Walking Speed: Japanese Data in Chronic Liver Diseases

Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Measurement of Walking Speed
2.3. Statistical Considerations
3. Results
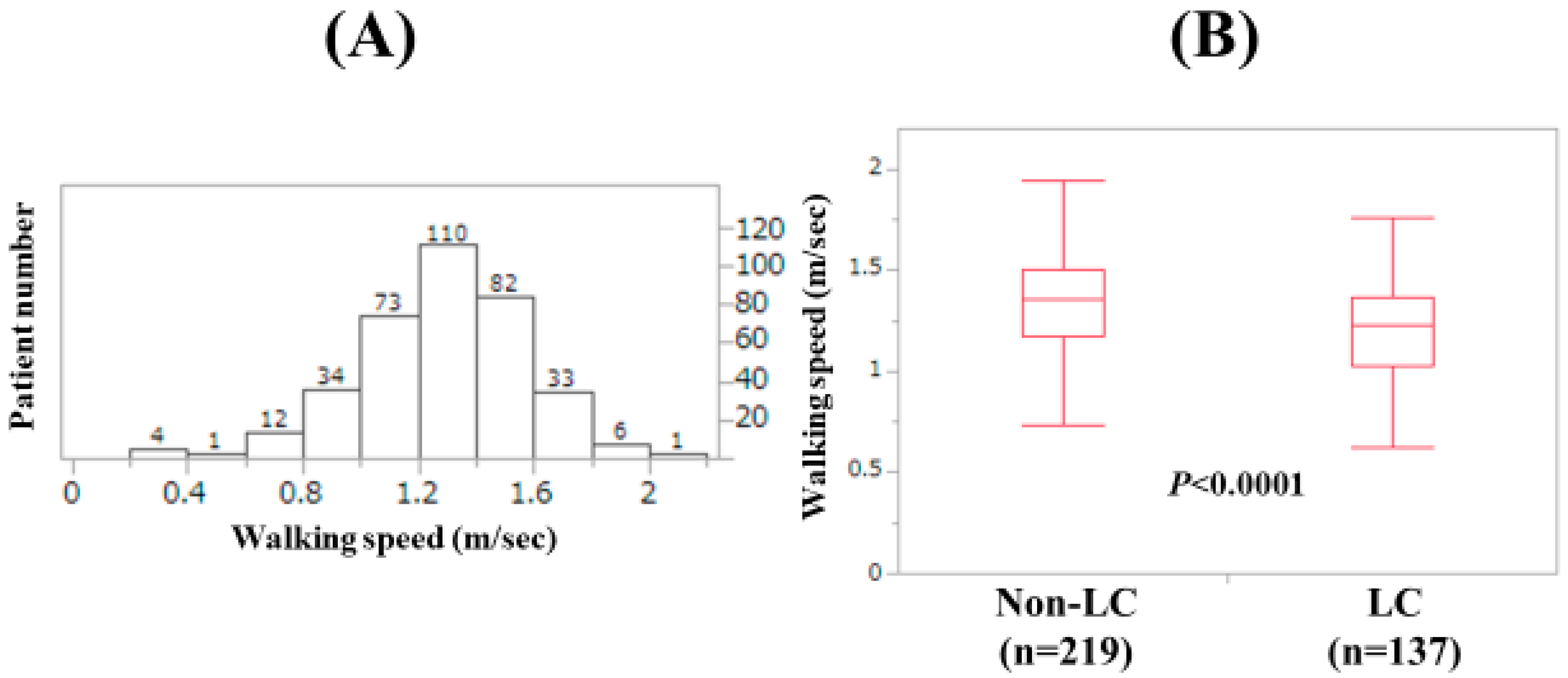
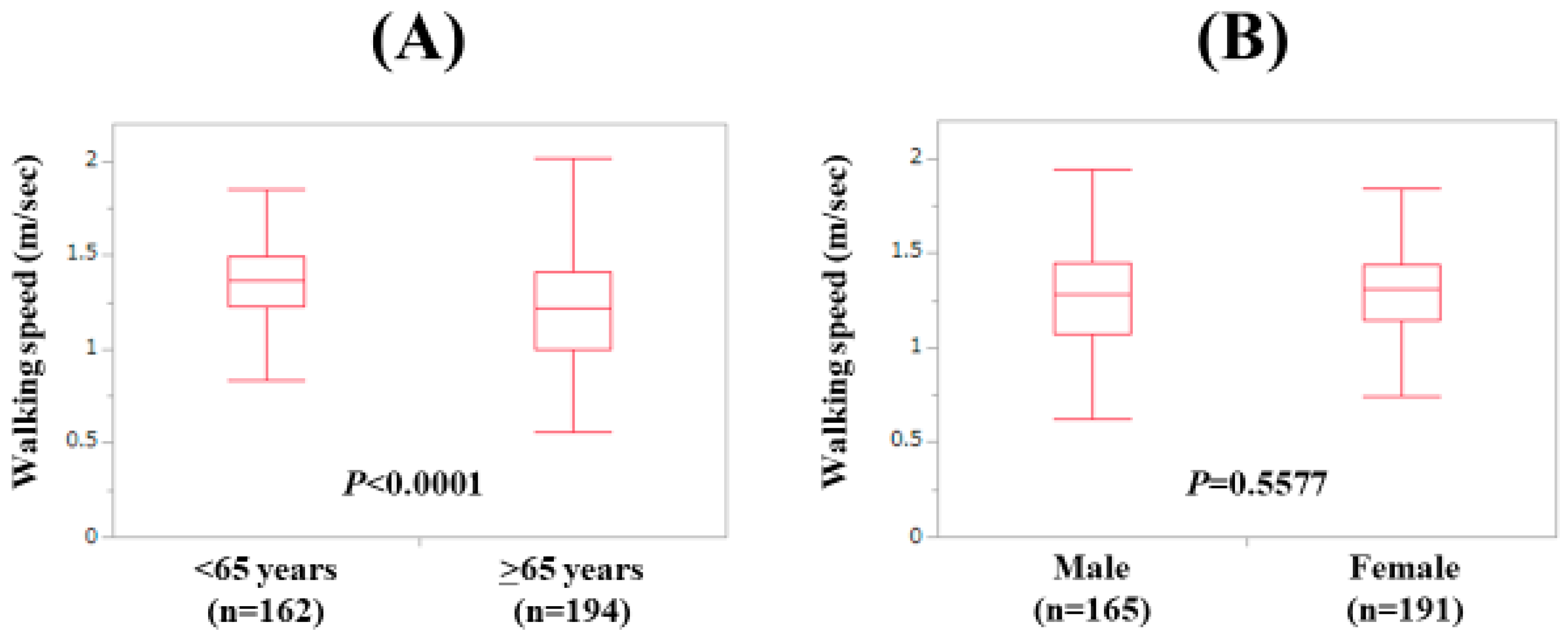
3.1. Baseline Features
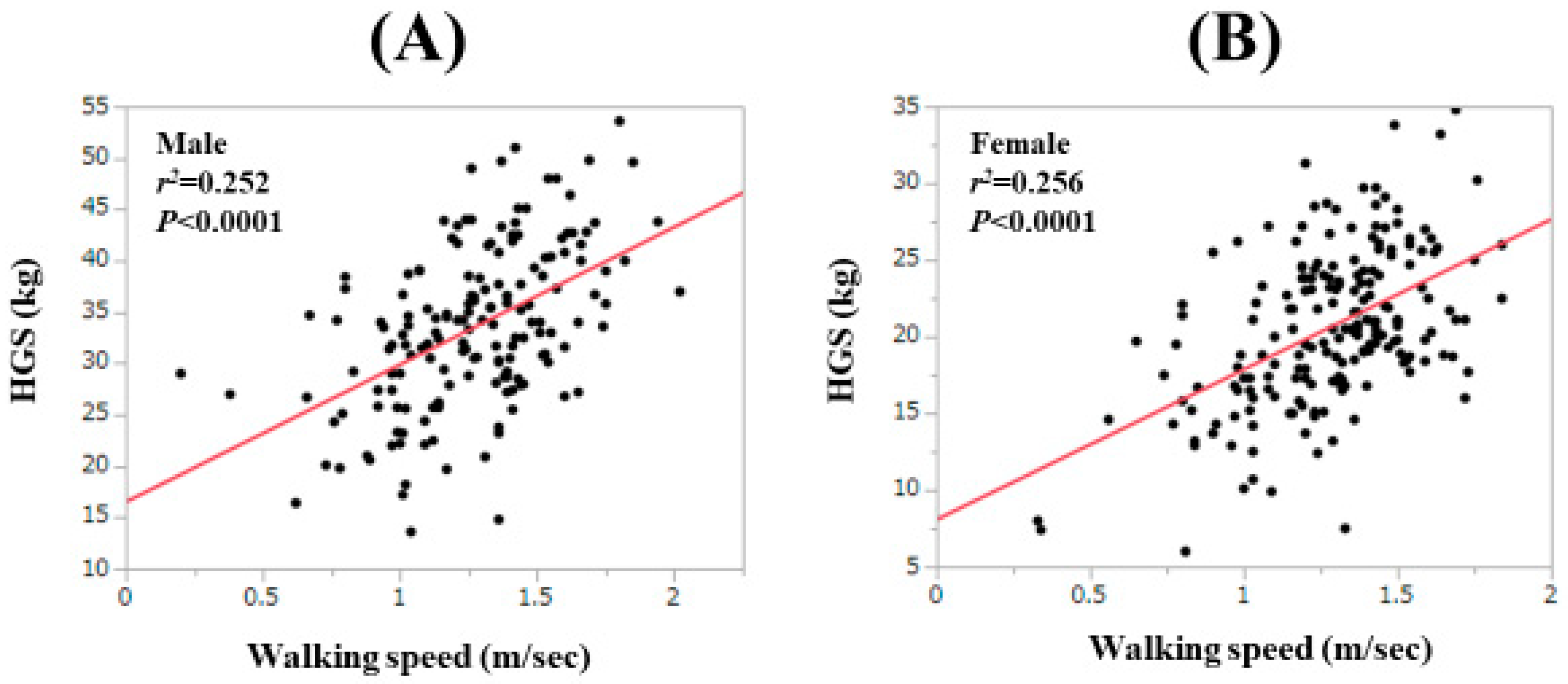
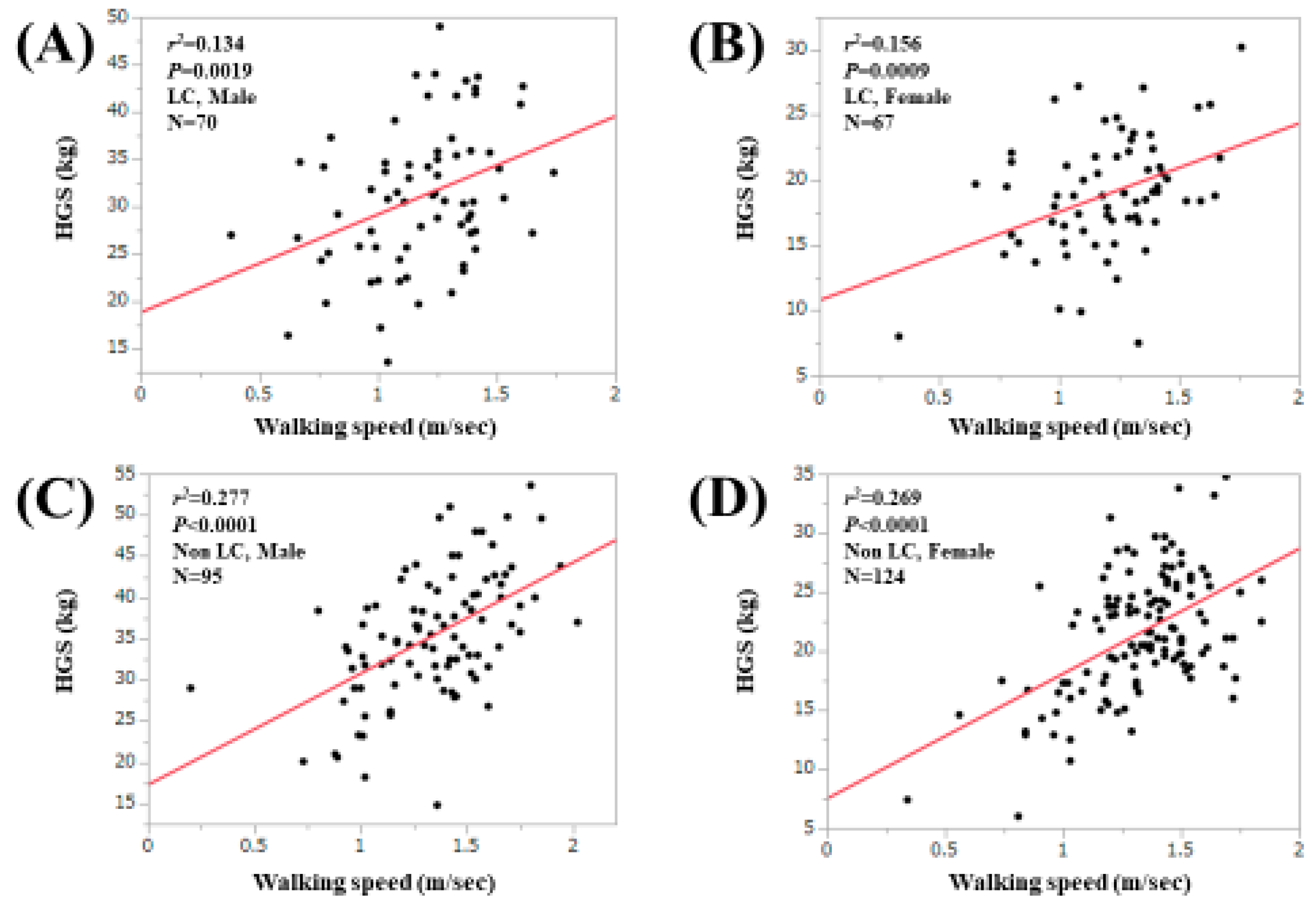
3.2. Relationship between WS and HGS for All Cases, LC Cases and Non-LC Cases
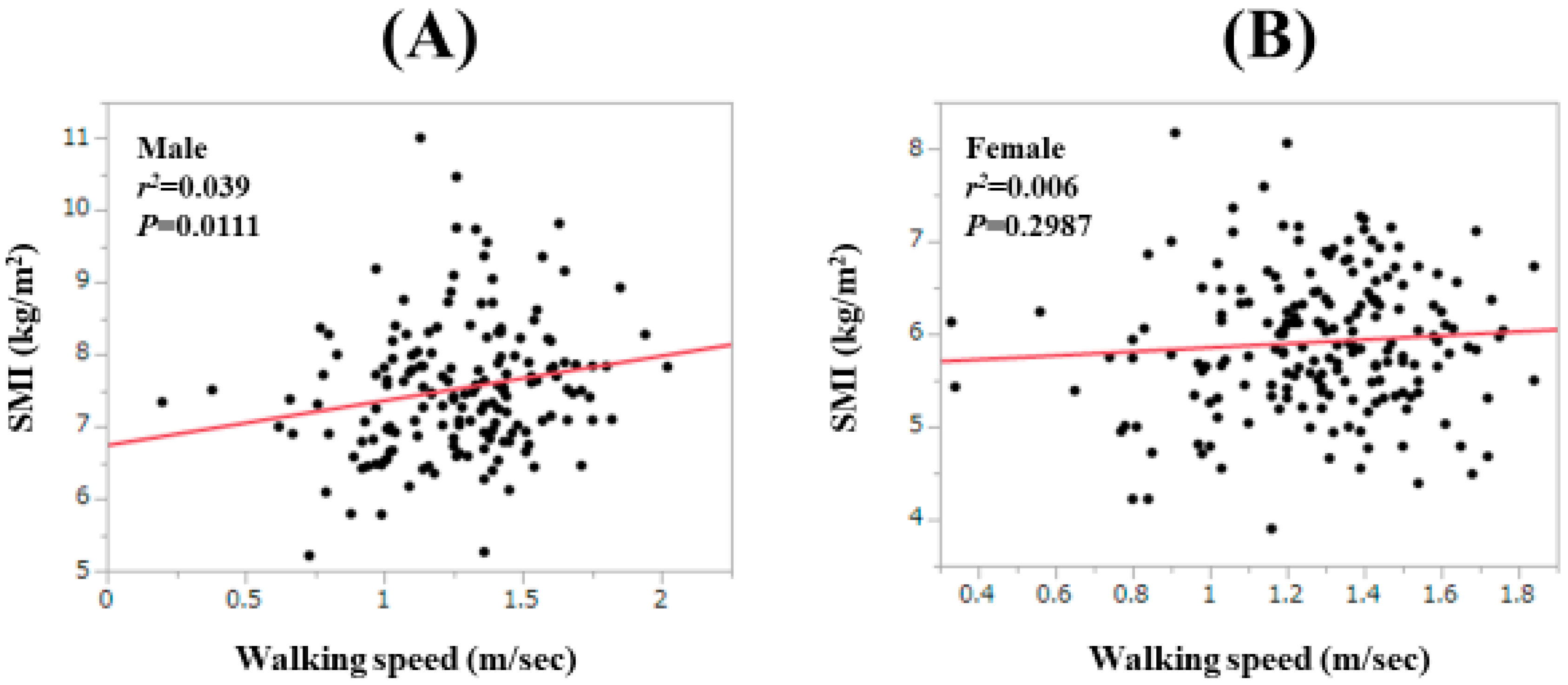
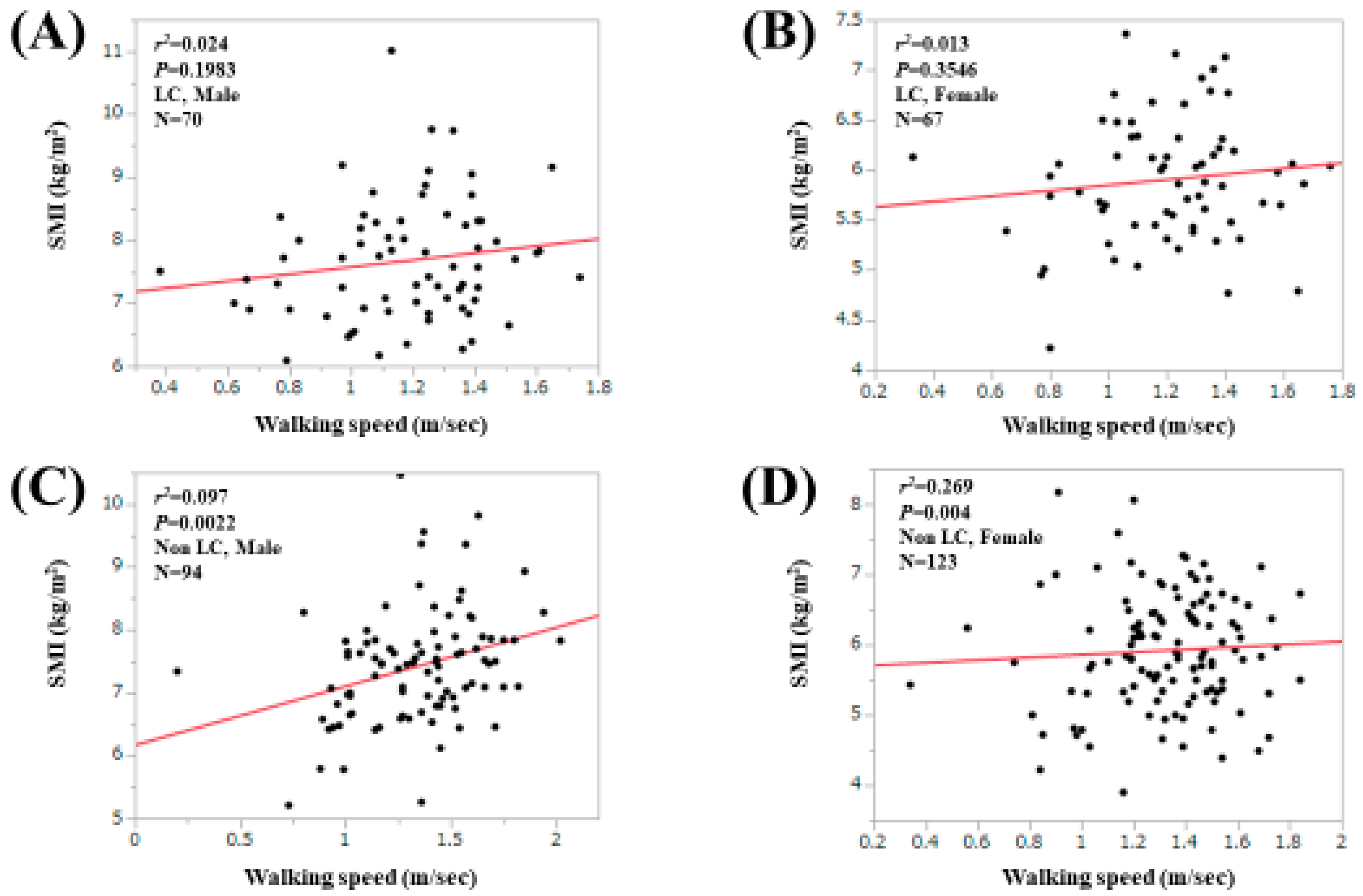
3.3. Relationship between WS and SMI for All Cases, LC Cases and Non-LC Cases
3.4. Correlation Coefficients between WS and Baseline Parameters Other than HGS
3.5. Uni- and Multivariate Analyses of Factors Related to the WS Decline (<0.8 m/s)
3.6. Uni- and Multivariate Analyses of Factors Related to the WS Decline (<1.0 m/s)
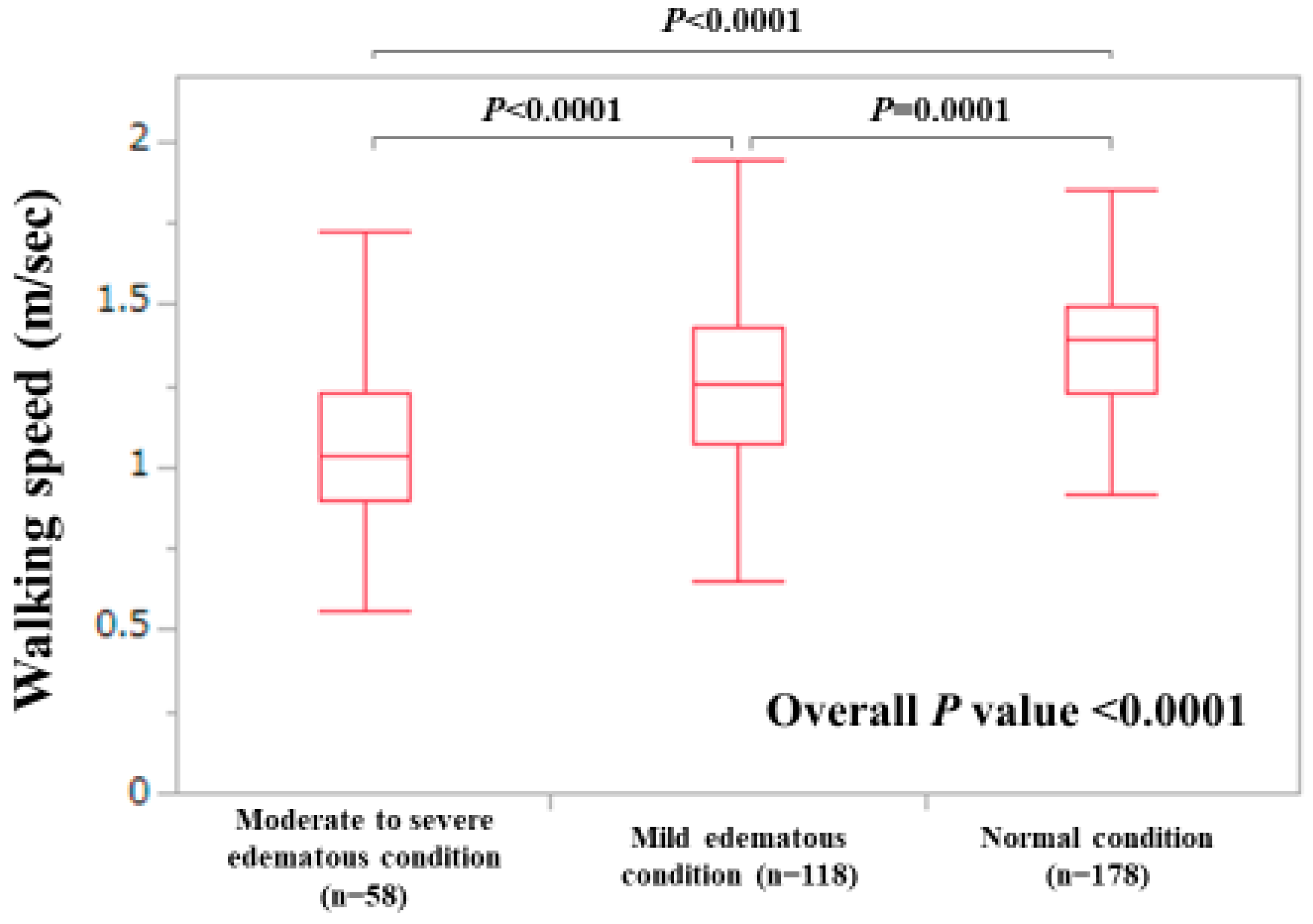
3.7. WS Stratified by ECW to TBW Ratio
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CLD | chronic liver disease |
| LC | liver cirrhosis |
| BIA | bioimpedance analysis |
| CT | computed tomography |
| HGS | hand grip strength |
| WS | walking speed |
| EWGSOP | European Working Group on Sarcopenia in Older People |
| AWGS | Asian Working Group on Sarcopenia |
| JSH | Japanese society of hepatology |
| M2BPGi | Mac-2 binding protein glycosylation isomer |
| SMI | skeletal muscle index |
| IRB | institutional review board |
| m/s | meter/second |
| ECW | extracellular water |
| TBW | total body water |
| BTR | branched-chain amino acid to tyrosine ratio |
| HR | hazard ratio |
| CI | confidence interval |
| NILS-LSA | National Institute for Longevity Sciences-Longitudinal Study of Aging |
| IWGS | International Working Group on Sarcopenia |
References
- Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; Takata, R.; et al. Combined Albumin-Bilirubin Grade and Skeletal Muscle Mass as a Predictor in Liver Cirrhosis. J. Clin. Med. 2019, 8, 782. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; Takata, R.; et al. Health-Related Quality of Life in Chronic Liver Diseases: A Strong Impact of Hand Grip Strength. J. Clin. Med. 2018, 7, 553. [Google Scholar] [CrossRef] [PubMed]
- Aby, E.S.; Saab, S. Frailty, Sarcopenia, and Malnutrition in Cirrhotic Patients. Clin. Liver Dis. 2019, 23, 589–605. [Google Scholar] [CrossRef] [PubMed]
- Williams, F.R.; Berzigotti, A.; Lord, J.M.; Lai, J.C.; Armstrong, M.J. Review article: Impact of exercise on physical frailty in patients with chronic liver disease. Aliment. Pharmacol. Ther. 2019. [Google Scholar] [CrossRef] [PubMed]
- Ebadi, M.; Bhanji, R.A.; Mazurak, V.C.; Montano-Loza, A.J. Sarcopenia in cirrhosis: From pathogenesis to interventions. J. Gastroenterol. 2019, 54, 845–859. [Google Scholar] [CrossRef]
- Ooi, P.H.; Hager, A.; Mazurak, V.C.; Dajani, K.; Bhargava, R.; Gilmour, S.M.; Mager, D.R. Sarcopenia in Chronic Liver Disease: Impact on Outcomes. Liver Transpl. 2019, 25, 1422–1438. [Google Scholar] [CrossRef]
- Hsu, C.S.; Kao, J.H. Sarcopenia and chronic liver diseases. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 1229–1244. [Google Scholar] [CrossRef]
- Nardelli, S.; Gioia, S.; Faccioli, J.; Riggio, O.; Ridola, L. Sarcopenia and cognitive impairment in liver cirrhosis: A viewpoint on the clinical impact of minimal hepatic encephalopathy. World J. Gastroenterol. 2019, 25, 5257–5265. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Werlang, M.; Panjawatanan, P.; Kroner, P.T.; Cheungpasitporn, W.; Lukens, F.J.; Pungpapong, S.; Ungprasert, P. Association between sarcopenia and hepatic encephalopathy: A systematic review and meta-analysis. Ann. Hepatol. 2019, S1665–S2681. [Google Scholar] [CrossRef]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Moriya, K.; Hino, K.; Nishiguchi, S. Japan Society of Hepatology guidelines for sarcopenia in liver disease (1st edition): Recommendation from the working group for creation of sarcopenia assessment criteria. Hepatol. Res. 2016, 46, 951–963. [Google Scholar] [CrossRef]
- Arai, H.; Akishita, M.; Chen, L.K. Growing research on sarcopenia in Asia. Geriatr. Gerontol. Int. 2014, 14, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, M.; Gow, P.J.; Grossmann, M.; Angus, P.W. Review article: Sarcopenia in cirrhosis—Aetiology, implications and potential therapeutic interventions. Aliment. Pharmacol. Ther. 2016, 43, 765–777. [Google Scholar] [CrossRef]
- Lai, J.C.; Covinsky, K.E.; McCulloch, C.E.; Feng, S. The Liver Frailty Index Improves Mortality Prediction of the Subjective Clinician Assessment in Patients with Cirrhosis. Am. J. Gastroenterol. 2018, 113, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Bhanji, R.A.; Montano-Loza, A.J.; Watt, K.D. SARCOPENIA IN CIRRHOSIS: Looking beyond the skeletal muscle loss to see the systemic disease. Hepatology 2019. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; van Kan, G.A.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An undiagnosed condition in older adults. Current consensus definition: Prevalence, etiology, and consequences. International working group on sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef]
- Nagamatsu, A.; Kawaguchi, T.; Hirota, K.; Koya, S.; Tomita, M.; Hashida, R.; Kida, Y.; Narao, H.; Manako, Y.; Tanaka, D.; et al. Slow walking speed overlapped with low handgrip strength in chronic liver disease patients with hepatocellular carcinoma. Hepatol. Res. 2019. [Google Scholar] [CrossRef]
- Harimoto, N.; Yoshizumi, T.; Izumi, T.; Motomura, T.; Harada, N.; Itoh, S.; Ikegami, T.; Uchiyama, H.; Soejima, Y.; Nishie, A.; et al. Clinical Outcomes of Living Liver Transplantation According to the Presence of Sarcopenia as Defined by Skeletal Muscle Mass, Hand Grip, and Gait Speed. Transplant. Proc. 2017, 49, 2144–2152. [Google Scholar] [CrossRef]
- Chou, M.Y.; Nishita, Y.; Nakagawa, T.; Tange, C.; Tomida, M.; Shimokata, H.; Otsuka, R.; Chen, L.K.; Arai, H. Role of gait speed and grip strength in predicting 10-year cognitive decline among community-dwelling older people. BMC Geriatr. 2019, 19, 186. [Google Scholar] [CrossRef]
- Yoshida, D.; Suzuki, T.; Shimada, H.; Park, H.; Makizako, H.; Doi, T.; Anan, Y.; Tsutsumimoto, K.; Uemura, K.; Ito, T.; et al. Using two different algorithms to determine the prevalence of sarcopenia. Geriatr. Gerontol. Int. 2014, 14, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Fukui, H.; Saito, H.; Ueno, Y.; Uto, H.; Obara, K.; Sakaida, I.; Shibuya, A.; Seike, M.; Nagoshi, S.; Segawa, M.; et al. Evidence-based clinical practice guidelines for liver cirrhosis 2015. J. Gastroenterol. 2016, 51, 629–650. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Zheng, R.Q.; Kim, S.R.; Okabe, Y.; Osaki, Y.; Iijima, H.; Itani, T.; Kasugai, H.; Kanematsu, M.; Ito, K.; et al. Diagnostic accuracy of imaging for liver cirrhosis compared to histologically proven liver cirrhosis. A multicenter collaborative study. Intervirology 2008, 51, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Zarski, J.P.; Sturm, N.; Guechot, J.; Paris, A.; Zafrani, E.S.; Asselah, T.; Boisson, R.C.; Bosson, J.L.; Guyader, D.; Renversez, J.C.; et al. ANRS HCEP 23 Fibrostar Group. Comparison of nine blood tests and transient elastography for liver fibrosis in chronic hepatitis C: The ANRS HCEP-23 study. J. Hepatol. 2012, 56, 55–62. [Google Scholar] [CrossRef]
- Tsochatzis, E.A.; Gurusamy, K.S.; Ntaoula, S.; Cholongitas, E.; Davidson, B.R.; Burroughs, A.K. Elastography for the diagnosis of severity of fibrosis in chronic liver disease: A meta-analysis of diagnostic accuracy. J. Hepatol. 2011, 54, 650–659. [Google Scholar] [CrossRef]
- Hasegawa, K.; Takata, R.; Nishikawa, H.; Enomoto, H.; Ishii, A.; Iwata, Y.; Miyamoto, Y.; Ishii, N.; Yuri, Y.; Nakano, C.; et al. Impact of Wisteria floribunda Agglutinin-Positive Mac-2-Binding Protein in Patients with Hepatitis C Virus-Related Compensated Liver Cirrhosis. Int. J. Mol. Sci. 2016, 17, 1500. [Google Scholar] [CrossRef]
- Nishikawa, H.; Enomoto, H.; Ishii, A.; Iwata, Y.; Miyamoto, Y.; Ishii, N.; Yuri, Y.; Takata, R.; Hasegawa, K.; Nakano, C.; et al. Development of a simple predictive model for decreased skeletal muscle mass in patients with compensated chronic liver disease. Hepatol. Res. 2017, 47, 1223–1234. [Google Scholar] [CrossRef]
- Shimokata, H.; Ando, F.; Niino, N. A new comprehensive study on aging--the National Institute for Longevity Sciences, Longitudinal Study of Aging (NILS-LSA). J. Epidemiol. 2000, 10, S1–S9. [Google Scholar] [CrossRef]
- Nishikawa, H.; Yoh, K.; Enomoto, H.; Ishii, N.; Iwata, Y.; Nakano, C.; Takata, R.; Nishimura, T.; Aizawa, N.; Sakai, Y.; et al. Extracellular Water to Total Body Water Ratio in Viral Liver Diseases: A Study Using Bioimpedance Analysis. Nutrients 2018, 10, 1072. [Google Scholar] [CrossRef]
- Wang, C.W.; Feng, S.; Covinsky, K.E.; Hayssen, H.; Zhou, L.Q.; Yeh, B.M.; Lai, J.C. A Comparison of Muscle Function, Mass, and Quality in Liver Transplant Candidates: Results from the Functional Assessment in Liver Transplantation Study. Transplantation 2016, 100, 1692–1698. [Google Scholar] [CrossRef]
- Sternäng, O.; Reynolds, C.A.; Finkel, D.; Ernsth-Bravell, M.; Pedersen, N.L.; Dahl Aslan, A.K. Grip strength and cognitive abilities: Associations in old age. J. Gerontol. B Psychol. Sci. Soc. Sci. 2015, 71, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Inzitari, M.; Newman, A.B.; Yaffe, K.; Boudreau, R.; de Rekeneire, N.; Shorr, R.; Harris, T.B.; Rosano, C. Gait speed predicts decline in attention and psychomotor speed in older adults: The health aging and body composition study. Neuroepidemiology 2007, 29, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.L.; Liang, C.K.; Liao, M.C.; Chou, M.Y.; Lin, Y.T. Slow gait speed as a predictor of 1-year cognitive decline in a veterans’ retirement community in southern Taiwan. Geriatr. Gerontol. Int. 2017, 17, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Clouston, S.A.; Brewster, P.; Kuh, D.; Richards, M.; Cooper, R.; Hardy, R.; Rubin, M.S.; Hofer, S.M. The dynamic relationship between physical function and cognition in longitudinal aging cohorts. Epidemiol. Rev. 2013, 35, 33–50. [Google Scholar] [CrossRef]
- Hadjihambi, A.; Arias, N.; Sheikh, M.; Jalan, R. Hepatic encephalopathy: A critical current review. Hepatol. Int. 2018, 12, 135–147. [Google Scholar] [CrossRef]
- Ji, F.; Pasternak, O.; Liu, S.; Loke, Y.M.; Choo, B.L.; Hilal, S.; Xu, X.; Ikram, M.K.; Venketasubramanian, N.; Chen, C.L.; et al. Distinct white matter microstructural abnormalities and extracellular water increases relate to cognitive impairment in Alzheimer’s disease with and without cerebrovascular disease. Alzheimers Res. Ther. 2017, 9, 63. [Google Scholar] [CrossRef]
- Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; Takata, R.; et al. Significant Correlation Between Grip Strength and m2bpgi in Patients with Chronic Liver Diseases. J. Clin. Med. 2019, 8, 1359. [Google Scholar] [CrossRef]
- Kojima, G.; Liljas, A.E.M.; Iliffe, S. Frailty syndrome: Implications and challenges for health care policy. Risk Manag. Healthc. Policy 2019, 12, 23–30. [Google Scholar] [CrossRef]
- Waldon, M. Frailty in older people: A principle-based concept analysis. Br. J. Community Nurs. 2018, 23, 482–494. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Kiesswetter, E.; Drey, M.; Sieber, C.C. Nutrition, frailty, and sarcopenia. Aging Clin. Exp. Res. 2017, 29, 43–48. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Number or |
|---|---|
| Median Value (Range) | |
| Age (years) | 66 (25, 94) |
| Gender, male/female | 165/191 |
| HCV/HBV/HCV and HBV/NBNC | 181/61/9/105 |
| Body mass index (kg/m2) | 22.7 (14.6, 41.4) |
| Walking speed (m/s) | 1.3 (0.2, 2.02) |
| Hand grip strength (kg, male) | 33.6 (13.6, 53.6) |
| Hand grip strength (kg, female) | 20.5 (6.0, 34.8) |
| Presence of LC, yes/no | 137/219 |
| Total bilirubin (mg/dL) | 0.8 (0.2, 5.1) |
| Serum albumin (g/dL) | 4.3 (2.0, 5.2) |
| Prothrombin time (%) | 91.2 (11.9, 122.9) |
| Platelet count (×104/mm3) | 17.5 (1.4, 51.4) |
| FIB-4 index | 2.16 (0.29, 30.98) |
| M2BPGi (cutoff index) | 1.255 (0.21, 11.93) |
| SMI (kg/m2, male) | 7.475 (5.21, 11.01) |
| SMI (kg/m2, female) | 5.875 (3.90, 8.17) |
| ECW to TBW ratio | 0.389 (0.367, 0.425) |
| AST (IU/L) | 25 (10, 222) |
| ALT (IU/L) | 19 (5, 232) |
| HbA1c (NGSP) | 5.7 (3.7, 12.6) |
| eGFR (ml/min/1.73 m2) | 81 (5, 173) |
| Serum zinc (μg/dL) | 73.9 (22.0, 124.6) |
| BTR | 5.65 (1.69, 13.82) |
| Serum ammonia (μg/dL) | 38 (12, 206) |
| r | p-Value | |
|---|---|---|
| Age | −0.3002 | <0.0001 |
| Body mass index | −0.02932 | 0.5825 |
| Total bilirubin | −0.07285 | 0.1702 |
| Serum albumin | 0.309146 | <0.0001 |
| Prothrombin time | 0.142872 | 0.0069 |
| Platelet count | 0.091789 | 0.0837 |
| AST | −0.06229 | 0.2411 |
| ALT | 0.02578 | 0.6278 |
| FIB-4 index | −0.17981 | 0.0007 |
| HbA1c (NGSP) | −0.05046 | 0.3459 |
| eGFR | 0.090435 | 0.0884 |
| SMI, male | 0.189214 | 0.0149 |
| SMI, female | 0.091065 | 0.2127 |
| ECW to TBW ratio | −0.41169 | <0.0001 |
| BTR | 0.252886 | <0.0001 |
| Serum zinc | 0.195912 | 0.0011 |
| Serum ammonia | −0.16623 | 0.0039 |
| M2BPGi | −0.2555 | <0.0001 |
| Variables | WS ≥ 0.8 m/s (n = 339) | WS < 0.8 m/s (n = 17) | p-Value |
|---|---|---|---|
| Age (years) | 65 (29, 94) | 71 (25, 83) | 0.0278 |
| Gender, male/female | 155/184 | 10/7 | 0.3265 |
| HBV/HCV/HBV and HCV/NBNC | 60/170/9/100 | 1/11/0/5 | 0.4852 |
| Body mass index (kg/m2) | 22.7 (14.6, 41.4) | 21.5 (17.7, 29.2) | 0.3367 |
| Presence of LC, yes/no | 125/214 | 12/5 | 0.0088 |
| Total bilirubin (mg/dL) | 0.8 (0.2, 5.1) | 0.9 (0.4, 3.2) | 0.7231 |
| Serum albumin (g/dL) | 4.3 (2.0, 5.2) | 4.0 (2.4, 4.6) | 0.0246 |
| Prothrombin time (%) | 91.4 (11.9, 122.9) | 84.7 (46.5, 103.9) | 0.1597 |
| Platelet count (×104/mm3) | 17.7 (1.4, 51.4) | 16.0 (2.8, 32.2) | 0.1401 |
| AST | 25 (12, 222) | 27 (10, 191) | 0.5570 |
| ALT | 19 (5, 206) | 16 (5, 232) | 0.2200 |
| M2BPGi | 1.24 (0.21, 11.93) | 2.31 (1.08, 10.82) | 0.0141 |
| eGFR (ml/min/1.73m2) | 81 (5, 173) | 76 (7, 99) | 0.0931 |
| HbA1c (NGSP) | 5.7 (3.7, 12.6) | 5.7 (4.6, 7.2) | 0.3573 |
| Serum ammonia (μg/dL) | 38 (12, 195) | 48 (18, 206) | 0.0534 |
| BTR | 5.71 (1.93, 13.82) | 3.92 (1.69, 8.8) | 0.0127 |
| Serum zinc (μg/dL) | 73.9 (22.0, 124.6) | 68.4 (38.0, 94.4) | 0.0764 |
| ECW to TBW ratio | 0.389 (0.367, 0.425) | 0.398 (0.387, 0.421) | <0.0001 |
| SMI decline, yes/no/unknown | 114/223/2 | 7/10/0 | 0.6024 |
| Multivariate Analysis | |||
|---|---|---|---|
| HR | 95% CI | p-Value | |
| Age # | 0.0267 | 9.251 × 10−5–7.700 | 0.1594 |
| Presence of LC | 0.779 | 0.109–5.589 | 0.8040 |
| Serum albumin # | 15.152 | 0.0548–4184.100 | 0.3333 |
| M2BPGi # | 0.764 | 0.0117–49.763 | 0.8998 |
| BTR # | 8.007 | 0.0614–1044.325 | 0.3874 |
| ECW to TBW ratio # | 0.00105 | 1.387 × 10−6–0.795 | 0.0398 |
| Variables | WS ≥ 1.0 m/s (n = 305) | WS < 1.0 m/s (n = 51) | p-Value |
|---|---|---|---|
| Age (years) | 64 (29, 90) | 73 (25, 94) | <0.0001 |
| Gender, male/female | 139/166 | 26/25 | 0.5446 |
| HBV/HCV/HBV and HCV/NBNC | 56/151/8/90 | 5/30/1/15 | 0.4421 |
| Body mass index (kg/m2) | 22.9 (14.8, 41.4) | 22.4 (14.6, 30.6) | 0.1246 |
| Presence of LC, yes/no | 109/196 | 28/23 | 0.0124 |
| Total bilirubin (mg/dL) | 0.8 (0.3, 5.1) | 0.9 (0.2, 3.8) | 0.9470 |
| Serum albumin (g/dL) | 4.3 (2.0, 5.1) | 4.1 (2.4, 5.2) | 0.0011 |
| Prothrombin time (%) | 91.4 (11.9, 122.9) | 88.9 (33.4, 122.5) | 0.1818 |
| Platelet count (×104/mm3) | 17.9 (1.4, 51.4) | 16.9 (2.8, 34.5) | 0.1531 |
| AST | 25 (12, 222) | 24 (10, 191) | 0.3413 |
| ALT | 20 (6, 206) | 17 (5, 232) | 0.6215 |
| M2BPGi | 1.2 (0.21, 11.93) | 2.18 (0.47, 10.82) | 0.0016 |
| eGFR (ml/min/1.73 m2) | 81 (5, 173) | 73 (7, 162) | 0.0709 |
| HbA1c (NGSP) | 5.7 (3.7, 12.6) | 5.7 (4.5, 9.8) | 0.5730 |
| Serum ammonia (μg/dL) | 38 (12, 195) | 40 (14, 206) | 0.7299 |
| BTR | 5.715 (1.93, 13.82) | 5.07 (1.69, 10.0) | 0.0289 |
| Serum zinc (μg/dL) | 74.2 (22.0, 124.6) | 69.5 (36.6, 118.2) | 0.1474 |
| ECW to TBW ratio | 0.389 (0.367, 0.425) | 0.398 (0.368, 0.421) | <0.0001 |
| SMI decline, yes/no/unknown | 94/209/2 | 27/24/0 | 0.0037 |
| Multivariate Analysis | |||
|---|---|---|---|
| HR | 95% CI | p-Value | |
| Age # | 0.0638 | 0.00205–1.989 | 0.0985 |
| Presence of LC | 0.973 | 0.320–2.957 | 0.9620 |
| SMI decline | 0.606 | 0.229–1.603 | 0.3132 |
| Serum albumin # | 2.596 | 0.0989–6.817 | 0.5665 |
| M2BPGi # | 0.887 | 0.0676–11.645 | 0.9275 |
| BTR # | 1.121 | 0.0760–16.540 | 0.9337 |
| ECW to TBW ratio # | 0.0284 | 0.000715–1.132 | 0.0556 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; Takata, R.; et al. Walking Speed: Japanese Data in Chronic Liver Diseases. J. Clin. Med. 2020, 9, 166. https://doi.org/10.3390/jcm9010166
Nishikawa H, Enomoto H, Yoh K, Iwata Y, Sakai Y, Kishino K, Ikeda N, Takashima T, Aizawa N, Takata R, et al. Walking Speed: Japanese Data in Chronic Liver Diseases. Journal of Clinical Medicine. 2020; 9(1):166. https://doi.org/10.3390/jcm9010166
Chicago/Turabian StyleNishikawa, Hiroki, Hirayuki Enomoto, Kazunori Yoh, Yoshinori Iwata, Yoshiyuki Sakai, Kyohei Kishino, Naoto Ikeda, Tomoyuki Takashima, Nobuhiro Aizawa, Ryo Takata, and et al. 2020. "Walking Speed: Japanese Data in Chronic Liver Diseases" Journal of Clinical Medicine 9, no. 1: 166. https://doi.org/10.3390/jcm9010166
APA StyleNishikawa, H., Enomoto, H., Yoh, K., Iwata, Y., Sakai, Y., Kishino, K., Ikeda, N., Takashima, T., Aizawa, N., Takata, R., Hasegawa, K., Ishii, N., Yuri, Y., Nishimura, T., Iijima, H., & Nishiguchi, S. (2020). Walking Speed: Japanese Data in Chronic Liver Diseases. Journal of Clinical Medicine, 9(1), 166. https://doi.org/10.3390/jcm9010166