The Role of Positive Psychological Factors in the Association between Pain Intensity and Pain Interference in Individuals with Chronic Musculoskeletal Pain: A Cross-Sectional Study



 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Setting
2.3. Eligibility Criteria
2.4. Sample Size Calculation
2.5. Measures
2.6. Statistical Analysis
3. Results
3.1. Baseline Demographic and Clinical Characteristics
3.2. Univariate Associations between Psychological Measures, Pain Intensity, and Pain Interference
3.3. Linear Regression Model
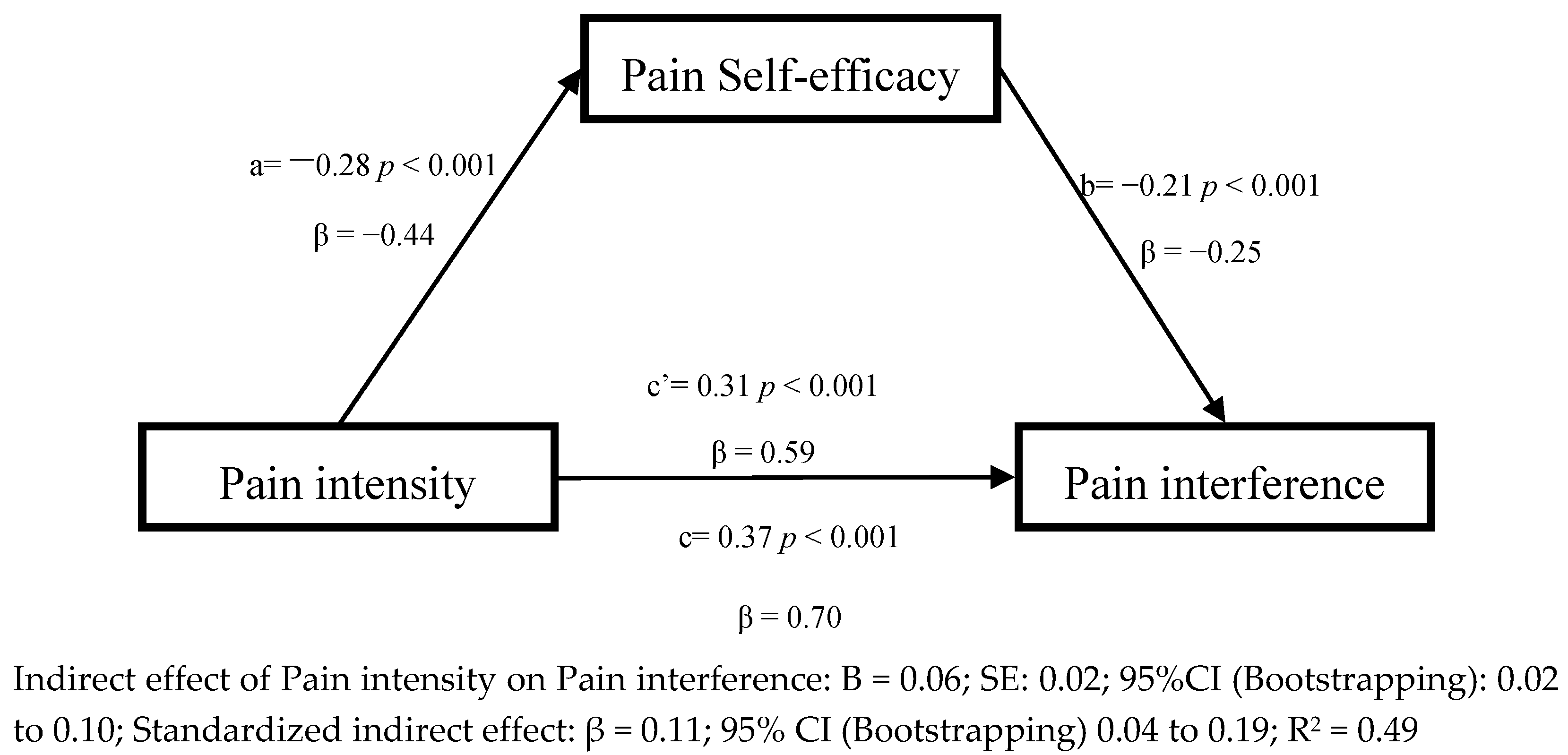
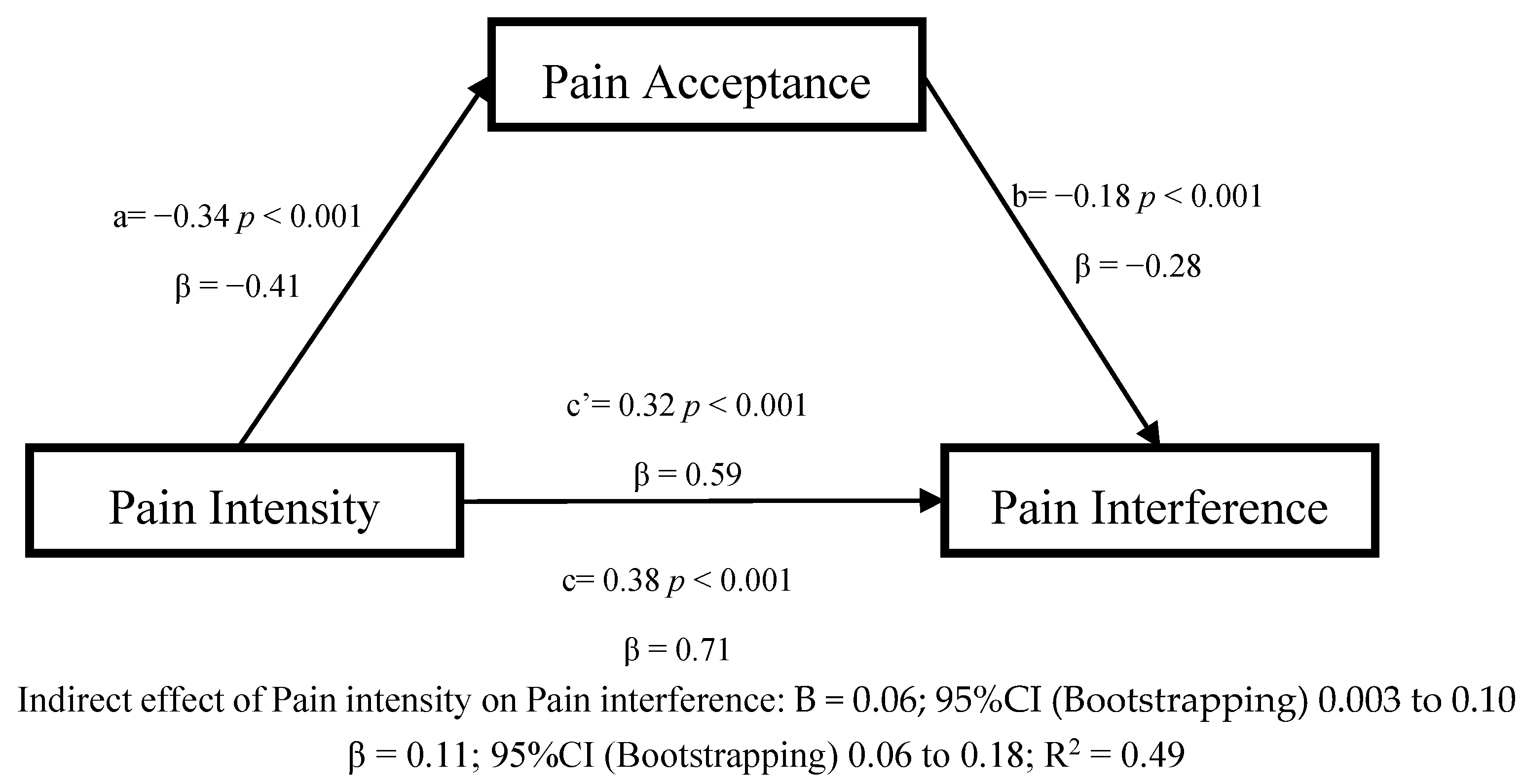
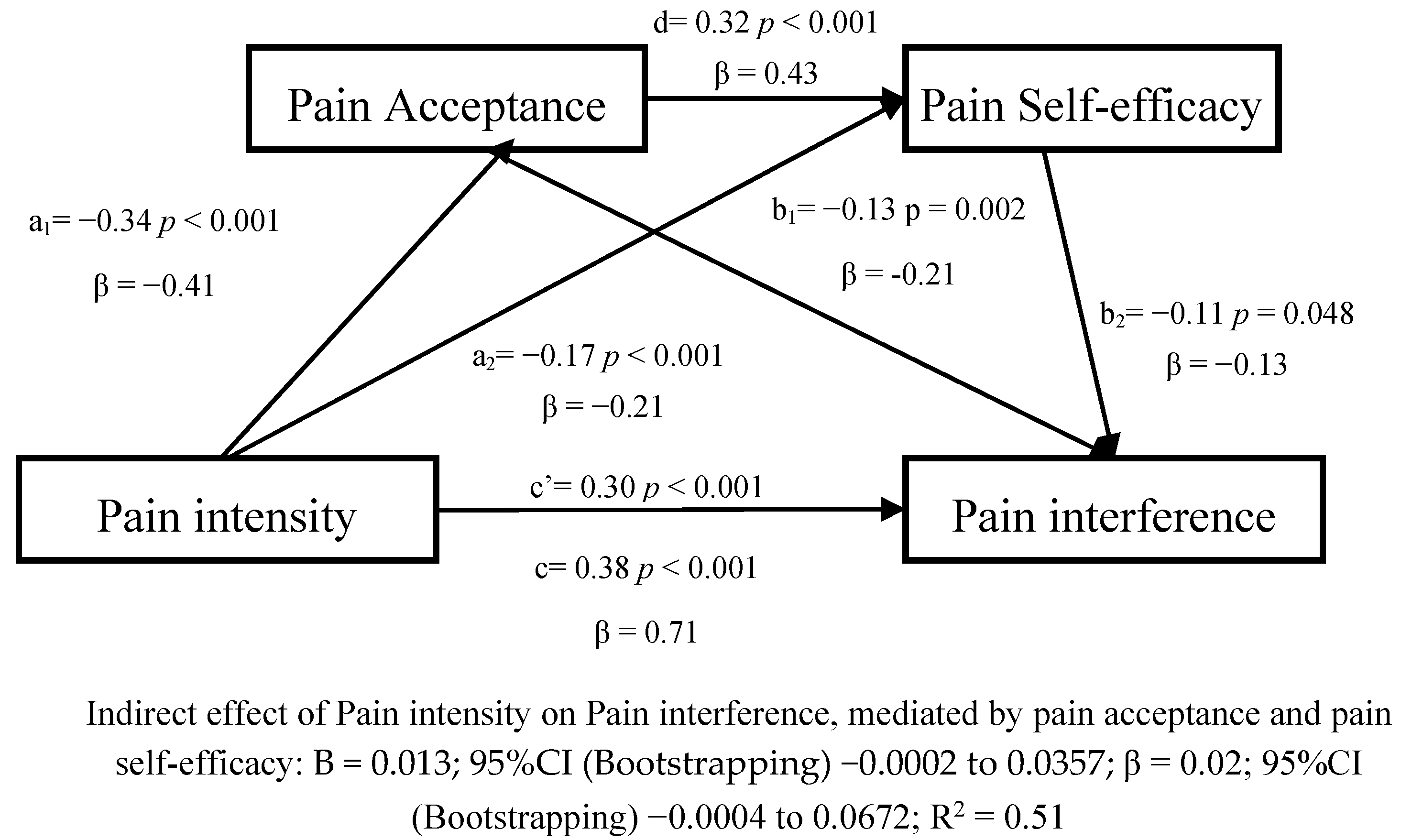
3.4. Cross-Sectional Mediating Effects of Pain Self-Efficacy and Pain Acceptance
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Briggs, A.M.; Woolf, A.D.; Dreinhöfer, K.; Homb, N.; Hoy, D.G.; Kopansky-Giles, D.Å.; Akesson, K.; March, L. Reducing the global burden of musculoskeletal conditions. Bull. World Health Organ. 2018, 96, 366–368. [Google Scholar] [CrossRef] [PubMed]
- GBD 2016 DALYs and HALE Collaborators. Global, regional, and national disabilityadjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1260–1344. [Google Scholar] [CrossRef]
- Schofield, D.J.; Shrestha, R.N.; Cunich, M.; Tanton, R.; Kelly, S.; Passey, M.E.; Veerman, L.J. Lost productive life years caused by chronic conditions in australians aged 45–l64 years, 2010–2030. Med. J. Aust. 2015, 203, 260.e1–260.e6. [Google Scholar] [CrossRef] [PubMed]
- Hsu, E.S. Medication Overuse in Chronic Pain. Curr. Pain Headache Rep. 2017, 21, 2. [Google Scholar] [CrossRef]
- Dueñas, M.; Ojeda, B.; Salazar, A.; Mico, J.A.; Failde, I. A review of chronic pain impact on patients, their social environment and the health care system. J. Pain Res. 2016, 9, 457–467. [Google Scholar] [CrossRef]
- Smith, T.O.; Dainty, J.R.; Williamson, E.; Martin, K.R. Association between musculoskeletal pain with social isolation and loneliness: Analysis of the English Longitudinal Study of Ageing. Br. J. Pain 2018, 13, 82–90. [Google Scholar] [CrossRef]
- Briggs, A.M.; Cross, M.J.; Hoy, D.G.; Sànchez-Riera, L.; Blyth, F.M.; Woolf, A.D.; March, L. Musculoskeletal Health Conditions Represent a Global Threat to Healthy Aging: A Report for the 2015 World Health Organization World Report on Ageing and Health. Gerontologist 2016, 56, S243–S255. [Google Scholar] [CrossRef]
- Crofford, L.J. Psychological aspects of chronic musculoskeletal pain. Best Pract. Res. Clin. Rheumatol. 2015, 29, 147–155. [Google Scholar] [CrossRef]
- Leeuw, M.; Goossens, M.E.J.B.; Linton, S.J.; Crombez, G.; Boersma, K.; Vlaeyen, J.W.S. The fear-avoidance model of musculoskeletal pain: Current state of scientific evidence. J. Behav. Med. 2007, 30, 77–94. [Google Scholar] [CrossRef]
- Gatchel, R.J.; Peng, Y.B.; Peters, M.L.; Fuchs, P.N.; Turk, D.C. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol. Bull. 2007, 133, 581–624. [Google Scholar] [CrossRef]
- Edwards, R.R.; Dworkin, R.H.; Sullivan, M.D.; Turk, D.C.; Wasan, A.D. The Role of Psychosocial Processes in the Development and Maintenance of Chronic Pain. J. Pain 2016, 17, T70–T92. [Google Scholar] [CrossRef]
- Denk, F.; McMahon, S.B.; Tracey, I. Pain vulnerability: A neurobiological perspective. Nat. Neurosci. 2014, 17, 192–200. [Google Scholar] [CrossRef]
- Che, X.; Cash, R.; Ng, S.K.; Fitzgerald, P.; Fitzgibbon, B.M. A Systematic Review of the Processes Underlying the Main and the Buffering Effect of Social Support on the Experience of Pain. Clin. J. Pain 2018, 34, 1061–1076. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Calderon, J.; Flores-Cortes, M.; Morales-Asencio, J.M.; Luque-Suarez, A. Pain-Related Fear, Pain Intensity and Function in Individuals with Chronic Musculoskeletal Pain: A Systematic Review and Meta-Analysis. J. Pain 2019, 20, 1394–1415. [Google Scholar] [CrossRef]
- McCracken, L.M.; Vowles, K.E. Acceptance of chronic pain. Curr. Pain Headache Rep. 2006, 10, 90–94. [Google Scholar] [CrossRef]
- Martinez-Calderon, J.; Jensen, M.P.; Morales-Asencio, J.M.; Luque-Suarez, A. Pain Catastrophizing and Function in Individuals with Chronic Musculoskeletal Pain. Clin. J. Pain 2019, 35, 279–293. [Google Scholar] [CrossRef]
- Sturgeon, J.A.; Zautra, A.J. Resilience: A new paradigm for adaptation to chronic pain. Curr. Pain Headache Rep. 2010, 14, 105–112. [Google Scholar] [CrossRef]
- McCracken, L.M.; Morley, S. The psychological flexibility model: A basis for integration and progress in psychological approaches to chronic pain management. J. Pain 2014, 15, 221–234. [Google Scholar] [CrossRef]
- Basten-Günther, J.; Peters, M.; Lautenbacher, S. Optimism and the Experience of Pain: A Systematic Review. Behav. Med. 2019, 45, 323–339. [Google Scholar] [CrossRef] [PubMed]
- Jackson, T.; Wang, Y.; Wang, Y.; Fan, H. Self-efficacy and chronic pain outcomes: A meta-analytic review. J. Pain 2014, 15, 800–814. [Google Scholar] [CrossRef]
- Finan, P.H.; Garland, E.L. The Role of Positive Affect in Pain and Its Treatment. Clin. J. Pain 2015, 31, 177–187. [Google Scholar] [CrossRef]
- Martinez-Calderon, J.; Zamora-Campos, C.; Navarro-Ledesma, S.; Luque-Suarez, A. The Role of Self-Efficacy on the Prognosis of Chronic Musculoskeletal Pain: A Systematic Review. J. Pain 2018, 19, 10–34. [Google Scholar] [CrossRef] [PubMed]
- Reneman, M.F.; Dijkstra, A.; Geertzen, J.H.B.; Dijkstra, P.U. Psychometric properties of Chronic Pain Acceptance Questionnaires: A systematic review. Eur. J. Pain 2010, 14, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, M.K. The pain self-efficacy questionnaire: Taking pain into account. Eur. J. Pain 2007, 11, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Scheier, M.F.; Carver, C.S.; Bridges, M.W. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): A reevaluation of the Life Orientation Test. J. Pers. Soc. Psychol. 1994, 67, 1063–1078. [Google Scholar] [CrossRef]
- Turner, J.A.; Ersek, M.; Kemp, C. Self-efficacy for managing pain is associated with disability, depression, and pain coping among retirement community residents with chronic pain. J. Pain 2005, 6, 471–479. [Google Scholar] [CrossRef]
- Ramírez-Maestre, C.; Esteve, R.; López, A.E. The Role of Optimism and Pessimism in Chronic Pain Patients Adjustment. Span J. Psychol. 2012, 15, 286–294. [Google Scholar] [CrossRef]
- McCracken, L.M.; Eccleston, C. Coping or acceptance: What to do about chronic pain? Pain 2003, 105, 197–204. [Google Scholar] [CrossRef]
- Kratz, A.L.; Murphy, J.; Kalpakjian, C.Z.; Chen, P. Medicate or Meditate? Greater Pain Acceptance is Related to Lower Pain Medication Use in Persons with Chronic Pain and Spinal Cord Injury. Clin. J. Pain 2018, 34, 357–365. [Google Scholar] [CrossRef]
- Ramírez-Maestre, C.; Esteve, R.; López-Martínez, A.E.; Serrano-Ibáñez, E.R.; Ruiz-Párraga, G.T.; Peters, M. Goal Adjustment and Well-Being: The Role of Optimism in Patients with Chronic Pain. Ann. Behav. Med. 2019, 53, 597–607. [Google Scholar] [CrossRef]
- Wright, M.A.; Wren, A.A.; Somers, T.J.; Goetz, M.C.; Fras, A.M.; Huh, B.K.; Rogers, L.L.; Keefe, F.J. Pain acceptance, hope, and optimism: Relationships to pain and adjustment in patients with chronic musculoskeletal pain. J. Pain 2011, 12, 1155–1162. [Google Scholar] [CrossRef]
- Thompson, E.; Broadbent, J.; Bertino, M.D.; Staiger, P.K. Do Pain-related Beliefs Influence Treatment adherence? A Systematic Review. Clin. J. Pain 2015, 32, 1. [Google Scholar]
- Esteve, R.; López-Martínez, A.E.; Peters, M.L.; Serrano-Ibáñez, E.R.; Ruiz-Párraga, G.T.; Ramírez-Maestre, C. Optimism, Positive and Negative Affect, and Goal Adjustment Strategies: Their Relationship to Activity Patterns in Patients with Chronic Musculoskeletal Pain. Pain Res. Manag. 2018, 2018, 6291719. [Google Scholar] [CrossRef] [PubMed]
- Peñacoba Puente, C.; Velasco Furlong, L.; Écija Gallardo, C.; Cigarán Méndez, M.; Bedmar Cruz, D.; Fernández-de-las-Peñas, C. Self-Efficacy and Affect as Mediators Between Pain Dimensions and Emotional Symptoms and Functional Limitation in Women with Fibromyalgia. Pain Manag. Nurs. 2015, 16, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Ahlstrand, I.; Vaz, S.; Falkmer, T.; Thyberg, I.; Björk, M. Self-efficacy and pain acceptance as mediators of the relationship between pain and performance of valued life activities in women and men with rheumatoid arthritis. Clin. Rehabil. 2017, 31, 824–834. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, S.A.; Gillanders, D.; Palmeira, L.; Pinto-Gouveia, J.; Castilho, P. Mindfulness, selfcompassion, and depressive symptoms in chronic pain: The role of pain acceptance. J. Clin. Psychol. 2018, 74, 2094–2106. [Google Scholar] [CrossRef]
- Costa Lda, C.; Maher, C.G.; McAuley, J.H.; Hancock, M.J.; Smeets, R.J. Self-efficacy is more important than fear of movement in mediating the relationship between pain and disability in chronic low back pain. Eur. J. Pain 2011, 15, 213–219. [Google Scholar] [CrossRef]
- Skidmore, J.R.; Koenig, A.L.; Dyson, S.J.; Kupper, A.E.; Garner, M.J.; Keller, C.J. Pain self-efficacy mediates the relationship between depressive symptoms and pain severity. Clin. J. Pain 2015, 31, 137–144. [Google Scholar] [CrossRef]
- Cederberg, J.T.; Cernvall, M.; Dahl, J.A.; von Essen, L.; Ljungman, G. Acceptance as a Mediator for Change in Acceptance and Commitment Therapy for Persons with Chronic Pain? Int. J. Behav. Med. 2016, 23, 21–29. [Google Scholar] [CrossRef]
- Day, M.A.; Thorn, B.E. The mediating role of pain acceptance during mindfulness-based cognitive therapy for headache. Complement. Ther. Med. 2016, 25, 51–54. [Google Scholar] [CrossRef]
- Luciano, J.V.; Guallar, J.A.; Aguado, J.; López-Del-Hoyo, Y.; Olivan, B.; Magallón, R.; Alda, M.; Antoni Serrano-Blanco, A.; Gili, M.; Garcia-Campayo, J.; et al. Effectiveness of group acceptance and commitment therapy for fibromyalgia: A 6-month randomized controlled trial (EFFIGACT study). Pain 2014, 155, 693–702. [Google Scholar] [CrossRef]
- Åkerblom, S.; Perrin, S.; Rivano Fischer, M.; McCracken, L.M. The Mediating Role of Acceptance in Multidisciplinary Cognitive-Behavioral Therapy for Chronic Pain. J. Pain 2015, 16, 606–615. [Google Scholar] [CrossRef]
- Bernardes, S.F.; Forgeron, P.; Fournier, K.; Reszel, J. Beyond solicitousness: A comprehensive review on informal pain-related social support. Pain 2017, 158, 2066–2076. [Google Scholar] [CrossRef]
- STROBE. STROBE Statement—Checklist of Items That Should Be Included in Reports of Cross-Sectional Studies. Available online: https://www.strobe-statement.org/fileadmin/Strobe/uploads/checklists/STROBE_checklist_v4_combined.pdf (accessed on 12 October 2020).
- Dworkin, R.H.; Bruehl, S.; Fillingim, R.B.; Loeser, J.D.; Terman, G.W.; Turk, D.C. Multidimensional Diagnostic Criteria for Chronic Pain: Introduction to the ACTTION-American Pain Society Pain Taxonomy (AAPT). J. Pain 2016, 17 (Suppl. 9), T1–T9. [Google Scholar] [CrossRef]
- Ferrer-Peña, R.; Gil-Martínez, A.; Pardo-Montero, J.; Jiménez-Penick, V.; Gallego-Izquierdo, T.; La Touche, R. Adaptación y validación de la Escala de gradación del dolor crónico al español. Reumatol. Clínica 2016, 12, 130–138. [Google Scholar] [CrossRef]
- Von Korff, M.; Ormel, J.; Keefe, F.J.D.S. Grading the severity of chronic pain. Pain 1992, 50, 133–149. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale. Arthritis Care Res. 2011, 63 (Suppl. 1), S240–S252. [Google Scholar] [CrossRef]
- Rodero, B.; García-Campayo, J.; Casanueva, B.; del Hoyo, Y.L.; Serrano-Blanco, A.; Luciano, J.V. Validation of the Spanish version of the Chronic Pain Acceptance Questionnaire (CPAQ) for the assessment of acceptance in fibromyalgia. Health Qual. Life Outcomes 2010, 8, 37. [Google Scholar] [CrossRef]
- McCracken, L.M.; Vowles, K.E.; Eccleston, C. Acceptance of chronic pain: Component analysis and a revised assessment method. Pain 2004, 107, 159–166. [Google Scholar] [CrossRef]
- Ferrando, P.J.; Chico, E.; Tous, M. Propiedades psicométricas del test de optimismo Life Orientation Test. Psicothema 2002, 14, 673–680. [Google Scholar]
- Cano-García, F.J.; Sanduvete-Chaves, S.; Chacón-Moscoso, S.; Rodríguez-Franco, L.; García-Martínez, J.; Antuña-Bellerín, M.A.; Pérez-Gil, J.A. Factor structure of the Spanish version of the Life Orientation Test-Revised (LOT-R): Testing several models. Int. J. Clin. Health Psychol. 2015, 15, 139–148. [Google Scholar] [CrossRef]
- Dancey, C.P.; Reidy, J. Statistics without Maths for Psychology, 4th ed.; Pearson Education: London, UK, 2008. [Google Scholar]
- Akinwande, M.O.; Dikko, H.G.; Samson, A. Variance Inflation Factor: As a Condition for the Inclusion of Suppressor Variable(s) in Regression Analysis. Open J. Stat. 2015, 5, 754–767. [Google Scholar] [CrossRef]
- O’Laughlin, K.D.; Martin, M.J.; Ferrer, E. Cross-Sectional Analysis of Longitudinal Mediation Processes. Multivar. Behav. Res. 2018, 53, 375–402. [Google Scholar] [CrossRef]
- Hayes, A.F. Beyond Baron and Kenny: Statistical Mediation Analysis in the New Millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Hayes, A.F. Part II: Mediation analysis. In Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Publications: New York, NY, USA, 2017; pp. 75–217. [Google Scholar]
- Craner, J.R.; Sperry, J.A.; Koball, A.M.; Morrison, E.J.; Gilliam, W.P. Unique Contributions of Acceptance and Catastrophizing on Chronic Pain Adaptation. Int. J. Behav. Med. 2017, 24, 542–551. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M. Learning to live with the pain: Acceptance of pain predicts adjustment in persons with chronic pain. Pain 1998, 74, 21–27. [Google Scholar] [CrossRef]
- Cousins, L.A.; Kalapurakkel, S.; Cohen, L.L.; Simons, L.E. Topical Review: Resilience Resources and Mechanisms in Pediatric Chronic Pain. J. Pediatr. Psychol. 2015, 40, 840–845. [Google Scholar] [CrossRef]
- Hassett, A.L.; Finan, P.H. The Role of Resilience in the Clinical Management of Chronic Pain. Curr. Pain Headache Rep. 2016, 20, 39. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Barker, E.; Chilcot, J. Decentering, rumination, cognitive defusion, and psychological flexibility in people with chronic pain. J. Behav. Med. 2014, 37, 1215–1225. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.S.; Clark, J.; Colclough, J.A.; Dale, E.; McMillan, D. Acceptance and Commitment Therapy (ACT) for Chronic Pain. Clin. J. Pain 2017, 33, 552–568. [Google Scholar] [CrossRef] [PubMed]
- Gentili, C.; Rickardsson, J.; Zetterqvist, V.; Simons, L.E.; Lekander, M.; Wicksell, R.K. Psychological Flexibility as a Resilience Factor in Individuals with Chronic Pain. Front. Psychol. 2019, 10, 2016. [Google Scholar] [CrossRef]
- Marshall, P.W.M.; Schabrun, S.; Knox, M.F. Physical activity and the mediating effect of fear, depression, anxiety, and catastrophizing on pain related disability in people with chronic low back pain. PLoS ONE 2017, 12, e0180788. [Google Scholar] [CrossRef]
- Wicksell, R.K.; Olsson, G.L.; Hayes, S.C. Psychological flexibility as a mediator of improvement in Acceptance and Commitment Therapy for patients with chronic pain following whiplash. Eur. J. Pain 2010, 14, 1059.e1–1059.e11. [Google Scholar] [CrossRef]
- Pulido-Martos, M.; Luque-Reca, O.; Segura-Jiménez, V.; Álvarez-Gallardo, I.C.; Soriano-Maldonado, A.; Acosta-Manzano, P.; Gavilán-Carrera, B.; McVeigh, J.G.; Geenen, R.; Delgado-Fernández, M.; et al. Physical and psychological paths toward less severe fibromyalgia: A structural equation model. Ann. Phys. Rehabil. Med. 2020, 63, 46–52. [Google Scholar] [CrossRef]
- Écija, C.; Luque-Reca, O.; Suso-Ribera, C.; Catala, P.; Peñacoba, C. Associations of Cognitive Fusion and Pain Catastrophizing with Fibromyalgia Impact through Fatigue, Pain Severity, and Depression: An Exploratory Study Using Structural Equation Modeling. J. Clin. Med. 2020, 9, 1763. [Google Scholar] [CrossRef]
- Deodhar, A.; Gensler, L.S.; Magrey, M.; Walsh, J.A.; Winseck, A.; Grant, D.; Mease, P.J. Assessing Physical Activity and Sleep in Axial Spondyloarthritis: Measuring the Gap. Rheumatol. Ther. 2019, 6, 487–501. [Google Scholar] [CrossRef] [PubMed]
- Luque-Reca, O.; Pulido-Martos, M.; Gavilán-Carrera, B.; García-Rodríguez, I.C.; McVeigh, J.G.; Aparicio, V.A.; Estévez-López, F. Emotional intelligence impairments in women with fibromyalgia: Associations with widespread pain. J. Health Psychol. 2019, 1359105319890916. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Mean (SD) or Number (%) |
|---|---|
| Age in years (n = 186) | 52.7 (10.6) |
| Gender (n = 186) | |
| Female | 133 (71.5%) |
| Male | 53 (28.5%) |
| Duration of symptoms (n = 186) | |
| 2–6 months | 12 (6.5%) |
| 6–12 months | 12 (6.5%) |
| >12 months | 162 (87.1%) |
| Pain site (n = 183) | |
| Low back | 78 (42.6%) |
| Neck | 41 (22.4%) |
| Shoulder | 43 (23.5%) |
| Knee/hip | 11 (6.0%) |
| Other sites | 10 (5.5%) |
| Employment status (n = 184) | |
| Employed | 73 (39.7%) |
| Unemployed | 28 (15.2%) |
| On sick leave | 14 (7.6%) |
| Retired | 30 (16.3%) |
| Homemaker | 39 (21.2%) |
| Educational level (n = 184) | |
| No formal education | 8 (4.3%) |
| Primary school | 50 (27.2%) |
| Secondary school | 72 (39.1%) |
| Bachelor’s degree, | 47 (25.5%) |
| Masters and/or PhD | 7 (3.8%) |
| Primary treatment received (n = 186) | |
| No treatment | 41 (22.0%) |
| Pharmacological treatment | 18 (9.7%) |
| Physiotherapy | 117 (62.9%) |
| Other treatment (e.g., acupuncture) | 8 (4.3%) |
| Presence of comorbidities (n = 186) | |
| Yes | 103 (55.5%) |
| No | 81 (43.5%) |
| Pain intensity (GCPS pain subscale score: 0–30, n = 161) | 17.3 (SD, 6.7) [min 0 to max 30] |
| Pain interference (GCPS pain interference subscale score: 0–30 n = 160) | 17.5 (SD, 12.1) [min 0 to max 40] |
| Pain self-efficacy (PSEQ score: 0–60, n = 180) | 37.6 (SD, 14.6) [min 2 to max 60] |
| Optimism (LOT-R score: 0–40, n = 160) | 15.8 (SD, 4.2) [min 4 to max 24] |
| Pain acceptance (CPAQ total score: 0–120, n= 153) | 62.6 (SD, 19.2) [min 15 to max 114] |
| Pain Intensity (GCPS) | Pain Interference (GCPS) | Pain Self-Efficacy (PSEQ) | Optimism (LOT-R) | |
|---|---|---|---|---|
| Pain interference (GCPS) | 0.71 * | - | - | - |
| Pain self-efficacy (PSEQ) | −0.44 * | −0.50 * | - | - |
| Optimism (LOT-R) | −0.13 | −0.08 | 0.28 * | - |
| Pain acceptance (CPAQ) | −0.40 * | −0.51 * | 0.54 * | 0.41 * |
| 95% CI | |||||||
|---|---|---|---|---|---|---|---|
| Model (R2) | β | p | LCI | UCI | Tolerance | VIF | |
| 1 (0.50) | (Constant) | <0.001 | 8.99 | 23.47 | |||
| Pain intensity | 0.71 | <0.001 | 1.06 | 1.48 | |||
| 2 (0.59) | (Constant) | <0.001 | 10.17 | 23.56 | |||
| Pain intensity | 0.56 | <0.001 | 0.78 | 1.21 | 0.75 | 1.32 | |
| Pain self-efficacy | −0.14 | 0.026 | −0.23 | −0.01 | 0.64 | 1.56 | |
| Pain acceptance | −0.28 | <0.001 | −0.26 | −0.08 | 0.59 | 1.67 | |
| Optimism | 0.14 | 0.015 | 0.07 | 0.76 | 0.82 | 1.22 | |
| 3 (0.60) | Pain intensity * Pain Self-Efficacy | −0.04 | 0.538 | −0.02 | 0.01 | 0.64 | 1.15 |
| Pain intensity * Pain Acceptance | −0.06 | 0.407 | −0.02 | 0.01 | 0.56 | 1.78 | |
| Pain intensity * Optimism | 0.01 | 0.825 | −0.04 | 0.06 | 0.74 | 1.35 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez-Calderon, J.; Flores-Cortes, M.; Clavero-Cano, S.; Morales-Asencio, J.M.; Jensen, M.P.; Rondon-Ramos, A.; Diaz-Cerrillo, J.L.; Ariza-Hurtado, G.R.; Luque-Suarez, A. The Role of Positive Psychological Factors in the Association between Pain Intensity and Pain Interference in Individuals with Chronic Musculoskeletal Pain: A Cross-Sectional Study. J. Clin. Med. 2020, 9, 3252. https://doi.org/10.3390/jcm9103252
Martinez-Calderon J, Flores-Cortes M, Clavero-Cano S, Morales-Asencio JM, Jensen MP, Rondon-Ramos A, Diaz-Cerrillo JL, Ariza-Hurtado GR, Luque-Suarez A. The Role of Positive Psychological Factors in the Association between Pain Intensity and Pain Interference in Individuals with Chronic Musculoskeletal Pain: A Cross-Sectional Study. Journal of Clinical Medicine. 2020; 9(10):3252. https://doi.org/10.3390/jcm9103252
Chicago/Turabian StyleMartinez-Calderon, Javier, Mar Flores-Cortes, Susana Clavero-Cano, Jose Miguel Morales-Asencio, Mark P. Jensen, Antonio Rondon-Ramos, Juan Luis Diaz-Cerrillo, Gina Rocío Ariza-Hurtado, and Alejandro Luque-Suarez. 2020. "The Role of Positive Psychological Factors in the Association between Pain Intensity and Pain Interference in Individuals with Chronic Musculoskeletal Pain: A Cross-Sectional Study" Journal of Clinical Medicine 9, no. 10: 3252. https://doi.org/10.3390/jcm9103252
APA StyleMartinez-Calderon, J., Flores-Cortes, M., Clavero-Cano, S., Morales-Asencio, J. M., Jensen, M. P., Rondon-Ramos, A., Diaz-Cerrillo, J. L., Ariza-Hurtado, G. R., & Luque-Suarez, A. (2020). The Role of Positive Psychological Factors in the Association between Pain Intensity and Pain Interference in Individuals with Chronic Musculoskeletal Pain: A Cross-Sectional Study. Journal of Clinical Medicine, 9(10), 3252. https://doi.org/10.3390/jcm9103252