Low Seroprevalence of SARS-CoV-2 Antibodies during Systematic Antibody Screening and Serum Responses in Patients after COVID-19 in a German Transplant Center

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Subjects
2.3. Serological Testing for SARS-CoV-2 Antibodies
2.4. RT-PCR Methodology for SARS-CoV-2 Infection
2.5. Statistics
3. Results
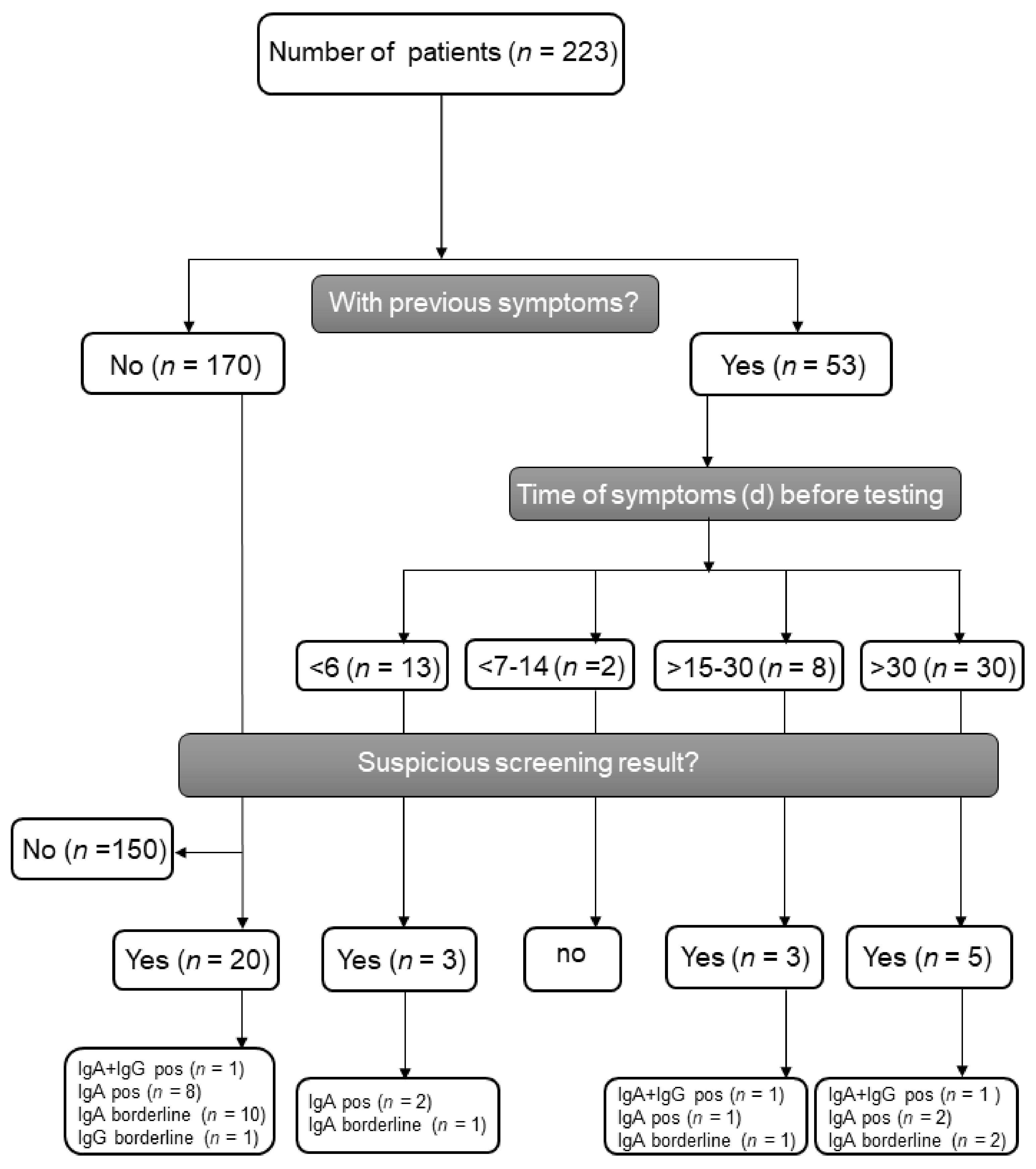
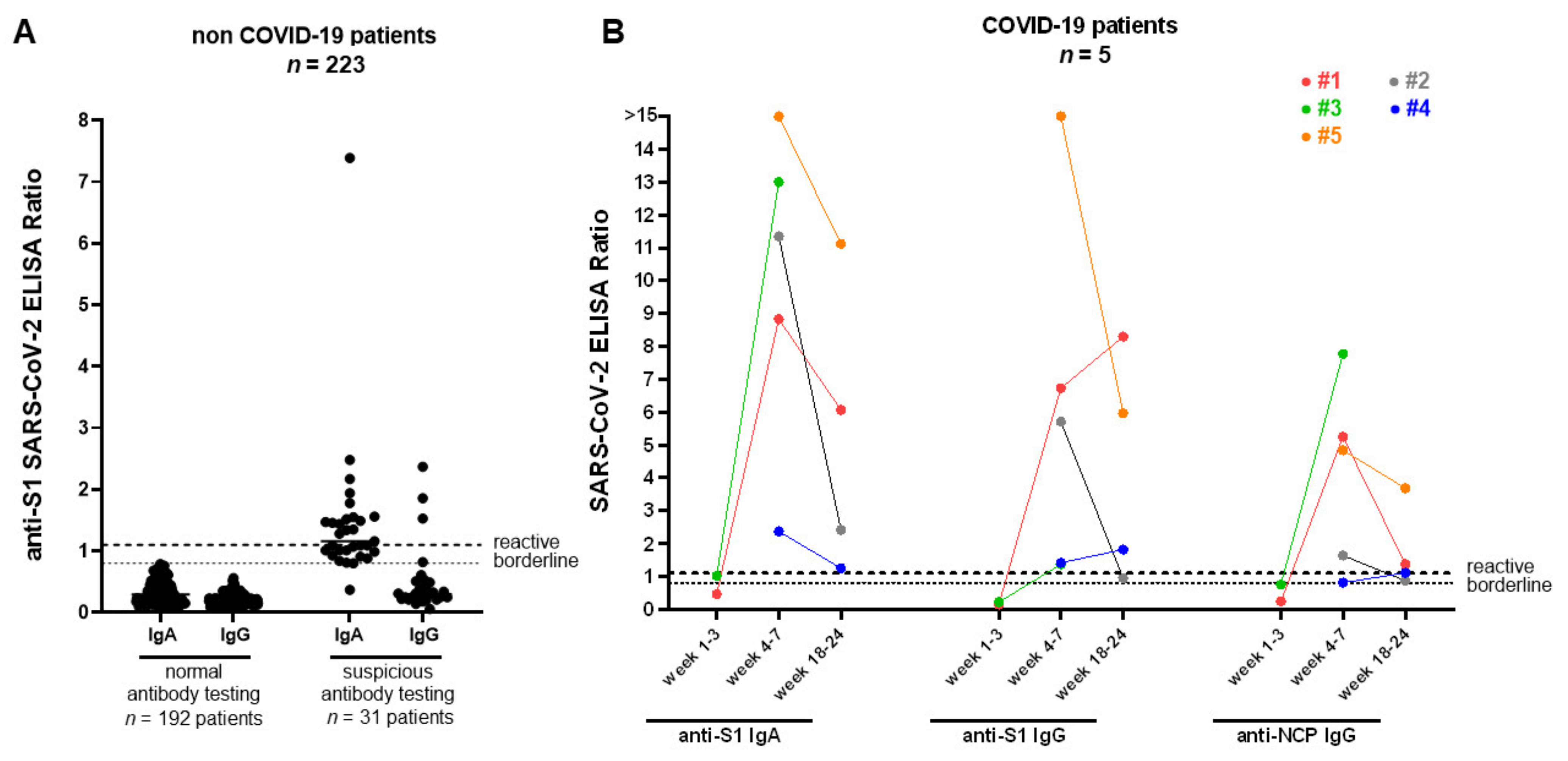
3.1. Patient Characteristics and SARS-CoV-2 Seroprevalence in Patients after Renal Transplantation in Our Outpatient Department
3.2. Seroconversion in Renal Transplant Patients after SARS-CoV-2 Infection
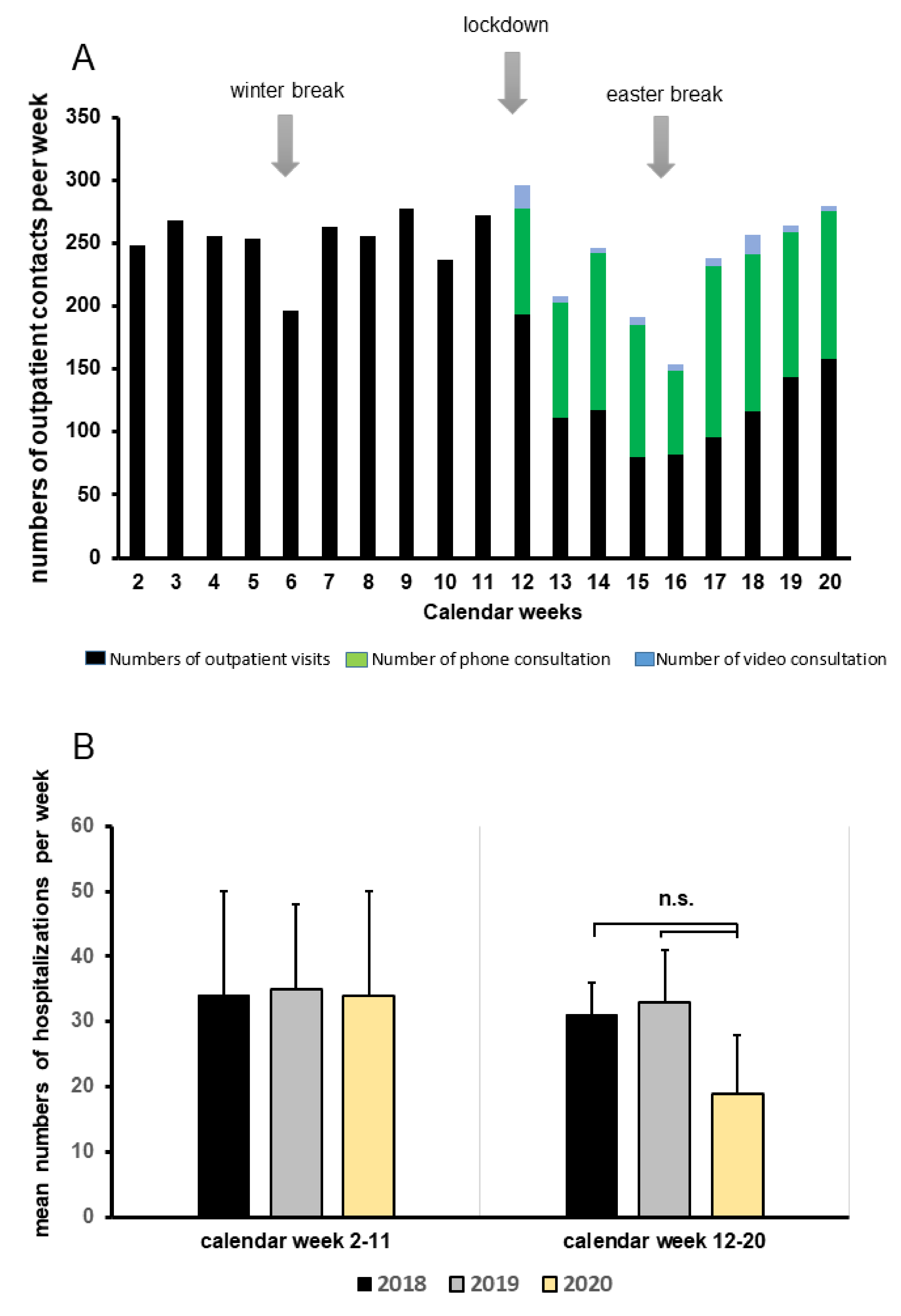
3.3. Patient Care during SARS-CoV-2 Pandemic
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Liu, X.; Xiong, L.; Cai, K. Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2: A systematic review and meta-analysis. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.R.; Mohan, S.; Cohen, D.J.; Husain, S.A.; Dube, G.K.; Ratner, L.E.; Arcasoy, S.; Aversa, M.M.; Benvenuto, L.J.; Dadhania, D.M.; et al. COVID-19 in solid organ transplant recipients: Initial report from the US epicenter. Am. J. Transplant. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kates, O.S.; Haydel, B.M.; Florman, S.S.; Rana, M.M.; Chaudhry, Z.S.; Ramesh, M.S.; Safa, K.; Kotton, C.N.; Blumberg, E.A.; Besharatian, B.D.; et al. COVID-19 in solid organ transplant: A multi-center cohort study. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Hoek, R.A.S.; Manintveld, O.C.; Betjes, M.G.H.; Hellemons, M.E.; Seghers, L.; Van Kampen, J.A.A.; Caliskan, K.; van de Wetering, J.; van den Hoogen, M.; Metselaar, H.J.; et al. COVID-19 in solid organ transplant recipients: A single-center experience. Transpl. Int. 2020. [Google Scholar] [CrossRef]
- Travi, G.; Rossotti, R.; Merli, M.; Sacco, A.; Perricone, G.; Lauterio, A.; Colombo, V.G.; De Carlis, L.; Frigerio, M.; Minetti, E.; et al. Clinical outcome in solid organ transplant recipients with COVID-19: A single-center experience. Am. J. Transplant. 2020, 20, 2628–2629. [Google Scholar] [CrossRef]
- Yi, S.G.; Rogers, A.W.; Saharia, A.; Aoun, M.; Faour, R.; Abdelrahim, M.; Knight, R.J.; Grimes, K.; Bullock, S.; Hobeika, M.; et al. Early Experience with COVID-19 and Solid Organ Transplantation at a US High-volume Transplant Center. Transplantation 2020. [Google Scholar] [CrossRef]
- Liu, R.; Han, H.; Liu, F.; Lv, Z.; Wu, K.; Liu, Y.; Feng, Y.; Zhu, C. Positive rate of RT-PCR detection of SARS-CoV-2 infection in 4880 cases from one hospital in Wuhan, China, from Jan to Feb 2020. Clin. Chim. Acta 2020, 505, 172–175. [Google Scholar] [CrossRef]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA 2020. [Google Scholar] [CrossRef]
- Wolfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Muller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020. [Google Scholar] [CrossRef]
- Xiang, F.; Wang, X.; He, X.; Peng, Z.; Yang, B.; Zhang, J.; Zhou, Q.; Ye, H.; Ma, Y.; Li, H.; et al. Antibody Detection and Dynamic Characteristics in Patients with COVID-19. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Fung, M.; Chiu, C.Y.; DeVoe, C.; Doernberg, S.B.; Schwartz, B.S.; Langelier, C.; Henrich, T.J.; Yokoe, D.; Davis, J.; Hays, S.R.; et al. Clinical outcomes and serologic response in solid organ transplant recipients with COVID-19: A case series from the United States. Am. J. Transplant. 2020. [Google Scholar] [CrossRef] [PubMed]
- Babel, N.; Anft, M.; Blazquez-Navarro, A.; Doevelaar, A.A.N.; Seibert, F.S.; Bauer, F.; Rohn, B.J.; Hoelzer, B.; Thieme, C.J.; Roch, T.; et al. Immune monitoring facilitates the clinical decision in multifocal COVID-19 of a pancreas-kidney transplant patient. Am. J. Transplant. 2020. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brunink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25. [Google Scholar] [CrossRef]
- Behrens, G.M.N.; Cossmann, A.; Stankov, M.V.; Schulte, B.; Streeck, H.; Forster, R.; Bosnjak, B.; Willenzon, S.; Boeck, A.L.; Thu Tran, A.; et al. Strategic Anti-SARS-CoV-2 Serology Testing in a Low Prevalence Setting: The COVID-19 Contact (CoCo) Study in Healthcare Professionals. Infect. Dis. Ther. 2020. [Google Scholar] [CrossRef]
- Neumann, J.; Zeeb, H.; Dotzauer, A.; Janssen-Weets, O. Geringe anti-SARS-CoV-2-Seroprävalenz unter Beschäftigten des Öffentlichen Dienstes in Bremen. Z. Med. Präevention 2020, 08. [Google Scholar]
- Okba, N.M.A.; Muller, M.A.; Li, W.; Wang, C.; GeurtsvanKessel, C.H.; Corman, V.M.; Lamers, M.M.; Sikkema, R.S.; de Bruin, E.; Chandler, F.D.; et al. Severe Acute Respiratory Syndrome Coronavirus 2-Specific Antibody Responses in Coronavirus Disease Patients. Emerg. Infect. Dis. 2020, 26, 1478–1488. [Google Scholar] [CrossRef]
- Beavis, K.G.; Matushek, S.M.; Abeleda, A.P.F.; Bethel, C.; Hunt, C.; Gillen, S.; Moran, A.; Tesic, V. Evaluation of the EUROIMMUN Anti-SARS-CoV-2 ELISA Assay for detection of IgA and IgG antibodies. J. Clin. Virol. 2020, 129, 104468. [Google Scholar] [CrossRef]
- Long, Q.X.; Tang, X.J.; Shi, Q.L.; Li, Q.; Deng, H.J.; Yuan, J.; Hu, J.L.; Xu, W.; Zhang, Y.; Lv, F.J.; et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat. Med. 2020, 26, 1200–1204. [Google Scholar] [CrossRef]
- Aziz, N.A.; Corman, V.M.; Echterhoff, A.K.C.; Richter, A.; Schmandke, A.; Schmidt, M.L.; Schmidt, T.H.; Vries, F.M.D.; Drosten, C.; Breteler, M.M.B. Seroprevalence and correlates of SARS-CoV-2 neutralizing antibodies: Results from a population-based study in Bonn, Germany. medRxiv 2020. [Google Scholar] [CrossRef]
- Wang, X.; Guo, X.; Xin, Q.; Pan, Y.; Hu, Y.; Li, J.; Chu, Y.; Feng, Y.; Wang, Q. Neutralizing Antibodies Responses to SARS-CoV-2 in COVID-19 Inpatients and Convalescent Patients. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Hartzell, S.; Bin, S.; Benedetti, C.; Haverly, M.; Gallon, L.; Zaza, G.; Riella, L.V.; Menon, M.C.; Florman, S.; Rahman, A.H.; et al. Evidence of potent humoral immune activity in COVID19-infected kidney transplant recipients. Am. J. Transplant. 2020. [Google Scholar] [CrossRef]
- Benotmane, I.; Gautier-Vargas, G.; Wendling, M.J.; Perrin, P.; Velay, A.; Bassand, X.; Bedo, D.; Baldacini, C.; Sagnard, M.; Bozman, D.F.; et al. In-depth virological assessment of kidney transplant recipients with COVID-19. Am. J. Transplant. 2020. [Google Scholar] [CrossRef]
- Montesinos, I.; Gruson, D.; Kabamba, B.; Dahma, H.; Van den Wijngaert, S.; Reza, S.; Carbone, V.; Vandenberg, O.; Gulbis, B.; Wolff, F.; et al. Evaluation of two automated and three rapid lateral flow immunoassays for the detection of anti-SARS-CoV-2 antibodies. J. Clin. Virol. 2020, 128, 104413. [Google Scholar] [CrossRef] [PubMed]
- Akalin, E.; Azzi, Y.; Bartash, R.; Seethamraju, H.; Parides, M.; Hemmige, V.; Ross, M.; Forest, S.; Goldstein, Y.D.; Ajaimy, M.; et al. Covid-19 and Kidney Transplantation. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Cravedi, P.; Suraj, S.M.; Azzi, Y.; Haverly, M.; Farouk, S.; Perez-Saez, M.J.; Redondo-Pachon, M.D.; Murphy, B.; Florman, S.; Cyrino, L.G.; et al. COVID-19 and Kidney Transplantation: Results from the TANGO International Transplant Consortium. Am. J. Transplant. 2020. [Google Scholar] [CrossRef]
- Caillard, S.; Anglicheau, D.; Matignon, M.; Durrbach, A.; Greze, C.; Frimat, L.; Thaunat, O.; Legris, T.; Moal, V.; Westeel, P.F.; et al. An initial report from the French SOT COVID Registry suggests high mortality due to Covid-19 in recipients of kidney transplants. Kidney Int. 2020. [Google Scholar] [CrossRef]
- Montagud-Marrahi, E.; Cofan, F.; Torregrosa, J.V.; Cucchiari, D.; Ventura-Aguiar, P.; Revuelta, I.; Bodro, M.; Pineiro, G.J.; Esforzado, N.; Ugalde, J.; et al. Preliminary data on outcomes of SARS-CoV-2 infection in a Spanish single centre cohort of kidney recipients. Am. J. Transplant. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kates, O.S.; Fisher, C.E.; Stankiewicz-Karita, H.C.; Shepherd, A.K.; Church, E.C.; Kapnadak, S.G.; Lease, E.D.; Riedo, F.X.; Rakita, R.M.; Limaye, A.P. Earliest cases of coronavirus disease 2019 (COVID-19) identified in solid organ transplant recipients in the United States. Am. J. Transplant. 2020. [Google Scholar] [CrossRef] [PubMed]
- Columbia University Kidney Transplant Program. Early Description of Coronavirus 2019 Disease in Kidney Transplant Recipients in New York. J. Am. Soc. Nephrol. 2020, 31, 1150–1156. [Google Scholar] [CrossRef] [PubMed]
- Hugo, C.; Strassburg, C.; Stecher, M.; Rahmel, A. Stable and safe organ procurement and transplantation during SARS-CoV-2 pandemic in Germany. Transpl. Int. 2020. [Google Scholar] [CrossRef]
- Loupy, A.; Aubert, O.; Reese, P.P.; Bastien, O.; Bayer, F.; Jacquelinet, C. Organ procurement and transplantation during the COVID-19 pandemic. Lancet 2020. [Google Scholar] [CrossRef]
- Kumar, D.; Manuel, O.; Natori, Y.; Egawa, H.; Grossi, P.; Han, S.H.; Fernandez-Ruiz, M.; Humar, A. COVID-19: A global transplant perspective on successfully navigating a pandemic. Am. J. Transplant. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.L.; Vest, L.; Schnitzler, M.A.; Mannon, R.B.; Kumar, V.; Doshi, M.D.; Cooper, M.; Mandelbrot, D.A.; Harhay, M.N.; Josephson, M.A.; et al. Survey of U.S. Living Kidney Donation and Transplant Practices in the COVID-19 Era. Kidney Int. Rep. 2020. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Recipients (n = 223) |
|---|---|
| Age at transplantation, years, median (IQR) | 46 (34, 56) |
| Age at serum assessment in years, median (IQR) | 54 (42, 64) |
| Type of transplant donor, n (%) | |
| Living donor | 82 (36.8%) |
| Deceased donor | 141 (63.2%) |
| Recipient gender male, n (%) | 138 (61.9%) |
| Organ transplant, n (%) | |
| Kidney | 210 (94.2%) |
| Kidney/pancreas | 9 (64.0%) |
| Kidney/liver | 3 (1.3%) |
| Multivisceral (kidney/pancreas/liver) | 1 (0.4%) |
| Time from transplant to screening, months, median (IQR) | 66 (14, 155) |
| Mean serum creatinine at screening, mg/dL (SD) | 1.6 (0.9–3.1) |
| No | Age, Years | Sex | Co- Morbi-Dities | Time since TX, Years | Baseline Crea, mg/dL | Symptom Start, Date | Date of Positive PCR | Crea, mg/dL | WBC G/L | CRP, mg/L | LDH, U/L | Date of Negative PCR | Time between PCR and 1st Serum Test, Days |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 78 | M | ADPKD HTN CAD | 6 | 1.6 | March 9th | March 24th | 3.1 | 3.5 | 68 | 676 | April 24th | 43 |
| 2 | 43 | M | MPGN HTN | 12 | 1.0 | March 19th | March 30th | 1.2 | 7.7 | 0.5 | 262 | Apr 14th | 31 |
| 3 | 53 | M | HTN Obesity CHF COPD Diabetes | 3 | 2.2 | March 20th | April 1st | 5.2 | 18.4 | 85 | 610 | positive until April 20th | 24 |
| 4 | 43 | F | HTN HCV | 15 | 1.4 | March 23rd | April 1st | 1.5 | 3.5 | 0.1 | 129 | May 4th | 43 |
| 5 | 61 | M | Diabetes NPTX HTN | 22 | 1.0 | April 2nd | April 15th | 1.0 | 5.0 | 31 | 229 | May 19th | 34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, M.; Bachmann, F.; Naik, M.G.; Duettmann, W.; Duerr, M.; Zukunft, B.; Schwarz, T.; Corman, V.M.; Liefeldt, L.; Budde, K.; et al. Low Seroprevalence of SARS-CoV-2 Antibodies during Systematic Antibody Screening and Serum Responses in Patients after COVID-19 in a German Transplant Center. J. Clin. Med. 2020, 9, 3401. https://doi.org/10.3390/jcm9113401
Choi M, Bachmann F, Naik MG, Duettmann W, Duerr M, Zukunft B, Schwarz T, Corman VM, Liefeldt L, Budde K, et al. Low Seroprevalence of SARS-CoV-2 Antibodies during Systematic Antibody Screening and Serum Responses in Patients after COVID-19 in a German Transplant Center. Journal of Clinical Medicine. 2020; 9(11):3401. https://doi.org/10.3390/jcm9113401
Chicago/Turabian StyleChoi, Mira, Friederike Bachmann, Marcel Ganesh Naik, Wiebke Duettmann, Michael Duerr, Bianca Zukunft, Tatjana Schwarz, Victor Max Corman, Lutz Liefeldt, Klemens Budde, and et al. 2020. "Low Seroprevalence of SARS-CoV-2 Antibodies during Systematic Antibody Screening and Serum Responses in Patients after COVID-19 in a German Transplant Center" Journal of Clinical Medicine 9, no. 11: 3401. https://doi.org/10.3390/jcm9113401
APA StyleChoi, M., Bachmann, F., Naik, M. G., Duettmann, W., Duerr, M., Zukunft, B., Schwarz, T., Corman, V. M., Liefeldt, L., Budde, K., & Halleck, F. (2020). Low Seroprevalence of SARS-CoV-2 Antibodies during Systematic Antibody Screening and Serum Responses in Patients after COVID-19 in a German Transplant Center. Journal of Clinical Medicine, 9(11), 3401. https://doi.org/10.3390/jcm9113401