Seroprevalence of SARS-CoV-2 IgG Antibodies in Corsica (France), April and June 2020

 ,
,  , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Experimental Section
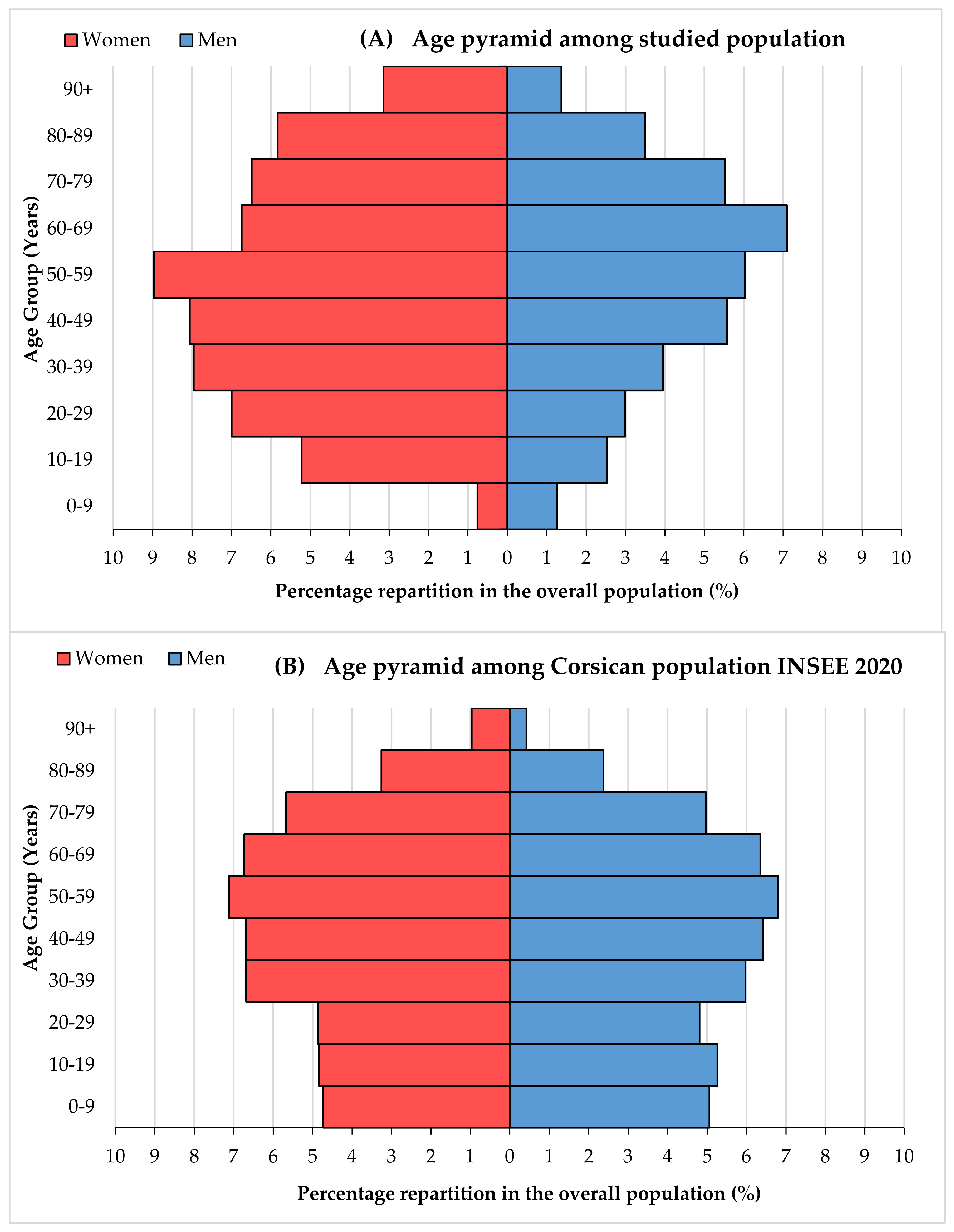
2.1. Study Area and Population
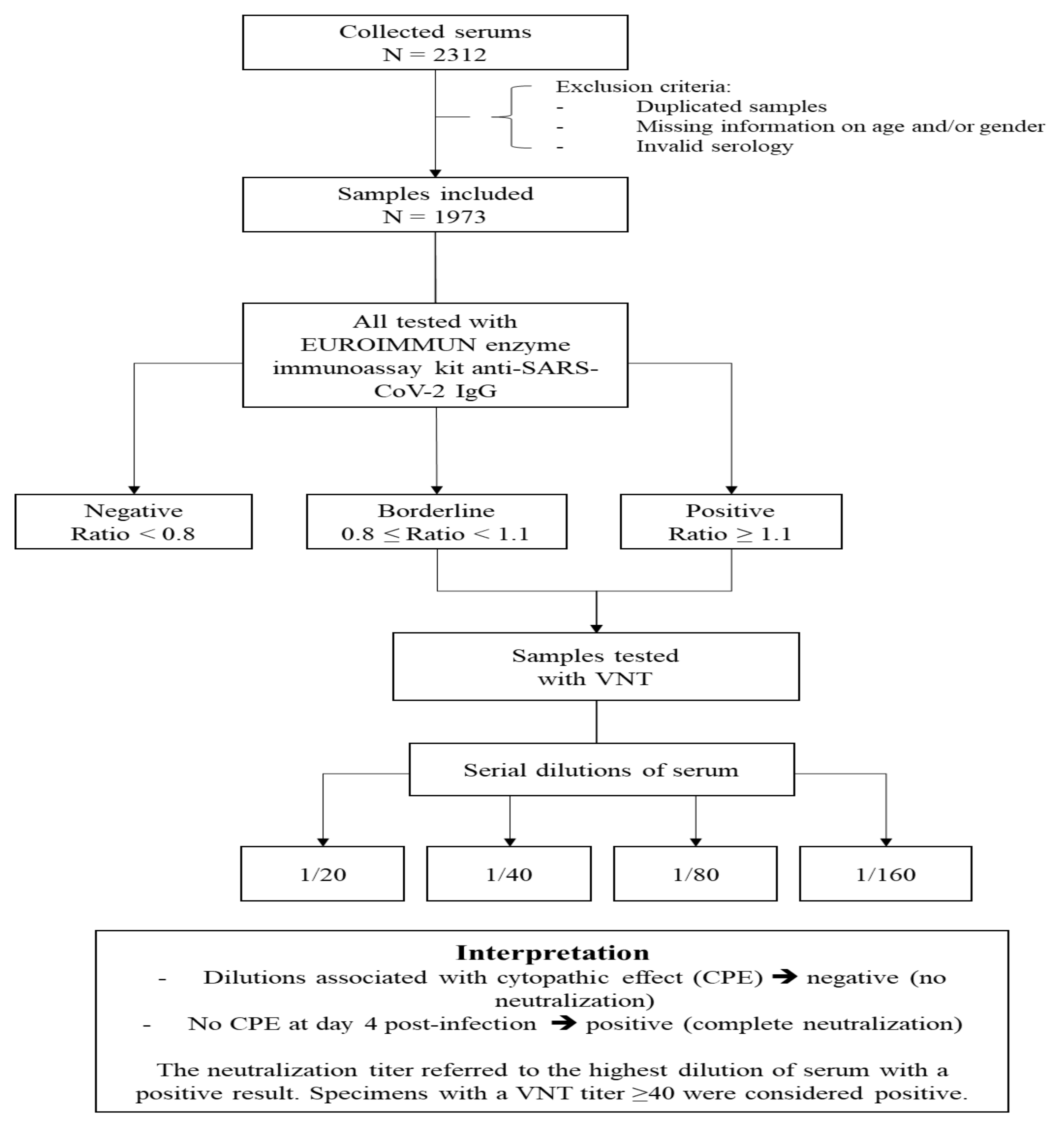
2.2. Sample Size
2.3. Studied Population
2.4. Serological Analyses
2.5. Ethical Statement
2.6. Collection Data and Statistical Analysis
3. Results
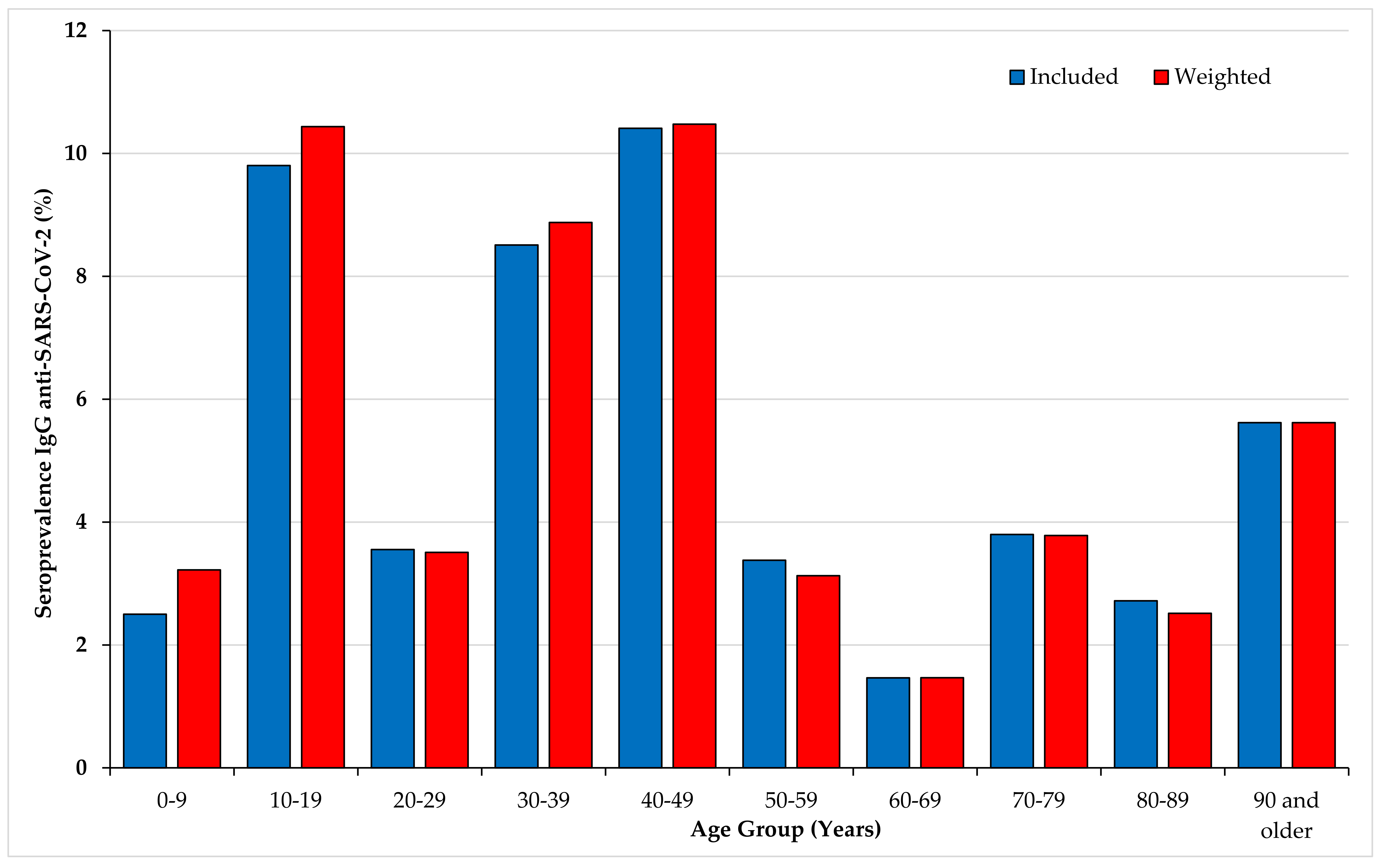
3.1. Seroprevalence Estimated with Results of the EUROIMMUN ELISA IgG Anti-SARS-CoV-2
3.2. Results of VNT Assay
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- Ren, L.-L.; Wang, Y.-M.; Wu, Z.-Q.; Xiang, Z.-C.; Guo, L.; Xu, T.; Jiang, Y.-Z.; Xiong, Y.; Li, Y.-J.; Li, X.-W.; et al. Identification of a novel coronavirus causing severe pneumonia in human: A descriptive study. Chin. Med. J. 2020, 133, 1015–1024. [Google Scholar] [CrossRef]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.; Xu, H.; Rebaza, A.; Sharma, L.; Cruz, C.S.D. Protecting health-care workers from subclinical coronavirus infection. Lancet Respir. Med. 2020, 8, e13. [Google Scholar] [CrossRef]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.-Y.; Chen, L.; Wang, M. Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef]
- Loos, C.; Atyeo, C.; Fischinger, S.; Burke, J.; Slein, M.D.; Streeck, H.; Lauffenburger, D.; Ryan, E.T.; Charles, R.C.; Alter, G. Evolution of Early SARS-CoV-2 and Cross-Coronavirus Immunity. mSphere 2020, 5, 00622-20. [Google Scholar] [CrossRef]
- Li, X.; Wang, W.; Zhao, X.; Zai, J.; Zhao, Q.; Li, Y.; Chaillon, A. Transmission dynamics and evolutionary history of 2019-nCoV. J. Med. Virol. 2020, 92, 501–511. [Google Scholar] [CrossRef]
- WHO Coronavirus Disease (COVID-19) Dashboard. 2020. Available online: https://covid19.who.int (accessed on 4 September 2020).
- Santé Publique France. COVID-19: Point Épidémiologique du 3 September 2020; Santé Publique: Bordeaux, France, 2020. [Google Scholar]
- Salje, H.; Kiem, C.T.; Lefrancq, N.; Courtejoie, N.; Bosetti, P.; Paireau, J.; Andronico, A.; Hozé, N.; Richet, J.; Dubost, C.-L.; et al. Estimating the burden of SARS-CoV-2 in France. Science 2020, 369, 208–211. [Google Scholar] [CrossRef]
- ARS, Agence Régionale de Santé Corse. Point Épidémio Régional Corse Spécial COVID-19 14 mai 2020; ARS: Ajaccio, France, 2020. [Google Scholar]
- Mizumoto, K.; Kagaya, K.; Zarebski, A.; Chowell, G. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020. Eurosurveillance 2020, 25, 2000180. [Google Scholar] [CrossRef]
- INSEE, Institut National de la Statistique et des Études Économiques. Pyramide des Âges 2020—Régions et Départements. 2020. Available online: https://www.insee.fr/fr/statistiques/3696315?p1=rfm&p2=r94&annee=2020 (accessed on 14 January 2020).
- Epitools. Sergent, ESG. Calculateurs Épidémiologiques Epitools. Ausvet. 2018. Available online: https://epitools.ausvet.com.au (accessed on 20 March 2020).
- Beavis, K.G.; Matushek, S.M.; Abeleda, A.P.F.; Bethel, C.; Hunt, C.; Gillen, S.; Moran, A.; Tesic, V. Evaluation of the EUROIMMUN Anti-SARS-CoV-2 ELISA Assay for detection of IgA and IgG antibodies. J. Clin. Virol. 2020, 129, 104468. [Google Scholar] [CrossRef] [PubMed]
- Jääskeläinen, A.J.; Kuivanen, S.; Kekäläinen, E.; Ahava, M.J.; Loginov, R.; Kallio-Kokko, H.; Vapalahti, O.; Jarva, H.; Kurkela, S.; Lappalainen, M. Performance of six SARS-CoV-2 immunoassays in comparison with microneutralisation. J. Clin. Virol. 2020, 129, 104512. [Google Scholar] [CrossRef] [PubMed]
- Kohmer, N.; Westhaus, S.; Rühl, C.; Ciesek, S.; Rabenau, H.F. Clinical performance of different SARS-CoV-2 IgG antibody tests. J. Med. Virol. 2020, 92, 2243–2247. [Google Scholar] [CrossRef] [PubMed]
- Nicol, T.; Lefeuvre, C.; Serri, O.; Pivert, A.; Joubaud, F.; Dubée, V.; Kouatchet, A.; Ducancelle, A.; Lunel-Fabiani, F.; Le Guillou-Guillemette, H. Assessment of SARS-CoV-2 serological tests for the diagnosis of COVID-19 through the evaluation of three immunoassays: Two automated immunoassays (Euroimmun and Abbott) and one rapid lateral flow immunoassay (NG Biotech). J. Clin. Virol. 2020, 129, 104511. [Google Scholar] [CrossRef] [PubMed]
- Jääskeläinen, A.J.; Kekäläinen, E.; Kallio-Kokko, H.; Mannonen, L.; Kortela, E.; Vapalahti, O.; Kurkela, S.; Lappalainen, M. Evaluation of commercial and automated SARS-CoV-2 IgG and IgA ELISAs using coronavirus disease (COVID-19) patient samples. Eurosurveillance 2020, 25, 2000603. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.S.; Hock, K.G.; Logsdon, N.M.; Hayes, J.E.; Gronowski, A.M.; Anderson, N.W.; Farnsworth, C.W. Clinical Performance of Two SARS-CoV-2 Serologic Assays. Clin. Chem. 2020, 66, 1055–1062. [Google Scholar] [CrossRef]
- Gallian, P.; Pastorino, B.; Morel, P.; Chiaroni, J.; Ninove, L.; De Lamballerie, X. Lower prevalence of antibodies neutralizing SARS-CoV-2 in group O French blood donors. Antivir. Res. 2020, 181, 104880. [Google Scholar] [CrossRef]
- Carrat, F.; De Lamballerie, X.; Rahib, D.; Blanche, H.; Lapidus, N.; Artaud, F.; Kab, S.; Renuy, A.; De Edelenyi, F.S.; Meyer, L.; et al. Seroprevalence of SARS-CoV-2 among adults in three regions of France following the lockdown and associated risk factors: A multicohort study. medRxiv 2020. [Google Scholar] [CrossRef]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; De Larrea, N.F.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Havers, F.P.; Reed, C.; Lim, T.; Montgomery, J.M.; Klena, J.D.; Hall, A.J.; Fry, A.M.; Cannon, D.L.; Chiang, C.-F.; Gibbons, A.; et al. Seroprevalence of Antibodies to SARS-CoV-2 in 10 Sites in the United States, March 23-May 12, 2020. JAMA Intern. Med. 2020. [Google Scholar] [CrossRef]
- Xu, X.; Sun, J.; Nie, S.; Li, H.; Kong, Y.; Liang, M.; Hou, J.; Huang, X.; Li, D.; Ma, T.; et al. Seroprevalence of immunoglobulin M and G antibodies against SARS-CoV-2 in China. Nat. Med. 2020, 26, 1193–1195. [Google Scholar] [CrossRef]
- Stringhini, S.; Wisniak, A.; Piumatti, G.; Azman, A.S.; Lauer, S.A.; Baysson, H.; De Ridder, D.; Petrovic, D.; Schrempft, S.; Marcus, K.; et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Geneva, Switzerland (SEROCoV-POP): A population-based study. Lancet 2020, 396, 313–319. [Google Scholar] [CrossRef]
- Vena, A.; Berruti, M.; Adessi, A.; Blumetti, P.; Brignole, M.; Colognato, R.; Gaggioli, G.; Giacobbe, D.R.; Bracci-Laudiero, L.; Magnasco, L.; et al. Prevalence of Antibodies to SARS-CoV-2 in Italian Adults and Associated Risk Factors. J. Clin. Med. 2020, 9, 2780. [Google Scholar] [CrossRef]
- Soriano, V.; Meirino, R.; Corral, O.; Guallar, M.P. SARS-CoV-2 antibodies in adults in Madrid, Spain. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Slot, E.; Hogema, B.M.; Reusken, C.B.; Reimerink, J.H.; Molier, M.; Karregat, J.H.; Ijlst, J.; Novotný, V.M.; Van Lier, R.A.; Zaaijer, H.L. Herd immunity is not a realistic exit strategy during a COVID-19 outbreak. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Gebhard, C.; Regitz-Zagrosek, V.; Neuhauser, H.K.; Morgan, R.; Klein, S.L. Impact of sex and gender on COVID-19 outcomes in Europe. Biol. Sex Differ. 2020, 11, 29. [Google Scholar] [CrossRef]
- Bunyavanich, S.; Do, A.; Vicencio, A. Nasal Gene Expression of Angiotensin-Converting Enzyme 2 in Children and Adults. JAMA 2020, 323, 2427–2429. [Google Scholar] [CrossRef]
- Takahashi, S.; Greenhouse, B.; Rodríguez-Barraquer, I. Are SARS-CoV-2 seroprevalence estimates biased? J. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Krüttgen, A.; Cornelissen, C.G.; Dreher, M.; Hornef, M.; Imöhl, M.; Kleines, M. Comparison of four new commercial serologic assays for determination of SARS-CoV-2 IgG. J. Clin. Virol. 2020, 128, 104394. [Google Scholar] [CrossRef]
- Algaissi, A.; Hashem, A.M. Evaluation of MERS-CoV Neutralizing Antibodies in Sera Using Live Virus Microneutralization Assay. Methods Mol. Biol. 2019, 2099, 107–116. [Google Scholar]
- Wu, F.; Wang, A.; Liu, M.; Wang, Q.; Chen, J.; Xia, S.; Ling, Y.; Zhang, Y.; Xun, J.; Lu, L.; et al. Neutralizing Antibody Responses to SARS-CoV-2 in a COVID-19 Recovered Patient Cohort and Their Implications. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Perreault, J.; Tremblay, T.; Fournier, M.J.; Drouin, M.; Beaudoin-Bussières, G.; Prévost, J.; Lewin, A.; Bégin, P.; Finzi, A.; Bazin, R. Waning of SARS-CoV-2 RBD antibodies in longitudinal convalescent plasma samples within four months after symptom onset. Blood 2020. [Google Scholar] [CrossRef]
- Choe, P.G.; Kang, C.K.; Suh, H.J.; Jung, J.; Song, K.-H.; Bang, J.H.; Kim, E.S.; Bin Kim, H.; Park, S.W.; Kim, N.J.; et al. Waning Antibody Responses in Asymptomatic and Symptomatic SARS-CoV-2 Infection. Emerg. Infect. Dis. 2021, 27. [Google Scholar] [CrossRef]
- Robbiani, D.F.; Gaebler, C.; Muecksch, F.; Lorenzi, J.C.C.; Wang, Z.; Cho, A.; Agudelo, M.; Barnes, C.O.; Gazumyan, A.; Finkin, S.; et al. Convergent antibody responses to SARS-CoV-2 in convalescent individuals. Nat. Cell Biol. 2020, 584, 437–442. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Items | Included Population | Weighted Population | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All (n) | EUROIMMUN IgG SARS-CoV-2 Positives | OR [95% CI] | p-Value | All (n) | Weighted Seroprevalences | OR [95%CI] | p-Value | ||||||
| n Positive | SARS-CoV-2 IgG+ (%) | [95% CI] | n Positives | Seroprevalence (%) | [95% CI] | ||||||||
| Overall | 1973 | 104 | 5.27 | [4.33–6.35] | 1973 | 107.66 | 5.46 | [4.37–7.00] | |||||
| Sex | Women | 1187 | 66 | 5.56 | [4.33–7.02] | 0.86 [0.57–1.29] | 0.48 | 1017.35 | 58.41 | 5.74 | [4.31–7.17] | 0.89 [0.56–1.42] | 0.63 |
| Men | 786 | 38 | 4.83 | [3.44–6.58] | 955.48 | 49.25 | 5.15 | [3.75–6.56] | |||||
| Age (years) | 0–9 | 40 | 1 | 2.50 | [0.063–13.16] | 0.73 [0.04–3.99] | < 0.0001 * | 193.05 | 6.22 | 3.22 | [0.73–5.71] | 1.03 [0.13–8.36] | 0.97 |
| 10–19 | 153 | 15 | 9.80 | [5.59–15.65] | 3.11 [1.38–7.32] * | 199.79 | 20.85 | 10.44 | [6.20–14.68] | 3.62 [1.54–8.53] * | 0.0033 * | ||
| 20–29 | 197 | 7 | 3.55 | [1.44–7.18] | 1.05 [0.38–2.79] | 191.59 | 6.72 | 3.51 | [0.90–6.10] | 1.13 [0.40–3.19] | 0.82 | ||
| 30–39 | 235 | 20 | 8.51 | [5.27–12.84] | 2.66 [1.25–6.04] * | 249.66 | 22.16 | 8.88 | [5.35–12.40] | 3.01 [1.35–6.69] * | 0.0069 * | ||
| 40–49 | 269 | 28 | 10.41 | [7.03–14.69] | 3.32 [1.63–7.32] * | 258.47 | 27.08 | 10.48 | [6.74–14.21] | 3.62 [1.71–7.68] * | 0.00079 * | ||
| 50–59 | 296 | 10 | 3.38 | [1.63–6.12] | reference | 274.30 | 8.58 | 3.13 | [1.07–5.19] | reference | |||
| 60–69 | 273 | 4 | 1.47 | [0.40–3.71] | 0.43 [0.12–1.29] | 257.60 | 3.78 | 1.47 | [0.00–2.94] | 0.46 [0.14–1.50] | 0.20 | ||
| 70–79 | 237 | 9 | 3.80 | [1.75–7.09] | 1.13 [0.44–2.85] | 209.46 | 7.92 | 3.78 | [1.20–6.36] | 1.21 [0.48–3.05] | 0.68 | ||
| 80–89 | 184 | 5 | 2.72 | [0.89–6.23] | 0.80 [0.25–2.29] | 111.32 | 2.80 | 2.52 | [0.00–5.42] | 0.79 [0.26–2.36] | 0.68 | ||
| 90 and older | 89 | 5 | 5.62 | [1.85–12.62] | 1.70 [0.52–4.93] | 27.59 | 1.55 | 5.62 | [0.00–14.21] | 1.80 [0.59–5.49] | 0.30 | ||
| VNT Titer | Number of Samples | % | VNT Interpretation n (%) |
|---|---|---|---|
| Negative at titer 20 | 67 | 47.9 | Beside the cut-off (titer 40) 81 (58.0%) |
| 20 | 14 | 10.0 | |
| 40 | 24 | 17.1 | 59 (42.0%) |
| 80 | 9 | 6.4 | |
| 160 | 26 | 18.6 | |
| Total | 140 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capai, L.; Ayhan, N.; Masse, S.; Canarelli, J.; Priet, S.; Simeoni, M.-H.; Charrel, R.; de Lamballerie, X.; Falchi, A. Seroprevalence of SARS-CoV-2 IgG Antibodies in Corsica (France), April and June 2020. J. Clin. Med. 2020, 9, 3569. https://doi.org/10.3390/jcm9113569
Capai L, Ayhan N, Masse S, Canarelli J, Priet S, Simeoni M-H, Charrel R, de Lamballerie X, Falchi A. Seroprevalence of SARS-CoV-2 IgG Antibodies in Corsica (France), April and June 2020. Journal of Clinical Medicine. 2020; 9(11):3569. https://doi.org/10.3390/jcm9113569
Chicago/Turabian StyleCapai, Lisandru, Nazli Ayhan, Shirley Masse, Jean Canarelli, Stéphane Priet, Marie-Hélène Simeoni, Remi Charrel, Xavier de Lamballerie, and Alessandra Falchi. 2020. "Seroprevalence of SARS-CoV-2 IgG Antibodies in Corsica (France), April and June 2020" Journal of Clinical Medicine 9, no. 11: 3569. https://doi.org/10.3390/jcm9113569
APA StyleCapai, L., Ayhan, N., Masse, S., Canarelli, J., Priet, S., Simeoni, M.-H., Charrel, R., de Lamballerie, X., & Falchi, A. (2020). Seroprevalence of SARS-CoV-2 IgG Antibodies in Corsica (France), April and June 2020. Journal of Clinical Medicine, 9(11), 3569. https://doi.org/10.3390/jcm9113569