Predictors for Target Vessel Failure after Recanalization of Chronic Total Occlusions in Patients Undergoing Surveillance Coronary Angiography

 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Methods
- (1)
- Re-occlusion: Defined as TIMI flow grade 0, as assessed by fluoroscopy of the treated vessel at the timepoint of surveillance coronary angiography.
- (2)
- Restenosis: Defined as the recurrence of lumen loss >50% in the CTO vessel as quantified retrospectively by QCA (including re-occlusion).
- (3)
- Target vessel failure (TVF): Defined as a combined endpoint by the presence of re-occlusion, restenosis, or target vessel revascularization (defined as a necessity for a repeated PCI within the former CTO vessel).
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Strauss, B.H.; Shuvy, M.; Wijeysundera, H.C. Revascularization of Chronic Total Occlusions. J. Am. Coll. Cardiol. 2014, 64, 1281–1289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fefer, P.; Knudtson, M.L.; Cheema, A.N.; Galbraith, P.D.; Osherov, A.B.; Yalonetsky, S.; Gannot, S.; Samuel, M.; Weisbrod, M.; Bierstone, D.; et al. Current perspectives on coronary chronic total occlusions: The Canadian Multicenter Chronic Total Occlusions Registry. J. Am. Coll. Cardiol. 2012, 59, 991–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathore, S.; Matsuo, H.; Terashima, M.; Kinoshita, Y.; Kimura, M.; Tsuchikane, E.; Nasu, K.; Ehara, M.; Asakura, Y.; Katho, O.; et al. Procedural and in-hospital outcomes after percutaneous coronary interventions for chronic total occlusion of coronary arteries 2002 to 2008: Impact of novel guidewire techniques. J. Am. Coll. Cardiol. Intv. 2009, 2, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Brilakis, E.S.; Banerjee, S.; Karmpaliotis, D.; Lombardi, W.L.; Tsai, T.T.; Shunk, K.A.; Kennedy, K.F.; Spertus, J.A.; Holmes, D.R., Jr.; Grantham, J.A. Procedural outcomes of chronic total occlusion percutaneous coronary intervention. A report from the NCDR (national cardiovascular data registry). J. Am. Coll. Cardiol. Intv. 2015, 8, 245–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christopoulos, G.; Karmpaliotis, D.; Alaswad, K.; Yeh, R.W.; Jaffer, F.A.; Wyman, R.M.; Lombardi, W.L.; Menon, R.V.; Grantham, J.A.; Kandzari, D.E.; et al. Application and outcomes of a hybrid approach to chronic total occlusion percutaneous coronary intervention in a contemporary multicenter US registry. Int. J. Cardiol. 2015, 98, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Morino, Y.; Abe, M.; Morimoto, T.; Kimura, T.; Hayashi, Y.; Muramatsu, T.; Ochiai, M.; Noguchi, Y.; Kato, K.; Shibata, Y.; et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes. J. Am. Coll. Cardiol. Intv. 2011, 4, 213–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoye, A.; van Domburg, R.T.; Sonnenschein, K.; Serruys, P.W. Percutaneous coronary interventions for chronic total occlusions: The Thoraxcenter experience 1992–2002. Eur. Heart J. 2005, 26, 2630–2636. [Google Scholar] [CrossRef] [PubMed]
- Suero, J.A.; Marso, S.P.; Jones, P.G.; Laster, S.B.; Huber, K.C.; Giorgi, L.V.; Johnson, W.L.; Rutherford, B.D. Procedural outcomes and long-term survival among patients undergoing percutaneous coronary intervention of a chronic total occlusion in native coronary arteries: A 20-year experience. J. Am. Coll. Cardiol. 2001, 38, 409–414. [Google Scholar] [CrossRef] [Green Version]
- George, S.; Cockburn, J.; Clayton, T.C.; Ludman, P.; Cotton, J.; Spratt, J.; Redwood, S.; de Belder, M.; de Belder, A.; Hill, J.; et al. Long-term follow-up of elective chronicl total coronary occlusion angioplasty. J. Am. Coll. Cardiol. 2014, 64, 235–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, D.A.; Rathod, K.S.; Pavlidis, A.N.; Gallagher, S.M.; Astroulakis, Z.; Lim, P.; Sirker, A.; Knight, C.J.; Dalby, M.C.; Malik, I.S.; et al. Outcomes after chronic total occlusion percutaneous coronary interventions: An observational study of 5496 patients from the Pan-London CTO Cohort. Coron. Artery Dis. 2018, 29, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Forounzandeh, F.; Suh, J.; Stahl, E.; Ko, Y.A.; Lee, S.; Joshi, U.; Sabharwal, N.; Almuwaqqat, Z.; Gandhi, R.; Lee, H.S.; et al. Performance of J-CTO and PROGRESS CTO-Scores in predicting angiographic success and long-term outcomes of percutaneous coronary interventions for chronic total occlusions. Am. J. Cardiol. 2018, 121, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Galassi, A.R.; Sianos, G.; Werner, G.S.; Escaned, J.; Tomasello, S.D.; Boukhris, M.; Castaing, M.; Büttner, J.H.; Bufe, A.; Kalnins, A.; et al. Retrograde recanalization of chronic total occlusions in Europe. J. Am. Coll. Cardiol. 2015, 65, 2388–2400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Pershad, A.; Gulati, M.; Karmpaliotis, D.; Moses, J.; Nicholson, W.J.; Nugent, K.; Tang, Y.; Sapontis, J.; Lombardi, W.; Grantham, J.A.; et al. A sex stratified outcome analysis from the OPEN-CTO registry. Catheter. Cardiovasc. Interv. 2019, 93, 1041–1047. [Google Scholar] [CrossRef]
- Toma, A.; Stähli, B.E.; Gick, M.; Ferenc, M.; Mashayekhi, K.; Buettner, H.J.; Neumann, F.J.; Gebhard, C. Temporal changes in outcomes of women and men undergoing percutaneous coronary intervention for chronic total occlusion: 2005–2013. Clin. Res. Cardiol. 2018, 107, 449–459. [Google Scholar] [CrossRef]
- Ahn, J.; Rha, S.W.; Choi, B.; Choi, S.Y.; Byun, J.K.; Mashaly, A.; Abdelshafi, K.; Park, Y.; Jang, W.Y.; Kim, W.; et al. Impact of chronic total occlusion length on six-month angiographic and 2-year clinical outcomes. PLoS ONE 2018, 13, 30198571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teeuwen, K.; van der Schaaf, R.; Adraenssens, T.; Koolen, J.J.; Smits, C.; Henriques, J.P.S.; Vermeersch, P.H.; Tjon Joe Gin, R.M.; Schölzel, B.E.; Kelder, J.C.; et al. Randomized multicenter trial investigating angiographic outcomes of hybrid sirolimus-eluting stents with biodegradable polymer compared with everolimus-eluting stents with durable polymer in chronic total occlusions. J. Am. Coll. Cardiol. Intervn. 2017, 10, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M.; et al. 2011 ACCF/AHA/SCAI Guideline for percutaneous coronary intervention: Executive summary. Circulation 2011, 124, 2474–2609. [Google Scholar] [CrossRef] [Green Version]
- Shiomi, H.; Morimoto, T.; Kitaguchi, S.; Nakagawa, Y.; Ishii, K.; Haruna, Y.; Takamisawa, I.; Motooka, M.; Nakao, K.; Matsuda, S.; et al. The ReACT Trial. Randomized evaluation of routine follow-up coronary angiography after percutaneous coronary intervention trial. J. Am. Coll. Cardiol. Intv. 2017, 10, 109–117. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameter | n (%) | Mean ± SD | Median (IQR) |
|---|---|---|---|
| Age at procedure (years) | 65.6 ± 11.0 | 66.5 (58.2/74.6) | |
| female gender | 14 (15.1%) | ||
| Angina before intervention | 53 (57.0%) | ||
| Symptoms before intervention | 76 (81.7%) | ||
| multivessel disease | 80 (86.0%) | ||
| previous CABG | 10 (10.8%) | ||
| previous PCI | 70 (74.2%) | ||
| Diabetes | 31 (33.3%) | ||
| Smoking | 53 (57.0%) | ||
| Hyperlipidemia | 55 (59.1%) | ||
| Family history of CAD | 24 (25.8%) | ||
| arterial hypertension | 74 (79.6%) | ||
| peripheral artery disease | 9 (9.7%) | ||
| cerebral artery disease | 8 (8.6%) | ||
| renal insufficiency | 6 (6.4%) | ||
| hyperthyroidism | 13 (14.0%) | ||
| weight (KG) | 90.2 ± 20.3 | 87.3 (78.0/100.8) | |
| height (meters) | 1.74 ± 0.10 | 1.76 (1.68/1.80) | |
| Body mass index (kg/m2) | 25.8 ± 4.8 | 24.9 (22.8/28.4) | |
| Adipositas | 14 (21.2%) | ||
| mean LVEF (%) | 50.5 ±9.6 | 55.0 (45.0/55.0) | |
| reduced LVEF at baseline | 19 (29.7%) | ||
| proof of vitality of CTO region prior to intervention | 52 (57.8%) | ||
| CTO vessel | |||
| LAD | 19 (20.4%) | ||
| LCX | 23 (24.7%) | ||
| RCA | 51 (54.8%) | ||
| J-CTO Score | 1.49 ± 1.09 | 1.0 (1.0/2.0) | |
| Components of the J-CTO Score | |||
| Entry | 27 (29.0%) | ||
| Calcification | 47 (50.5%) | ||
| Bending > 45° | 25 (26.9%) | ||
| Lesion Length > 20 mm | 29 (31.2%) | ||
| Retry Lesion | 12 (12.9%) |
| Re-Occlusion | Restenosis | TVF | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Re-Occlusion (n = 7) | No Re-Occlusion (n = 86) | p-Value | Restenosis (n = 11) | No Restenosis (n = 82) | p-Value | TVF (n = 14) | No TVF (n = 79) | p-Value | |
| Baseline parameters | |||||||||
| female gender | 28.6 | 14.0 | 0.283 | 36.4 | 12.2 | 0.058 | 35.7 | 11.3 | 0.034 |
| Age at procedure | 65.1 ± 6.9 | 65.6 ± 11.3 | 0.843 | 65.6 ± 7.5 | 65.6 ± 11.5 | 0.988 | 60.6 ± 13.4 | 66.5 ± 10.4 | 0.063 |
| Reduced LVEF | 20.0 | 30.5 | 1.000 | 22.2 | 30.9 | 0.713 | 30.0 | 29.6 | 1.000 |
| LVEF baseline | 51.8 ± 6.6 | 50.4 ± 9.8 | 0.923 | 51.0 ± 6.4 | 50.5 ± 10.0 | 0.667 | 50.4 ± 6.4 | 50.6 ± 10.1 | 0.466 |
| Angina at baseline | 57.1 | 57.0 | 1.000 | 54.5 | 57.3 | 1.000 | 50.0 | 58.2 | 0.574 |
| Symptoms at baseline | 100 | 80.2 | 0.342 | 100.0 | 79.3 | 0.206 | 92.9 | 79.7 | 0.453 |
| Body Mass Index | 23.6 ± 2.1 | 25.9 ± 4.9 | 0.356 | 23.1 ± 2.7 | 26.1 ± 4.9 | 0.130 | 23.8 ± 4.8 | 26.1 ± 4.8 | 0.158 |
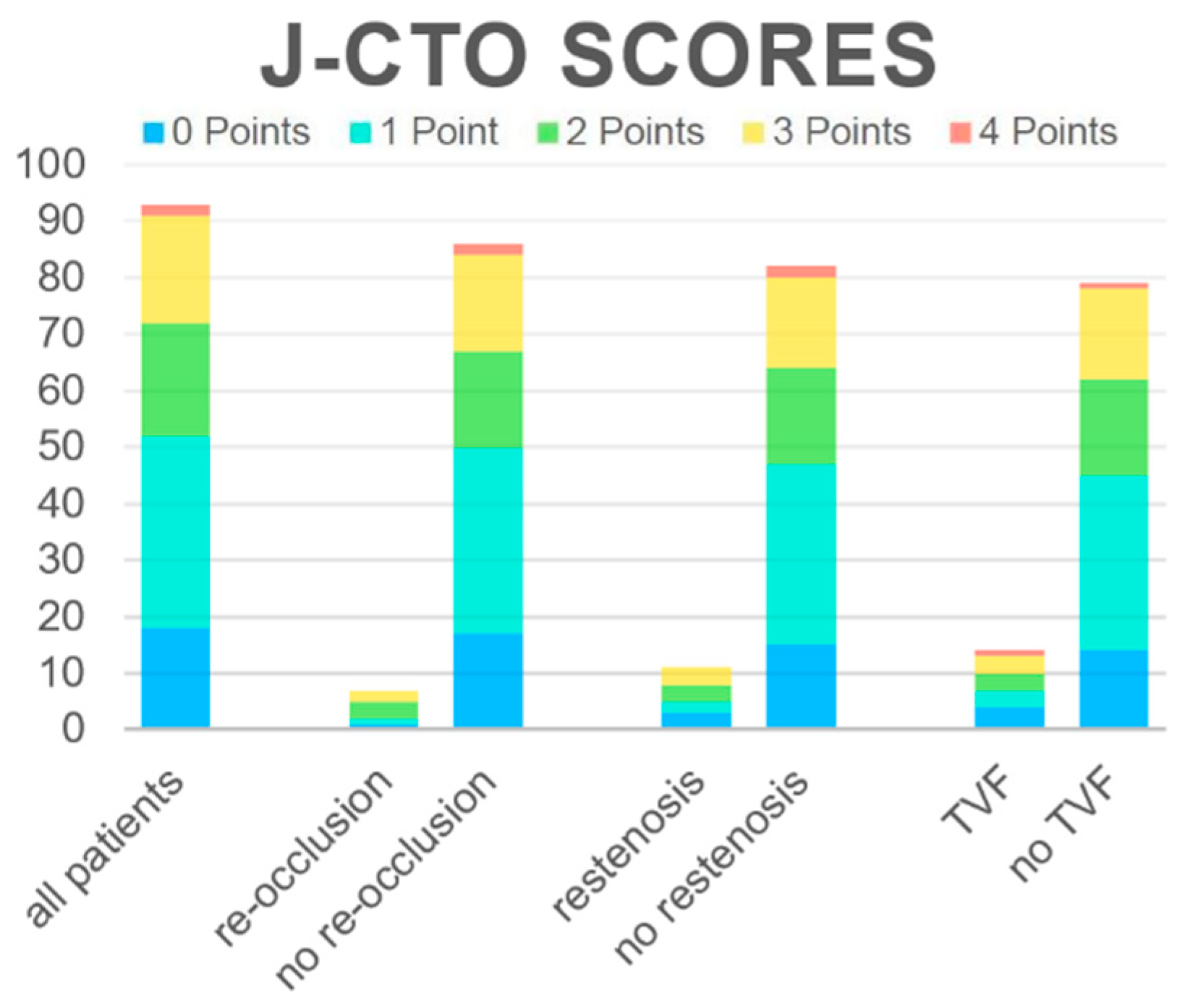
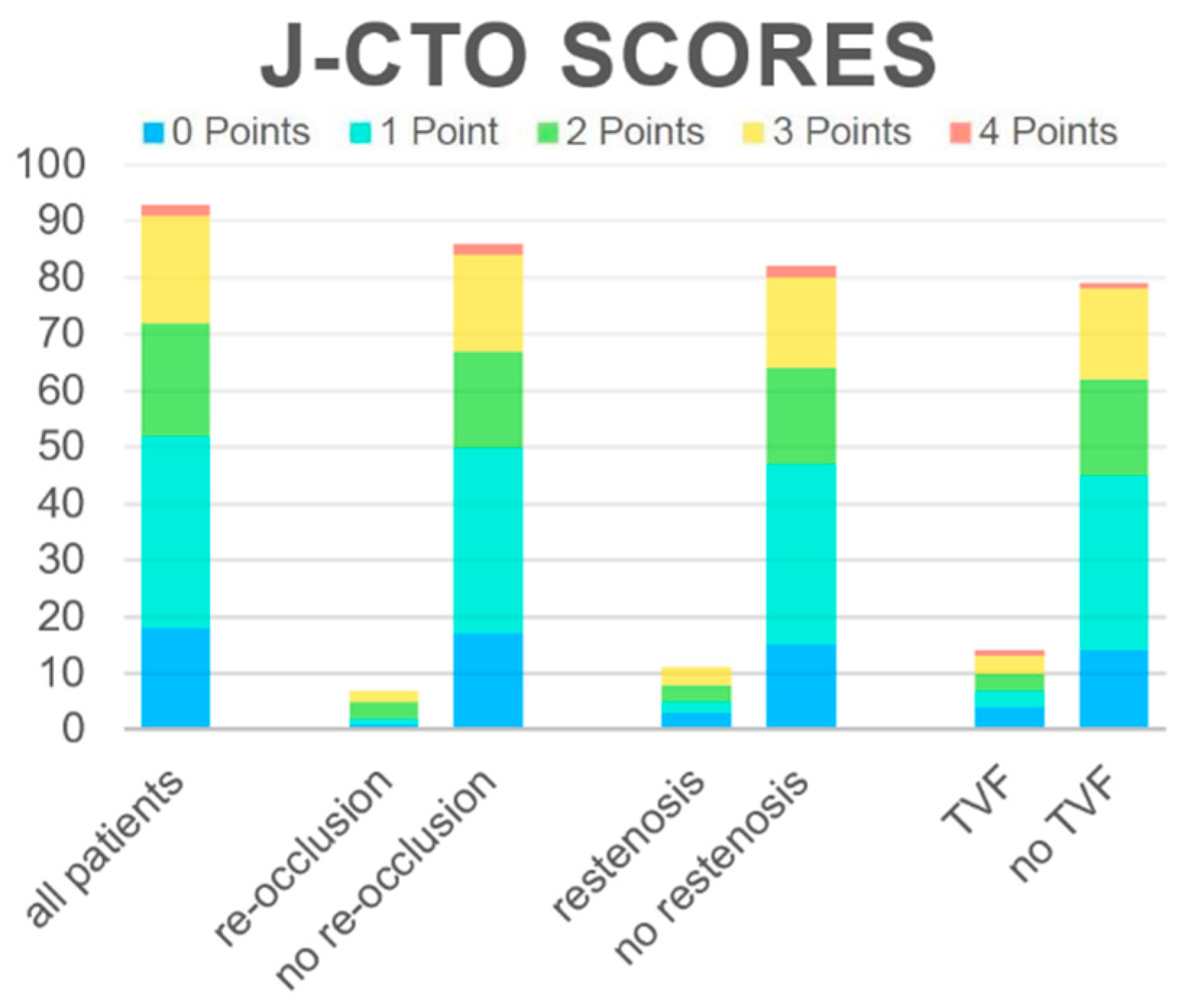
| J-CTO Score | 1.86 ± 1.07 | 1.47 ± 1.09 | 0.307 | 1.55 ± 1.21 | 1.49 ± 1.08 | 0.843 | 1.60 ± 1.82 | 1.49 ± 1.05 | 0.889 |
| J-CTO Score ≥ 3 | 28.6 | 22.1 | 0.654 | 37.5 | 22.0 | 0.707 | 28.6 | 21.5 | 0.511 |
| Periprocedural characteristics | |||||||||
| CTO vessel | |||||||||
| - LAD | 28.6 | 19.8 | 0.332 | 18.2 | 20.7 | 0.969 | 14.3 | 21.5 | 0.811 |
| - LCx | 42.9 | 23.3 | 27.3 | 24.4 | 28.6 | 24.1 | |||
| - RCA | 28.6 | 57.0 | 54.5 | 54.9 | 57.1 | 54.40 | |||
| Reduced TIMI-flow post intervention | 100.0 | 8.1 | <0.001 | 90.9 | 4.9 | <0.001 | 71.4 | 5.1 | <0.001 |
| Stent length (mm) | 36.3 ± 41.1 | 58.3 ± 29.2 | 0.044 | 38.2 ± 36.2 | 59.1 ± 29.0 | 0.020 | 43.0 ± 35.9 | 59.0 ± 29.0 | 0.042 |
| Stent number | 1.6 ± 1.6 | 2.2 ± 1.0 | 0.065 | 1.6 ± 1.4 | 2.2 ± 1.0 | 0.040 | 1.9 ± 1.3 | 2.2 ± 1.0 | 0.183 |
| Fluoroscopy dose (cgy*dm) | 8062 ± 4148 | 7363 ± 6308 | 0.351 | 7547 ± 4697 | 7398 ± 6352 | 0.677 | 7134 ± 4324 | 7465 ± 6449 | 0.830 |
| Fluoroscopy time (min) | 29.6 ± 18.0 | 26.0 ± 15.9 | 0.570 | 30.8 ± 18.8 | 25.7 ± 15.6 | 0.388 | 30.2 ± 18.0 | 25.6 ± 15.6 | 0.347 |
| Duration (total) (min) | 165.1 ± 26.8 | 123.8 ± 44.8 | 0.006 | 154.6 ± 44.0 | 123.2 ± 44.0 | 0.013 | 144.4 ± 45.7 | 123.8 ± 44.4 | 0.056 |
| Contrast volume (mL) | 277.4 ± 159.4 | 240.7 ± 103.1 | 0.662 | 279.2 ± 141.2 | 238.8 ± 102.4 | 0.372 | 263.8 ± 132.2 | 239.9 ± 103.2 | 0.576 |
| Periinterventional CK (u/L) | 178.3 ± 141.2 | 116.0 ± 94.9 | 0.276 | 132.7 ± 120.8 | 118.8 ± 96.6 | 0.929 | 123.5 ± 108.9 | 119.9 ± 98.9 | 0.802 |
| High-sensitive Troponin I periinterventional (pg/mL) | 1126.3 ± 1560.6 | 412.0 ± 1391.4 | 0.013 | 771.4 ± 1255.7 | 420.7 ± 1425.5 | 0.013 | 662.4 ± 1124.7 | 425.5 ± 1451.3 | 0.044 |
| Creatinine periinterventional (mg/dL) | 0.93 ± 0.11 | 1.16 ± 0.97 | 0.412 | 0.96 ± 0.14 | 1.17 ± 0.99 | 0.636 | 0.96 ± 0.13 | 1.18 ± 1.01 | 0.580 |
| CrP periinterventional (mg/L) | 37.0 ± 59.5 | 7.77 ± 15.7 | 0.238 | 23.6 ± 47.7 | 8.1 ± 16.4 | 0.712 | 21.8 ± 45.6 | 8.1 ± 16.5 | 0.685 |
| Symptoms at follow-up | |||||||||
| Angina | 28.6 | 32.5 | 1.000 | 36.4 | 31.6 | 0.741 | 35.7 | 31.6 | 0.763 |
| Symptoms | 42.9 | 53.4 | 0.704 | 54.5 | 52.4 | 1.000 | 50.0 | 53.2 | 1.000 |
| Re-Occlusion | Restenosis | TVF | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Baseline parameters | ||||||
| female gender | 3.77 (0.54–26.43) | 0.182 | 8.88 (1.58–49.89) | 0.013 | 11.03 (2.08–58.47) | 0.005 |
| Age at procedure | 0.99 (0.91–1.08) | 0.822 | 1.00 (0.93–1.07) | 0.995 | 0.95 (0.90–1.01) | 0.080 |
| Reduced LVEF | 0.43 (0.04–5.09) | 0.426 | 0.49 (0.08–3.10) | 0.449 | 0.70 (0.13–3.87) | 0.680 |
| LVEF baseline | 1,92 (0.91–1.16) | 0.713 | 1.01 (0.92–1.10) | 0.895 | 1.00 (0.92–1.09) | 0.956 |
| Angina at baseline | 0.96 (0.19–4.79) | 0.957 | 0.78 (0.20–2.97) | 0.712 | 0.70 (0.21–2.40) | 0.704 |
| Symptoms at baseline | not calculable | not calculable | 8.65 (0.62–121.31) | 0.109 | ||
| Body Mass Index | 0.79 (0.57–1.09) | 0.147 | 0.73 (0.55–0.98) | 0.037 | 0.80 (0.65–0.99) | 0.037 |
| J-CTO-Score | 1.42 (0.64–3.16) | 0.394 | 1.03 (0.54–1.95) | 0.929 | 1.11 (0.62–1.98) | 0.728 |
| J-CTO Score ≥ 3 | 1.40 (0.21–8.99) | 0.721 | 1.26 (0.27–5.84) | 0.768 | 1.35 (0.33–5.45) | 0.676 |
| Periprocedural characteristics | ||||||
| CTO vessel | 0.50 (0.18–1.38) | 0.180 | 0.98 (0.37–2.14) | 0.797 | 0.97 (0.43–2.19) | 0.936 |
| -LAD | ||||||
| -LCx | ||||||
| -RCA | ||||||
| Reduced TIMI-flow post intervention | 20.36 (3.21–129.00) | 0.001 | 21.29 (4.28–105.97) | <0.001 | 11.00 (2.66–45.45) | 0.001 |
| Stent length (mm) | 0.97 (0.94–1.00) | 0.081 | 0.98 (0.95–1.00) | 0.051 | 0.98 (0.95–1.00) | 0.060 |
| Stent number | 0.52 (0.21–1.29) | 0.156 | 0.58 (0.28–1.17) | 0.125 | 0.70 (0.38–1.29) | 0.255 |
| Fluoroscopy dose (cgy*dm) | 1.00 (1.00–1.00) | 0.748 | 1.00 (1.00–1.00) | 0.871 | 1.00 (1.00–1.00) | 0.868 |
| Fluoroscopy time (min) | 1.02 (0.97–1.07) | 0.470 | 1.02 (0.99–1.07) | 0.233 | 1.03 (0.99–1.06) | 0.185 |
| Duration (total) (min) | 1.02 (1.00–1.04) | 0.025 | 1.02 (1.00–1.03) | 0.030 | 1.01 (1.00–1.03) | 0.056 |
| Contrast volume (mL) | 1.00 (1.00–1.01) | 0.287 | 1.00 (1.00–1.01) | 0.200 | 1.00 (1.00–1.01) | 0.486 |
| Periinterventional CK (u/L) | 1.01 (1.00–1.01) | 0.153 | 1.00 (0.99–1.01) | 0.757 | 1.00 (0.99–1.01) | 0.973 |
| High-sensitive Troponin I periinterventional (pg/mL) | 1.00 (1.00–1.00) | 0.286 | 1.00 (1.00–1.00) | 0.247 | 1.00 (1.00–1.00) | 0.459 |
| Creatinine periinterventional (mg/dL) | 0.07 (0.00–8.94) | 0.284 | 0.12 (0.00–4.57) | 0.256 | 0.22 (0.01–5.91) | 0.366 |
| CrP periinterventional (mg/L) | 1.03 (1.00–1.06) | 0.049 | 1.02 (1.00–1.05) | 0.067 | 1.02 (1.00–1.04) | 0.103 |
| Symptoms at follow-up | ||||||
| Angina | 0.75 (0.13–4.45) | 0.750 | 1.24 (0.30–5.07) | 0.762 | 0.99 (0.28–3.59) | 0.992 |
| Symptoms | 0.69 (0.14–3.36) | 0.642 | 1.27 (0.34–4.71) | 0.723 | 0.92 (0.28–3.01) | 0.891 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geyer, M.; Wild, J.; Hirschmann, M.; Dimitriadis, Z.; Münzel, T.; Gori, T.; Wenzel, P. Predictors for Target Vessel Failure after Recanalization of Chronic Total Occlusions in Patients Undergoing Surveillance Coronary Angiography. J. Clin. Med. 2020, 9, 178. https://doi.org/10.3390/jcm9010178
Geyer M, Wild J, Hirschmann M, Dimitriadis Z, Münzel T, Gori T, Wenzel P. Predictors for Target Vessel Failure after Recanalization of Chronic Total Occlusions in Patients Undergoing Surveillance Coronary Angiography. Journal of Clinical Medicine. 2020; 9(1):178. https://doi.org/10.3390/jcm9010178
Chicago/Turabian StyleGeyer, Martin, Johannes Wild, Marc Hirschmann, Zisis Dimitriadis, Thomas Münzel, Tommaso Gori, and Philip Wenzel. 2020. "Predictors for Target Vessel Failure after Recanalization of Chronic Total Occlusions in Patients Undergoing Surveillance Coronary Angiography" Journal of Clinical Medicine 9, no. 1: 178. https://doi.org/10.3390/jcm9010178
APA StyleGeyer, M., Wild, J., Hirschmann, M., Dimitriadis, Z., Münzel, T., Gori, T., & Wenzel, P. (2020). Predictors for Target Vessel Failure after Recanalization of Chronic Total Occlusions in Patients Undergoing Surveillance Coronary Angiography. Journal of Clinical Medicine, 9(1), 178. https://doi.org/10.3390/jcm9010178