, D.; Garg, N.; Mandelbrot, D.; Djamali, A. Hypertension guidelines: How do they apply to kidney transplant recipients. Transpl. Rev. 2018, 32, 225–233. [Google Scholar] [CrossRef]
- Kuźmiuk-Glembin, I.; Adrych, D.; Tylicki, L.; Heleniak, Z.; Garnier, H.; Wiśniewski, J.; Rutkowski, P.; Rutkowski, B.; Dębska-Ślizień, A. Treatment of Hypertension in Renal Transplant Recipients in Four Independent Cross-Sectional Analyses. Kidney Blood Press. Res. 2018, 43, 45–54. [Google Scholar] [CrossRef]
- The GISEN Group (Gruppo Italiano di Studi Epidemiologici in Nefrologia). Randomised placebo-controlled trial of effect of ramipril on decline in glomerular filtration rate and risk of terminal renal failure in proteinuric, non-diabetic nephropathy. Lancet 1997, 349, 1857–1863. [Google Scholar] [CrossRef]
- Brenner, B.M.; Cooper, M.E.; de Zeeuw, D.; Keane, W.F.; Mitch, W.E.; Parving, H.H.; Remuzzi, G.; Snapinn, S.M.; Zhang, Z.; Shahinfar, S. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N. Engl. J. Med. 2001, 345, 861–869. [Google Scholar] [CrossRef]
- Hillebrand, U.; Suwelack, B.M.; Loley, K.; Lang, D.; Reuter, S.; Amler, S.; Pavenstädt, H.; Hausberg, M.; Büssemaker, E. Blood pressure, antihypertensive treatment, and graft survival in kidney transplant patients. Transpl. Int. 2009, 22, 1073–1080. [Google Scholar] [CrossRef]
- Pisano, A.; Bolignano, D.; Mallamaci, F.; D’Arrigo, G.; Halimi, J.-M.; Persu, A.; Wuerzner, G.; Sarafidis, P.; Watschinger, B.; Burnier, M.; et al. Comparative effectiveness of different antihypertensive agents in kidney transplantation: A systematic review and meta-analysis. Nephrol. Dial. Transpl. 2020, 35, 878–887. [Google Scholar] [CrossRef]
- Ananthapanyasut, W.; Napan, S.; Rudolph, E.H.; Harindhanavudhi, T.; Ayash, H.; Guglielmi, K.E.; Lerma, E.V. Prevalence of atrial fibrillation and its predictors in nondialysis patients with chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2010, 5, 173–181. [Google Scholar] [CrossRef]
- Ojo, A.O. Cardiovascular complications after renal transplantation and their prevention. Transplantation 2006, 82, 603–611. [Google Scholar] [CrossRef]
- Sandal, S.; Bansal, P.; Cantarovich, M. The evidence and rationale for the perioperative use of loop diuretics during kidney transplantation: A comprehensive review. Transpl. Rev. 2018, 32, 92–101. [Google Scholar] [CrossRef]
- Ying, T.; Shi, B.; Kelly, P.J.; Pilmore, H.; Clayton, P.A.; Chadban, S.J. Death after Kidney Transplantation: An Analysis by Era and Time Post-Transplant. J. Am. Soc. Nephrol. 2020. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redón, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; de Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J. Hypertens. 2013, 31, 1281–1357. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Cox, D.R. Regression Models and Life-Tables. J. R. Stat. Soc. Ser. B Methodol. 1972, 34, 187–202. [Google Scholar] [CrossRef]
- Taler, S.J.; Agarwal, R.; Bakris, G.L.; Flynn, J.T.; Nilsson, P.M.; Rahman, M.; Sanders, P.W.; Textor, S.C.; Weir, M.R.; Townsend, R.R. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for management of blood pressure in CKD. Am. J. Kidney Dis. 2013, 62, 201–213. [Google Scholar] [CrossRef]
- Woźniak, I.; Kolonko, A.; Chudek, J.; Nowak, Ł.; Farnik, M.; Więcek, A. Influence of Polypharmacy on the Quality of Life in Stable Kidney Transplant Recipients. Transpl. Proc. 2018, 50, 1896–1899. [Google Scholar] [CrossRef] [PubMed]
- Bril, F.; Castro, V.; Centurion, I.G.; Espinosa, J.; Keller, G.A.; Gonzalez, C.D.; Riera, M.C.S.; Saubidet, C.L.; Di Girolamo, G.; Pujol, G.S.; et al. A Systematic Approach to Assess the Burden of Drug Interactions in Adult Kidney Transplant Patients. Curr. Drug Saf. 2016, 11, 156–163. [Google Scholar] [CrossRef]
- Nevins, T.E.; Nickerson, P.W.; Dew, M.A. Understanding Medication Nonadherence after Kidney Transplant. J. Am. Soc. Nephrol. 2017, 28, 2290–2301. [Google Scholar] [CrossRef]
- Ishikawa, S.; Naito, S.; Iimori, S.; Takahashi, D.; Zeniya, M.; Sato, H.; Nomura, N.; Sohara, E.; Okado, T.; Uchida, S.; et al. Loop diuretics are associated with greater risk of sarcopenia in patients with non-dialysis-dependent chronic kidney disease. PLoS ONE 2018, 13, e0192990. [Google Scholar] [CrossRef]
- Aomatsu, A.; Ookawara, S.; Ishibashi, K.; Morishita, Y. Protective Effects of Diuretics Against the Development of Cardiovascular Disease in Patients with Chronic Kidney Disease: A Systematic Review. Cardiovasc. Hematol. Agents Med. Chem. 2018, 16, 12–19. [Google Scholar] [CrossRef]
- Sibbel, S.; Walker, A.G.; Colson, C.; Tentori, F.; Brunelli, S.M.; Flythe, J. Association of Continuation of Loop Diuretics at Hemodialysis Initiation with Clinical Outcomes. Clin. J. Am. Soc. Nephrol. 2019, 14, 95–102. [Google Scholar] [CrossRef]
- Patschan, D.; Patschan, S.; Buschmann, I.; Ritter, O. Loop Diuretics in Acute Kidney Injury Prevention, Therapy, and Risk Stratification. Kidney Blood Press. Res. 2019, 44, 457–464. [Google Scholar] [CrossRef]
- Cross, N.B.; Webster, A.C.; Masson, P.; OʼConnell, P.J.; Craig, J.C. Antihypertensives for Kidney Transplant Recipients: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Transplantation 2009, 88, 7–18. [Google Scholar] [CrossRef]
- Agodoa, L.Y.; Appel, L.; Bakris, G.L.; Beck, G.; Bourgoignie, J.; Briggs, J.P.; Charleston, J.; Cheek, D.; Cleveland, W.; Douglas, J.G.; et al. Effect of ramipril vs amlodipine on renal outcomes in hypertensive nephrosclerosis: A randomized controlled trial. JAMA 2001, 285, 2719–2728. [Google Scholar] [CrossRef]
- Suwelack, B.; Kobelt, V.; Erfmann, M.; Hausberg, M.; Gerhardt, U.; Rahn, K.-H.; Hohage, H. Long-term follow-up of ACE-inhibitor versus beta-blocker treatment and their effects on blood pressure and kidney function in renal transplant recipients. Transpl. Int. 2003, 16, 313–320. [Google Scholar] [CrossRef]
- Hiremath, S.; Fergusson, D.; Doucette, S.; Mulay, A.V.; Knoll, G.A. Renin Angiotensin System Blockade in Kidney Transplantation: A Systematic Review of the Evidence. Am. J. Transpl. 2007, 7, 2350–2360. [Google Scholar] [CrossRef]
- Rigatto, C.; Parfrey, P.; Foley, R.; Negrijn, C.; Tribula, C.; Jeffery, J. Congestive heart failure in renal transplant recipients: Risk factors, outcomes, and relationship with ischemic heart disease. J. Am. Soc. Nephrol. 2002, 13, 1084–1090. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variable | All | No Antihypertensive Medication * | 1–2 Antihypertensive Drugs * | 3–4 Antihypertensive Drugs * | 5+ Antihypertensive Drugs * | p Value |
|---|---|---|---|---|---|---|
| Patients (n) | 850 | 40 (4.7%) | 330 (38.6%) | 325 (38.0%) | 70 (8.1%) | |
| Age at KTx * (years) | 52.9 ± 14.2 | 41.7 ± 13.2 | 49.8 ± 13.9 | 55.2 ± 13.3 | 59.3 ± 11.6 | <0.001 a |
| Sex, male (n) | 521 (61.0%) | 14 (35.0%) | 191 (58.1%) | 203 (62.3%) | 53 (75.7%) | |
| Mismatch-HLA-A | 0.582 b | |||||
| none | 297 (34.8%) | 12 (30.0%) | 122 (37.1%)\ | 112 (34.4%) | 21 (30.0%) | |
| 1 | 402 (47.1%) | 23 (57.5%) | 147 (44.7%) | 158 (48.5%) | 32 (45.7%) | |
| 2 | 148 (17.3%) | 5 (12.5%) | 59 (17.9%) | 52 (16.0%) | 16 (22.9%) | |
| Mismatch-HLA-B | 0.852 b | |||||
| none | 189 (22.1%) | 7 (17.5%) | 70 (21.3%) | 46 (23.3%) | 16 (22.9%) | |
| 1 | 404 (47.7%) | 19 (47.5%) | 168 (51.1%) | 149 (45.7%) | 32 (45.7%) | |
| 2 | 251 (29.4%) | 14 (35.0%) | 90 (27.4%) | 97 (29.8%) | 21 (30.0%) | |
| mismatch-HLA-DR | 0.012 b | |||||
| none | 221 (25.9%) | 8 (20.0%) | 75 (22.8%) | 94 (28.8%) | 23 (32.9%) | |
| 1 | 397 (46.5%) | 22 (55.0%) | 173 (52.6%) | 150 (46.0%) | 20 (28.6%) | |
| 2 | 229 (26.8%) | 10 (25.0%) | 80 (24.3%) | 78 (23.9%) | 26 (37.1%) | |
| PRA% | 5.4 ± 17.7 | 5.7 ± 16.8 | 6.2 ± 19.5 | 5.2 ± 17.0 | 1.5 ± 8.9 | 0.165 a |
| Living donor Tx * (n) | 230 (26.9%) | 22 (55.0%) | 125 (38.0%) | 66 (20.2%) | 9 (12.9%) | <0.001 b |
| Cold ischemia time (hours) | 8.7 ± 5.2 | 5.8 ± 4.5 | 8.0 ± 5.3 | 9.2 ± 5.0 | 9.5 ± 5.0 | <0.001 a |
| Dialysis prior to Tx * (n) | 795 (93.1%) | 34 (85.0%) | 296 (90.0%) | 314 (96.3%) | 67 (95.7%) | 0.001 b |
| Previous Tx* (n) | 113 (13.2%) | 6 (15.0%) | 46 (14.0%) | 43 (13.2%) | 4 (5.7%) | 0.346 b |
| CMV mismatch D/R | 0.130 c | |||||
| D−/R- | 142 (16.6%) | 9 (22.5%) | 68 (20.7%) | 39 (12.0%) | 11 (15.7%) | |
| D−/R+ | 147 (17.2%) | 6 (15.0%) | 54 (16.4%) | 62 (19.0%) | 9 (12.9%) | |
| D+/R− | 203 (23.8%) | 9 (22.5%) | 81 (24.6%) | 75 (23.0%) | 21 (30.0%) | |
| D+/R+ | 354 (41.5%) | 16 (40.0%) | 123 (37.4%) | 148 (45.3%) | 29 (41.4%) | |
| Warm ischemia period (minutes) | 33 ± 8 | 30 ± 8 | 33 ± 9 | 34 ± 8 | 34 ± 8 | 0.127 a |
| Time on dialysis (months) | 57.7 ± 40.8 | 52.1 ± 45.1 | 55.6 ± 45.3 | 58.4 ± 37.0 | 61.7 ± 35.3 | 0.164 a |
| Initial steroid use | 844 (98.8%) | 38 (%) | 315 (95.5%) | 323 (99.4%) | (%) | 0.107 b |
| Initial MMF* use | 824 (96.5%) | 40 (100%) | 315 (95.5%) | 315 (97.2%) | 69 (98.6%) | 0.425 b |
| Initial CyA* use | 42 (4.9%) | 0 (0%) | 15 (4.5%) | 19 (5.8%) | 4 (5.7%) | 0.325 b |
| Initial tacrolimus use (n) | 804 (94.1%) | 40 (100%) | 310 (93.9%) | 305 (93.8%) | 66 (94.3%) | 0.397 b |
| Initial mTOR * inhibitor use(n) | 26 (3.0%) | 0 (0%) | 11 (3.3%) | 11 (3.4%) | 1 (1.4%) | 0.568 b |
| Diagnosis of ESRD, (n) | 0.001 c | |||||
| Hypertension | 74 (8.7%) | 1 (2.5%) | 24 (7.3%) | 36 (11.0%) | 6 (8.6%) | |
| Diabetes mellitus | 54 (6.3%) | 3 (7.5%) | 14 (4.3%) | 22 (6.7%) | 5 (7.1%) | |
| Polycystic kidney disease | 127 (14.9%) | 3 (7.5%) | 57 (17.3%) | 43 (13.2%) | 10 (14.3%) | |
| Obstructive nephropathy | 39 (4.6%) | 3 (7.5%) | 20 (6.1%) | 14 (4.3%) | 1 (1.4%) | |
| Glomerulonephritis | 271 (31.7%) | 7 (17.5%) | 113 (34.3%) | 106 (32.5%) | 26 (37.1%) | |
| FSGS | 36 (4.2%) | 0 (0%) | 9 (2.7%) | 16 (4.9%) | 5 (7.1%) | |
| Interstitial nephritis | 45 (5.3%) | 7 (17.5%) | 14 (4.3%) | 14 (4.3%) | 4 (5.7%) | |
| Vasculitis | 21 (2.5%) | 0 (0%) | 4 (1.2%) | 11 (3.4%) | 4 (5.7%) | |
| Other | 110 (12.9%) | 12 (30.0%) | 43 (13.1%) | 37 (11.3%) | 3 (4.3%) | |
| Unknown | 73 (8.5%) | 4 (10.0%) | 29 (8.8%) | 26 (8.0%) | 6 (8.6%) |
| Variable | All | No Antihypertensive Drugs | 1–2 Antihypertensive Drugs | 3–4 Antihypertensive Drugs | ≥5 Antihypertensive Drugs | p Value |
|---|---|---|---|---|---|---|
| Mean syst. BP after one year (mmHg) | 135 ± 17 | 125 ± 24 | 133 ± 15 | 136 ± 17 | 142 ± 16 | <0.001 a |
| Mean diast. BP after one year (mmHg) | 82 ± 11 | 81 ± 13 | 82± 11 | 81 ± 12 | 80 ± 12 | 0.374 a |
| DGF (n) | 208 (24.4%) | 4 (10%) | 52 (15.8%) | 84 (25.8%) | 22 (31.4%) | 0.001 b |
| CMV DNAemia | 265 (31.0%) | 12 (30.0%) | 94 (28.6%) | 123 (37.3%) | 25 (35.7%) | 0.101 b |
| BKV DNAemia | 182 (21.3%) | 8 (20.0%) | 75 (22.8%) | 72 (22.1%) | 18 (25.7%) | 0.736 b |
| eGFR at year 1 (mL/min/1.73 m2) | 52.6 ± 20.2 | 63.9 ± 19.4 | 57.4 ± 19.7 | 49.2 ± 19.5 | 40.5 ± 16.2 | <0.001 a |
| eGFR at year 2 (mL/min/1.73 m2) | 53.1 ± 20.9 | 65.9 ± 23.1 | 57.4 ± 20.1 | 49.6 ± 20.5 | 43.0 ± 17.6 | <0.001 a |
| eGFR at year 5 (mL/min/1.73 m2) | 52.5 ± 21.8 | 56.0 ± 27.2 | 57.9 ± 22.4 | 49.9 ± 20.6 | 37.5 ± 11.2 | <0.001 a |
| UPCR at year 1 mg/g crea | 283 ± 732 | 160 ± 181 | 183 ± 306 | 352 ± 874 | 549 ± 1410 | <0.001 a |
| UPCR at year 2 mg/g crea | 260 ± 517 | 217 ± 271 | 196 ± 489 | 286 ± 465 | 481 ± 857 | 0.008 a |
| UPCR at year 5 (mg/g crea) | 323 ± 672 | 272 ± 272 | 150 ± 96 | 553 ± 1088 | 489 ± 487 | 0.102 a |
| Rejection yes (n) | 257 (30.1%) | 10 (25%) | 97 (29.5%) | 101 (31.0%) | 26 (37.1%) | 0.607 b |
| ACE-I/ARB use | 443 (51.9%) | - | 117 (35.6%) | 261 (80.0%) | 65 (92.8%) | <0.001b |
| Calcium-channel blocker use | 440 (51.5%) | - | 108 (32.8%) | 264 (81.0%) | 68 (97.1%) | <0.001b |
| Beta-blocker use | 582 (68.1%) | - | 217 (66.0%) | 296 (90.8%) | 69 (98.6%) | <0.001b |
| Diuretic use | 375 (43.9%) | - | 89 (27.0%) | 219 (67.2%) | 67 (95.7%) | <0.001b |
| Antisympathotonic use | 94 (11.0%) | - | 0 (0%) | 42 (12.9%) | 52 (74.3%) | <0.001b |
| Vasodilator use | 20 (2.3%) | - | 0 (0%) | 8 (2.5%) | 12 (17.1%) | <0.001b |
| Alpha1-receptor blocker use | 30 (3.5%) | - | 0 (0%) | 9 (2.8%) | 21 (30.0%) | <0.001b |
| Antihypertensive Agent | Mean eGFR (mL/min/1.73 m2) | Mean UPCR (mg/g Creatinine) |
|---|---|---|
| ACE-I/ARB use (n = 443) | 51.4 ± 19.5 | 289 ± 758 |
| Beta-blocker use (n = 582) | 50.5 ± 19.9 | 304 ± 818 |
| Loop diuretic use (n = 331) | 44.4 ± 17.6 | 417 ± 1049 |
| CCB use (n = 440) | 51.3 ± 20.5 | 306 ± 715 |
| Variable | Hazard Ratio | 95% CI | p Value |
|---|---|---|---|
| Age at KTx | 0.980 | 0.953–1.008 | 0.161 |
| Previous KTx | 0.514 | 0.151–1.744 | 0.285 |
| CMV-DNAemia | 1.576 | 0.842–2.950 | 0.155 |
| BKV-DNAemia | 1.279 | 0.650–2.517 | 0.476 |
| Post-mortal donation | 0.411 | 0.116–1.464 | 0.170 |
| Donor age | 1.023 | 0.992–1.055 | 0.152 |
| Dialysis vintage | 1.001 | 0.991–1.012 | 0.842 |
| Cold ischemia time | 1.104 | 1.021–1.195 | 0.014 |
| Delayed graft function | 0.969 | 0.477–1.966 | 0.930 |
| Acute rejection | 4.428 | 2.249–8.720 | <0.001 |
| Beta-blocker use | 0.884 | 0.305–2.561 | 0.820 |
| Loop diuretic use | 1.388 | 0.643–2.995 | 0.404 |
| CCB use | 0.604 | 0.248–1.468 | 0.266 |
| ACE-I/ARB | 0.619 | 0.278–1.379 | 0.240 |
| Number of antihypertensives after 12 months | 1.585 | 1.061–2.367 | 0.025 |
| Underlying renal disease | - | - | 0.764 |
| Variable | All | No Antihypertensive Drugs | 1–2 Antihypertensive Drugs | 3–4 Antihypertensive Drugs | ≥5 Antihypertensive Drugs | p Value |
|---|---|---|---|---|---|---|
| eGFR-change year 1–2, mL/min/1.73 m² (Mean, SD) | 0.31 ± 10.2 | 2.2 (12.6) | −0.17 (10.5) | 0.9 (10.1) | 1.8 (7.4) | 0.405 * |
| eGFR-change year 1–5, mL/min/1.73 m² (Mean, SD) | 2.4 (16.3) | −6.6 (15.6) | 3.7 (15.7) | 3.0 (16.9) | −1.8 (15.4) | 0.032 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jehn, U.; Schütte-Nütgen, K.; Strauss, M.; Kunert, J.; Pavenstädt, H.; Thölking, G.; Suwelack, B.; Reuter, S. Antihypertensive Treatment in Kidney Transplant Recipients—A Current Single Center Experience. J. Clin. Med. 2020, 9, 3969. https://doi.org/10.3390/jcm9123969
Jehn U, Schütte-Nütgen K, Strauss M, Kunert J, Pavenstädt H, Thölking G, Suwelack B, Reuter S. Antihypertensive Treatment in Kidney Transplant Recipients—A Current Single Center Experience. Journal of Clinical Medicine. 2020; 9(12):3969. https://doi.org/10.3390/jcm9123969
Chicago/Turabian StyleJehn, Ulrich, Katharina Schütte-Nütgen, Markus Strauss, Jan Kunert, Hermann Pavenstädt, Gerold Thölking, Barbara Suwelack, and Stefan Reuter. 2020. "Antihypertensive Treatment in Kidney Transplant Recipients—A Current Single Center Experience" Journal of Clinical Medicine 9, no. 12: 3969. https://doi.org/10.3390/jcm9123969
APA StyleJehn, U., Schütte-Nütgen, K., Strauss, M., Kunert, J., Pavenstädt, H., Thölking, G., Suwelack, B., & Reuter, S. (2020). Antihypertensive Treatment in Kidney Transplant Recipients—A Current Single Center Experience. Journal of Clinical Medicine, 9(12), 3969. https://doi.org/10.3390/jcm9123969