Professional Assessment of the Impact of COVID-19 on Handling NET Patients

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
3. Results
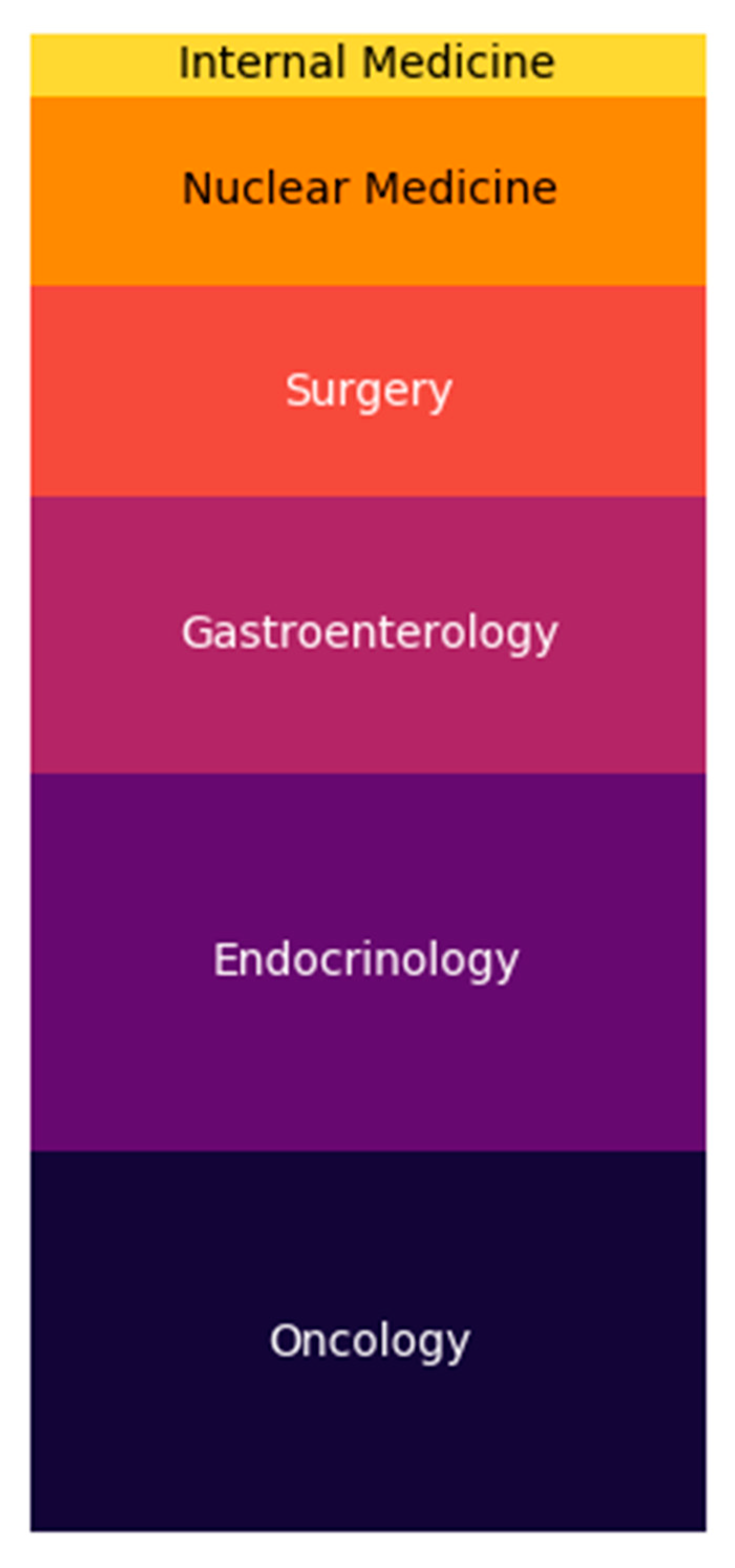
3.1. Characteristics of Physicians and Facilities
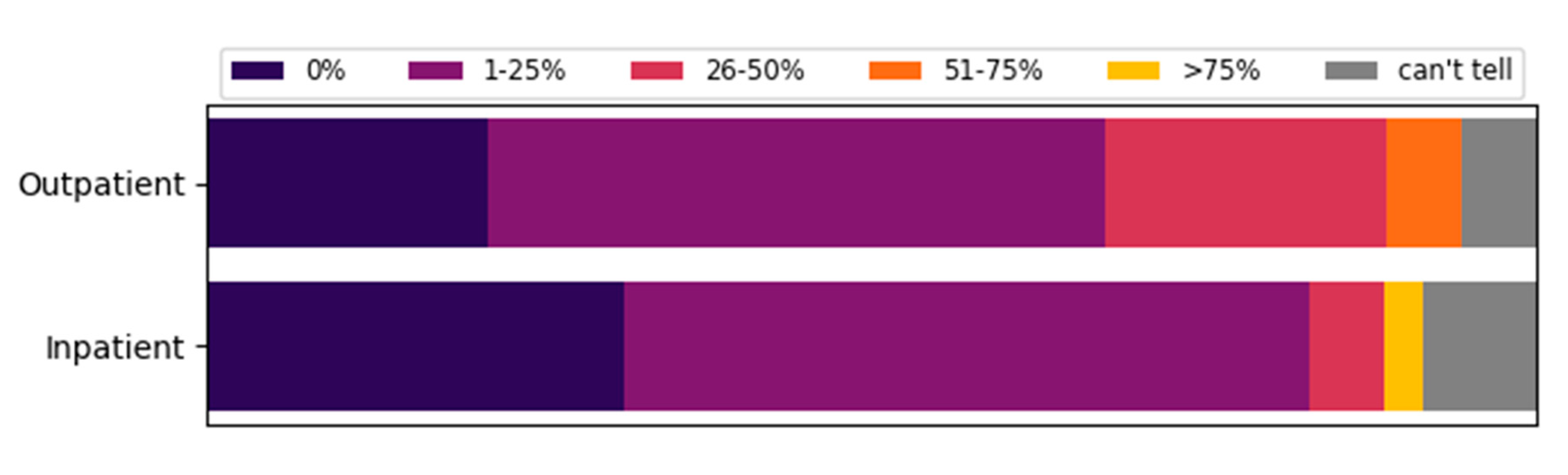
3.2. Influence of COVID-19 on Outpatient and Inpatient Care
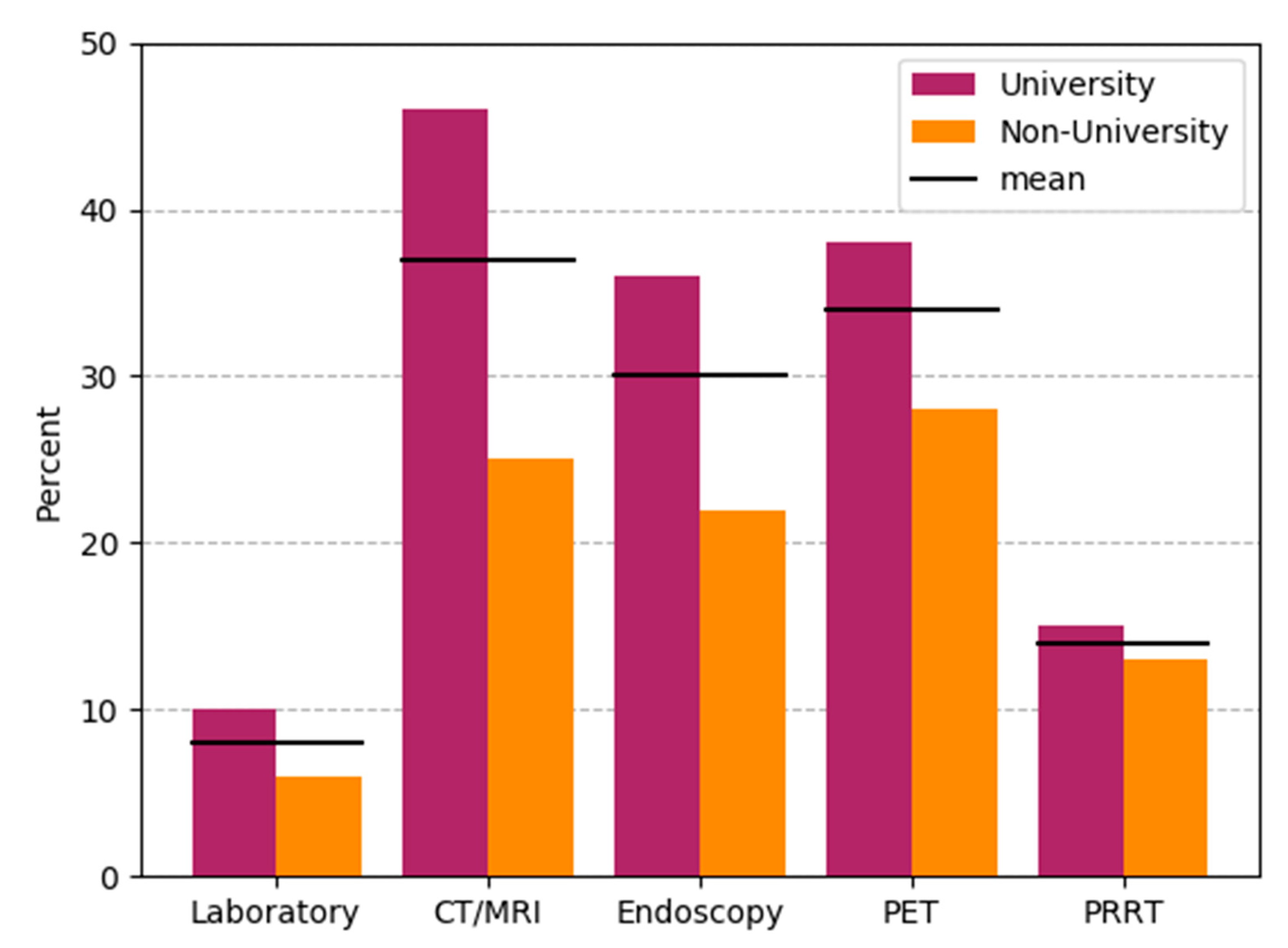
3.3. Reasons for Cancellation/Postponing of Appointments
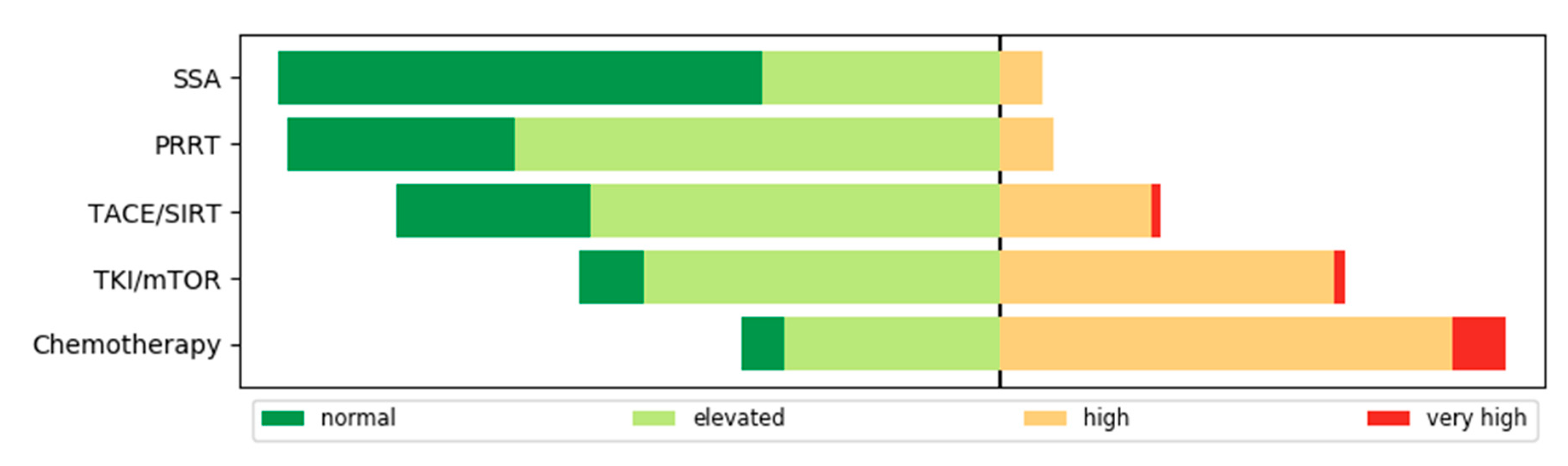
3.4. Risk for a Severe Course of COVID-19 and Recommendation of COVID-19 Tests
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- RKI. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Risikobewertung.html?nn=13490888 (accessed on 9 September 2020).
- Tartarone, A.; Lerose, R. COVID-19 and cancer care: What do international guidelines say? Med. Oncol. 2020, 37, 1–5. [Google Scholar] [CrossRef] [PubMed]
- ESMO. Available online: https://www.esmo.org/guidelines/cancer-patient-management-during-the-covid-19-pandemic (accessed on 9 September 2020).
- Pavel, M.; O’Toole, D.; Costa, F.; Capdevila, J.; Gross, D.; Kianmanesh, R.; Krenning, E.; Knigge, U.; Salazar, R.; Pape, U.-F.; et al. ENETS Consensus Guidelines Update for the Management of Distant Metastatic Disease of Intestinal, Pancreatic, Bronchial Neuroendocrine Neoplasms (NEN) and NEN of Unknown Primary Site. Neuroendocrinology 2016, 103, 172–185. [Google Scholar] [CrossRef] [PubMed]
- Rinke, A.; Wiedenmann, B.; Auernhammer, C.; Bartenstein, P.; Bartsch, D.K.; Begum, N.; Faiss, S.; Fottner, C.; Gebauer, B.; Goretzki, P.; et al. Practice guideline neuroendocrine tumors—AWMF-Reg. 021-27. Z. Gastroenterol. 2018, 56, 583–681. [Google Scholar] [CrossRef]
- Ramirez, R.A.; Bren-Mattison, Y.; Thiagarajan, R.; Boudreaux, J.P.; Marsala, A.J.; Ryan, P.; Maluccio, M.A. A Neuroendocrine Tumor Specialty Center in New Orleans’ (NOLANETS) Response to Patient Care During the COVID-19 Pandemic. Oncologist 2020, 25, 548–551. [Google Scholar] [CrossRef] [PubMed]
- Riechelmann, R.P.; Peixoto, R.D.; Fernandes, G.D.S.; Weschenfelder, R.F.; Prolla, G.; Filho, D.R.; Andrade, A.C.; Crosara, M.; Rego, J.F.M.; Gansi, R.C.; et al. Evidence-based recommendations for gastrointestinal cancers during the COVID-19 pandemic by the Brazilian Gastrointestinal Tumours Group. Ecancermedicalscience 2020, 14, 14. [Google Scholar] [CrossRef] [PubMed]
- Spada, F.; Pellicori, S.; Zampino, G.; Funicelli, L.; Gervaso, L.; Laffi, A.; Rubino, M.; Garcia-Carbonero, R.; Fazio, N. SARS-CoV-2-related pneumonia can be successfully managed in patients with metastatic neuroendocrine tumors: A critical point of view. Endocrine 2020, 70, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Bergsland, E.K.; Halperin, D.M.; Dillon, J.S.; Dasari, N.A.; Kunz, P.L.; Soares, H.P.; Pryma, D.; Bodei, L.; Hope, T.; Soulen, M.C.; et al. North American Neuroendocrine Tumor Society Guide for Neuroendocrine Tumor Patient Health Care Providers during COVID-19. Pancreas 2020, 49, 723–728. [Google Scholar] [CrossRef] [PubMed]
- Panzuto, F.; Maccauro, M.; Campana, D.; Faggiano, A.; Massironi, S.; Pusceddu, S.; Spada, F.; Ferone, D.; Modica, R.; Grana, C.M.; et al. Impact of the SARS-CoV2 pandemic dissemination on the management of neuroendocrine neoplasia in Italy: A report from the Italian Association for Neuroendocrine Tumors (Itanet). J. Endocrinol. Investig. 2020, 1–6. [Google Scholar] [CrossRef]
- Zhang, L.; Zhu, F.; Xie, L.; Wang, C.; Wang, J.; Chen, R.; Jia, P.; Guan, H.; Peng, L.; Chen, Y.; et al. Clinical characteristics of COVID-19-infected cancer patients: A retrospective case study in three hospitals within Wuhan, China. Ann. Oncol. 2020, 31, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Langley, J.M.; Dodds, L.; Fell, D.; Langley, G.R. Pneumococcal and influenza immunization in asplenic persons: A retrospective population-based cohort study 1990–2002. BMC Infect. Dis. 2010, 10, 219. [Google Scholar] [CrossRef] [PubMed]
- Casey, R.T.; Valk, G.D.; Schalin-Jäntti, C.; Grossman, A.B.; Thakker, R. ENDOCRINOLOGY IN THE TIME OF COVID-19: Clinical management of neuroendocrine neoplasms (NENs). Eur. J. Endocrinol. 2020, 183, G79–G88. [Google Scholar] [CrossRef] [PubMed]
- De Azambuja, E.; Trapani, D.; Loibl, S.; Delaloge, S.; Senkus, E.; Criscitiello, C.; Poortman, P.; Gnant, M.; Di Cosimo, S.; Cortes, J.; et al. ESMO Management and treatment adapted recommendations in the COVID-19 era: Breast Cancer. ESMO Open 2020, 5, e000793. [Google Scholar] [CrossRef] [PubMed]
- Bodei, L.; Bergsland, E.K.; De Herder, W.K.; Ferone, D.; Hicks, R.J.; Hope, T.A.; Kunikowska, J.A.; Pavel, M.; Reidy-Lagunes, D.L.; Siveke, J.; et al. Peptide Receptor Radionuclide Therapy During the COVID-19 Pandemic: Are There Any Concerns? J. Nucl. Med. 2020, 61, 1094–1095. [Google Scholar] [CrossRef] [PubMed]
- Aeppli, S.; Eboulet, E.I.; Eisen, T.; Escudier, B.; Fischer, S.; Larkin, J.; Grünwald, V.; McDermott, D.; Oldenburg, J.; Omlin, A.; et al. Impact of COVID-19 pandemic on treatment patterns in metastatic clear cell renal cell carcinoma. ESMO Open 2020, 5, e000852. [Google Scholar] [CrossRef] [PubMed]
- Terrazzano, G.; Rubino, V.; Palatucci, A.T.; Giovazzino, A.; Carriero, F.; Ruggiero, G. An Open Question: Is It Rational to Inhibit the mTor-Dependent Pathway as COVID-19 Therapy? Front. Pharmacol. 2020, 11, 856. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.Y.W.; Cazier, J.-B.; Starkey, T.; Briggs, S.E.W.; Arnold, R.; Bisht, V.; Booth, S.; Campton, N.A.; Cheng, V.W.T.; Collins, G.; et al. COVID-19 prevalence and mortality in patients with cancer and the effect of primary tumour subtype and patient demographics: A prospective cohort study. Lancet Oncol. 2020, 21, 1309–1316. [Google Scholar] [CrossRef]
- Pinato, D.J.; Zambelli, A.; Aguilar-Company, J.; Bower, M.; Sng, C.; Salazar, R.; Bertuzzi, A.; Brunet, J.; Mesia, R.; Segui, E.; et al. Clinical portrait of the SARS-CoV-2 epidemic in European cancer patients. Cancer Discov. 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Jee, J.; Foote, M.B.; Lumish, M.; Stonestrom, A.J.; Wills, B.; Narendra, V.; Avutu, V.; Murciano-Goroff, Y.R.; Chan, J.E.; Derkach, A.; et al. Chemotherapy and COVID-19 Outcomes in Patients with Cancer. J. Clin. Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krug, S.; Garbe, J.; König, S.; Ungewiss, H.; Michl, P.; Rinke, A.; Schrader, J. Professional Assessment of the Impact of COVID-19 on Handling NET Patients. J. Clin. Med. 2020, 9, 3633. https://doi.org/10.3390/jcm9113633
Krug S, Garbe J, König S, Ungewiss H, Michl P, Rinke A, Schrader J. Professional Assessment of the Impact of COVID-19 on Handling NET Patients. Journal of Clinical Medicine. 2020; 9(11):3633. https://doi.org/10.3390/jcm9113633
Chicago/Turabian StyleKrug, Sebastian, Jakob Garbe, Senta König, Hanna Ungewiss, Patrick Michl, Anja Rinke, and Jörg Schrader. 2020. "Professional Assessment of the Impact of COVID-19 on Handling NET Patients" Journal of Clinical Medicine 9, no. 11: 3633. https://doi.org/10.3390/jcm9113633
APA StyleKrug, S., Garbe, J., König, S., Ungewiss, H., Michl, P., Rinke, A., & Schrader, J. (2020). Professional Assessment of the Impact of COVID-19 on Handling NET Patients. Journal of Clinical Medicine, 9(11), 3633. https://doi.org/10.3390/jcm9113633