Excessive Gestational Weight Gain: Long-Term Consequences for the Child

 ,
,  , ,
, ,  ,
,  , and
, and 
Abstract
1. Introduction
2. Experimental Section
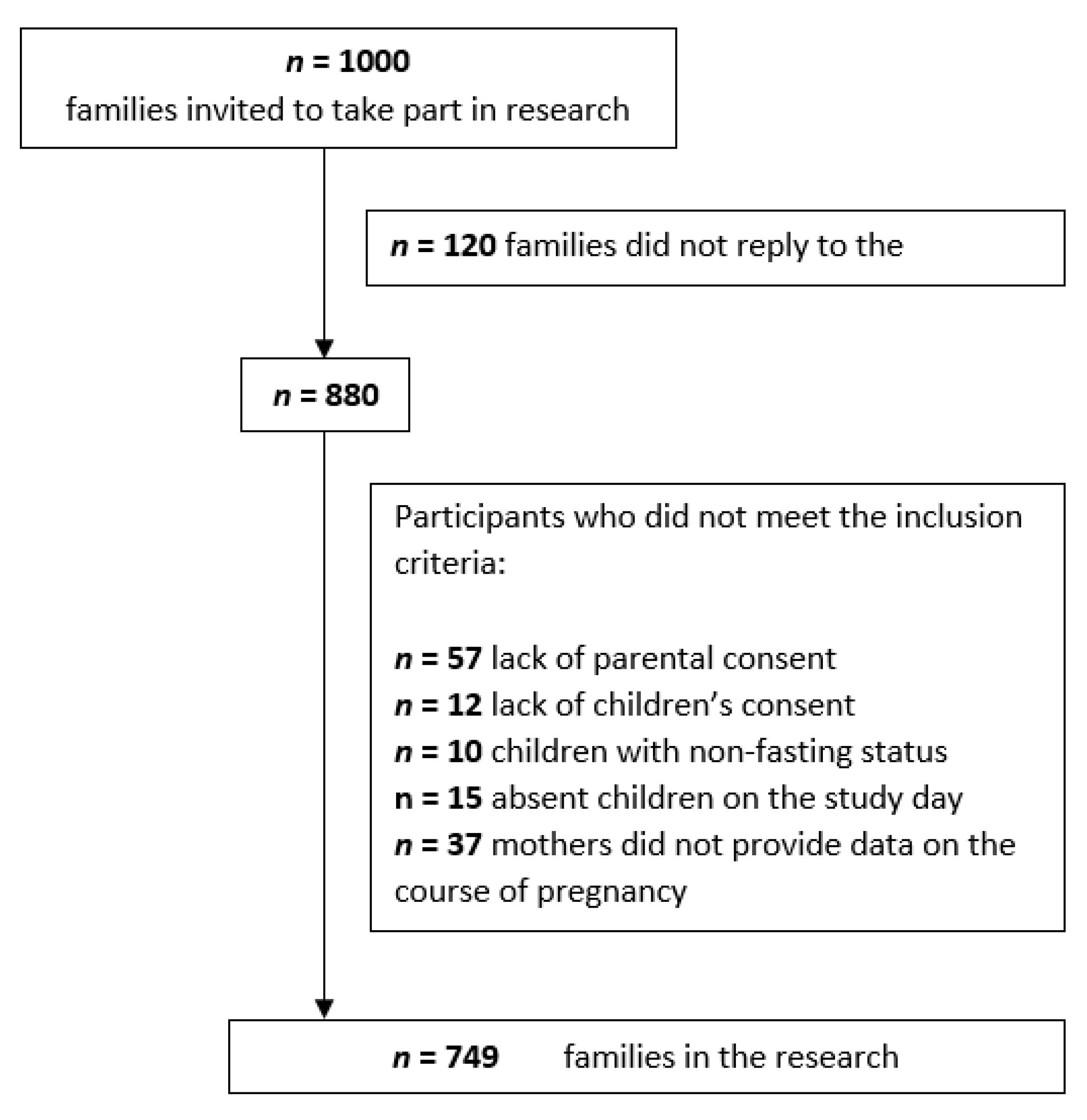
2.1. Participants
2.2. Physical Examination
2.3. Maternal Factors
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Facts and Figures on Childhood Obesity. Available online: www.who.int/end-childhood-obesity/facts/en/ (accessed on 23 August 2020).
- Kumaran, A.; Sakka, S.; Dias, R.P. Obesity in children: Recent NICE guidance. Arch. Dis. Child. Educ. Pract. Ed. 2017, 102, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Simmonds, M.; Llewellyn, A.; Owen, C.G.; Woolacott, N. Predicting adult obesity from childhood obesity: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Mazur, A.; Klimek, K.; Małecka-Tendera, E. Risk factors of obesity in school children from Podkarpatian Region. Endocr. Obes. Met. Dis. 2011, 7, 157–166. [Google Scholar]
- Eriksson, J.; Forsén, T.; Tuomilehto, J.; Osmond, C.; Barker, D. Size at birth, childhood growth and obesity in adult life. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Herman, A.N.; Malhotra, K.; Wright, G.; Fisher, J.; Whitaker, R.C. A qualitative study of the aspirations and challenges of low-income mothers in feeding their preschool-aged children. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 132. [Google Scholar] [CrossRef]
- Carnell, S.; Cooke, L.; Cheng, R.; Robbins, A.; Wardle, J. Parental feeding behaviours and motivations. A qualitative study in mothers of UK pre-schoolers. Appetite 2011, 57, 665–673. [Google Scholar] [CrossRef]
- Mourtakos, S.P.; Tambalis, K.D.; Panagiotakos, D.B.; Antonogeorgos, G.; Arnaoutis, G.; Karteroliotis, K.; Sidossis, L.S. Maternal lifestyle characteristics during pregnancy, and the risk of obesity in the offspring: A study of 5125 children. BMC Pregnancy Childbirth 2015, 15, 66. [Google Scholar] [CrossRef]
- Li, L.; Peters, H.; Gama, A.; Carvalhal, M.I.M.; Nogueira, H.G.M.; Rosadomarques, V.; Padez, C. Maternal smoking in pregnancy association with childhood adiposity and blood pressure. Pediatr. Obes. 2015, 11, 202–209. [Google Scholar] [CrossRef]
- Suzuki, K.; Sato, M.; Ando, D.A.; Kondo, N.; Yamagata, Z. Differences in the effect of maternal smoking during pregnancy for childhood overweight before and after 5 years of age. J. Obstet. Gynaecol. Res. 2013, 39, 914–921. [Google Scholar] [CrossRef]
- Gorog, K.; Pattenden, S.; Antova, T.; Niciu, E.; Rudnai, P.; Scholtens, S.; Splichalova, A.; Slotova, K.; Vokó, Z.; Zlotkowska, R.; et al. Maternal Smoking During Pregnancy and Childhood Obesity: Results from the CESAR Study. Matern. Child Health J. 2011, 15, 985–992. [Google Scholar] [CrossRef]
- Guo, L.; Liu, J.; Ye, R.; Liu, J.; Zhuang, Z.; Ren, A. Gestational Weight Gain and Overweight in Children Aged 3–6 Years. J. Epidemiol. 2015, 25, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Tennant, G. Preventing Childhood Obesity by Managing Pregnancy Weight Gain. Int. J. Childbirth Educ. 2014, 29, 41–45. [Google Scholar]
- American College of Obstetricians and Gynecologists. ACOG Committee opinion no. 548: Weight gain during pregnancy. Obstet Gynecol. 2013, 121, 210–212. [Google Scholar] [CrossRef] [PubMed]
- Nehring, I.; Lehmann, S.; von Kries, R. Gestational weight gain in accordance to the IOM/NRC criteria and the risk for childhood overweight: A meta-analysis. Pediatr. Obes. 2012, 8, 218–224. [Google Scholar] [CrossRef]
- Siega-Riz, A.M.; Viswanathan, M.; Moos, M.K.; Deierlein, A.; Mumford, S.; Knaack, J.; Thieda, P.; Lux, L.J.; Lohr, K.N. A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: Birthweight, fetal growth, and postpartum weight retention. Am. J. Obstet. Gynecol. 2009, 201, 339.e1–339.e14. [Google Scholar] [CrossRef]
- Cardwell, C.R.; Stene, L.C.; Joner, G.; Bulsara, M.K.; Cinek, O.; Rosenbauer, J.; Ludvigsson, J.; Jané, M.; Svensson, J.; Goldacre, M.J.; et al. Maternal age at birth and childhood type 1 DIABETES: A Pooled analysis of 30 observational studies. Diabetes 2010, 59, 486–494. [Google Scholar] [CrossRef]
- Bingley, P.J.; Douek, I.F.; Rogers, C.A.; Gale, E.A.; Bart’s-Oxford Family Study Group. Influence of maternal age at delivery and birth order on risk of type 1 diabetes in childhood: Prospective population based family study. BMJ 2000, 321, 420–424. [Google Scholar] [CrossRef]
- Li, S.; Hua, J.; Hong, H.; Wang, Y.; Zhang, J. Interpregnancy interval, maternal age, and offspring’s BMI and blood pressure at 7 years of age. J. Hum. Hypertens. 2018, 32, 349–358. [Google Scholar] [CrossRef]
- Rocca, W.A.; Van Duijn, C.M.; Clayton, D.; Chandra, V.; Fratiglioni, L.; Graves, A.B.; Heyman, A.; Jorm, A.F.; Kokmen, E.; Kondo, K.; et al. Maternal age and Alzheimer’s disease: A collaborative re-analysis of case-control studies. Int. J. Epidemiol. 1991, 20 (Suppl. 2), S21–S27. [Google Scholar] [CrossRef]
- Johnson, K.J.; Carozza, S.E.; Chow, E.J.; Fox, E.E.; Horel, S.; McLaughlin, C.C.; Mueller, B.A.; Puumala, S.E.; Reynolds, P.; Von Behren, J.; et al. Parental age and risk of childhood cancer: A pooled analysis. Epidemiology 2009, 20, 475–483. [Google Scholar] [CrossRef]
- Saloojee, H.; Coovadia, H. Maternal age matters: For a lifetime, or longer. Lancet Glob. Health 2015, 3, e342–e343. [Google Scholar] [CrossRef][Green Version]
- Myrskylä, M.; Fenelon, A. Maternal Age and Offspring Adult Health: Evidence from the Health and Retirement Study. Demography 2012, 9, 1231–1257. [Google Scholar] [CrossRef] [PubMed]
- Województwo podkarpackie w liczbach (mapy, miasta, nieruchomości, GUS, noclegi, regon, wypadki drogowe, bezrobocie, zarobki, wynagrodzenie). Available online: http://www.polskawliczbach.pl/podkarpackie#biologiczne-grupy-wieku (accessed on 1 September 2020).
- Kułaga, Z.; Grajda, A.; Gurzkowska, B.; Wojtyło, M.; Góźdź, M.; Litwin, M. The prevalence of overweight and obesity among Polish school- aged children and adolescents. Przeglad Epidemiologiczny 2016, 70, 641–651. [Google Scholar] [PubMed]
- Dżygadło, B.; Łepecka-Klusek, C.; Pilewski, B. Wykorzystanie analizy impedancji bioelektrycznej w profilaktyce i leczeniu nadwagi i otyłości. Probl. Hig. Epidemiol. 2012, 93, 274–280. [Google Scholar]
- Instytut Pomnik-Centrum Zdrowia Dziecka. Siatki centylowe dzieci i młodzieży w wieku 3-18 lat. Available online: http://www.czd.pl/index.php?option=com_content&view=article&id=1717&Itemid=538 (accessed on 1 September 2020).
- Barlow, S.E.; Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007, 120, 164–192. [Google Scholar] [CrossRef]
- Trandafir, L.M.; Temneanu, O.R. Pre and post-natal risk and determination of factors for child obesity. J. Med. Life 2016, 9, 386–391. [Google Scholar]
- Sridhar, S.B.; Darbinian, J.; Ehrlich, S.F.; Markman, M.A.; Gunderson, E.P.; Ferrara, A.; Hedderson, M.M. Maternal gestational weight gain and offspring risk for childhood overweight or obesity. Am. J. Obstet. Gynecol. 2014, 211, 259.e1–259.e8. [Google Scholar] [CrossRef]
- Varela-Silva, M.I.; Azcorra, H.; Dickinson, F.; Bogin, B.; Frisancho, A.R. Influence of maternal stature, pregnancy age, and infant birth weight on growth during childhood in Yucatan, Mexico: A test of the intergenerational effects hypothesis. Am. J. Hum. Biol. 2009, 21, 657–663. [Google Scholar] [CrossRef]
- Mourtakos, S.P.; Tambalis, K.D.; Panagiotakos, D.B.; Antonogeorgos, G.; Alexi, C.D.; Georgoulis, M.; Saade, G.; Sidossis, L.S. Association between gestational weight gain and risk of obesity in preadolescence: A longitudinal study (1997–2007) of 5125 children in Greece. J. Hum. Nutr. Diet. 2017, 30, 51–58. [Google Scholar] [CrossRef]
- Woo Baidal, J.A.; Locks, L.M.; Cheng, E.R.; Blake-Lamb, T.L.; Perkins, M.E.; Taveras, E.M. Risk Factors for Childhood Obesity in the First 1000 Days A Systematic Review. Am. J. Prev. Med. 2016, 50, 761–779. [Google Scholar] [CrossRef]
- Janjua, N.Z.; Mahmood, B.; Islam, M.A.; Goldenberg, R.L. Maternal and Early Childhood Risk Factors for Overweight and Obesity among Low-Income Predominantly Black Children at Age Five Years: A Prospective Cohort Study. J. Obes. 2012, 2012, 457173. [Google Scholar] [CrossRef] [PubMed]
- Barclay, K.; Myrskylä, M. Maternal age and offspring health and health behaviours in late adolescence in Sweden. SSM-Popul. Health 2016, 2, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Lei, J.; Ma, J.; Ma, Y.; Wang, S.; Yuan, Y.; Shang, Y.; Zhang, Z.; Niu, W. Interaction between delivery mode and maternal age in predicting overweight and obesity in 1123 Chinese preschool children. Ann. Transl. Med. 2020, 8, 474. [Google Scholar] [CrossRef] [PubMed]
- Saunders, T. Potential contributors to the Canadian pediatric obesity epidemic. ISRN Pediatr. 2011, 2011, 917684. [Google Scholar] [CrossRef] [PubMed]
- Power, M.L.; Lott, M.L.; Mackeen, A.D.; DiBari, J.; Schulkin, J. A retrospective study of gestational weight gain in relation to the Institute of Medicine’s recommendations by maternal body mass index in rural Pennsylvania from 2006 to 2015. BMC Pregnancy Childbirth 2018, 18, 239. [Google Scholar] [CrossRef]
- Von Kries, R.; Ensenauer, R.; Beyerlein, A.; Amann-Gassner, U.; Hauner, H.; Rosario, A.S. Gestational weight gain and overweight in children: Results from the cross-sectional German KiGGS study. Int. J. Ped. Obes. 2011, 6, 45–52. [Google Scholar] [CrossRef]
- Li, Q.; Xia, Y.-Y.; Zeng, Y.-S.; Zhang, Y.; Dai, C.-L.; Guo, J.J.; Zhao, Y. Risk of childhood overweight or obesity associated with excessive weight gain during pregnancy: A meta-analysis. Arch. Gynecol. Obstet. 2014, 289, 247–257. [Google Scholar] [CrossRef]
- Lau, E.Y.; Liu, J.; Archer, E.; McDonald, S.M.; Liu, J. Maternal Weight Gain in Pregnancy and Risk of Obesity among Offspring: A Systematic Review. J. Obes. 2014, 2014, 1–16. [Google Scholar] [CrossRef]
- Leonard, S.A.; Petito, L.C.; Rehkopf, D.H.; Ritchie, L.D.; Abrams, B. Weight gain in pregnancy and child weight status from birth to adulthood in the United States. Pediatr. Obes. 2017, 12, 18–25. [Google Scholar] [CrossRef]
- Whitaker, R.C. Predicting Preschooler Obesity at Birth: The Role of Maternal Obesity in Early Pregnancy. Pediatrics 2004, 114, e29–e36. [Google Scholar] [CrossRef]
- Olson, C.M.; Demment, M.M.; Carling, S.J.; Strawderman, M.S. Associations between Mothers’ and Their Children’s Weights at 4 Years of Age. Child. Obes. 2010, 6, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Olson, C.M.; Strawderman, M.S.; Dennison, B.A. Maternal Weight Gain during Pregnancy and Child Weight at Age 3 Years. Matern. Child Health J. 2009, 13, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Shao, T.; Tao, H.; Ni, L.; Sun, Y.; Yan, S.Q.; Gu, C.L.; Cao, H.; Huang, K.; Hao, J.H.; Tao, F.B. Maternal pre-pregnancy body mass index and gestational weight gain with preschool children’s overweight and obesity. Chin. J. Prev. Med. 2016, 50, 123–128. (In Chinese) [Google Scholar] [CrossRef]
- Leonard, S.A.; Rasmussen, K.M.; King, J.C.; Abrams, B. Trajectories of maternal weight from before pregnancy through postpartum and associations with childhood obesity. Am. J. Clin. Nutr. 2017, 106, 1295–1301. [Google Scholar] [CrossRef]
- Ludwig, D.S.; Currie, J. The association between pregnancy weight gain and birthweight: A within-family comparison. Lancet 2010, 376, 984–990. [Google Scholar] [CrossRef]
- Wrotniak, B.H.; Shults, J.; Butts, S.; Stettler, N. Gestational weight gain and risk of overweight in the offspring at age 7 y in a multicenter, multiethnic cohort study. Am. J. Clin. Nutr. 2008, 87, 1818–1824. [Google Scholar] [CrossRef]
- Houghton, L.C.; Ester, W.A.; Lumey, L.H.; Michels, K.; Wei, Y.; Cohn, B.; Susser, E.; Terry, M. Maternal weight gain in excess of pregnancy guidelines is related to daughters being overweight 40 years later. Am. J. Obstet. Gynecol. 2016, 215, 246.e1–246.e8. [Google Scholar] [CrossRef]
- Wan, N.; Cai, L.; Tan, W.; Zhang, T.; Yang, J.; Chen, Y. Associations of gestational weight gain with offspring thinness and obesity: By prepregnancy body mass index. Reprod. Health 2018, 15, 149. [Google Scholar] [CrossRef]
- Voerman, E.; Santos, S.; Patro Golab, B.; Amiano, P.; Ballester, F.; Barros, H.; Bergström, A.; Charles, M.-A.; Chatzi, L.; Chevrier, C.; et al. Maternal body mass index, gestational weight gain, and the risk of overweight and obesity across childhood: An individual participant data meta-analysis. PLoS Med. 2019, 16, e1002744. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Maternal Perinatal Risk Factors | Girls n = 358 | Boys n = 391 | p | ||||
|---|---|---|---|---|---|---|---|
| Me | s | Me | s | ||||
| Mother’s age at birth (y) | 27.1 | 27 | 4.8 | 27.4 | 27 | 4.8 | 0.379 |
| Gestational weight gain (kg) | 14.4 | 13 | 5.8 | 15.7 | 15 | 7.1 | 0.021 |
| Children | Body Mass Category | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Girls | Boys | All | |||||||
| NW UW | OW OB | p | NW UW | OW OB | p | NW UW | OW OB | p | |
| Mother’s age at birth (y) | |||||||||
| all | 27.2 | 26.4 | 0.245 | 27.3 | 28.2 | 0.436 | 27.2 | 27.3 | 0.754 |
| 4–6 y | 26.7 | 26.6 | 0.894 | 27.2 | 29.8 | 0.199 | 26.9 | 28.7 | 0.275 |
| 7–11 y | 27.5 | 26.3 | 0.293 | 27.8 | 27.6 | 0.732 | 27.6 | 27.0 | 0.330 |
| 12–15 y | 27.2 | 26.5 | 0.583 | 26.4 | 27.2 | 0.772 | 26.8 | 26.7 | 0.885 |
| Gestational weight gain (kg) | |||||||||
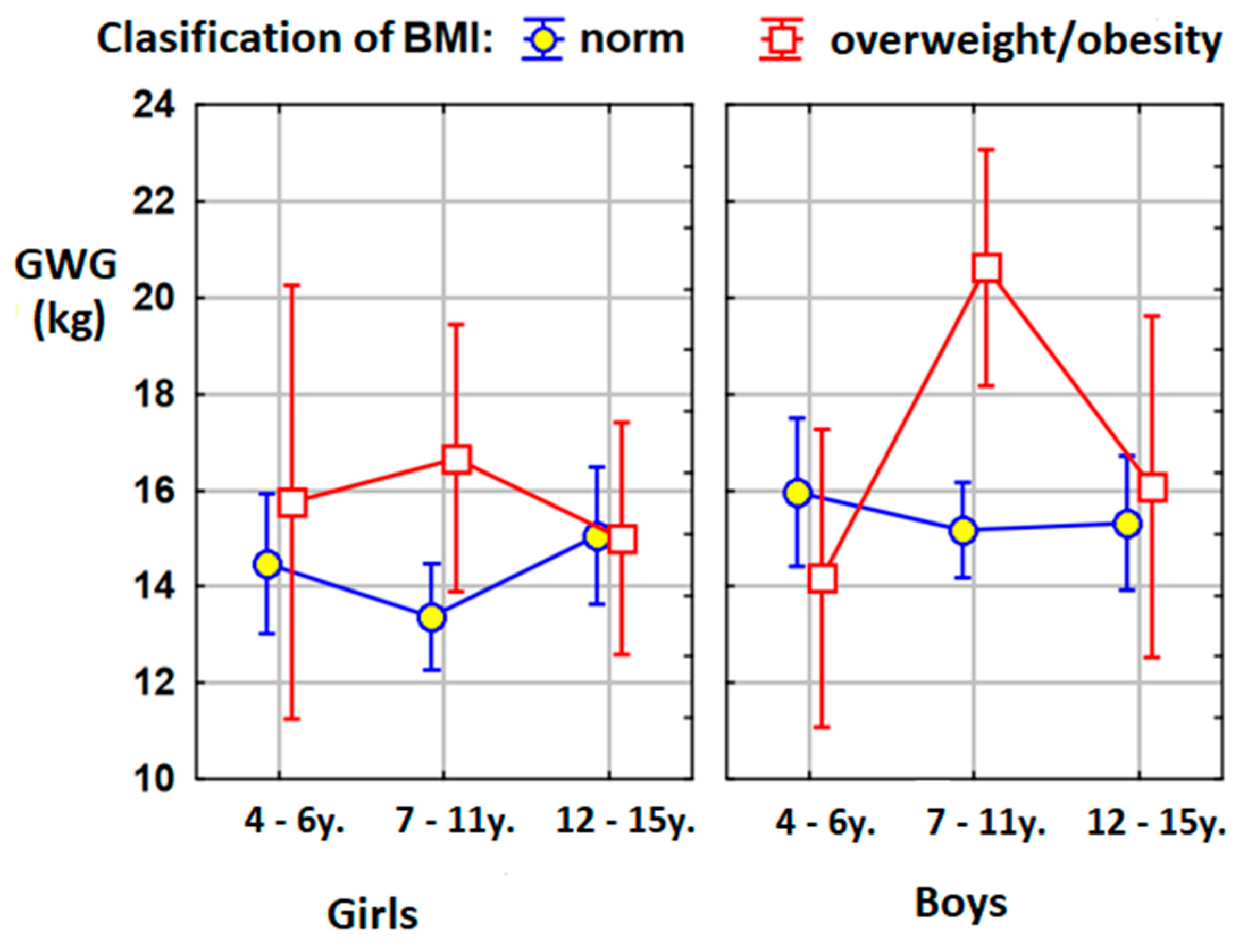
| all | 14.2 | 15.7 | 0.134 | 15.3 | 17.6 | 0.163 | 14.8 | 16.6 | 0.057 |
| 4–6 y | 14.6 | 15.8 | 0.379 | 15.9 | 14.3 | 0.468 | 15.2 | 14.8 | 0.959 |
| 7–11 y | 13.4 | 16.5 | 0.063 | 15.1 | 20.6 | 0.005 | 14.3 | 18.8 | 0.002 |
| 12–15 y | 15.1 | 15.0 | 0.685 | 15.4 | 15.8 | 0.980 | 15.3 | 15.3 | 0.797 |
| Children | BMI Percentile | ||
|---|---|---|---|
| Girls | Boys | All | |
| Mother’s age at birth (y) | |||
| All | 0.01 (p = 0.902) | 0.05 (p = 0.369) | 0.03 (p = 0.455) |
| 4–6 y | 0.05 (p = 0.640) | 0.09 (p = 0.390) | 0.09 (p = 0.260) |
| 7–11 y | −0.02 (p = 0.841) | −0.02 (p = 0.759) | −0.02 (p = 0.760) |
| 12–15 y | 0.01 (p = 0.877) | 0.09 (p = 0.377) | 0.06 (p = 0.356) |
| Gestational weight gain (kg) | |||
| All | 0.13 (p = 0.017) | 0.09 (p = 0.068) | 0.11 (p = 0.004) |
| 4–6 y | 0.12 (p = 0.249) | −0.01 (p = 0.944) | 0.06 (p = 0.461) |
| 7–11 y | 0.19 (p = 0.017) | 0.17 (p = 0.014) | 0.18 (p < 0.001) |
| 12–15 y | −0.02 (p = 0.802) | 0.04 (p = 0.660) | 0.01 (p = 0.831) |
| ANOVA Test | Mother’s Age at Birth (y) | Gestational Weight Gain (kg) |
|---|---|---|
| Sex | 0.081 | 0.107 |
| Age | 0.563 | 0.210 |
| body weight category by BMI percentile | 0.787 | 0.040 |
| sex × age | 0.301 | 0.183 |
| sex × body weight category by BMI percentile | 0.099 | 0.986 |
| age × body weight category by BMI percentile | 0.521 | 0.008 |
| sex × age × body weight category by BMI percentile | 0.702 | 0.351 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baran, J.; Weres, A.; Czenczek-Lewandowska, E.; Leszczak, J.; Kalandyk-Osinko, K.; Łuszczki, E.; Sobek, G.; Mazur, A. Excessive Gestational Weight Gain: Long-Term Consequences for the Child. J. Clin. Med. 2020, 9, 3795. https://doi.org/10.3390/jcm9123795
Baran J, Weres A, Czenczek-Lewandowska E, Leszczak J, Kalandyk-Osinko K, Łuszczki E, Sobek G, Mazur A. Excessive Gestational Weight Gain: Long-Term Consequences for the Child. Journal of Clinical Medicine. 2020; 9(12):3795. https://doi.org/10.3390/jcm9123795
Chicago/Turabian StyleBaran, Joanna, Aneta Weres, Ewelina Czenczek-Lewandowska, Justyna Leszczak, Katarzyna Kalandyk-Osinko, Edyta Łuszczki, Grzegorz Sobek, and Artur Mazur. 2020. "Excessive Gestational Weight Gain: Long-Term Consequences for the Child" Journal of Clinical Medicine 9, no. 12: 3795. https://doi.org/10.3390/jcm9123795
APA StyleBaran, J., Weres, A., Czenczek-Lewandowska, E., Leszczak, J., Kalandyk-Osinko, K., Łuszczki, E., Sobek, G., & Mazur, A. (2020). Excessive Gestational Weight Gain: Long-Term Consequences for the Child. Journal of Clinical Medicine, 9(12), 3795. https://doi.org/10.3390/jcm9123795