MRI Characteristics Accurately Predict Biochemical Recurrence after Radical Prostatectomy

 , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Experimental Section
2.1. Patient Selection, Assessment, Treatment, and Follow-Up
2.2. MRI Protocol
2.3. BCR
2.4. Statistical Analyses
3. Results
3.1. Population Characteristics
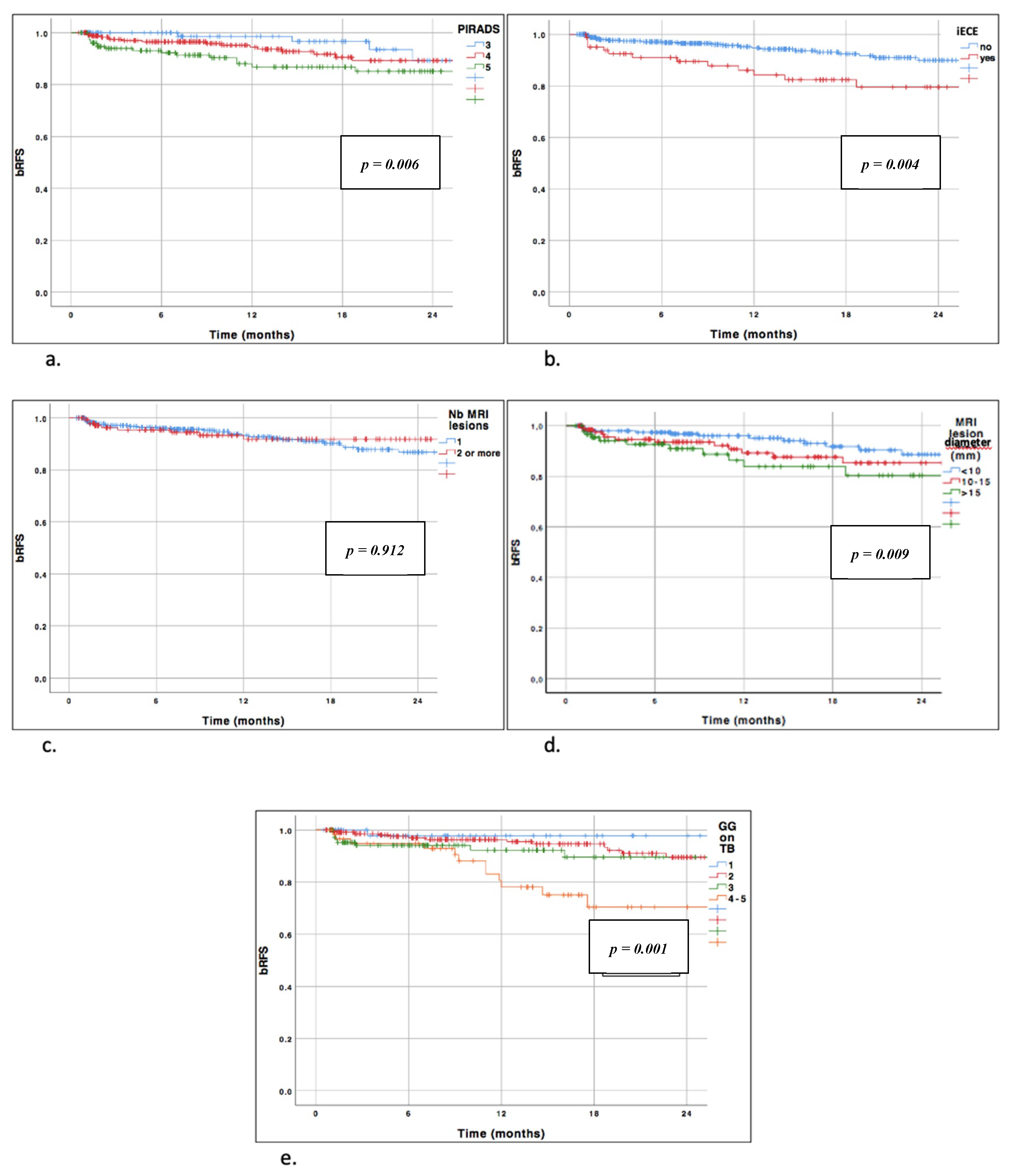
3.2. BCR-Free Survival According to PI-RADS Score
3.3. BCR-Free Survival According to ECE on MRI
3.4. BCR-Free Survival According to Number of MRI Lesions
3.5. BCR-Free Survival According to Maximal Lesion Diameter
3.6. BCR-Free Survival According to ISUP Grade Group in Targeted Biopsy
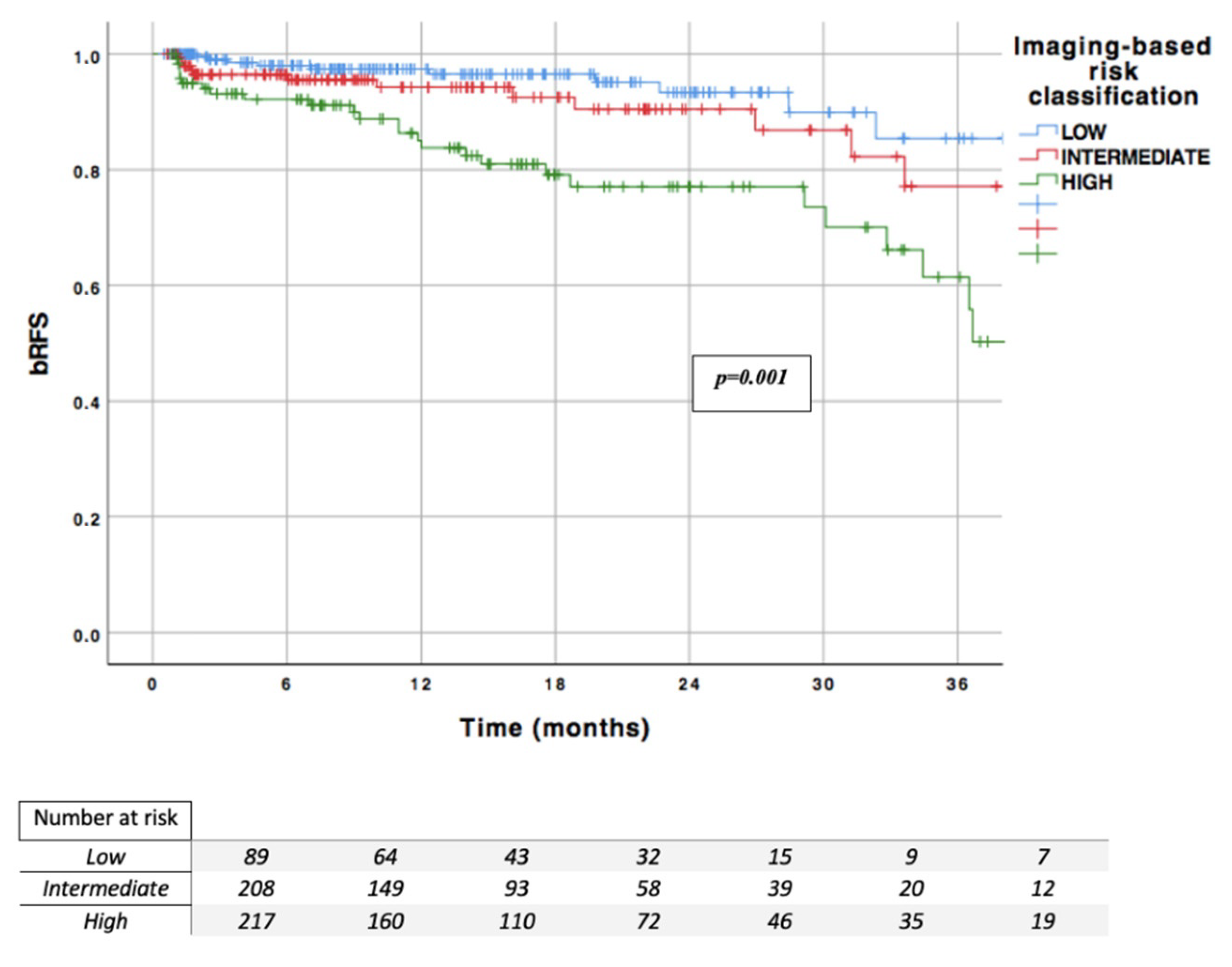
3.7. MRI Imaging-Based Risk Classification
- Low risk, which includes no ECE on MRI, ISUP grade group 1–2 in TB, and PI-RADS < 5
- Intermediate risk, which includes PI-RADS = 5 or ISUP grade group 3 in TB with no ECE MRI
- High-risk, which includes ECE on MRI or ISUP grade group 4–5 in TB (regardless of the PI-RADS)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; Bellmunt, J.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; De Santis, M.; Fossati, N.; Gross, T.; Henry, A.M.; Joniau, S.; et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2017, 71, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Van den Broeck, T.; van den Bergh, R.C.N.; Arfi, N.; Gross, T.; Moris, L.; Briers, E.; Cumberbatch, M.; De Santis, M.; Tilki, D.; Fanti, S.; et al. Prognostic Value of Biochemical Recurrence Following Treatment with Curative Intent for Prostate Cancer: A Systematic Review. Eur. Urol. 2019, 75, 967–987. [Google Scholar] [CrossRef] [PubMed]
- Rouvière, O.; Puech, P.; Renard-Penna, R.; Claudon, M.; Roy, C.; Mège-Lechevallier, F.; Decaussin-Petrucci, M.; Dubreuil-Chambardel, M.; Magaud, L.; Remontet, L.; et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients (MRI-FIRST): A prospective, multicentre, paired diagnostic study. Lancet Oncol. 2019, 20, 100–109. [Google Scholar] [CrossRef]
- Siddiqui, M.M.; George, A.K.; Rubin, R.; Rais-Bahrami, S.; Parnes, H.L.; Merino, M.J.; Simon, R.M.; Turkbey, B.; Choyke, P.L.; Wood, B.J.; et al. Efficiency of Prostate Cancer Diagnosis by MR/Ultrasound Fusion-Guided Biopsy vs Standard Extended-Sextant Biopsy for MR-Visible Lesions. J. Natl. Cancer Inst. 2016, 108, djw039. [Google Scholar] [CrossRef] [PubMed]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef] [PubMed]
- van der Leest, M.; Cornel, E.; Israël, B.; Hendriks, R.; Padhani, A.R.; Hoogenboom, M.; Zamecnik, P.; Bakker, D.; Setiasti, A.Y.; Veltman, J.; et al. Head-to-head Comparison of Transrectal Ultrasound-guided Prostate Biopsy Versus Multiparametric Prostate Resonance Imaging with Subsequent Magnetic Resonance-guided Biopsy in Biopsy-naïve Men with Elevated Prostate-specific Antigen: A Large Prospective Multicenter Clinical Study. Eur. Urol. 2019, 75, 570–578. [Google Scholar] [CrossRef]
- Ho, R.; Siddiqui, M.M.; George, A.K.; Frye, T.; Kilchevsky, A.; Fascelli, M.; Shakir, N.A.; Chelluri, R.; Abboud, S.F.; Walton-Diaz, A.; et al. Preoperative Multiparametric Magnetic Resonance Imaging Predicts Biochemical Recurrence in Prostate Cancer after Radical Prostatectomy. PLoS ONE 2016, 11, e0157313. [Google Scholar] [CrossRef]
- Park, S.Y.; Oh, Y.T.; Jung, D.C.; Cho, N.H.; Choi, Y.D.; Rha, K.H.; Hong, S.J. Prediction of biochemical recurrence after radical prostatectomy with PI-RADS version 2 in prostate cancers: Initial results. Eur. Radiol. 2016, 26, 2502–2509. [Google Scholar] [CrossRef]
- Kim, R.; Kim, C.K.; Park, J.J.; Kim, J.-H.; Seo, S.I.; Jeon, S.S.; Lee, H.M. Prognostic Significance for Long-Term Outcomes Following Radical Prostatectomy in Men with Prostate Cancer: Evaluation with Prostate Imaging Reporting and Data System Version 2. Korean J. Radiol. 2019, 20, 256. [Google Scholar] [CrossRef]
- Manceau, C.; Beauval, J.-B.; Lesourd, M.; Almeras, C.; Gautier, J.-R.; Soulié, M.; Loison, G.; Salin, A.; Tollon, C.; Malavaud, B.; et al. Confirmation by Early Oncologic Outcomes After Surgery of the Accuracy of Intermediate-risk Prostate Cancer Classification Based on Magnetic Resonance Imaging Staging and Targeted Biopsy. Eur. Urol. Open Sci. 2020, 21, 5–8. [Google Scholar] [CrossRef]
- Epstein, J.I.; Zelefsky, M.J.; Sjoberg, D.D.; Nelson, J.B.; Egevad, L.; Magi-Galluzzi, C.; Vickers, A.J.; Parwani, A.V.; Reuter, V.E.; Fine, S.W.; et al. A Contemporary Prostate Cancer Grading System: A Validated Alternative to the Gleason Score. Eur. Urol. 2016, 69, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Barentsz, J.O.; Richenberg, J.; Clements, R.; Choyke, P.; Verma, S.; Villeirs, G.; Rouviere, O.; Logager, V.; Fütterer, J.J. ESUR prostate MR guidelines 2012. Eur. Radiol. 2012, 22, 746–757. [Google Scholar] [CrossRef]
- Barentsz, J.O.; Weinreb, J.C.; Verma, S.; Thoeny, H.C.; Tempany, C.M.; Shtern, F.; Padhani, A.R.; Margolis, D.; Macura, K.J.; Haider, M.A.; et al. Synopsis of the PI-RADS v2 Guidelines for Multiparametric Prostate Magnetic Resonance Imaging and Recommendations for Use. Eur. Urol. 2016, 69, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Sanda, M.G.; Chen, R.C.; Crispino, T.; Freedland, S.; Greene, K.; Klotz, L.H.; Makarov, D.V.; Reston, J.; Rodrigues, G.; Sandler, H.M.; et al. Clinically localized prostate cancer: AUA/ASTRO/SUO guideline. Prostate Cancer 2017, 6, 27. [Google Scholar]
- Rozet, F.; Hennequin, C.; Beauval, J.-B.; Beuzeboc, P.; Cormier, L.; Fromont-Hankard, G.; Mongiat-Artus, P.; Ploussard, G.; Mathieu, R.; Brureau, L.; et al. Recommandations françaises du Comité de Cancérologie de l’AFU – Actualisation 2018–2020: Cancer de la prostate. Prog. En Urol. 2018, 28, S79–S130. [Google Scholar] [CrossRef]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Schultz, D.; Blank, K.; Broderick, G.A.; Tomaszewski, J.E.; Renshaw, A.A.; Kaplan, I.; Beard, C.J.; et al. Biochemical Outcome after Radical Prostatectomy, External Beam Radiation Therapy, or Interstitial Radiation Therapy for Clinically Localized Prostate Cancer. JAMA 1998, 280, 969–974. [Google Scholar] [CrossRef]
- Diamand, R.; Oderda, M.; Al Hajj Obeid, W.; Albisinni, S.; Van Velthoven, R.; Fasolis, G.; Simone, G.; Ferriero, M.; Roche, J.-B.; Piechaud, T.; et al. A multicentric study on accurate grading of prostate cancer with systematic and MRI/US fusion targeted biopsies: Comparison with final histopathology after radical prostatectomy. World J. Urol. 2019, 37, 2109–2117. [Google Scholar] [CrossRef]
- Drost, F.-J.H.; Osses, D.F.; Nieboer, D.; Steyerberg, E.W.; Bangma, C.H.; Roobol, M.J.; Schoots, I.G. Prostate MRI, with or without MRI-targeted biopsy, and systematic biopsy for detecting prostate cancer. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef]
- Ploussard, G.; Beauval, J.B.; Lesourd, M.; Almeras, C.; Assoun, J.; Aziza, R.; Gautier, J.R.; Loison, G.; Portalez, D.; Salin, A.; et al. Added value of concomitant systematic biopsies for grade group prediction based on radical prostatectomy final pathology in MRI-positive patients undergoing fusion targeted biopsies. J. Urol. 2019, 202, 1182–1187. [Google Scholar] [CrossRef]
- Radtke, J.P.; Wiesenfarth, M.; Kesch, C.; Freitag, M.T.; Alt, C.D.; Celik, K.; Distler, F.; Roth, W.; Wieczorek, K.; Stock, C.; et al. Combined Clinical Parameters and Multiparametric Magnetic Resonance Imaging for Advanced Risk Modeling of Prostate Cancer—Patient-tailored Risk Stratification Can Reduce Unnecessary Biopsies. Eur. Urol. 2017, 72, 888–896. [Google Scholar] [CrossRef] [PubMed]
- Freedland, S.J.; Humphreys, E.B.; Mangold, L.A.; Eisenberger, M.; Partin, A.W. Time to Prostate Specific Antigen Recurrence After Radical Prostatectomy and Risk of Prostate Cancer Specific Mortality. J. Urol. 2006, 176, 1404–1408. [Google Scholar] [CrossRef] [PubMed]
- Sugano, D.; Sidana, A.; Jain, A.L.; Calio, B.; Gaur, S.; Maruf, M.; Merino, M.; Choyke, P.; Turkbey, B.; Wood, B.J.; et al. Index tumor volume on MRI as a predictor of clinical and pathologic outcomes following radical prostatectomy. Int. Urol. Nephrol. 2019, 51, 1349–1355. [Google Scholar] [CrossRef] [PubMed]
- Capogrosso, P.; Vertosick, E.A.; Benfante, N.E.; Sjoberg, D.D.; Vickers, A.J.; Eastham, J.A. Can We Improve the Preoperative Prediction of Prostate Cancer Recurrence With Multiparametric MRI? Clin. Genitourin. Cancer 2019, 17, e745–e750. [Google Scholar] [CrossRef] [PubMed]
- Reisæter, L.A.R.; Fütterer, J.J.; Losnegård, A.; Nygård, Y.; Monssen, J.; Gravdal, K.; Halvorsen, O.J.; Akslen, L.A.; Biermann, M.; Haukaas, S.; et al. Optimising preoperative risk stratification tools for prostate cancer using mpMRI. Eur. Radiol. 2018, 28, 1016–1026. [Google Scholar] [CrossRef]
- Takeuchi, N.; Sakamoto, S.; Nishiyama, A.; Horikoshi, T.; Yamada, Y.; Iizuka, J.; Maimaiti, M.; Imamura, Y.; Kawamura, K.; Imamoto, T.; et al. Biparametric Prostate Imaging Reporting and Data System version2 and International Society of Urological Pathology Grade Predict Biochemical Recurrence after Radical Prostatectomy. Clin. Genitourin. Cancer 2018, 16, e817–e829. [Google Scholar] [CrossRef]
- Faiena, I.; Salmasi, A.; Mendhiratta, N.; Markovic, D.; Ahuja, P.; Hsu, W.; Elashoff, D.A.; Raman, S.S.; Reiter, R.E. PI-RADS Version 2 Category on 3 Tesla Multiparametric Prostate Magnetic Resonance Imaging Predicts Oncologic Outcomes in Gleason 3 + 4 Prostate Cancer on Biopsy. J. Urol. 2019, 201, 91–97. [Google Scholar] [CrossRef]
- Freedland, S.J.; Humphreys, E.B.; Mangold, L.A.; Eisenberger, M.; Dorey, F.J.; Walsh, P.C.; Partin, A.W. Risk of Prostate Cancer–Specific Mortality Following Biochemical Recurrence After Radical Prostatectomy. JAMA 2005, 294, 433–439. [Google Scholar] [CrossRef]
- Gandaglia, G.; Ploussard, G.; Valerio, M.; Mattei, A.; Fiori, C.; Roumiguié, M.; Fossati, N.; Stabile, A.; Beauval, J.-B.; Malavaud, B.; et al. The Key Combined Value of Multiparametric Magnetic Resonance Imaging, and Magnetic Resonance Imaging–targeted and Concomitant Systematic Biopsies for the Prediction of Adverse Pathological Features in Prostate Cancer Patients Undergoing Radical Prostatectomy. Eur. Urol. 2020, 77, 733–741. [Google Scholar] [CrossRef]
- Cornud, F.; Roumiguié, M.; Barry de Longchamps, N.; Ploussard, G.; Bruguière, E.; Portalez, D.; Malavaud, B. Precision Matters in MR Imaging–targeted Prostate Biopsies: Evidence from a Prospective Study of Cognitive and Elastic Fusion Registration Transrectal Biopsies. Radiology 2018, 287, 534–542. [Google Scholar] [CrossRef]
- Covin, B.; Roumiguié, M.; Quintyn-Ranty, M.-L.; Graff, P.; Khalifa, J.; Aziza, R.; Ploussard, G.; Portalez, D.; Malavaud, B. Refining the risk-stratification of transrectal biopsy-detected prostate cancer by elastic fusion registration transperineal biopsies. World J. Urol. 2019, 37, 269–275. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall | |
|---|---|
| n = 521 | |
| Age (years): | |
| Mean | 64.86 |
| Median (Range) | 65.70 (46.80–77.90) |
| PSA (ng/mL): | |
| Mean | 10.26 |
| Median (Range) | 8 (0.65–69) |
| PSAD: | |
| Mean | 0.24 |
| Median (Range) | 0.18 (0.03–1.28) |
| Clinical stage: | |
| T1 | 342 (65.6%) |
| T2 | 168 (32.2%) |
| T3 | 11 (2.1%) |
| PI-RADS | |
| 3 | 103 (19.8%) |
| 4 | 260 (49.9%) |
| 5 | 158 (30.3%) |
| No of MRI lesions | |
| 1 | 373 (71.6%) |
| 2 | 121 (23.2%) |
| ≥3 | 27 (5.2%) |
| MRI Maximal lesion diameter (mm): | |
| <10 | 211 (40.5%) |
| 10–15 | 130 (25%) |
| >15 | 91 (17.5%) |
| Missing | 89 (17.0%) |
| MRI stage: | |
| No ECE on MRI | 436 (83.7%) |
| ECE on MRI | 83 (15.9%) |
| Missing | 2 (0.4%) |
| ISUP grade group TB | |
| Negative biopsies | 57 (11.0%) |
| 1 | 60 (11.5%) |
| 2 | 235 (45.1%) |
| 3 | 108 (20.7%) |
| 4–5 | 61 (11.7%) |
| ISUP grade group TB | |
| Negative biopsies | 82 (15.7%) |
| 1 | 134 (25.7%) |
| 2 | 203 (39.0%) |
| 3 | 64 (12.3%) |
| 4–5 | 38 (7.3%) |
| Pathological stage pT: | |
| pT2 | 245 (47.0%) |
| pT3a | 185 (35.5%) |
| pT3b | 91 (17.5%) |
| Regional lymph nodes pN | |
| pNx | 68 (13.1%) |
| pN0 | 403 (77.4%) |
| pN1 | 50 (9.6%) |
| ISUP grade group RP: | |
| 1 | 16 (3.1%) |
| 2 | 269 (51.6%) |
| 3 | 189 (36.3%) |
| 4–5 | 47 (9.0%) |
| Margin: | |
| Negative | 406 (77.9%) |
| Positive | 115 (22.1%) |
| Biochemical recurrence: | |
| YES | 49 (9.4%) |
| NO | 465 (89.3%) |
| Missing | 7 (1.3%) |
| Overall | pT Stage in RP | pN1 | ISUP Grade Group in RP | Margin R1 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| pT2 245 (47.0%) | pT3a 185 (35.5%) | pT3b–pT4 91 (17.5%) | 50 (9.6%) | 1 16 (3.1%) | 2 269 (51.6%) | 3 189 (36.3%) | 4–5 47 (9.0%) | 115 (22.1%) | ||||||
| PIRADS | p = 0.013 | p < 0.001 | p = 0.001 | p = 0.053 | ||||||||||
| 3 | (n = 103) | 53 (51.5%) | 35 (34.0%) | 15 (14.6%) | 2 (1.9%) | 5 (4.9%) | 57 (55.3%) | 34 (33.0%) | 7 (6.8%) | 28 (27.2%) | ||||
| 4 | (n = 260) | 135 (51.9%) | 87 (33.5%) | 38 (14.6%) | 22 (8.5%) | 6 (2.3%) | 155 (59.6%) | 78 (30.0%) | 21 (8.0%) | 46 (17.7%) | ||||
| 5 | (n = 158) | 57 (36.1%) | 63 (39.9%) | 38 (24.1%) | 26 (16.5%) | 5 (3.2%) | 57 (36.1%) | 77 (48.7%) | 19 (12.0%) | 41 (25.9%) | ||||
| ECE on MRI | p < 0.001 | p < 0.001 | p <0.001 | p < 0.001 | ||||||||||
| No | (n = 436) | 232 (53.2%) | 152 (34.9%) | 52 (11.9%) | 25 (5.7%) | 16 (3.7%) | 243 (55.7%) | 149 (34.2%) | 28 (6.4%) | 85 (19.5%) | ||||
| Yes | (n = 83) | 11 (13.2%) | 33 (39.8%) | 39 (47.0%) | 25 (30.1%) | 0 (0.0%) | 25 (30.1%) | 39 (47.0%) | 19 (22.9%) | 30 (36.1%) | ||||
| No of MRI lesions | p < 0.001 | p = 0.269 | p = 0.216 | p = 0.262 | ||||||||||
| 1 | (n = 373) | 174 (46.6%) | 132 (35.4%) | 67 (18.0%) | 34 (9.1%) | 11 (2.9%) | 191 (51.2%) | 138 (37.0%) | 33 (8.9%) | 87 (23.3%) | ||||
| 2 | (n = 121) | 60 (49.6%) | 41 (33.9%) | 20 (16.5%) | 14 (11.6%) | 4 (3.3%) | 59 (48.8%) | 44 (36.4%) | 14 (11.6%) | 25 (20.7%) | ||||
| ≥3 | (n = 27) | 11 (47.0%) | 12 (44.4%) | 4 (14.8%) | 2 (7.4%) | 1 (3.7%) | 19 (70.4%) | 7 (25.9%) | 0 (0.0%) | 3 (11.1%) | ||||
| MRI Maximal lesion diameter (mm): | p = 0.003 | p = 0.070 | p = 0.045 | p = 0.125 | ||||||||||
| <10 | (n = 211) | 109 (51.7%) | 72 (34.1%) | 30 (14.2%) | 14 (6.6%) | 5 (2.4%) | 120 (56.9%) | 65 (30.8%) | 21 (10.0%) | 46 (21.8%) | ||||
| 10–15 | (n = 130) | 60 (46.2%) | 44 (33.8%) | 26 (20.0%) | 16 (12.3%) | 4 (3.1%) | 59 (45.4%) | 56 (43.1%) | 11 (8.5%) | 25 (19.2%) | ||||
| >15 | (n = 91) | 28 (45.6%) | 35 (38.5%) | 28 (30.8%) | 16 (17.6%) | 2 (2.2%) | 35 (38.5%) | 40 (44.0%) | 14 (15.4%) | 28 (30.8%) | ||||
| ISUP grade group in TB | p < 0.001 | p < 0.001 | p < 0.001 | p = 0.001 | ||||||||||
| 1 | (n = 60) | 33 (55.0%) | 19 (31.7%) | 8 (13.3%) | 1 (1.7%) | 3 (33%) | 44 (73.3%) | 2 (3.3%) | 3 (5.0%) | 12 (20%) | ||||
| 2 | (n = 235) | 123 (35.2%) | 82 (34.9%) | 30 (12.8%) | 12 (5.1%) | 4 (1.7%) | 152 (64.7%) | 72 (30.6%) | 7 (3.0%) | 42 (17.9%) | ||||
| 3 | (n = 108) | 38 (35.2%) | 41 (38.0%) | 29 (26.9%) | 19 (17.6%) | 2 (1.9%) | 29 (26.9%) | 69 (63.9%) | 8 (7.5%) | 27 (25%) | ||||
| 4–5 | (n = 61) | 14 (23.0%) | 24 (39.3%) | 23 (37.7%) | 15 (24.6%) | 0 (0.0%) | 6 (9.8%) | 29 (47.5%) | 26 (42.6%) | 26 (42.6%) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manceau, C.; Beauval, J.-B.; Lesourd, M.; Almeras, C.; Aziza, R.; Gautier, J.-R.; Loison, G.; Salin, A.; Tollon, C.; Soulié, M.; et al. MRI Characteristics Accurately Predict Biochemical Recurrence after Radical Prostatectomy. J. Clin. Med. 2020, 9, 3841. https://doi.org/10.3390/jcm9123841
Manceau C, Beauval J-B, Lesourd M, Almeras C, Aziza R, Gautier J-R, Loison G, Salin A, Tollon C, Soulié M, et al. MRI Characteristics Accurately Predict Biochemical Recurrence after Radical Prostatectomy. Journal of Clinical Medicine. 2020; 9(12):3841. https://doi.org/10.3390/jcm9123841
Chicago/Turabian StyleManceau, Cécile, Jean-Baptiste Beauval, Marine Lesourd, Christophe Almeras, Richard Aziza, Jean-Romain Gautier, Guillaume Loison, Ambroise Salin, Christophe Tollon, Michel Soulié, and et al. 2020. "MRI Characteristics Accurately Predict Biochemical Recurrence after Radical Prostatectomy" Journal of Clinical Medicine 9, no. 12: 3841. https://doi.org/10.3390/jcm9123841
APA StyleManceau, C., Beauval, J.-B., Lesourd, M., Almeras, C., Aziza, R., Gautier, J.-R., Loison, G., Salin, A., Tollon, C., Soulié, M., Malavaud, B., Roumiguié, M., & Ploussard, G. (2020). MRI Characteristics Accurately Predict Biochemical Recurrence after Radical Prostatectomy. Journal of Clinical Medicine, 9(12), 3841. https://doi.org/10.3390/jcm9123841