Characterization of Preoperative, Postsurgical, Acute and Chronic Pain in High Risk Breast Cancer Patients

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Patients and Methods
2.1. Settings
2.2. Participants
2.3. Intervention
2.4. Data Collection
2.5. Data Processing and Analyses
2.5.1. Quantitative Analyses
2.5.2. Thematical/Framework Type Analyses
- (1)
- Identify information about the type of pain, the site and cause, and how it has changed over time.
- (2)
- Organise the codes according to the similar meaning identified in a second and third round until the saturation is considered reached. The codes were grouped into categories, without any interpretation concerning a possible aetiology: “permanent pain”, “musculoskeletal pain”, “pain located in surgical area”, “other located pain”, “polyneuropathy”, and “no pain”. “Permanent pain” refers to “pain all the time”; “musculoskeletal pain” refers to any pain originating from or resembling arthralgia, myalgia, or low back pain; “pain located in surgical area” refers to the patient’s interpretation, primarily related to the pain localisation; “polyneuropathy” refers to pain in the extremities associated with positive and/or negative symptoms (like paraesthesia and numbness).
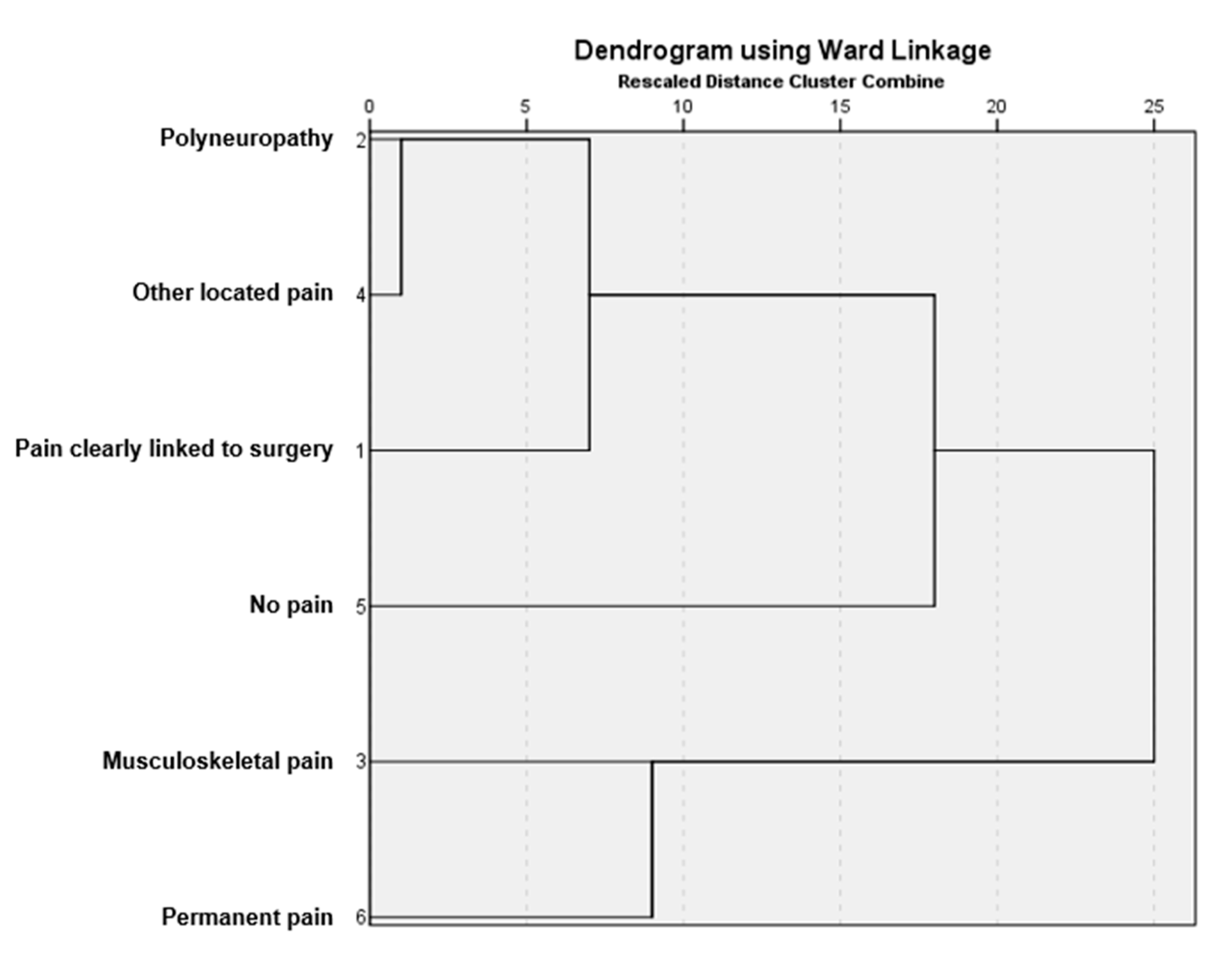
- (3)
- Classify and group codes in clusters: patients with different types of pain (e.g., with both polyneuropathy and musculoskeletal pain) were counted in different categories. In contrast, patients experiencing more than one type of pain within a category were counted once in that category (e.g., musculoskeletal pain for patients reporting arthralgia and low back pain). Hierarchical clustering was used to group the different categories, according to the frequency of their co-occurrence in the individual patient data. Hierarchical clustering has already been described as useful in pain studies to identify profiles, multiple associations of descriptors, and combine symptoms into subgroups [7]. The final analysis was expressed by a network plot using Ward coupling, i.e., showing the clusters with the smallest variance (the most similar) and a dendrogram (Appendix A).
3. Results
3.1. Patient Characteristics and Quantitative Analyses
3.2. Pain Characteristics
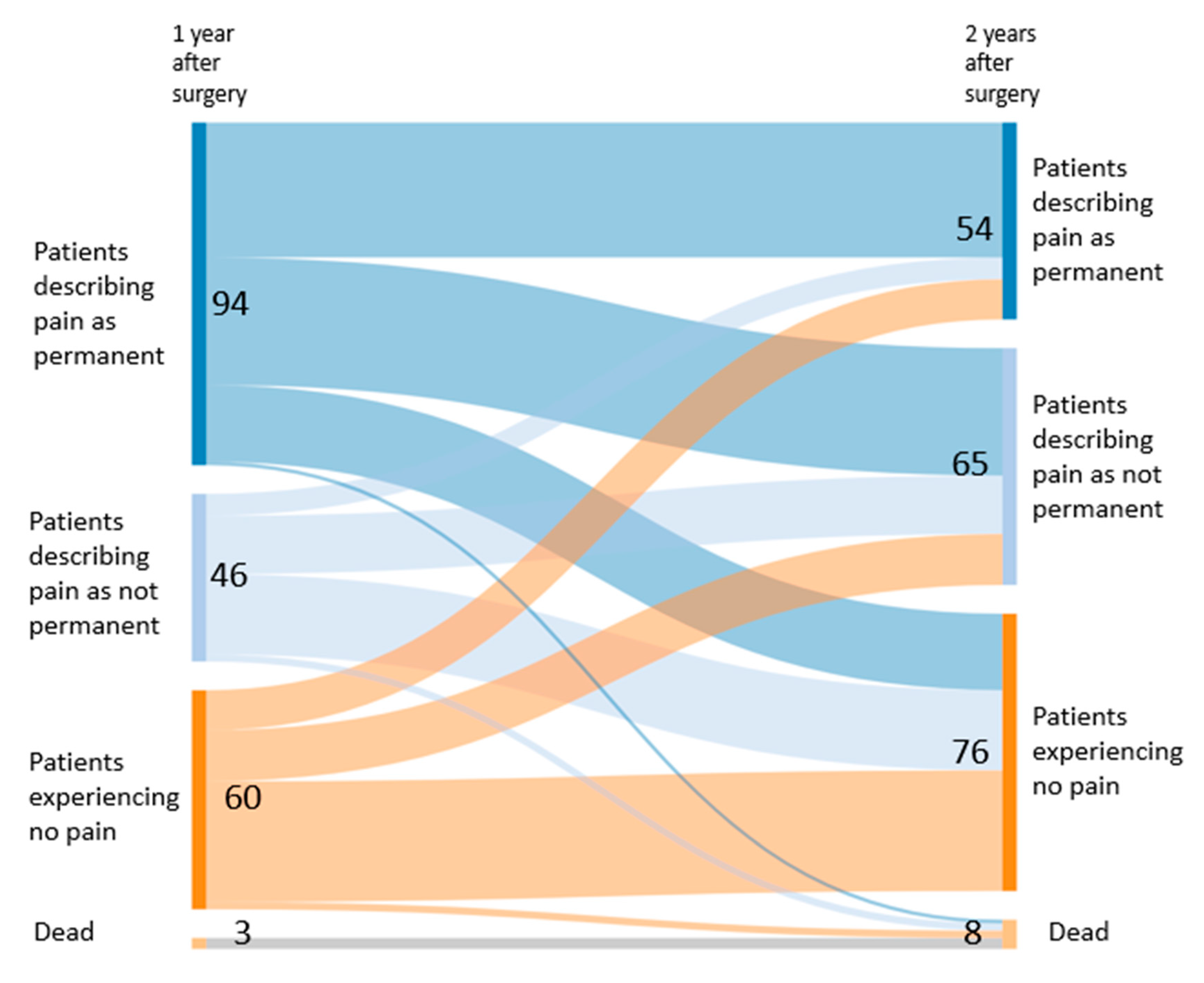
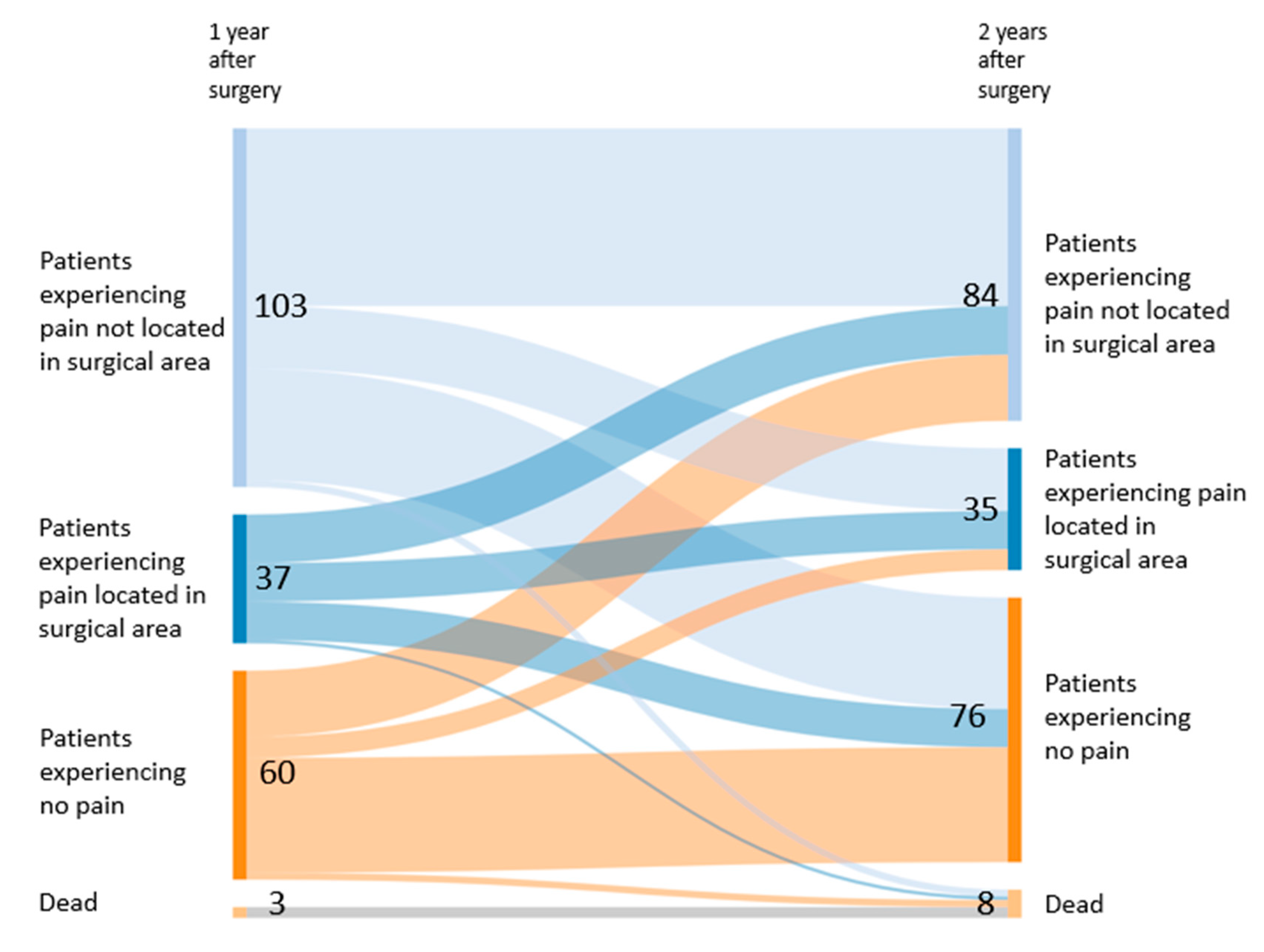
3.3. Similarities and Differences in Patients with Pain after One and Two Years
4. Discussion
4.1. Summary of the Results
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- Wang, L.; Guyatt, G.H.; Kennedy, S.A.; Romerosa, B.; Kwon, H.Y.; Kaushal, A.; Chang, Y.; Craigie, S.; De Almeida, C.P.; Couban, R.J.; et al. Predictors of persistent pain after breast cancer surgery: A systematic review and meta-analysis of observational studies. Can. Med Assoc. J. 2016, 188, E352–E361. [Google Scholar] [CrossRef] [PubMed]
- Bruce, J.; Williamson, E.; Lait, C.; Richmond, H.; Betteley, L.; Lall, R.; Petrou, S.; Rees, S.; Withers, E.J.; Lamb, S.E.; et al. Randomised controlled trial of exercise to prevent shoulder problems in women undergoing breast cancer treatment: Study protocol for the prevention of shoulder problems trial (UK PROSPER). BMJ Open 2018, 8, e019078. [Google Scholar] [CrossRef] [PubMed]
- Forget, P.; Bouche, G.; Duhoux, F.P.; Coulie, P.G.; Decloedt, J.; Dekleermaker, A.; Guillaume, J.E.; Ledent, M.; Machiels, J.P.; Mustin, V.; et al. In-traoperative ketorolac in high-risk breast cancer patients. A prospective, randomized, placebo-controlled clini-cal trial. PLoS ONE 2019, 14, e0225748. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D. For the CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (RED-Cap)—A metadata-driven methodology and workflow process for providing translational research informat-ics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Pinedo-Villanueva, R.; Khalid, S.; Wylde, V.; Gooberman-Hill, R.; Soni, A.; Judge, A. Identifying individuals with chronic pain after knee replacement: A population-cohort, cluster-analysis of Oxford knee scores in 128,145 patients from the English National Health Service. BMC Musculoskelet. Disord. 2018, 19, 354. [Google Scholar] [CrossRef] [PubMed]
- American Society of Anesthesiologists Task Force on Acute Pain Management. Practice guidelines for acute pain management in the perioperative setting: An updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology 2012, 116, 248–273. [Google Scholar] [CrossRef] [PubMed]
- Gärtner, R.; Jensen, M.-B.; Nielsen, J.; Ewertz, M.; Kroman, N.; Kehlet, H. Prevalence of and Factors Associated With Persistent Pain Following Breast Cancer Surgery. JAMA 2009, 302, 1985–1992. [Google Scholar] [CrossRef] [PubMed]
- Saporito, A.; Aguirre, J.; Borgeat, A.; Perren, A.; Anselmi, L.; Poggi, R.; Minotti, B.; Cafarotti, S.; La Regina, D.; Ceruti, S. Persistent postdischarge pain and chronic postoperative pain after breast cancer surgery under general anesthesia and single-shot paravertebral block: Incidence, characteristics and impact on quality of life and healthcare costs. J. Pain Res. 2019, 12, 1193–1199. [Google Scholar] [CrossRef] [PubMed]
- Hamood, R.; Hamood, H.; Merhasin, I.; Keinan-Boker, L. Chronic pain and other symptoms among breast cancer survivors: Prevalence, predictors, and effects on quality of life. Breast Cancer Res. Treat. 2017, 167, 157–169. [Google Scholar] [CrossRef] [PubMed]
- Meretoja, T.J.; Andersen, K.G.; Bruce, J.; Haasio, L.; Sipilä, R.; Scott, N.W.; Ripatti, S.; Kehlet, H.; Kalso, M.E.A. Clinical Prediction Model and Tool for Assessing Risk of Persistent Pain After Breast Cancer Surgery. J. Clin. Oncol. 2017, 35, 1660–1667. [Google Scholar] [CrossRef] [PubMed]
- Andersen, K.G.; Duriaud, H.M.; Jensen, H.E.; Kroman, N.; Kehlet, H. Predictive factors for the development of persistent pain after breast cancer surgery. Pain 2015, 156, 2413–2422. [Google Scholar] [CrossRef] [PubMed]
- Niravath, P. Aromatase inhibitor-induced arthralgia: A review. Ann. Oncol. 2013, 24, 1443–1449. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Entire Series n = 203 | Ketorolac n = 96 | Placebo n = 107 |
|---|---|---|---|
| Age, years | |||
| Mean (SD) | 55.7 (14.0) | 56.1 (14.0) | 55.4 (13.9) |
| Range | 28–85 | 30–85 | 28–85 |
| Gender, n (%) | |||
| Female | 202 (99%) | 95 (99%) | 107 (100%) |
| Male | 1 (1%) | 1 (1%) | 0 |
| Chemotherapy, n (%) | |||
| Yes | 161 (79%) | 80 (83%) | 81 (76%) |
| No | 42 (21%) | 16 (17%) | 26 (24%) |
| If chemotherapy (anthracyclines with/without taxanes), type (%) | |||
| Adjuvant | 54 (27%) | 27 (28%) | 27 (25%) |
| Neoadjuvant | 107 (53%) | 53 (55%) | 54 (51%) |
| Type of surgery, n (%) | |||
| Mastectomy | 119 (59%) | 60 (63%) | 59 (55%) |
| Breast-conserving surgery | 82 (40%) | 34 (35%) | 48 (45%) |
| Missing | 2 (1%) | 2 (2%) | 0 |
| Type of lymphadenectomy, n (%) | |||
| None | 14 (7%) | 6 (6%) | 8 (8%) |
| Sentinel | 12 (6%) | 5 (5%) | 7 (6%) |
| Complete axillary | 176 (87%) | 85 (89%) | 91 (85%) |
| Missing | 1 (1%) | 0 | 1 (1%) |
| Post-operative radiotherapy, n (%) | |||
| Yes | 165 (81%) | 77 (80%) | 88 (82%) |
| No | 38 (19%) | 19 (20%) | 19 (18%) |
| Endocrine therapy, n (%) | |||
| Yes | 138 (68%) | 69 (72%) | 69 (64%) |
| No | 64 (31%) | 27 (28%) | 37 (35%) |
| Missing | 1 (1%) | 0 | 1 (1%) |
| Characteristics | Ketorolac (n = 96) | Placebo (n = 107) | p-Value | ||
|---|---|---|---|---|---|
| Preoperative chronic pain | |||||
| 13 | (14%) | 24 | (23%) | 0.356 | |
| Preoperative pain (any type, including post-biopsy) | |||||
| Every day | 59 | (62%) | 62 | (58%) | 0.583 |
| One to 3 days a week | 0 | (0%) | 1 | (1%) | |
| Less than once a week | 27 | (28%) | 36 | (34%) | |
| Missing | 10 | (10%) | 8 | (8%) | |
| Acute pain | |||||
| Pain at rest at D1 after surgery Verbal simple scale (0–4), N (%) | 0.620 | ||||
| 0 | 18 | (19%) | 17 | (16%) | |
| 1 | 35 | (37%) | 31 | (29%) | |
| 2 | 37 | (38%) | 47 | (44%) | |
| 3 | 5 | (5%) | 10 | (9%) | |
| 4 | 1 | (1%) | 1 | (1%) | |
| Missing | 0 | (0%) | 1 | (1%) | |
| Morphine equivalent at D1 (in mg) Median (interquartile range 25–75) | 5 | (0–10) | 8 | (4–14) | 0.001 |
| Mean change in pain score to Day 1 (SD) | −0.6 | (1.16) | −0.7 | (1.24) | 0.357 |
| Mean change in pain score to Day 2 (SD) | −0.1 | (1.42) | 0.1 | (1.42) | 0.631 |
| Mean change in pain score to Day 3 (SD) | 0.7 | (1.24) | 0.8 | (1.27) | 0.869 |
| Persistent pain 1 year after surgery | |||||
| Presence of any type of pain | 72 | (75%) | 70 | (65%) | 0.137 |
| Average pain score Mean Visual Analogue Scale (0–10) (SD) | 2.6 | (1.4) | 2.9 | (1.4) | 0.166 |
| Persistent pain 2 years after surgery | |||||
| Presence of any type of pain | 57 | (63%) | 62 | (59%) | 0.541 |
| Average pain score Mean Visual Analogue Scale (0–10) (SD) | 2.4 | (1.5) | 2.3 | (1.7) | 0.805 |
| Localisation of Pain after 1 Year | n | Experiencing Permanent Pain (%) |
| Pain in surgical area | 37 | 21 (58) |
| Polyneuropathy | 23 | 22 (96) |
| Musculoskeletal | 56 | 37 (66) |
| Other | 28 | 17 (61) |
| None | 61 | 0 |
| Total: 200 patients (with and without pain), 205 reported pain types | ||
| Localisation of Pain after 2 Year | n | Experiencing Permanent Pain (%) |
| Pain in surgical area | 35 | 18 (51) |
| Polyneuropathy | 20 | 10 (50) |
| Musculoskeletal | 66 | 31 (47) |
| Other | 60 | 27 (45) |
| None | 77 | 0 |
| Total: 195 patients (with and without pain), 258 reported pain types | ||
| Patients’ Characteristics | 1 Year after Surgery | 2 Years after Surgery | ||||
|---|---|---|---|---|---|---|
| Pain n = 140 | Pain Free n = 60 | p | Pain n = 119 | Pain Free n = 76 | p | |
| Gender n (%) | ||||||
| Female | 139 (99) | 60 (100) | - | 118 (99) | 76 (100) | - |
| Male | 1 (1) | 0 | - | 1 (1) | 0 | - |
| Age (Mean; SD; CI) | 59.7 (26.5; 55.2–65.1) | 52.8 (13.3; 49.3–56.2) | 0.02 | 56.0 (13.8; 53.3–63.6) | 58.5 (13.8; 52.8–59.1) | 0.87 |
| BMI (Mean; SD; 95%CI) | 26.0 (5.0; 25.1–26.8) | 24.4 (4.4; 23.2–25.5) | 0.03 | 25.8 (5.3; 24.8–26.8) | 24.8 (4.1; 23.8–25.7) | 0.14 |
| Preoperative Pain (Yes/No) | 28/108 | 6/52 | 0.13 | 23/91 | 10/65 | 0.31 |
| Surgery n (%) | 0.53 | 0.50 | ||||
| Mastectomy | 84 (60) | 32 (53) | 67 (56) | 46 (61) | ||
| Quadrantectomy/Lumpectomy | 55 (39) | 27 (45) | 52 (44) | 28 (37) | ||
| Bilateral | 13 (9) | 8 (13) | 11 (9) | 10 (13) | ||
| Axillary lymph node resection n (%) | 0.42 | 0.69 | ||||
| Complete axillary lymph nodes resection | 119(85) | 54 (90) | 104(87) | 64 (84) | ||
| Sentinel lymph node | 8 (6) | 4 (7) | 6 (5) | 6 (8) | ||
| None | 12 (9) | 2 (3) | 8 (7) | 6 (8) | ||
| Hormonotherapy | 96 (69) | 43 (72) | 0.66 | 47 (41) | 37 (49) | 0.30 |
| Sensation of phantom breast (%) | 1 (1) | 0 | - | 0 | 0 | - |
| Association with pain (Yes/No) | 0/1 | 0/0 | - | 0/0 | 0/0 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forget, P.; Sitter, T.M.; Hollick, R.J.; Dixon, D.; van Maanen, A.; Dekleermaker, A.; Duhoux, F.P.; De Kock, M.; Berliere, M.; on behalf of the KBCt Group. Characterization of Preoperative, Postsurgical, Acute and Chronic Pain in High Risk Breast Cancer Patients. J. Clin. Med. 2020, 9, 3831. https://doi.org/10.3390/jcm9123831
Forget P, Sitter TM, Hollick RJ, Dixon D, van Maanen A, Dekleermaker A, Duhoux FP, De Kock M, Berliere M, on behalf of the KBCt Group. Characterization of Preoperative, Postsurgical, Acute and Chronic Pain in High Risk Breast Cancer Patients. Journal of Clinical Medicine. 2020; 9(12):3831. https://doi.org/10.3390/jcm9123831
Chicago/Turabian StyleForget, Patrice, Taalke M. Sitter, Rosemary J. Hollick, Diane Dixon, Aline van Maanen, Alain Dekleermaker, Francois P. Duhoux, Marc De Kock, Martine Berliere, and on behalf of the KBCt Group. 2020. "Characterization of Preoperative, Postsurgical, Acute and Chronic Pain in High Risk Breast Cancer Patients" Journal of Clinical Medicine 9, no. 12: 3831. https://doi.org/10.3390/jcm9123831
APA StyleForget, P., Sitter, T. M., Hollick, R. J., Dixon, D., van Maanen, A., Dekleermaker, A., Duhoux, F. P., De Kock, M., Berliere, M., & on behalf of the KBCt Group. (2020). Characterization of Preoperative, Postsurgical, Acute and Chronic Pain in High Risk Breast Cancer Patients. Journal of Clinical Medicine, 9(12), 3831. https://doi.org/10.3390/jcm9123831