Risk of Developing Pancreatic Cancer in Patients with Chronic Pancreatitis

 , , ,
, , ,
Abstract
1. Introduction
2. Patients and Methods
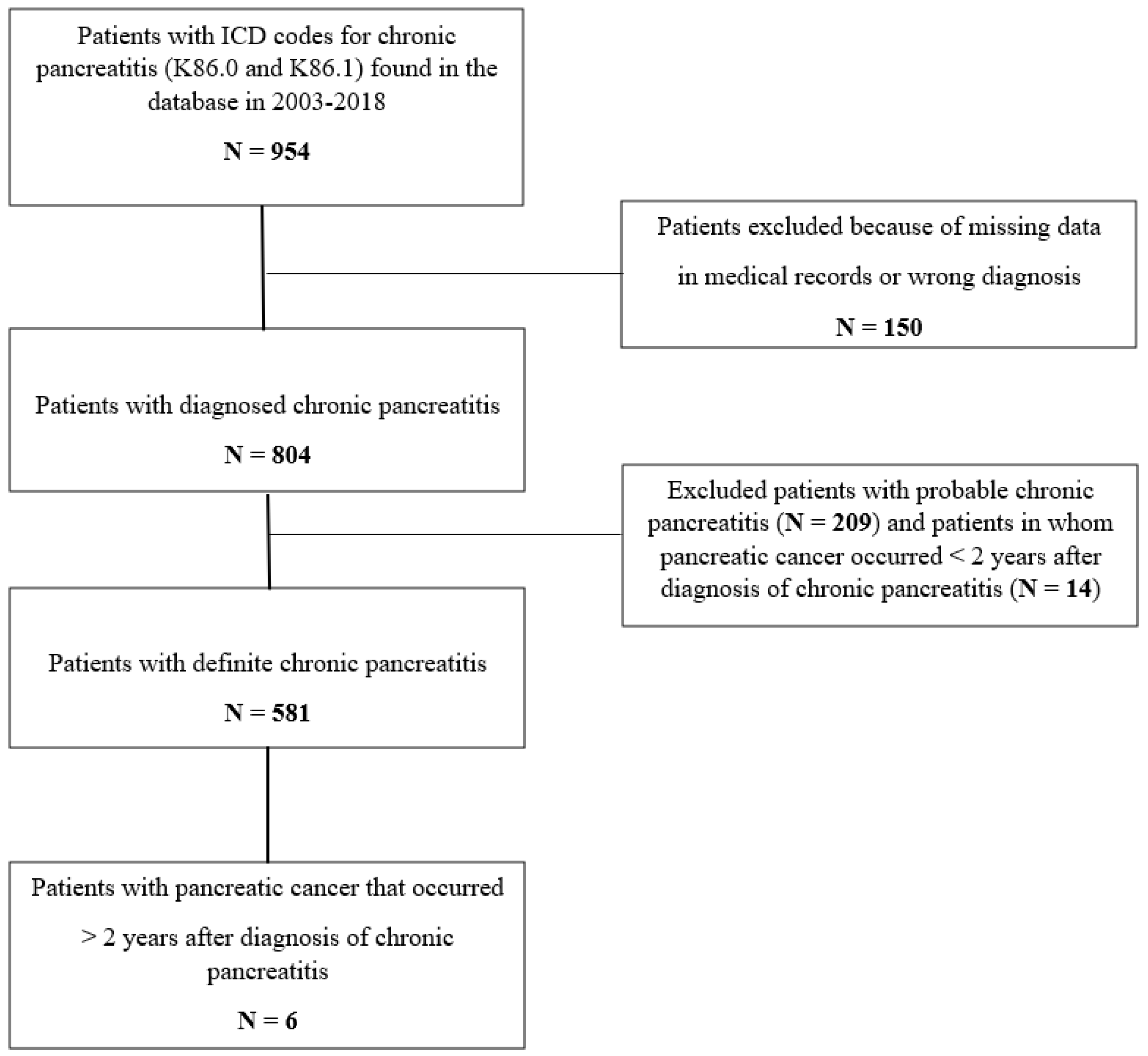
2.1. Study Population
2.2. Variables
2.3. Follow-Up
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Löhr, J.M.; Dominguez-Munoz, E.; Rosendahl, J.; Besselink, M.; Mayerle, J.; Lerch, M.M.; Haas, S.; Akisik, F.; Kartalis, N.; Iglesias-Garcia, J.; et al. United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU). United Eur. Gastroenterol. J. 2017, 5, 153–199. [Google Scholar] [CrossRef]
- Xiao, A.Y.; Tan, M.L.Y.; Wu, L.M.; Asrani, V.M.; Windsor, J.A.; Yadav, D.; Petrov, M.S. Global incidence and mortality of pancreatic diseases: A systematic review, meta-analysis, and meta-regression of population-based cohort studies. Lancet Gastroenterol. Hepatol. 2016, 1, 45–55. [Google Scholar] [CrossRef]
- Lévy, P.; Domínguez-Muñoz, E.; Imrie, C.; Löhr, M.; Maisonneuve, P. Epidemiology of chronic pancreatitis: Burden of the disease and consequences. United Eur. Gastroenterol. J. 2014, 2, 345–354. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Hidalgo, M.; Cascinu, S.S.; Kleeff, J.J.; Labianca, R.; Löhr, J.M.J.; Neoptolemos, J.; Real, F.F.; Van Laethem, J.-L.; Heinemann, V. Addressing the challenges of pancreatic cancer: Future directions for improving outcomes. Pancreatology 2015, 15, 8–18. [Google Scholar] [CrossRef]
- Kirkegård, J.; Mortensen, F.V.; Cronin-Fenton, D. Chronic Pancreatitis and Pancreatic Cancer Risk: A Systematic Review and Meta-analysis. Am. J. Gastroenterol. 2017, 112, 1366–1372. [Google Scholar] [CrossRef] [PubMed]
- Petrov, M.S.; Yadav, D. Global epidemiology and holistic prevention of pancreatitis. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Schneider, A.; Löhr, J.M.; Singer, M.V. The M-ANNHEIM classification of chronic pancreatitis: Introduction of a unifying classification system based on a review of previous classifications of the disease. J. Gastroenterol. 2007, 42, 101–119. [Google Scholar] [CrossRef] [PubMed]
- Shimosegawa, T.; Okazaki, K.; Kamisawa, T.; Kawa, S.; Notohara, K. International Consensus Diagnostic Criteria for autoimmune pancreatitis -Guidelines of the International Association of Pancreatology. Suizo 2011, 26, 684–698. [Google Scholar] [CrossRef]
- Luebeck, E.G. Cancer: Genomic evolution of metastasis. Nature 2010, 467, 1053–1055. [Google Scholar] [CrossRef] [PubMed]
- Howes, N.; Lerch, M.M.; Greenhalf, W.; Stocken, D.D.; Ellis, I.; Simon, P.; Truninger, K.; Ammann, R.; Cavallini, G.; Charnley, R.M.; et al. Clinical and genetic characteristics of hereditary pancreatitis in Europe. Clin. Gastroenterol. Hepatol. 2004, 2, 252–261. [Google Scholar] [CrossRef]
- Lowenfels, A.B.; Maisonneuve, P.; Cavallini, G.; Ammann, R.W.; Lankisch, P.G.; Andersen, J.R.; DiMagno, E.P.; Andren-Sandberg, A.; Domellof, L. Pancreatitis and the Risk of Pancreatic Cancer. N. Engl. J. Med. 1993, 328, 1433–1437. [Google Scholar] [CrossRef] [PubMed]
- Hart, P.A.; Bellin, M.D.; Andersen, D.K.; Bradley, D.; Cruz-Monserrate, Z.; Forsmark, C.E.; Goodarzi, M.O.; Habtezion, A.; Korc, M.; Kudva, Y.C.; et al. Type 3c (pancreatogenic) diabetes mellitus secondary to chronic pancreatitis and pancreatic cancer. Lancet Gastroenterol. Hepatol. 2016, 1, 226–237. [Google Scholar] [CrossRef]
- Duggan, S.N.; Smyth, N.D.; O’Sullivan, M.; Feehan, S.; Ridgway, P.F.; Conlon, K.C. The Prevalence of Malnutrition and Fat-Soluble Vitamin Deficiencies in Chronic Pancreatitis. Nutr. Clin. Pancreat. 2014, 29, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Duggan, S.N.; Ewald, N.; Kelleher, L.; Griffin, O.; Gibney, J.; Conlon, K.C. The nutritional management of type 3c (pancreatogenic) diabetes in chronic pancreatitis. Eur. J. Clin. Nutr. 2017, 71, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Sah, R.P.; Nagpal, S.J.; Mukhopadhyay, D.; Chari, S.T. New insights into pancreatic cancer-induced paraneoplastic diabetes. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 423–433. [Google Scholar] [CrossRef]
- Liao, K.-F.; Lai, S.-W.; Li, C.-I.; Chen, W.-C. Diabetes mellitus correlates with increased risk of pancreatic cancer: A population-based cohort study in Taiwan. J. Gastroenterol. Hepatol. 2012, 27, 709–713. [Google Scholar] [CrossRef]
- Trajkovic-Arsic, M.; Kalideris, E.; Siveke, J.T. The role of insulin and IGF system in pancreatic cancer. J. Mol. Endocrinol. 2013, 50, R67–R74. [Google Scholar] [CrossRef]
- Cascetta, P.; Cavaliere, A.; Piro, G.; Torroni, L.; Santoro, R.; Tortora, G.; Melisi, D.; Carbone, C. Pancreatic Cancer and Obesity: Molecular Mechanisms of Cell Transformation and Chemoresistance. Int. J. Mol. Sci. 2018, 19, 3331. [Google Scholar] [CrossRef]
- Eibl, G.; Rozengurt, E. KRAS, YAP, and obesity in pancreatic cancer: A signaling network with multiple loops. Semin. Cancer Biol. 2019, 54, 50–62. [Google Scholar] [CrossRef]
- Vujasinovic, M.; Valente, R.; Del Chiaro, M.; Permert, J.; Löhr, J.-M. Pancreatic Exocrine Insufficiency in Pancreatic Cancer. Nutrients 2017, 9, 183. [Google Scholar] [CrossRef] [PubMed]
- Löhr, J.M. Weighing in on weight loss in pancreatic cancer. Nature 2018, 558, 526–528. [Google Scholar] [CrossRef] [PubMed]
- Danai, L.V.; Babic, A.; Rosenthal, M.H.; Dennstedt, E.A.; Muir, A.; Lien, E.C.; Mayers, J.R.; Tai, K.; Lau, A.N.; Jones-Sali, P.; et al. Altered exocrine function can drive adipose wasting in early pancreatic cancer. Nature 2018, 558, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Sah, R.P.; Sharma, A.; Nagpal, S.; Patlolla, S.H.; Sharma, A.; Kandlakunta, H.; Anani, V.; Angom, R.S.; Kamboj, A.K.; Ahmed, N.; et al. Phases of Metabolic and Soft Tissue Changes in Months Preceding a Diagnosis of Pancreatic Ductal Adenocarcinoma. Gastroenterology 2019, 156, 1742–1752. [Google Scholar] [CrossRef] [PubMed]
- Lowenfels, A.B.; Maisonneuve, P.; Whitcomb, D.C. Risk Factors for Cancer in Hereditary Pancreatitis. Med. Clin. N. Am. 2000, 84, 565–573. [Google Scholar] [CrossRef]
- Hirano, K.; Tada, M.; Sasahira, N.; Isayama, H.; Mizuno, S.; Takagi, K.; Watanabe, T.; Saito, T.; Kawahata, S.; Uchino, R.; et al. Incidence of Malignancies in Patients with IgG4-related Disease. Intern. Med. 2014, 53, 171–176. [Google Scholar] [CrossRef]
- Schneider, A.; Hirth, M.; Münch, M.; Weiss, C.; Löhr, J.M.; Ebert, M.P.; Pfützer, R.H. Risk of Cancer in Patients with Autoimmune Pancreatitis: A Single-Center Experience from Germany. Digestion 2017, 95, 172–180. [Google Scholar] [CrossRef]
- Löhr, J.M.; Beuers, U.; Vujasinovic, M.; Alvaro, D.; Frokjaer, J.B.; Buttgereit, F.; Capurso, G.; Culver, E.L.; De-Madaria, E.; Della-Torre, E.; et al. European Guideline on IgG4-related digestive disease—UEG and SGF evidence-based recommendations. United Eur. Gastroenterol. J. 2020, 8, 637–666. [Google Scholar] [CrossRef]
- Rocca, G.; Gaia, E.; Iuliano, R.; Caselle, M.T.; Rocca, N.; Calcamuggi, G.; Emanuelli, G. Increased Incidence of Cancer in Chronic Pancreatitis. J. Clin. Gastroenterol. 1987, 9, 175–179. [Google Scholar] [CrossRef]
- Karlson, B.M.; Ekbom, A.; Josefsson, S.; McLaughlin, J.K.; Fraumeni, J.F.; Nyren, O. The risk of pancreatic cancer following pancreatitis: An association due to confounding? Gastroenterology 1997, 113, 587–592. [Google Scholar] [CrossRef]
- Talamini, G.; Falconi, M.; Bassi, C.; Sartori, N.; Salvia, R.; Caldiron, E.; Frulloni, L.; di Francesco, V.; Vaona, B.; Bovo, P.; et al. Incidence of cancer in the course of chronic pancreatitis. Am. J. Gastroenterol. 1999, 94, 1253–1260. [Google Scholar] [CrossRef] [PubMed]
- Malka, D.; Hammel, P.; Maire, F.; Rufat, P.; Madeira, I.; Pessione, F.; Lévy, P.; Ruszniewski, P. Risk of pancreatic adenocarcinoma in chronic pancreatitis. Gut 2002, 51, 849–852. [Google Scholar] [CrossRef] [PubMed]
- Seicean, A.; Tantău, M.; Grigorescu, M.; Mocan, T.; Seicean, R.; Pop, T. Mortality risk factors in chronic pancreatitis. J. Gastrointest. Liver Dis. 2006, 15, 21–26. [Google Scholar]
- Goldacre, M.J.; Wotton, C.J.; Yeates, D.; Seagroatt, V.; Collier, J. Liver cirrhosis, other liver diseases, pancreatitis and subsequent cancer: Record linkage study. Eur. J. Gastroenterol. Hepatol. 2008, 20, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Pedrazzoli, S.; Pasquali, C.; Guzzinati, S.; Berselli, M.; Sperti, C. Survival Rates and Cause of Death in 174 Patients with Chronic Pancreatitis. J. Gastrointest. Surg. 2008, 12, 1930–1937. [Google Scholar] [CrossRef]
- Wang, W.; Liao, Z.; Li, G.; Li, Z.; Chen, J.; Zhan, X.; Wang, L.-W.; Liu, F.; Hu, L.-H.; Guo, Y.; et al. Incidence of Pancreatic Cancer in Chinese Patients with Chronic Pancreatitis. Pancreatology 2011, 11, 16–23. [Google Scholar] [CrossRef]
- Kudo, Y.; Kamisawa, T.; Anjiki, H.; Takuma, K.; Egawa, N. Incidence of and risk factors for developing pancreatic cancer in patients with chronic pancreatitis. Hepatogastroenterology 2011, 58, 609–611. [Google Scholar]
- Dite, P.; Hermanová, M.; Trna, J.; Novotný, I.; Ružicka, M.; Liberda, M.; Bártková, A. The Role of Chronic Inflammation: Chronic Pancreatitis as a Risk Factor of Pancreatic Cancer. Dig. Dis. 2012, 30, 277–283. [Google Scholar] [CrossRef]
- Bang, U.C.; Benfield, T.; Hyldstrup, L.; Bendtsen, F.; Jensen, J.B. Mortality, Cancer, and Comorbidities Associated With Chronic Pancreatitis: A Danish Nationwide Matched-Cohort Study. Gastroenterology 2014, 146, 989–994. [Google Scholar] [CrossRef]
- Hao, L.; Zeng, X.-P.; Xin, L.; Wang, D.; Pan, J.; Wen-Bin, Z.; Ji, J.-T.; Du, T.-T.; Lin, J.-H.; Zhang, D.; et al. Incidence of and risk factors for pancreatic cancer in chronic pancreatitis: A cohort of 1656 patients. Dig. Liver Dis. 2017, 49, 1249–1256. [Google Scholar] [CrossRef]
- Zheng, Z.; Chen, Y.; Tan, C.; Ke, N.; Du, B.; Liu, X. Risk of pancreatic cancer in patients undergoing surgery for chronic pancreatitis. BMC Surg. 2019, 19, 83. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Sharma, S.; Gunjan, D.; Singh, N.; Kaushal, K.; Poudel, S.; Anand, A.; Gopi, S.; Mohta, S.; Sonika, U.; et al. Natural course of chronic pancreatitis and predictors of its progression. Pancreatology 2020, 20, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Maisonneuve, P.; Lowenfels, A.B.; Müllhaupt, B.; Cavallini, G.; Lankisch, P.G.; Andersen, J.R.; DiMagno, E.P.; Andrén-Sandberg, Å.; Domellöf, L.; Frulloni, L.; et al. Cigarette smoking accelerates progression of alcoholic chronic pancreatitis. Gut 2005, 54, 510–514. [Google Scholar] [CrossRef] [PubMed]
- Korc, M.; Jeon, C.Y.; Edderkaoui, M.; Pandol, S.J.; Petrov, M.S. Tobacco and alcohol as risk factors for pancreatic cancer. Best Pract. Res. Clin. Gastroenterol. 2017, 31, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Ueda, J.; Tanaka, M.; Ohtsuka, T.; Tokunaga, S.; Shimosegawa, T. Surgery for chronic pancreatitis decreases the risk for pancreatic cancer: A multicenter retrospective analysis. Surgery 2013, 153, 357–364. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | All CP Patients N (%) † | Pancreas Cancer N (%) | Person-Year | Rate Per 100-Year | Log-Rank p |
|---|---|---|---|---|---|
| All | 581 (100.0) | 6 (1.03) | 3423 | 0.18 | |
| Sex | |||||
| Female | 210 (36.1) | 3 (1.43) | 1232 | 0.24 | |
| Male | 371 (63.9) | 3 (0.81) | 2191 | 0.14 | 0.48 |
| Age at diagnosis | |||||
| <50 | 183 (31.5) | - | 1223 | 0.00 | |
| 50–59 | 134 (23.1) | - | 842 | 0.00 | |
| 60–69 | 133 (22.9) | 4 (3.01) | 710 | 0.56 | |
| 70–79 | 105 (18.1) | 2 (1.90) | 532 | 0.38 | |
| ≥80 | 26 (4.5) | - | 116 | 0.00 | 0.020 |
| BMI at diagnosis | |||||
| <20 | 94 (16.2) | 2 (2.13) | 554 | 0.36 | |
| 21–25 | 165 (28.4) | - | 941 | 0.00 | |
| 26–31 | 98 (16.9) | 3 (3.06) | 492 | 0.61 | |
| 31+ | 18 (3.1) | 1 (5.56) | 93 | 1.08 | 0.065 |
| Family history of pancreas diseases | |||||
| No | 404 (69.5) | 4 (0.99) | 2491 | 0.16 | |
| Yes | 41 (7.1) | - | 258 | 0.00 | 0.51 |
| Aetiology | |||||
| Idiopathic | 47 (8.1) | - | 229 | 0.00 | |
| Alcohol and nicotine | 220 (37.9) | 1 (0.45) | 1343 | 0.07 | |
| Nicotine | 81 (13.9) | 2 (2.47) | 458 | 0.44 | |
| Alcohol | 49 (8.4) | 1 (2.04) | 312 | 0.32 | |
| Hereditary | 38 (6.5) | - | 281 | 0.00 | |
| Immunological | 59 (10.2) | - | 318 | 0.00 | |
| Efferent duct | 62 (10.7) | 1 (1.61) | 359 | 0.28 | |
| Miscellaneous/other | 25 (4.3) | 1 (4.00) | 123 | 0.81 | 0.40 |
| Diabetes mellitus at diagnosis | |||||
| No | 419 (72.1) | 3 (0.72) | 2570 | 0.12 | |
| Yes | 147 (25.3) | 3 (2.04) | 799 | 0.38 | 0.12 |
| PEI at diagnosis | |||||
| No | 273 (47.0) | 3 (1.10) | 1749 | 0.17 | |
| Yes | 226 (38.9) | 3 (1.33) | 1082 | 0.28 | 0.52 |
| History of acute pancreatitis | |||||
| No | 195 (33.6) | 5 (2.56) | 986 | 0.51 | |
| Yes | 379 (65.2) | 1 (0.26) | 2376 | 0.04 | 0.003 |
| Recurrent acute pancreatitis | |||||
| No | 303 (52.2) | 6 (1.98) | 1705 | 0.35 | |
| Yes | 267 (46.0) | - | 1646 | 0.00 | 0.014 |
| Patient | Age * | Sex | Aetiology CP | Previous AP | Smoking | Alcohol | BMI | DM | PEI | Time to PDAC ** | Survival after PDAC |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 63 | female | nicotine | no | former | never | 18.9 | developed after CP diagnosis; (1 year before PDAC diagnosis) | present at CP diagnosis | 2.7 years | 1.5 months |
| 2 | 65 | male | alcohol and nicotine | no | active | 30 years | 18.0 | developed after CP diagnosis; (at the time of PDAC diagnosis) | presentat CP diagnosis | 6.6 years | 6 months |
| 3 | 64 | male | unexplained | no | former | never | 26.3 | present at CP diagnosis; (52 years before PDAC diagnosis) | developed after CP diagnosis | 8.6 years | 13 months |
| 4 | 68 | female | alcohol and nicotine | no | former | 40 years | 32.4 | present at CP diagnosis; (33 years before PDAC diagnosis) | developed after CP diagnosis | 7.0 years | 1 month |
| 5 | 74 | female | nicotine | no | active | never | 26.0 | present at CP diagnosis; (11 years before PDAC diagnosis) | developed after CP diagnosis | 6.0 years | 2 months |
| 6 | 79 | male | efferent duct factors | yes | never | never | 29.1 | no | no | 4.8 years | 0.5 months |
| Patients N | Pancreatic Cancers Diagnosed in the First 2 Years after CP * N (%) | Pancreas Cancers Diagnosed More than 2 Years after CP N (%) | ||
|---|---|---|---|---|
| All | 595 | 14 (2.4) | 6 (1.01) | |
| Risk group | ||||
| No previous AP, low BMI, and PEI | 22 | 2 (9.1) | 2 (9.1) | |
| No previous AP, high BMI, and DM | 12 | 2 (16.7) | 3 (25.0) | |
| Other CP patients | 561 | 10 (1.8) | 1 (0.18) | p < 0.001 |
| First Author | Year | Study Type | Period | Follow-Up | N | PDAC | SEX | AGE (Years) |
|---|---|---|---|---|---|---|---|---|
| Rocca [29] | 1987 | Single centre study | Italy 1970–1984 | 14 years | 172 | 2 cases (1.1%) | males 85.7% | 50 |
| Lowenfels [12] | 1993 | Multicentric multinational | Multinational 1946–1989 | 7.4 years (11,438-person years) | 1552 | 29 cases * (2.5%) | males 81% | 44.6 |
| Karlson [30] | 1997 | Swedish Inpatient Registry | Sweden 1965–1983 | NA | 4546 | 189 cases (4.2%) | males 72% | 53.2 |
| Talamini [31] | 1999 | Single centre study | Italy 1971–1995 | 10 years (7287-person years) | 715 | 14 cases (2.0%) | males 88% | 40.8 |
| Malka [32] | 2002 | Single centre study | France 1973–1997 | 9.2 years | 373 | 4 cases (1.1%) | males 86% | 42 |
| Seicean [33] | 2006 | Single centre study | Romania 1999–2005 | 2 years | 82 | 3 cases (3.6%) | Male:female Ratio = 6.5:1 | 48.7 |
| Goldacre [34] | 2008 | Oxford Record Linkage Study | United Kingdom 1963–1999 | NA | 1496 | 86 cases (5.7%) | males 55% | NA |
| Pedrazzoli [35] | 2008 | Single centre study | Italy 1970–1997 | NA | 170 | 2 cases (1.2%) | males 87% | 45 |
| Wang [36] | 2011 | Single centre study | China 1997–2007 | 8.5 years | 420 | 4 cases (0.9%) | males 68% | 43.4 |
| Kudo [37] | 2011 | Single centre study | Japan 1970–2008 | NA | 218 | 9 cases (4.1%) | males 91.3% | 56.8 |
| Dite [38] | 2012 | Single centre study | Czech Republic 1992–2005 | 6.7 years | 223 | 13 cases (5.8%) | males 66.4% | 56.1 |
| Ueda [45] | 2013 | Nationwide survey | Japan 2009–2010 | 8 years | 506 | 19 cases (3.7%) | males 83.6% | 52.5 |
| Bang [39] | 2014 | Nationwide register retrospective cohort | Denmark 1997–2010 | 71,814-person years | 11,972 | 510 cases (4.25%) 172 cases * (1.4%) | males 66.5% | 54.5 |
| Hao [40] | 2017 | Single centre study | China 2000–2013 | 8.0 years | 1656 | 21 cases (1.3%) | males 69.6% | 43 |
| Zheng [41] | 2019 | Single centre study | China 2009–2017 | 4.4 years | 650 | 12 cases (1.8%) | males 78.5% | 45 |
| Agarwal [42] | 2020 | Single centre study | India 1998–2019 | 3.6 years | 1415 | 29 cases (2.0%) | males 78.3% | 34 |
| Present Study | 2020 | Single centre study | Sweden 2003–2018 | 5.9 years (3423-person years) | 581 | 6 cases * (1.0%) 0.2% per year | males 63.9% | 55.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vujasinovic, M.; Dugic, A.; Maisonneuve, P.; Aljic, A.; Berggren, R.; Panic, N.; Valente, R.; Pozzi Mucelli, R.; Waldthaler, A.; Ghorbani, P.; et al. Risk of Developing Pancreatic Cancer in Patients with Chronic Pancreatitis. J. Clin. Med. 2020, 9, 3720. https://doi.org/10.3390/jcm9113720
Vujasinovic M, Dugic A, Maisonneuve P, Aljic A, Berggren R, Panic N, Valente R, Pozzi Mucelli R, Waldthaler A, Ghorbani P, et al. Risk of Developing Pancreatic Cancer in Patients with Chronic Pancreatitis. Journal of Clinical Medicine. 2020; 9(11):3720. https://doi.org/10.3390/jcm9113720
Chicago/Turabian StyleVujasinovic, Miroslav, Ana Dugic, Patrick Maisonneuve, Amer Aljic, Robin Berggren, Nikola Panic, Roberto Valente, Raffaella Pozzi Mucelli, Alexander Waldthaler, Poya Ghorbani, and et al. 2020. "Risk of Developing Pancreatic Cancer in Patients with Chronic Pancreatitis" Journal of Clinical Medicine 9, no. 11: 3720. https://doi.org/10.3390/jcm9113720
APA StyleVujasinovic, M., Dugic, A., Maisonneuve, P., Aljic, A., Berggren, R., Panic, N., Valente, R., Pozzi Mucelli, R., Waldthaler, A., Ghorbani, P., Kordes, M., Hagström, H., & Löhr, J.-M. (2020). Risk of Developing Pancreatic Cancer in Patients with Chronic Pancreatitis. Journal of Clinical Medicine, 9(11), 3720. https://doi.org/10.3390/jcm9113720