Diagnostic Accuracy and Clinical Impact of Sentinel Lymph Node Sampling in Endometrial Cancer at High Risk of Recurrence: A Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Patients and Methods
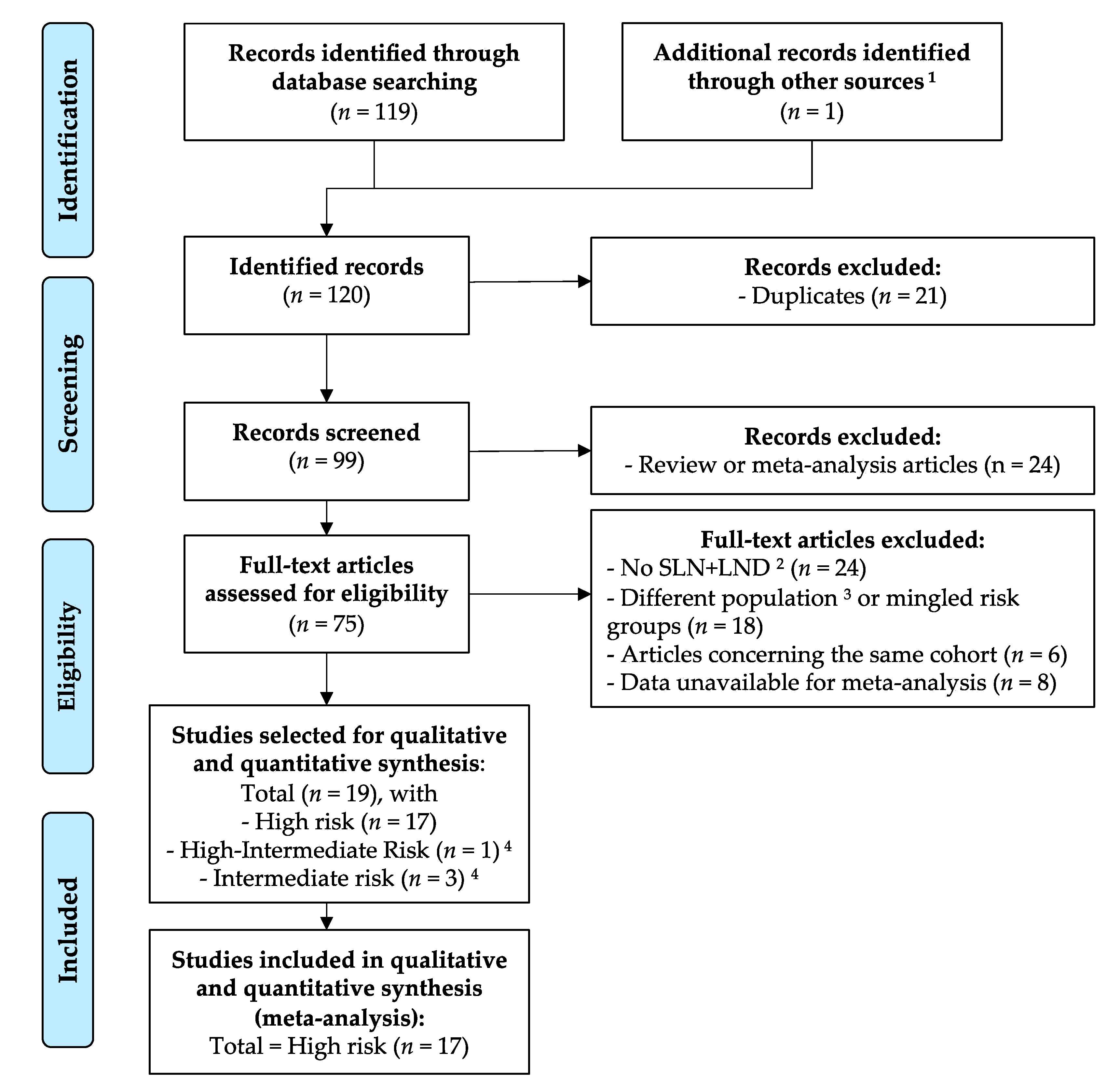
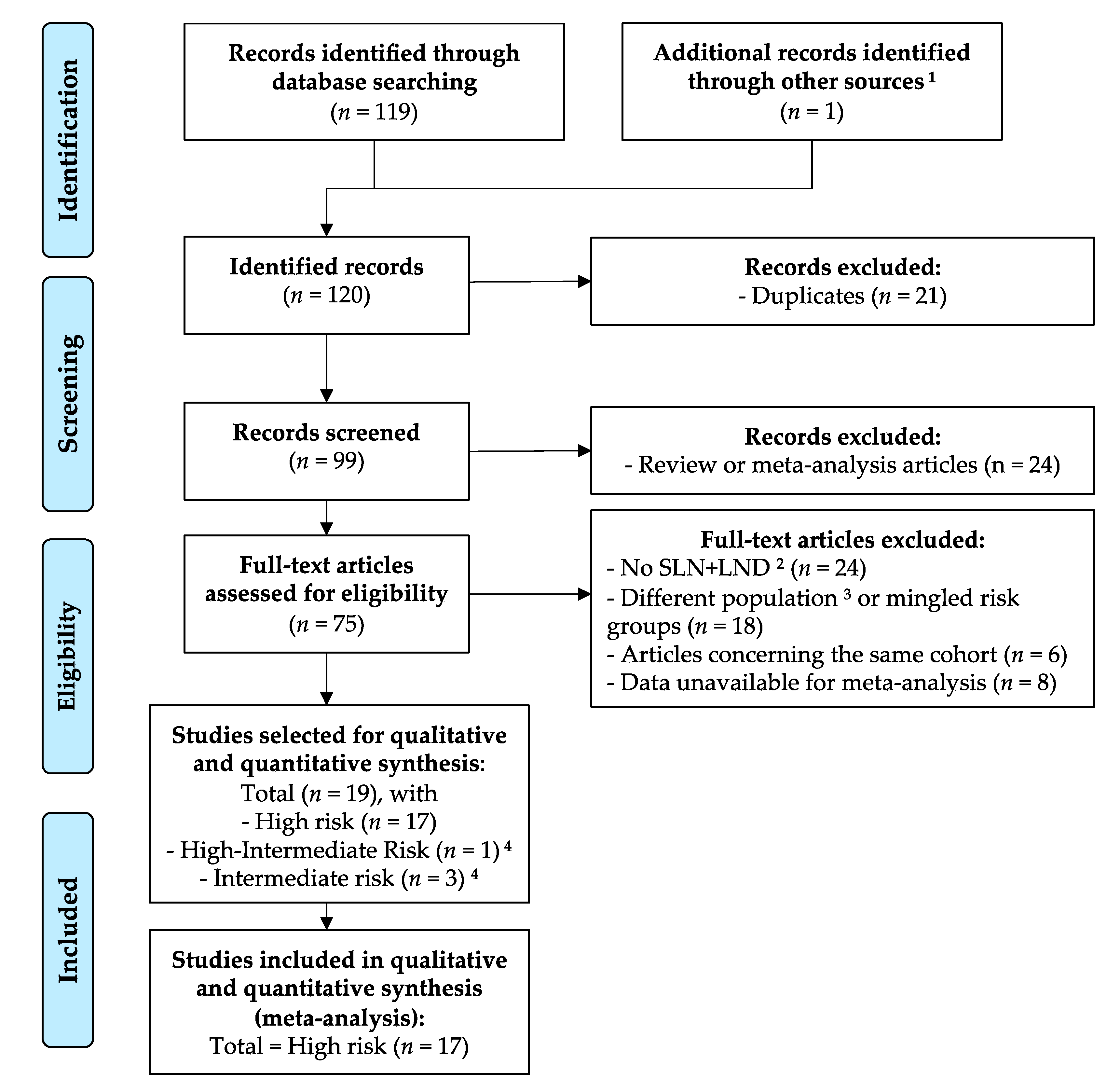
2.1. Bibliographic Selection
2.2. Inclusion Criteria
2.3. Data Extraction
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. SLN Techniques
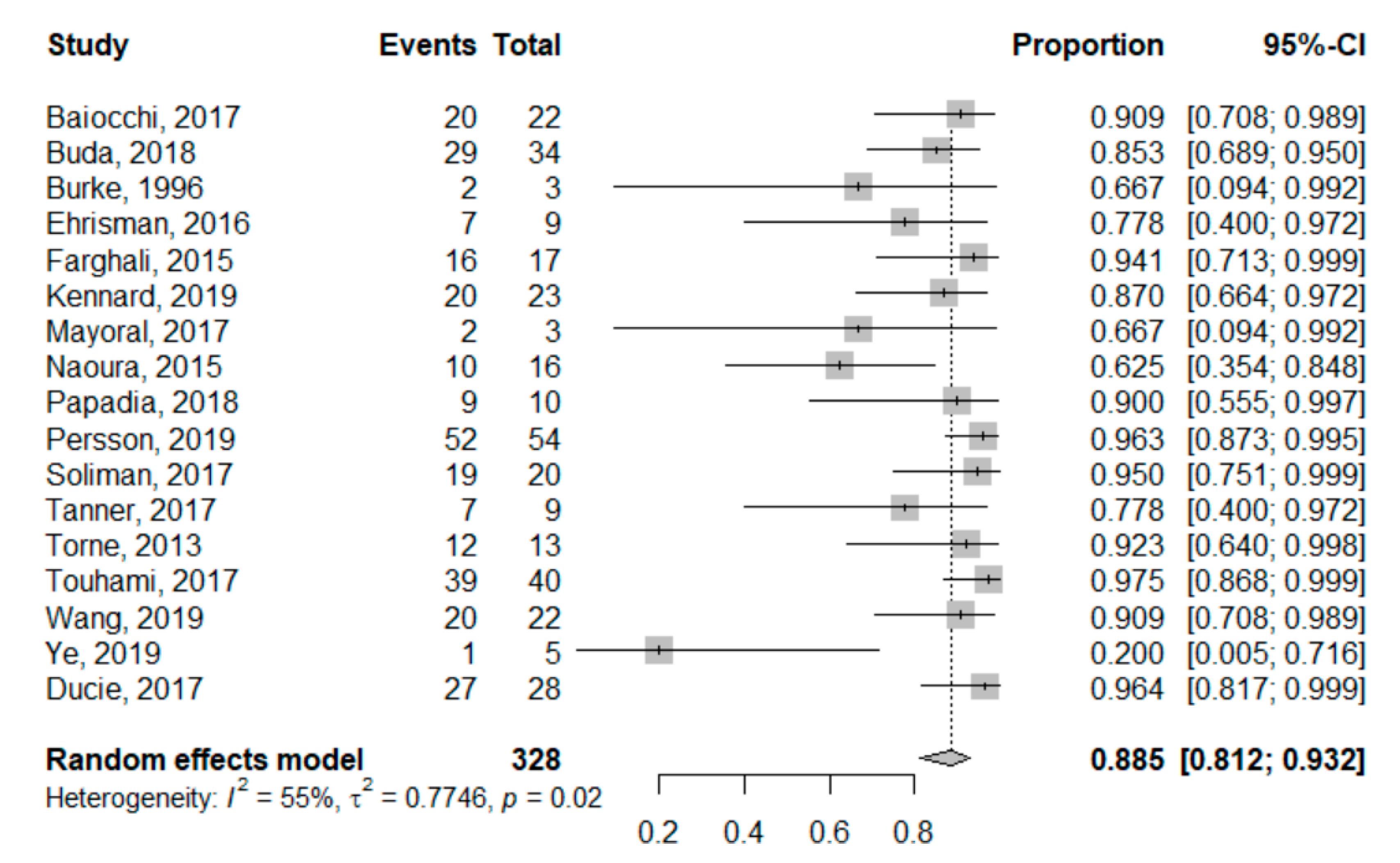
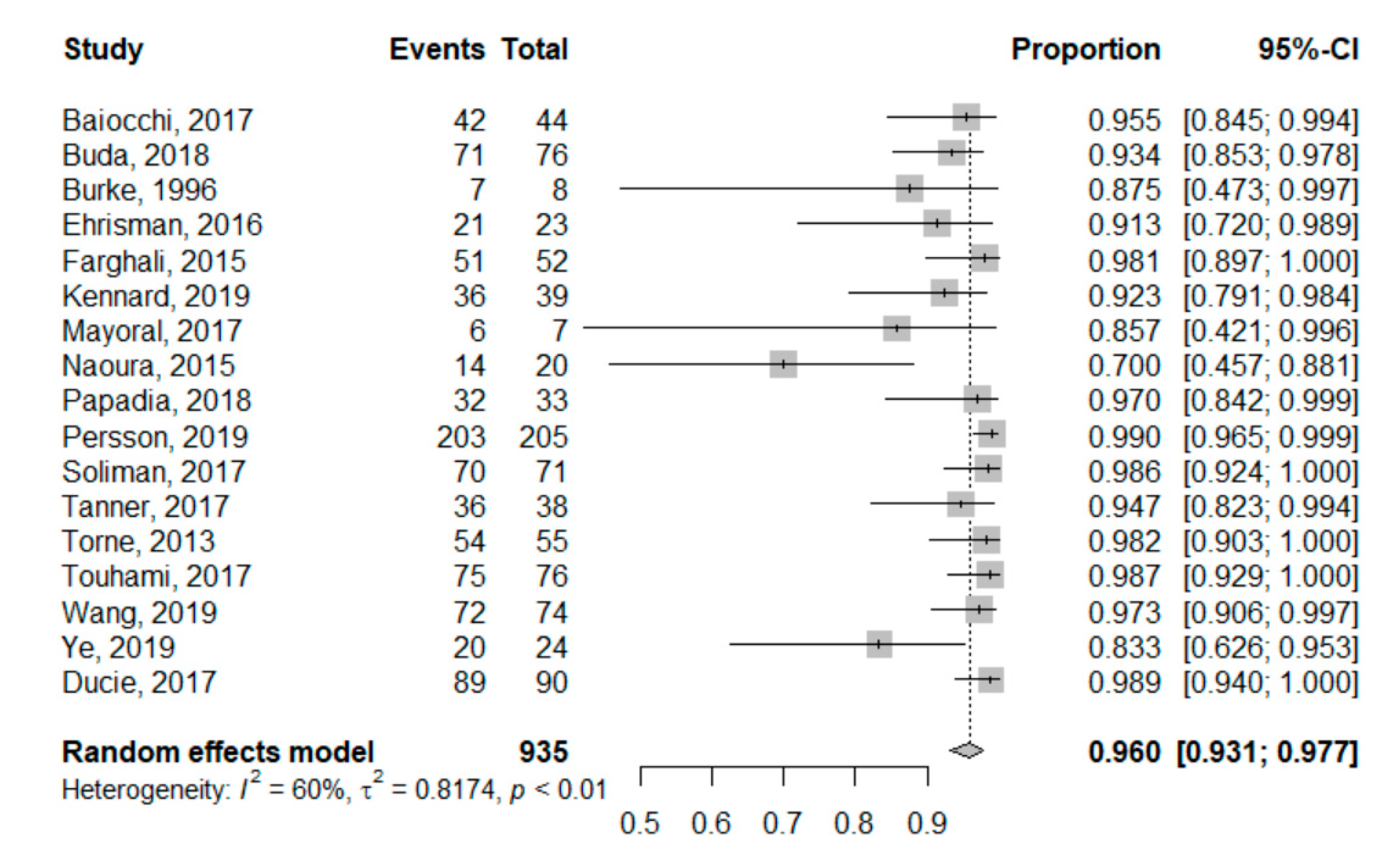
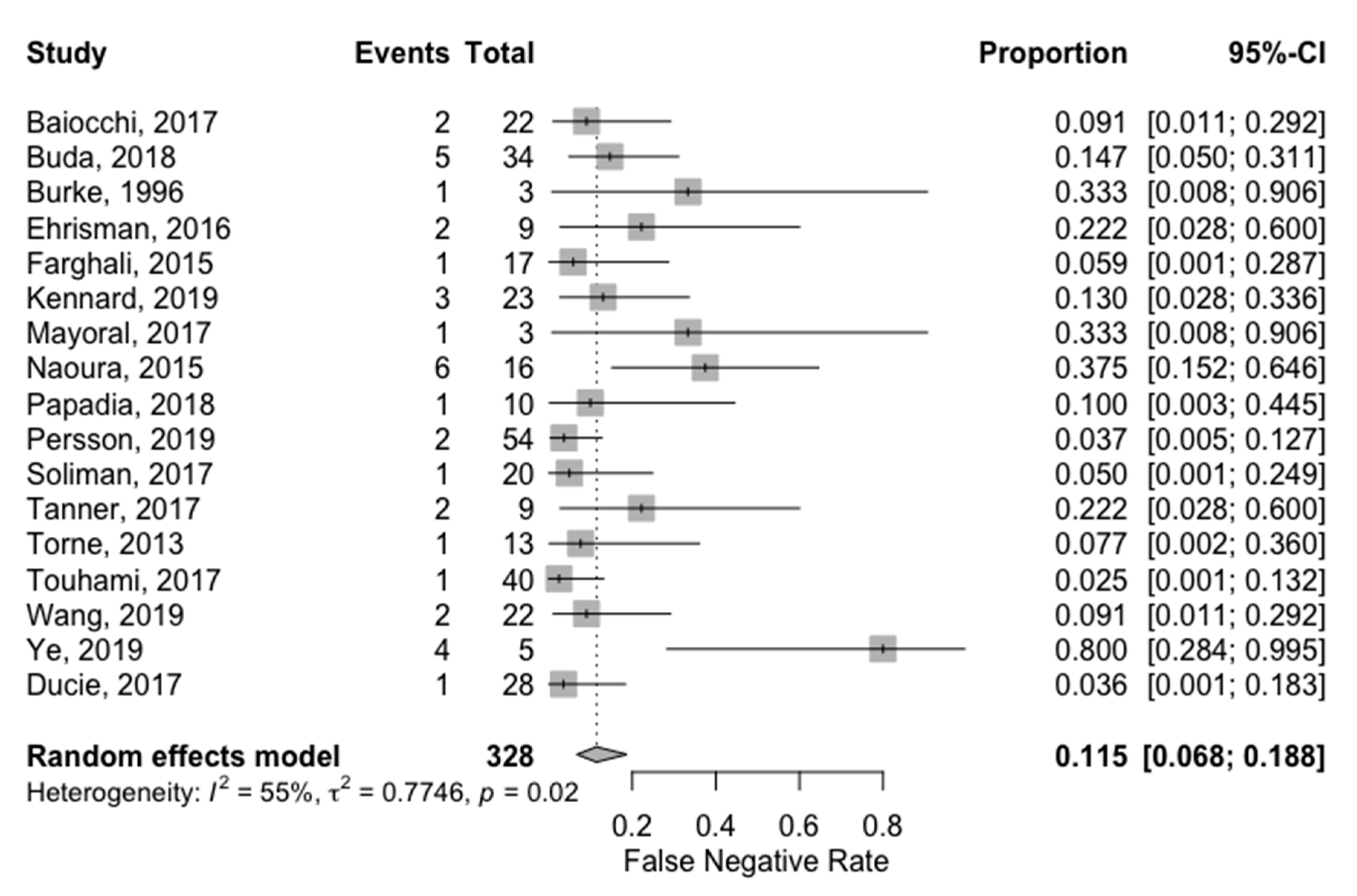
3.2. Detection Rates
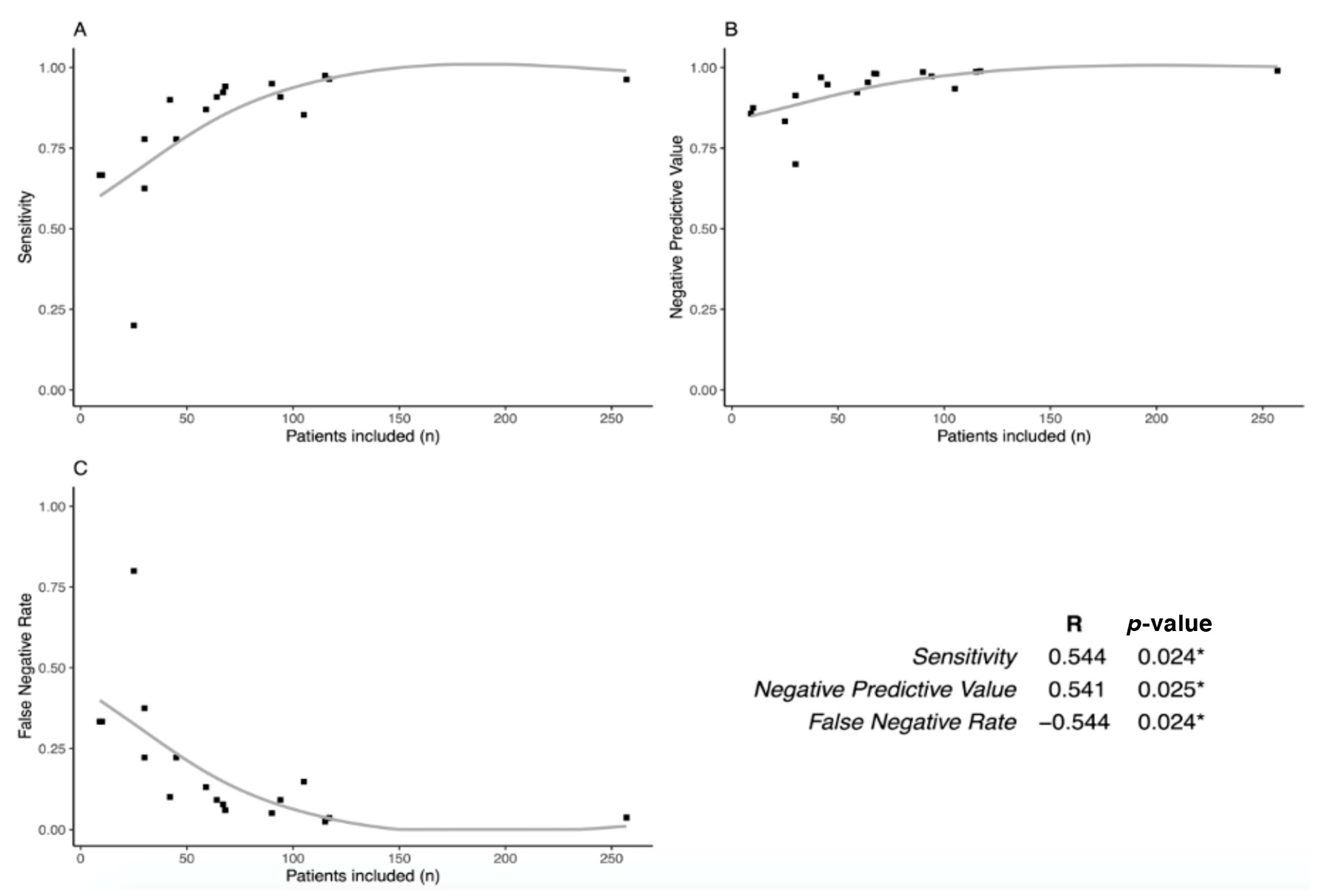
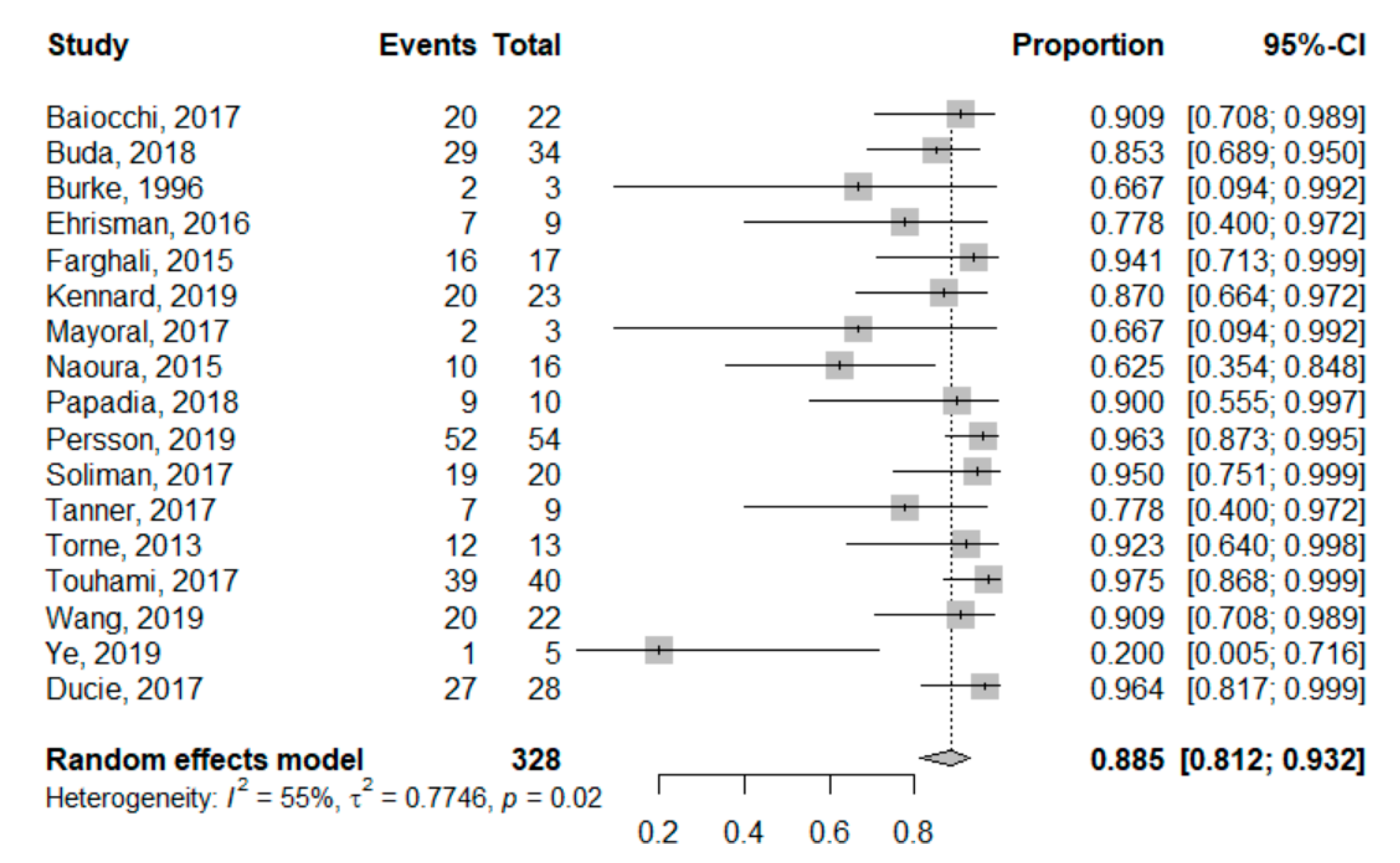
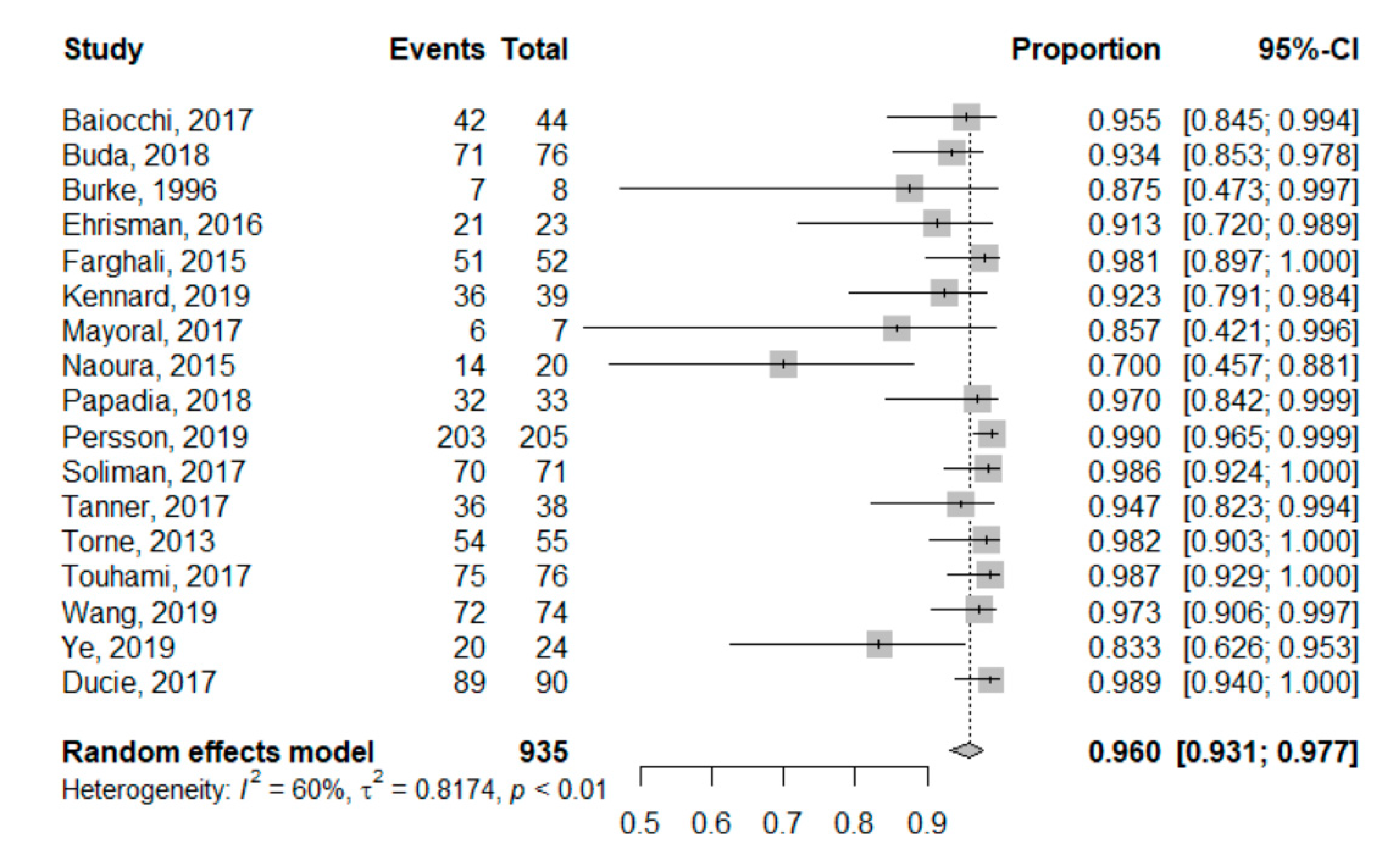
3.3. Global Measures of SLN Performance
3.4. Surgical Complications
3.5. Survival and Recurrence
4. Discussion
4.1. SLN Sampling is Also Feasible in High Risk Endometrial Cancer
4.2. SLN Sampling Performance in High Risk Endometrial Cancer
4.3. SLN Sampling Surgical Safety
4.4. SLN Sampling Contributes to Surgical De-Escalation in Endometrial Cancer
4.5. Limits of the Meta-Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. 2018. Available online: https://gco.iarc.fr/today (accessed on 8 October 2020).
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; Gonzalez-Martin, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.R.; et al. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: Diagnosis, Treatment and Follow-up. Int. J. Gynecol. Cancer 2016, 26, 2–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koh, W.J.; Abu-Rustum, N.R.; Bean, S.; Bradley, K.; Campos, S.M.; Cho, K.R.; Chon, H.S.; Chu, C.; Cohn, D.; Crispens, M.A.; et al. Uterine Neoplasms, Version 1.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2018, 16, 170–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Querleu, D.; Darai, E.; Lecuru, F.; Rafii, A.; Chereau, E.; Collinet, P.; Crochet, P.; Marret, H.; Mery, E.; Thomas, L.; et al. Primary management of endometrial carcinoma. Joint recommendations of the French society of gynecologic oncology (SFOG) and of the French college of obstetricians and gynecologists (CNGOF). Gynaecol. Obstet. Fertil. Senol. 2017, 45, 715–725. [Google Scholar] [CrossRef]
- Creutzberg, C.L.; van Putten, W.L.; Warlam-Rodenhuis, C.C.; van den Bergh, A.C.; de Winter, K.A.; Koper, P.C.; Lybeert, M.L.; Slot, A.; Lutgens, L.C.; Stenfert Kroese, M.C.; et al. Outcome of high-risk stage IC, grade 3, compared with stage I endometrial carcinoma patients: The Postoperative Radiation Therapy in Endometrial Carcinoma Trial. J. Clin. Oncol. 2004, 22, 1234–1241. [Google Scholar] [CrossRef] [PubMed]
- Ballester, M.; Dubernard, G.; Lecuru, F.; Heitz, D.; Mathevet, P.; Marret, H.; Querleu, D.; Golfier, F.; Leblanc, E.; Rouzier, R.; et al. Detection rate and diagnostic accuracy of sentinel-node biopsy in early stage endometrial cancer: A prospective multicentre study (SENTI-ENDO). Lancet Oncol. 2011, 12, 469–476. [Google Scholar] [CrossRef]
- Sanjuan, A.; Cobo, T.; Pahisa, J.; Escaramis, G.; Ordi, J.; Ayuso, J.R.; Garcia, S.; Hernandez, S.; Torne, A.; Martinez Roman, S.; et al. Preoperative and intraoperative assessment of myometrial invasion and histologic grade in endometrial cancer: Role of magnetic resonance imaging and frozen section. Int. J. Gynecol. Cancer 2006, 16, 385–390. [Google Scholar] [CrossRef]
- Epstein, E.; Blomqvist, L. Imaging in endometrial cancer. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 721–739. [Google Scholar] [CrossRef]
- Efficacy of systematic pelvic lymphadenectomy in endometrial cancer (MRC ASTEC trial): A randomised study. Lancet 2009, 373, 125–136. [CrossRef] [Green Version]
- Amant, F.; Mirza, M.R.; Koskas, M.; Creutzberg, C.L. Cancer of the corpus uteri. Int. J. Gynaecol. Obstet. 2018, 143 (Suppl. 2), 37–50. [Google Scholar] [CrossRef] [Green Version]
- Benedetti Panici, P.; Basile, S.; Maneschi, F.; Alberto Lissoni, A.; Signorelli, M.; Scambia, G.; Angioli, R.; Tateo, S.; Mangili, G.; Katsaros, D.; et al. Systematic pelvic lymphadenectomy vs. no lymphadenectomy in early-stage endometrial carcinoma: Randomized clinical trial. J. Natl. Cancer Inst. 2008, 100, 1707–1716. [Google Scholar] [CrossRef] [Green Version]
- Franchi, M.; Ghezzi, F.; Riva, C.; Miglierina, M.; Buttarelli, M.; Bolis, P. Postoperative complications after pelvic lymphadenectomy for the surgical staging of endometrial cancer. J. Surg. Oncol. 2001, 78, 232–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hidaka, T.; Kato, K.; Yonezawa, R.; Shima, T.; Nakashima, A.; Nagira, K.; Nakamura, T.; Saito, S. Omission of lymphadenectomy is possible for low-risk corpus cancer. Eur J. Surg. Oncol. 2007, 33, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Delpech, Y.; Coutant, C.; Darai, E.; Barranger, E. Sentinel lymph node evaluation in endometrial cancer and the importance of micrometastases. Surg. Oncol. 2008, 17, 237–245. [Google Scholar] [CrossRef]
- Bergstrom, J.; Aloisi, A.; Armbruster, S.; Yen, T.T.; Casarin, J.; Leitao, M.M., Jr.; Tanner, E.J.; Matsuno, R.; Machado, K.K.; Dowdy, S.C.; et al. Minimally invasive hysterectomy surgery rates for endometrial cancer performed at National Comprehensive Cancer Network (NCCN) Centers. Gynecol. Oncol. 2018, 148, 480–484. [Google Scholar] [CrossRef] [PubMed]
- Holloway, R.W.; Abu-Rustum, N.R.; Backes, F.J.; Boggess, J.F.; Gotlieb, W.H.; Jeffrey Lowery, W.; Rossi, E.C.; Tanner, E.J.; Wolsky, R.J. Sentinel lymph node mapping and staging in endometrial cancer: A Society of Gynecologic Oncology literature review with consensus recommendations. Gynecol. Oncol. 2017, 146, 405–415. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Balduzzi, S.; Rucker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Doebler, P.; Holling, H. Meta-Analysis of Diagnostic Accuracy, R package version 0.5.9; R Core Team: Vienna, Austria, 2019. [Google Scholar]
- Baiocchi, G.; Mantoan, H.; Kumagai, L.Y.; Goncalves, B.T.; Badiglian-Filho, L.; de Oliveira Menezes, A.N.; Faloppa, C.C.; De Brot, L.; da Costa, A. The Impact of Sentinel Node-Mapping in Staging High-Risk Endometrial Cancer. Ann. Surg. Oncol. 2017, 24, 3981–3987. [Google Scholar] [CrossRef]
- Buda, A.; Gasparri, M.L.; Puppo, A.; Mereu, L.; De Ponti, E.; Di Martino, G.; Novelli, A.; Tateo, S.; Muller, M.; Landoni, F.; et al. Lymph node evaluation in high-risk early stage endometrial cancer: A multi-institutional retrospective analysis comparing the sentinel lymph node (SLN) algorithm and SLN with selective lymphadenectomy. Gynecol. Oncol. 2018, 150, 261–266. [Google Scholar] [CrossRef]
- Burke, T.W.; Levenback, C.; Tornos, C.; Morris, M.; Wharton, J.T.; Gershenson, D.M. Intraabdominal lymphatic mapping to direct selective pelvic and paraaortic lymphadenectomy in women with high-risk endometrial cancer: Results of a pilot study. Gynecol. Oncol. 1996, 62, 169–173. [Google Scholar] [CrossRef]
- Ducie, J.A.; Eriksson, A.G.Z.; Ali, N.; McGree, M.E.; Weaver, A.L.; Bogani, G.; Cliby, W.A.; Dowdy, S.C.; Bakkum-Gamez, J.N.; Soslow, R.A.; et al. Comparison of a sentinel lymph node mapping algorithm and comprehensive lymphadenectomy in the detection of stage IIIC endometrial carcinoma at higher risk for nodal disease. Gynecol. Oncol. 2017, 147, 541–548. [Google Scholar] [CrossRef]
- Ehrisman, J.; Secord, A.A.; Berchuck, A.; Lee, P.S.; Di Santo, N.; Lopez-Acevedo, M.; Broadwater, G.; Valea, F.A.; Havrilesky, L.J. Performance of sentinel lymph node biopsy in high-risk endometrial cancer. Gynecol. Oncol. Rep. 2016, 17, 69–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farghali, M.M.; Allam, I.S.; Abdelazim, I.A.; El-Kady, O.S.; Rashed, A.R.; Gareer, W.Y.; Sweed, M.S. Accuracy of Sentinel Node in Detecting Lymph Node Metastasis in Primary Endometrial Carcinoma. Asian Pac. J. Cancer Prev. 2015, 16, 6691–6696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennard, J.A.; Stephens, A.J.; Ahmad, S.; Zhu, X.; Singh, C.; McKenzie, N.D.; Kendrick, J.E.; Holloway, R.W. Sentinel lymph nodes (SLN) in endometrial cancer: The relationship between primary tumor histology, SLN metastasis size, and non-sentinel node metastasis. Gynecol. Oncol. 2019, 154, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Mayoral, M.; Paredes, P.; Domenech, B.; Fuste, P.; Vidal-Sicart, S.; Tapias, A.; Torne, A.; Pahisa, J.; Ordi, J.; Pons, F.; et al. (18)F-FDG PET/CT and sentinel lymph node biopsy in the staging of patients with cervical and endometrial cancer. Role of dual-time-point imaging. Rev. Esp. Med. Nucl. Imagen Mol. 2017, 36, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Naoura, I.; Canlorbe, G.; Bendifallah, S.; Ballester, M.; Darai, E. Relevance of sentinel lymph node procedure for patients with high-risk endometrial cancer. Gynecol. Oncol. 2015, 136, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Papadia, A.; Gasparri, M.L.; Radan, A.P.; Stampfli, C.A.L.; Rau, T.T.; Mueller, M.D. Retrospective validation of the laparoscopic ICG SLN mapping in patients with grade 3 endometrial cancer. J. Cancer Res. Clin. Oncol. 2018, 144, 1385–1393. [Google Scholar] [CrossRef]
- Persson, J.; Salehi, S.; Bollino, M.; Lonnerfors, C.; Falconer, H.; Geppert, B. Pelvic Sentinel lymph node detection in High-Risk Endometrial Cancer (SHREC-trial)-the final step towards a paradigm shift in surgical staging. Eur. J. Cancer 2019, 116, 77–85. [Google Scholar] [CrossRef]
- Soliman, P.T.; Westin, S.N.; Dioun, S.; Sun, C.C.; Euscher, E.; Munsell, M.F.; Fleming, N.D.; Levenback, C.; Frumovitz, M.; Ramirez, P.T.; et al. A prospective validation study of sentinel lymph node mapping for high-risk endometrial cancer. Gynecol. Oncol. 2017, 146, 234–239. [Google Scholar] [CrossRef]
- Tanner, E.J.; Ojalvo, L.; Stone, R.L.; Levinson, K.; Temkin, S.M.; Murdock, T.; Vang, R.; Sinno, A.K.; Fader, A.N. The Utility of Sentinel Lymph Node Mapping in High-Grade Endometrial Cancer. Int. J. Gynecol. Cancer 2017, 27, 1416–1421. [Google Scholar] [CrossRef]
- Torne, A.; Pahisa, J.; Vidal-Sicart, S.; Martinez-Roman, S.; Paredes, P.; Puerto, B.; Albela, S.; Fuste, P.; Perisinotti, A.; Ordi, J. Transvaginal ultrasound-guided myometrial injection of radiotracer (TUMIR): A new method for sentinel lymph node detection in endometrial cancer. Gynecol. Oncol. 2013, 128, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Touhami, O.; Gregoire, J.; Renaud, M.C.; Sebastianelli, A.; Plante, M. Performance of sentinel lymph node (SLN) mapping in high-risk endometrial cancer. Gynecol. Oncol. 2017, 147, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Hu, Y.; He, Y.; Sun, P.; Guo, Z. A retrospective validation study of sentinel lymph node mapping for high-risk endometrial cancer. Arch. Gynecol. Obstet. 2019, 299, 1429–1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, L.; Li, S.; Lu, W.; He, Q.; Li, Y.; Li, B.; Wang, X.; Yan, Q.; Wan, X. A Prospective Study of Sentinel Lymph Node Mapping for Endometrial Cancer: Is It Effective in High-Risk Subtypes? Oncologist 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selman, T.J.; Mann, C.H.; Zamora, J.; Khan, K.S. A systematic review of tests for lymph node status in primary endometrial cancer. BMC Womens Health 2008, 8, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodurtha Smith, A.J.; Fader, A.N.; Tanner, E.J. Sentinel lymph node assessment in endometrial cancer: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2017, 216, 459–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, S.; Yoo, H.J.; Hwang, J.H.; Lim, M.C.; Seo, S.S.; Park, S.Y. Sentinel lymph node biopsy in endometrial cancer: Meta-analysis of 26 studies. Gynecol. Oncol. 2011, 123, 522–527. [Google Scholar] [CrossRef]
- Buda, A.; Bussi, B.; Di Martino, G.; Di Lorenzo, P.; Palazzi, S.; Grassi, T.; Milani, R. Sentinel Lymph Node Mapping With Near-Infrared Fluorescent Imaging Using Indocyanine Green: A New Tool for Laparoscopic Platform in Patients With Endometrial and Cervical Cancer. J. Minim. Invasive Gynecol. 2016, 23, 265–269. [Google Scholar] [CrossRef]
- Buda, A.; Di Martino, G.; Vecchione, F.; Bussi, B.; Dell’Anna, T.; Palazzi, S.; Cantu, M.G.; Marchette, M.D.; Milani, R. Optimizing Strategies for Sentinel Lymph Node Mapping in Early-Stage Cervical and Endometrial Cancer: Comparison of Real-Time Fluorescence With Indocyanine Green and Methylene Blue. Int. J. Gynecol. Cancer 2015, 25, 1513–1518. [Google Scholar] [CrossRef]
- Rossi, E.C.; Ivanova, A.; Boggess, J.F. Robotically assisted fluorescence-guided lymph node mapping with ICG for gynecologic malignancies: A feasibility study. Gynecol. Oncol. 2012, 124, 78–82. [Google Scholar] [CrossRef]
- Rossi, E.C.; Jackson, A.; Ivanova, A.; Boggess, J.F. Detection of sentinel nodes for endometrial cancer with robotic assisted fluorescence imaging: Cervical versus hysteroscopic injection. Int. J. Gynecol. Cancer 2013, 23, 1704–1711. [Google Scholar] [CrossRef] [PubMed]
- Plante, M.; Touhami, O.; Trinh, X.B.; Renaud, M.C.; Sebastianelli, A.; Grondin, K.; Gregoire, J. Sentinel node mapping with indocyanine green and endoscopic near-infrared fluorescence imaging in endometrial cancer. A pilot study and review of the literature. Gynecol. Oncol. 2015, 137, 443–447. [Google Scholar] [CrossRef] [PubMed]
- How, J.; Gotlieb, W.H.; Press, J.Z.; Abitbol, J.; Pelmus, M.; Ferenczy, A.; Probst, S.; Gotlieb, R.; Brin, S.; Lau, S. Comparing indocyanine green, technetium, and blue dye for sentinel lymph node mapping in endometrial cancer. Gynecol. Oncol. 2015, 137, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Ruscito, I.; Gasparri, M.L.; Braicu, E.I.; Bellati, F.; Raio, L.; Sehouli, J.; Mueller, M.D.; Panici, P.B.; Papadia, A. Sentinel Node Mapping in Cervical and Endometrial Cancer: Indocyanine Green Versus Other Conventional Dyes-A Meta-Analysis. Ann. Surg. Oncol. 2016, 23, 3749–3756. [Google Scholar] [CrossRef] [PubMed]
- Cormier, B.; Rozenholc, A.T.; Gotlieb, W.; Plante, M.; Giede, C. Communities of Practice Group of Society of Gynecologic Oncology of, C. Sentinel lymph node procedure in endometrial cancer: A systematic review and proposal for standardization of future research. Gynecol. Oncol. 2015, 138, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, F.; Ditto, A.; Bogani, G.; Leone Roberti Maggiore, U.; Signorelli, M.; Chiappa, V.; Raspagliesi, F. Sentinel lymph node mapping in endometrial cancer: Performance of hysteroscopic injection of tracers. Int. J. Gynecol. Cancer 2020, 30, 332–338. [Google Scholar] [CrossRef]
- Solima, E.; Martinelli, F.; Ditto, A.; Maccauro, M.; Carcangiu, M.; Mariani, L.; Kusamura, S.; Fontanelli, R.; Grijuela, B.; Raspagliesi, F. Diagnostic accuracy of sentinel node in endometrial cancer by using hysteroscopic injection of radiolabeled tracer. Gynecol. Oncol. 2012, 126, 419–423. [Google Scholar] [CrossRef]
- Levinson, K.L.; Mahdi, H.; Escobar, P.F. Feasibility and optimal dosage of indocyanine green fluorescence for sentinel lymph node detection using robotic single-site instrumentation: Preclinical study. J. Minim. Invasive Gynecol. 2013, 20, 691–696. [Google Scholar] [CrossRef]
- Sinno, A.K.; Fader, A.N.; Roche, K.L.; Giuntoli, R.L., 2nd; Tanner, E.J. A comparison of colorimetric versus fluorometric sentinel lymph node mapping during robotic surgery for endometrial cancer. Gynecol. Oncol. 2014, 134, 281–286. [Google Scholar] [CrossRef]
- Frumovitz, M.; Plante, M.; Lee, P.S.; Sandadi, S.; Lilja, J.F.; Escobar, P.F.; Gien, L.T.; Urbauer, D.L.; Abu-Rustum, N.R. Near-infrared fluorescence for detection of sentinel lymph nodes in women with cervical and uterine cancers (FILM): A randomised, phase 3, multicentre, non-inferiority trial. Lancet Oncol. 2018, 19, 1394–1403. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.H.; Soslow, R.A.; Park, K.J.; Barber, E.L.; Khoury-Collado, F.; Barlin, J.N.; Sonoda, Y.; Hensley, M.L.; Barakat, R.R.; Abu-Rustum, N.R. Pathologic ultrastaging improves micrometastasis detection in sentinel lymph nodes during endometrial cancer staging. Int. J. Gynecol. Cancer 2013, 23, 964–970. [Google Scholar] [CrossRef] [PubMed]
- Frost, J.A.; Webster, K.E.; Bryant, A.; Morrison, J. Lymphadenectomy for the management of endometrial cancer. Cochrane Database Syst. Rev. 2017, 10, CD007585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, J.K.; Cheung, M.K.; Huh, W.K.; Osann, K.; Husain, A.; Teng, N.N.; Kapp, D.S. Therapeutic role of lymph node resection in endometrioid corpus cancer: A study of 12,333 patients. Cancer 2006, 107, 1823–1830. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
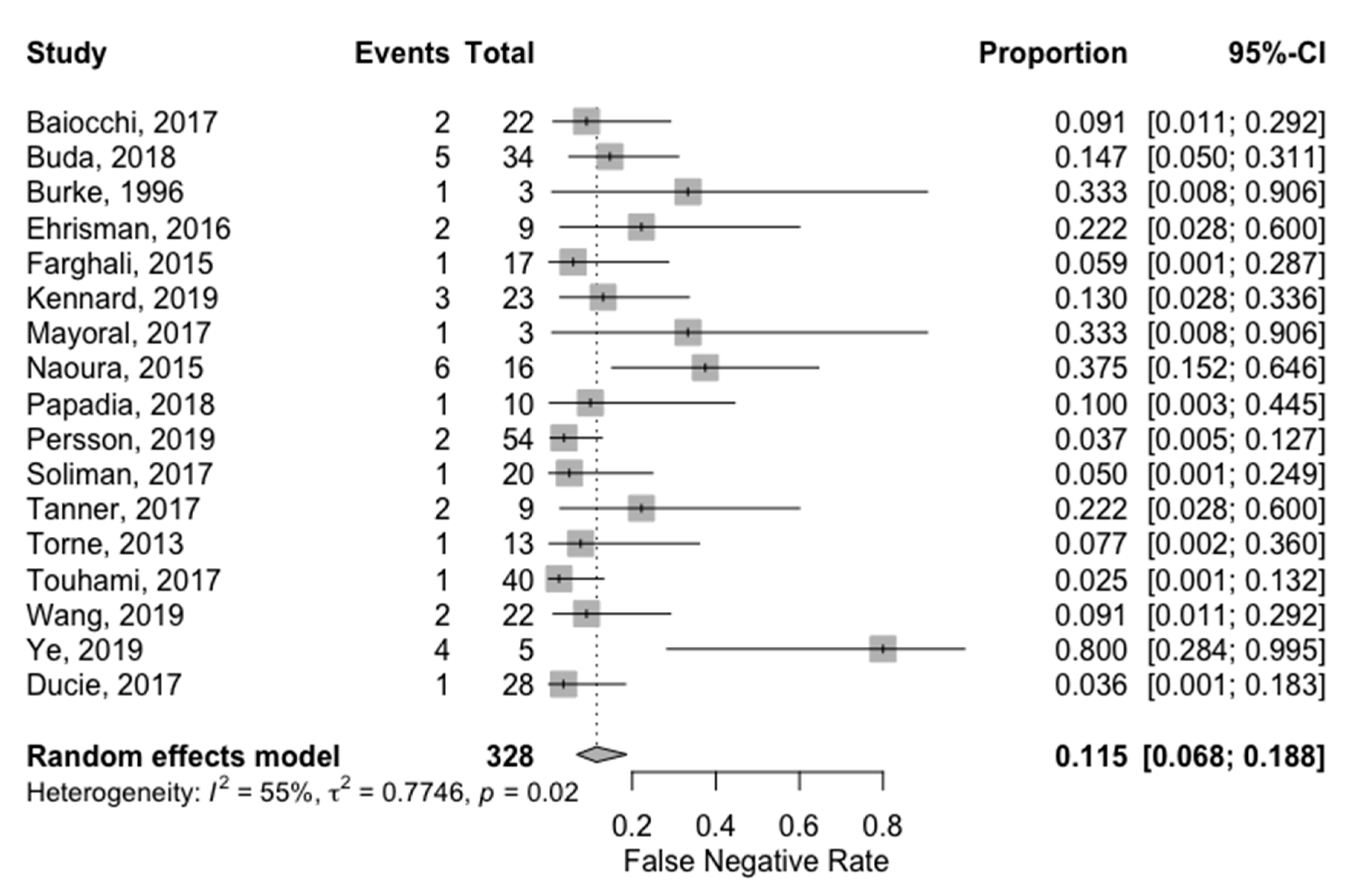
| Study (Author, Year, Country) | Sentinel Lymph Node Mapping Technique | Surgical Approach | Lymphadenectomy Areas | Total Population Included | Unilateral Detection Rate | Bilateral Detection Rate | True Positive | False Positive | False Negative | True Negative | Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value | False Negative Rate | Prevalence (N+ Patients) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baiocchi, 2017, Brazil | BD, cervical injection | Laparoscopy or robotic-assisted laparoscopy | Pelvic with or without para-aortic | 75 | 85% | 60% | 20 | 0 | 2 | 42 | 90.90% | 100% | 100% | 95.50% | 9.10% | 34.38% |
| Buda, 2018, Italy and Switzerland | BD + RC or ICG, cervical injection | Not available | Pelvic with or without para-aortic | 105 | 98% | 80% | 29 | 0 | 5 | 71 | 85.30% | 100% | 100% | 93.40% | 14.70% | 32.38% |
| Burke, 1996, United States | BD (isosulfan), subserosal myometrium injection | Laparotomy | Pelvic and para-aortic | 15 | 67% | -- | 2 | 0 | 1 | 7 | 66.70% | 100% | 100% | 87.50% | 33.30% | 30.00% |
| Ducie, 2017, United States | BD (methylene or isosulfan) or ICG, cervical injection | Not available | Pelvic with or without para-aortic | 117 | -- | -- | 27 | 0 | 1 | 89 | 96.40% | 100% | 100% | 98.90% | 3.60% | 23.93% |
| Ehrisman, 2016, United States | BD or ICG, cervical injection | Laparoscopy or robotic-assisted laparoscopy | Pelvic with or without para-aortic | 36 | 83% | 56% | 7 | 0 | 2 | 21 | 77.80% | 100% | 100% | 91.30% | 22.20% | 30.00% |
| Farghali, 2015, Egypt | BD (methylene), subserosal myometrium injection | Laparotomy | Pelvic and para-aortic | 93 | 73% | 41% | 16 | 0 | 1 | 51 | 94.10% | 100% | 100% | 98.10% | 5.90% | 25.00% |
| Kennard, 2019, United States | ICG with or without BD, cervical injection | Robotic-assisted laparoscopy | Pelvic with or without para-aortic | 59 | -- | -- | 20 | 0 | 3 | 36 | 87.00% | 100% | 100% | 92.30% | 13.00% | 38.98% |
| Mayoral, 2017, Spain | RC, subserosal myometrium injection | Laparoscopy | Pelvic and para-aortic | 11 | 82% | -- | 2 | 0 | 1 | 6 | 66.70% | 100% | 100% | 85.70% | 33.30% | 33.33% |
| Naoura, 2015, France | BD and RC, cervical injection | Not available | Pelvic with or without para-aortic | 34 | 88% | 59% | 10 | 0 | 6 | 14 | 62.50% | 100% | 100% | 70.00% | 37.50% | 53.33% |
| Papadia, 2018, Switzerland | ICG, cervical injection | Laparoscopy | Pelvic and para-aortic | 42 | 100% | 90% | 9 | 0 | 1 | 32 | 90.00% | 100% | 100% | 97.00% | 10.00% | 23.81% |
| Persson, 2019, Sweden | ICG, cervical injection with or without reinjection | Robotic-assisted laparoscopy | Pelvic and para-aortic | 257 | 100% | 95% | 52 | 0 | 2 | 203 | 96.30% | 100% | 100% | 99.00% | 3.70% | 21.01% |
| Soliman, 2017, United States | BD, ICG, or RC, alone or combination, cervical injection | Laparoscopy or robotic-assisted laparoscopy or laparotomy | Pelvic and para-aortic | 101 | 89% | 58% | 19 | 0 | 1 | 70 | 95.00% | 100% | 100% | 98.60% | 5.00% | 22.22% |
| Tanner, 2017, United States | BD (isosulfan) or ICG, cervical injection | Robotic-assisted laparoscopy | Pelvic with or without para-aortic | 52 | 87% | 60% | 7 | 0 | 2 | 36 | 77.80% | 100% | 100% | 94.70% | 22.20% | 20.00% |
| Torne, 2013, Spain | RC, subserosal myometrium injection | Laparoscopy | Pelvic and para-aortic | 74 | 91% | -- | 12 | 0 | 1 | 54 | 92.30% | 100% | 100% | 98.20% | 7.70% | 19.40% |
| Touhami, 2017, Canada | BD, ICG, or RC, alone or combination, cervical injection | Laparoscopy or robotic-assisted laparoscopy or laparotomy | Pelvic with or without para-aortic | 128 | 90% | 63% | 39 | 0 | 1 | 75 | 97.50% | 100% | 100% | 98.70% | 2.50% | 34.78% |
| Wang, 2019, China | ICG, cervical injection | Laparoscopy | Pelvic and para-aortic | 98 | 96% | 78% | 20 | 0 | 2 | 72 | 90.90% | 100% | 100% | 97.30% | 9.10% | 23.40% |
| Ye, 2019, China | ICG, cervical injection | Laparoscopy | Pelvic and para-aortic | 25 | 100% | 72% | 1 | 0 | 4 | 20 | 20.00% | 100% | 100% | 83.30% | 80.00% | 20.00% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lecointre, L.; Lodi, M.; Faller, É.; Boisramé, T.; Agnus, V.; Baldauf, J.-J.; Gallix, B.; Akladios, C. Diagnostic Accuracy and Clinical Impact of Sentinel Lymph Node Sampling in Endometrial Cancer at High Risk of Recurrence: A Meta-Analysis. J. Clin. Med. 2020, 9, 3874. https://doi.org/10.3390/jcm9123874
Lecointre L, Lodi M, Faller É, Boisramé T, Agnus V, Baldauf J-J, Gallix B, Akladios C. Diagnostic Accuracy and Clinical Impact of Sentinel Lymph Node Sampling in Endometrial Cancer at High Risk of Recurrence: A Meta-Analysis. Journal of Clinical Medicine. 2020; 9(12):3874. https://doi.org/10.3390/jcm9123874
Chicago/Turabian StyleLecointre, Lise, Massimo Lodi, Émilie Faller, Thomas Boisramé, Vincent Agnus, Jean-Jacques Baldauf, Benoît Gallix, and Chérif Akladios. 2020. "Diagnostic Accuracy and Clinical Impact of Sentinel Lymph Node Sampling in Endometrial Cancer at High Risk of Recurrence: A Meta-Analysis" Journal of Clinical Medicine 9, no. 12: 3874. https://doi.org/10.3390/jcm9123874