Association between Multidimensional Prognostic Index and Hospitalization and Mortality among Older Adults with Chronic Kidney Disease on Conservative or on Replacement Therapy

 ,
,  , , , , , ,
, , , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Calculation of the MPI at Baseline
2.3. Hospitalization and Mortality over the 24-Month Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics at Baseline
3.2. MPI Classes
3.3. 24-Month Follow-Up and Clinical Characteristics
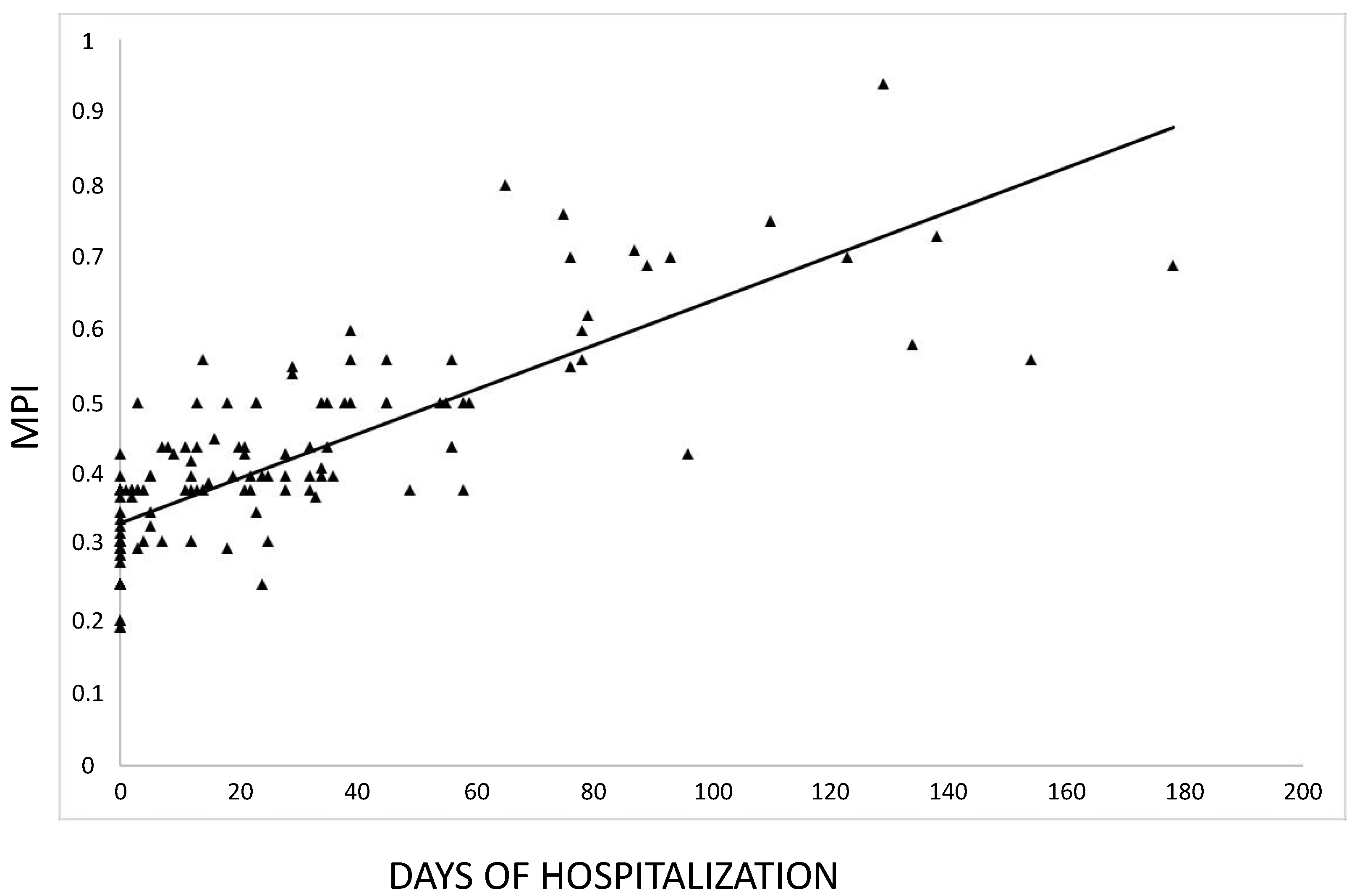
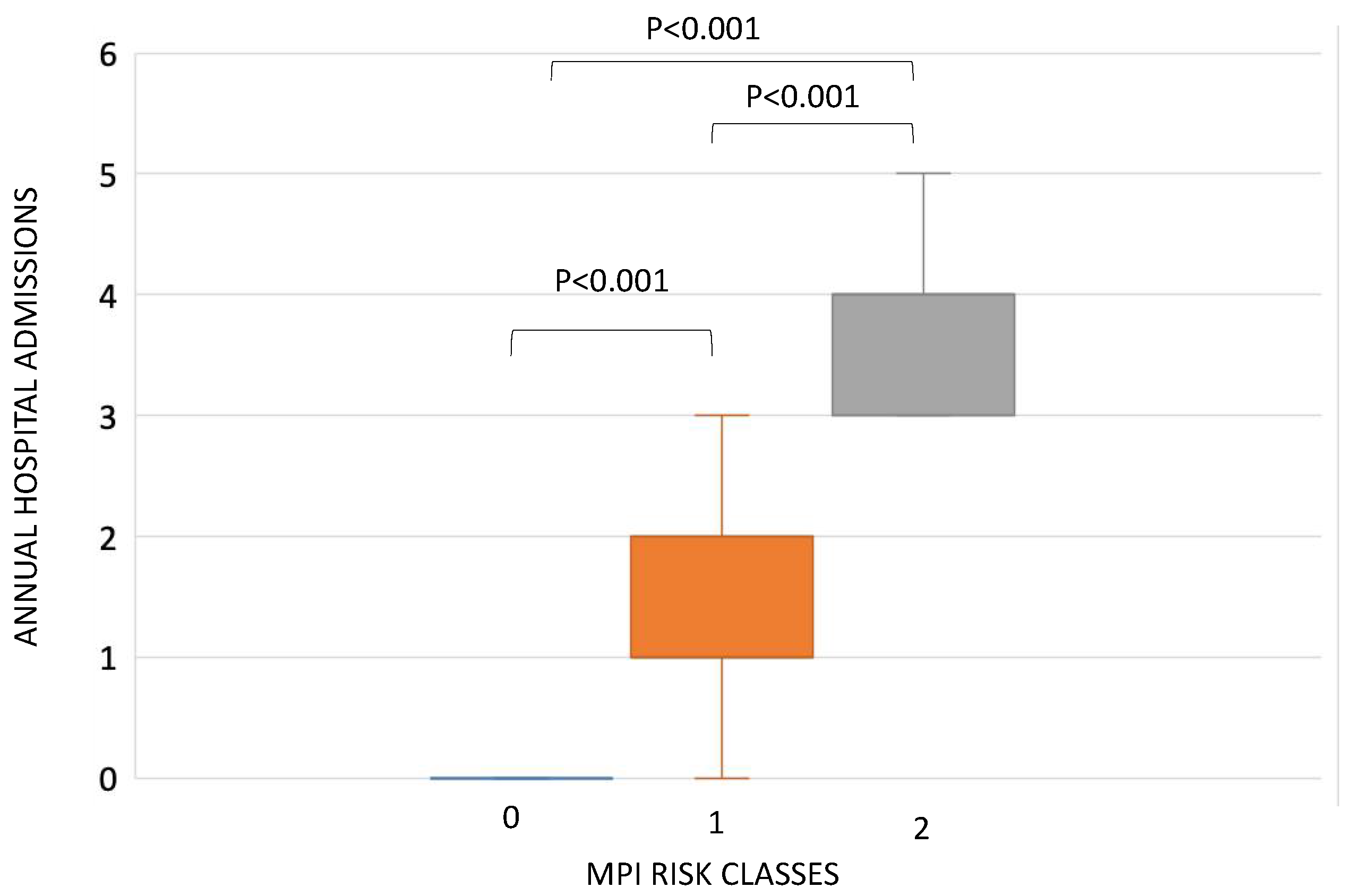
3.4. MPI and Hospitalization
3.5. MPI and Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pyart, R.; Evans, K.M.; Steenkamp, R.; Casula, A.; Wong, E.; Magadi, W.; Medcalf, J. The 21st UK Renal Registry Annual Report: A Summary of Analyses of Adult Data in 2017. Nephron 2019, 144, 59–66. [Google Scholar] [CrossRef]
- United States Renal Data System. 2017 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2017. Available online: https://www.usrds.org/annual-data-report/previous-adrs (accessed on 10 October 2020).
- Lai, S.; Muscaritoli, M.; Andreozzi, P.; Sgreccia, A.; De Leo, S.; Mazzaferro, S.; Mitterhofer, A.P.; Pasquali, M.; Protopapa, P.; Spagnoli, A.; et al. Sarcopenia and cardiovascular risk indices in patients with chronic kidney disease on conservative and replacement therapy. Nutrition 2019, 62, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Angleman, S.B.; Santoni, G.; Pilotto, A.; Fratiglioni, L.; Welmer, A.-K.; on behalf of the MPI_AGE Project Investigators. Multidimensional Prognostic Index in Association with Future Mortality and Number of Hospital Days in a Population-Based Sample of Older Adults: Results of the EU Funded MPI_AGE Project. PLoS ONE 2015, 10, e0133789. [Google Scholar] [CrossRef] [PubMed]
- Pilotto, A.; Panza, F.; Sancarlo, D.; Paroni, G.; Maggi, S.; Ferrucci, L. Usefulness of the multidimensional prognostic index (MPI) in the management of older patients with chronic kidney disease. J. Nephrol. 2012, 25, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Pilotto, A.; Sancarlo, D.; Aucella, F.; Fontana, A.; Addante, F.; Copetti, M.; Panza, F.; Strippoli, G.F.; Ferrucci, L. Addition of the Multidimensional Prognostic Index to the Estimated Glomerular Filtration Rate Improves Prediction of Long-Term All-Cause Mortality in Older Patients with Chronic Kidney Disease. Rejuvenation Res. 2012, 15, 82–88. [Google Scholar] [CrossRef]
- Pilotto, A.; Sancarlo, D.; Franceschi, M.; Yang, X.; D’Ambrosio, P.; Scarcelli, C.; Ferrucci, L. A multidimensional approach to the geriatric patient with chronic kidney disease. J. Nephrol. 2010, 23. [Google Scholar]
- Sy, J.; Streja, E.; Grimes, B.; Johansen, K.L. The Marginal Cost of Frailty among Medicare Patients on Hemodialysis. Kidney Int. Rep. 2020, 5, 289–295. [Google Scholar] [CrossRef]
- Pilotto, A.; Custodero, C.; Maggi, S.; Polidori, M.C.; Veronese, N.; Ferrucci, L. A multidimensional approach to frailty in older people. Ageing Res. Rev. 2020, 60, 101047. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y. (Lucy); Hendriksen, S.; Kusek, J.W.; Van Lente, F.; for the Chronic Kidney Disease Epidemiology Collaboration. Using Standardized Serum Creatinine Values in the Modification of Diet in Renal Disease Study Equation for Estimating Glomerular Filtration Rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Lai, S.; Molfino, A.; Russo, G.E.; Testorio, M.; Galani, A.; Innico, G.; Frassetti, N.; Pistolesi, V.; Morabito, S.; Fanelli, F.R. Cardiac, Inflammatory and Metabolic Parameters: Hemodialysis versus Peritoneal Dialysis. Cardiorenal Med. 2015, 5, 20–30. [Google Scholar] [CrossRef]
- Molfino, A.; Chiappini, M.G.; Laviano, A.; Ammann, T.; Bollea, M.R.; Alegiani, F.; Fanelli, F.R.; Molfino, A. Effect of intensive nutritional counseling and support on clinical outcomes of hemodialysis patients. Nutrition 2012, 28, 1012–1015. [Google Scholar] [CrossRef] [PubMed]
- Volpato, S.; Bazzano, S.; Fontana, A.; Ferrucci, L.; Pilotto, A. Multidimensional Prognostic Index Predicts Mortality and Length of Stay During Hospitalization in the Older Patients: A Multicenter Prospective Study. J. Gerontol. Ser. A Biol. Sci. Med Sci. 2014, 70, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Kallenberg, M.H.; Kleinveld, H.A.; Dekker, F.W.; Van Munster, B.C.; Rabelink, T.J.; Van Buren, M.; Mooijaart, S.P. Functional and Cognitive Impairment, Frailty, and Adverse Health Outcomes in Older Patients Reaching ESRD—A Systematic Review. Clin. J. Am. Soc. Nephrol. 2016, 11, 1624–1639. [Google Scholar] [CrossRef] [PubMed]
- McAdams-DeMarco, M.A.; Ying, H.; Olorundare, I.; King, E.A.; Haugen, C.; Buta, B.; Gross, A.L.; Kalyani, R.; Desai, N.M.; Dagher, N.N.; et al. Individual Frailty Components and Mortality in Kidney Transplant Recipients. Transplantation 2017, 101, 2126–2132. [Google Scholar] [CrossRef]
- Villarreal, I.R.; Ortega, O.; Hinostroza, J.; Cobo, G.; Gallar, P.; Mon, C.; Herrero, J.C.; Ortiz, M.; Di Giogia, C.; Oliet, A.; et al. Geriatric Assessment for Therapeutic Decision-Making Regarding Renal Replacement in Elderly Patients with Advanced Chronic Kidney Disease. Nephron Clin. Pract. 2014, 128, 73–78. [Google Scholar] [CrossRef]
- Lee, S.-Y.; Yang, D.H.; Hwang, E.; Kang, S.H.; Park, S.-H.; Kim, T.W.; Lee, D.H.; Park, K.; Kim, J.C. The Prevalence, Association, and Clinical Outcomes of Frailty in Maintenance Dialysis Patients. J. Ren. Nutr. 2017, 27, 106–112. [Google Scholar] [CrossRef]
- Sancarlo, D.; Pilotto, A.; Panza, F.; Copetti, M.; Longo, M.G.; D’Ambrosio, P.; D’Onofrio, G.; Ferrucci, L.; Pilotto, A. A Multidimensional Prognostic Index (MPI) based on a comprehensive geriatric assessment predicts short- and long-term all-cause mortality in older hospitalized patients with transient ischemic attack. J. Neurol. 2011, 259, 670–678. [Google Scholar] [CrossRef][Green Version]
- Lai, S.; Molfino, A.; Mecarelli, O.; Pulitano, P.; Morabito, S.; Pistolesi, V.; Romanello, R.; Zarabla, A.; Galani, A.; Frassetti, N.; et al. Neurological and Psychological Changes in Hemodialysis Patients before and after the Treatment. Ther. Apher. Dial. 2018, 22, 530–538. [Google Scholar] [CrossRef]
- McAdams-DeMarco, M.A.; Tan, J.; Salter, M.L.; Gross, A.L.; Meoni, L.A.; Jaar, B.G.; Kao, W.-H.L.; Parekh, R.S.; Segev, D.L.; Sozio, S.M. Frailty and Cognitive Function in Incident Hemodialysis Patients. Clin. J. Am. Soc. Nephrol. 2015, 10, 2181–2189. [Google Scholar] [CrossRef]
- Foster, R.; Walker, S.; Brar, R.; Hiebert, B.; Komenda, P.; Rigatto, C.; Storsley, L.; Prasad, B.; Bohm, C.; Tangri, N. Cognitive Impairment in Advanced Chronic Kidney Disease: The Canadian Frailty Observation and Interventions Trial. Am. J. Nephrol. 2016, 44, 473–480. [Google Scholar] [CrossRef]
- Lai, S.; Amabile, M.I.; Bargagli, M.B.; Musto, T.G.; Martinez, A.; Testorio, M.; Mastroluca, D.; Lai, C.; Aceto, P.; Molfino, A.; et al. Peritoneal dialysis in older adults: Evaluation of clinical, nutritional, metabolic outcomes, and quality of life. Medicine 2018, 97, e11953. [Google Scholar] [CrossRef] [PubMed]
- Maher, R.L.; Hanlon, J.; Hajjar, E.R. Clinical consequences of polypharmacy in elderly. Expert Opin. Drug Saf. 2014, 13, 57–65. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline | Month 24 | |
|---|---|---|
| Male, n (%) | 107 (62) | 84 (60) |
| Age, y | 76 (70; 80) | 73 (69; 79) |
| BMI, kg/m2 | 26.4 ± 4.4 | 23.9 ± 3.4 |
| Hemoglobin, g/dL | 11.6 (10.6; 13) | 12.6 (11.6; 13.4) |
| Serum creatinine, mg/dL | ||
| All | 2.1(1.8; 6.0) | 2.8 (1.9; 7.2) |
| CKD stage 3 * | 1.8 (1.4; 2) | 2.08 (1.49; 2.5) |
| CKD stage 4–5 # | 1.9 (1.8; 2.2) | 2.63 (2.03; 2.9) |
| Replacement therapy § | 6.3 (5.6; 7) | 9 (7.53; 11) |
| Total serum nitrogen, mg/dL | ||
| All | 97 (69; 138) | 99 (87; 131) |
| CKD stage 3 * | 73 (64; 95) | 89 (67; 102) |
| CKD stage 4–5 # | 76.5 (58; 101) | 98 (76; 115) |
| Replacement therapy § | 147 (114; 179) | 122 (99; 148) |
| eGFR, mL/min/1.73 m2 | ||
| All | 27.5 (10; 39) | 21 (8.2; 30.3) |
| CKD stage 3 * | 39 (35; 52) | 30 (25; 39) |
| CKD stage 4–5 # | 25 (22; 28) | 25 (19.8; 29.3) |
| Replacement therapy § | 8.7 (7.3; 10.7) | 7.1 (5.5; 8.8) |
| pH | 7.33 (7.30; 7.38) | 7.37 (7.33; 7.40) |
| Base excess | −2.50 (−6.00; 1.00) | −1.90 (−3.50; −0.80) |
| Sodium, mEq/L | 139 (137; 142) | 140 (139; 143) |
| Potassium, mEq/L | 4.79 ± 0.63 | 4.63 ± 0.62 |
| Albumin, mg/dL | ||
| All | 3.98 (3.5; 4.1) | 4.60 (4.2; 5.0) |
| CKD stage 3 * | 3.89 (3.45; 4.1) | 4.67 (4.4; 5.0) |
| CKD stage 4–5 # | 3.8 (3.5; 4) | 4.7 (4.5; 5.1) |
| Replacement therapy § | 4.0 (3.8; 4.4) | 3.8 (3.4; 4.2) |
| iPTH, pg/mL | 160.5 (58.5; 165) | 109.5 (76.0; 221.3) |
| 25-OH-VitD, ng/mL | 21.5 (14.4; 29.3) | 14.8 (7; 20) |
| SBP, mmHg | 130 (120; 140) | 130 (120; 140) |
| DBP, mmHg | 80 (70; 86) | 80 (70; 85) |
| Days of Hospitalization | n° of Hospitalizations per Year | |
|---|---|---|
| Each of the 6 domains of MPI | ||
| ADL | ||
| r | −0.629 | −0.573 |
| p-value | <0.00001 | <0.00001 |
| IADL | ||
| r | −0.544 | −0.572 |
| p-value | <0.00001 | <0.00001 |
| SPMSQ | ||
| r | −0.419 | −0.381 |
| p-value | <0.00001 | <0.00001 |
| EXTON-SMITH | ||
| r | −0.476 | −0.480 |
| p-value | <0.00001 | <0.00001 |
| CIRS | ||
| r | 0.19 | 0.232 |
| p-value | 0.013 | 0.002 |
| MNA | ||
| r | −0.533 | −0.585 |
| p-value | <0.00001 | <0.00001 |
| MPI Risk Class | Total (n) | |||||
|---|---|---|---|---|---|---|
| 0 | 1 | 2 | ||||
| Death | NO | Count | 60 | 80 | 0 | 140 |
| Expected count | 48.6 | 82.5 | 8.9 | 140.0 | ||
| Standardized residual | 4.7 | −1.0 | −7.1 | |||
| YES | Count | 0 | 22 | 11 | 33 | |
| Expected count | 11.4 | 19.5 | 2.1 | 33.0 | ||
| Standardized residual | −4.7 | 1 | 7.1 | |||
| Total | Count | 60 | 102 | 11 | 173 | |
| Person’s Chi-square | Value 61.22 | p-value < 0.0001 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, S.; Amabile, M.I.; Mazzaferro, S.; Imbimbo, G.; Mitterhofer, A.P.; Galani, A.; Aucella, F.; Brunori, G.; Menè, P.; Molfino, A.; et al. Association between Multidimensional Prognostic Index and Hospitalization and Mortality among Older Adults with Chronic Kidney Disease on Conservative or on Replacement Therapy. J. Clin. Med. 2020, 9, 3965. https://doi.org/10.3390/jcm9123965
Lai S, Amabile MI, Mazzaferro S, Imbimbo G, Mitterhofer AP, Galani A, Aucella F, Brunori G, Menè P, Molfino A, et al. Association between Multidimensional Prognostic Index and Hospitalization and Mortality among Older Adults with Chronic Kidney Disease on Conservative or on Replacement Therapy. Journal of Clinical Medicine. 2020; 9(12):3965. https://doi.org/10.3390/jcm9123965
Chicago/Turabian StyleLai, Silvia, Maria Ida Amabile, Sandro Mazzaferro, Giovanni Imbimbo, Anna Paola Mitterhofer, Alessandro Galani, Filippo Aucella, Giuliano Brunori, Paolo Menè, Alessio Molfino, and et al. 2020. "Association between Multidimensional Prognostic Index and Hospitalization and Mortality among Older Adults with Chronic Kidney Disease on Conservative or on Replacement Therapy" Journal of Clinical Medicine 9, no. 12: 3965. https://doi.org/10.3390/jcm9123965
APA StyleLai, S., Amabile, M. I., Mazzaferro, S., Imbimbo, G., Mitterhofer, A. P., Galani, A., Aucella, F., Brunori, G., Menè, P., Molfino, A., & The Study Group on Geriatric Nephrology of the Italian Society of Nephrology (SIN). (2020). Association between Multidimensional Prognostic Index and Hospitalization and Mortality among Older Adults with Chronic Kidney Disease on Conservative or on Replacement Therapy. Journal of Clinical Medicine, 9(12), 3965. https://doi.org/10.3390/jcm9123965