Phase I Study of a B Cell-Based and Monocyte-Based Immunotherapeutic Vaccine, BVAC-C in Human Papillomavirus Type 16- or 18-Positive Recurrent Cervical Cancer


Abstract
1. Introduction
2. Methods
2.1. Patients and Eligibility Criteria
2.2. Preparation of BVAC-C
2.3. Treatment and Assessments
2.4. Immunological Response
2.4.1. Ex Vivo IFN-γ ELISPOT
2.4.2. Serum-Cytokine Analysis
2.4.3. Intracellular Staining
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. Adverse Events
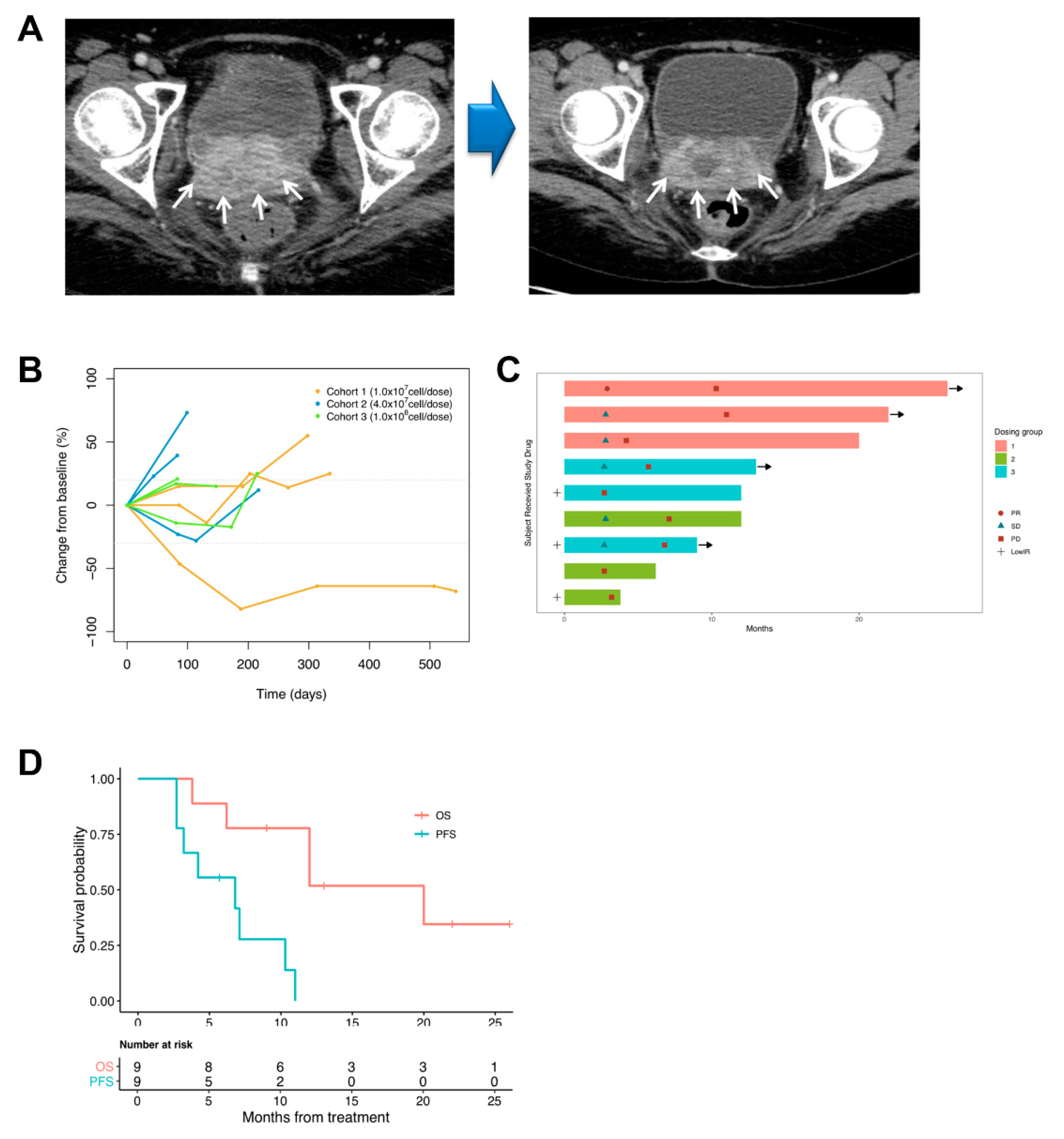
3.3. Tumor Response
3.4. Immunogenicity
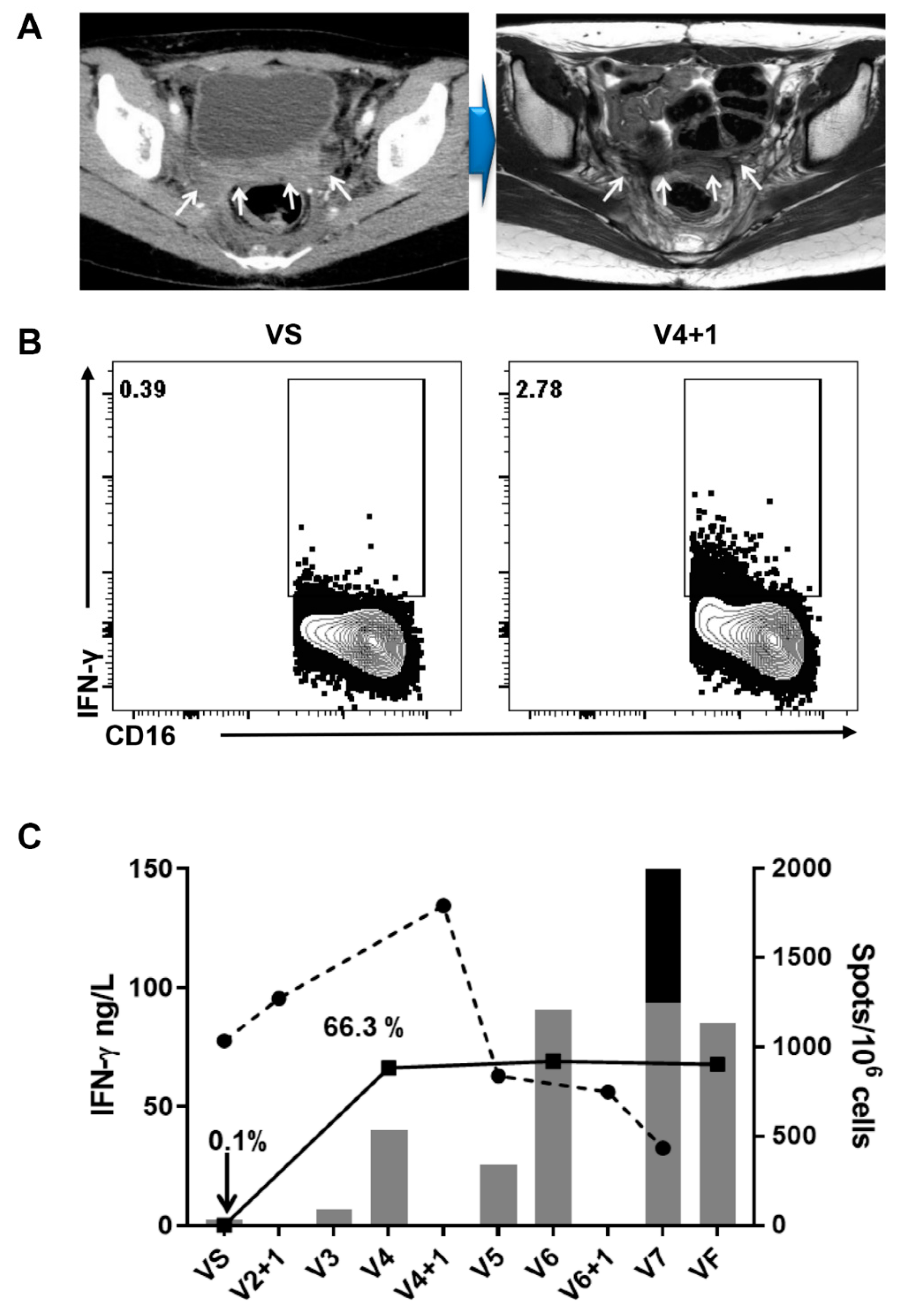
3.4.1. Serum-Cytokine Analysis and Intracellular Staining
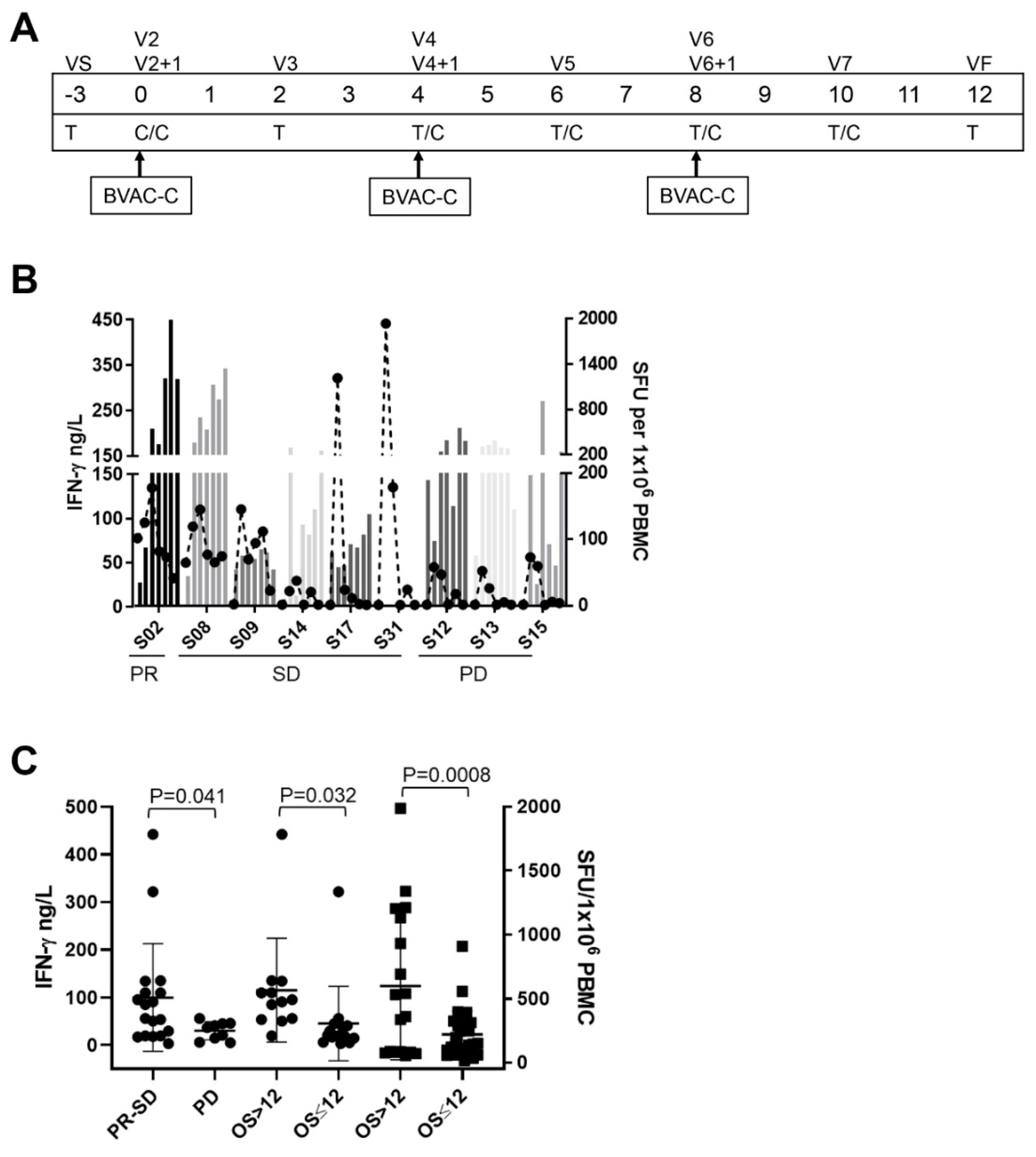
3.4.2. Ex Vivo IFN-γ ELISPOT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Monk, B.J.; Sill, M.W.; McMeekin, D.S.; Cohn, D.E.; Ramondetta, L.M.; Boardman, C.H.; Benda, J.; Cella, D. Phase III trial of four cisplatin-containing doublet combinations in stage IVB, recurrent, or persistent cervical carcinoma: A Gynecologic Oncology Group study. J. Clin. Oncol. 2009, 27, 4649–4655. [Google Scholar] [CrossRef]
- Moore, D.H.; Blessing, J.A.; McQuellon, R.P.; Thaler, H.T.; Cella, D.; Benda, J.; Miller, D.S.; Olt, G.; King, S.; Boggess, J.F.; et al. Phase III study of cisplatin with or without paclitaxel in stage IVB, recurrent, or persistent squamous cell carcinoma of the cervix: A gynecologic oncology group study. J. Clin. Oncol. 2004, 22, 3113–3119. [Google Scholar] [CrossRef]
- Tewari, K.S.; Sill, M.W.; Long, H.J.; Penson, R.T.; Huang, H.; Ramondetta, L.M.; Landrum, L.M.; Oaknin, A.; Reid, T.J.; Leitao, M.M.; et al. Improved survival with bevacizumab in advanced cervical cancer. N. Engl. J. Med. 2014, 370, 734–743. [Google Scholar] [CrossRef]
- Pfaendler, K.S.; Tewari, K.S. Changing paradigms in the systemic treatment of advanced cervical cancer. Am. J. Obstet. Gynecol. 2016, 214, 22–30. [Google Scholar] [CrossRef]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef]
- Topalian, S.L.; Sznol, M.; McDermott, D.F.; Kluger, H.M.; Carvajal, R.D.; Sharfman, W.H.; Brahmer, J.R.; Lawrence, D.P.; Atkins, M.B.; Powderly, J.D.; et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J. Clin. Oncol. 2014, 32, 1020–1030. [Google Scholar] [CrossRef]
- Frenel, J.S.; Le Tourneau, C.; O’Neil, B.; Ott, P.A.; Piha-Paul, S.A.; Gomez-Roca, C.; van Brummelen, E.M.J.; Rugo, H.S.; Thomas, S.; Saraf, S.; et al. Safety and Efficacy of Pembrolizumab in Advanced, Programmed Death Ligand 1-Positive Cervical Cancer: Results From the Phase Ib KEYNOTE-028 Trial. J. Clin. Oncol. 2017, 35, 4035–4041. [Google Scholar] [CrossRef]
- Walboomers, J.M.; Jacobs, M.V.; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K.V.; Snijders, P.J.; Peto, J.; Meijer, C.J.; Munoz, N. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J. Pathol. 1999, 189, 12–19. [Google Scholar] [CrossRef]
- Khallouf, H.; Grabowska, A.K.; Riemer, A.B. Therapeutic Vaccine Strategies against Human Papillomavirus. Vaccines (Basel) 2014, 2, 422–462. [Google Scholar] [CrossRef]
- Brun, J.L.; Dalstein, V.; Leveque, J.; Mathevet, P.; Raulic, P.; Baldauf, J.J.; Scholl, S.; Huynh, B.; Douvier, S.; Riethmuller, D.; et al. Regression of high-grade cervical intraepithelial neoplasia with TG4001 targeted immunotherapy. Am. J. Obstet. Gynecol. 2011, 204, e161–e168. [Google Scholar] [CrossRef]
- Kawana, K.; Adachi, K.; Kojima, S.; Kozuma, S.; Fujii, T. Therapeutic Human Papillomavirus (HPV) Vaccines: A Novel Approach. Open Virol. J. 2012, 6, 264–269. [Google Scholar] [CrossRef][Green Version]
- Morrow, M.P.; Yan, J.; Sardesai, N.Y. Human papillomavirus therapeutic vaccines: Targeting viral antigens as immunotherapy for precancerous disease and cancer. Expert Rev. Vaccines 2013, 12, 271–283. [Google Scholar] [CrossRef]
- Tran, N.P.; Hung, C.F.; Roden, R.; Wu, T.C. Control of HPV infection and related cancer through vaccination. Recent Results Cancer Res. 2014, 193, 149–171. [Google Scholar] [CrossRef]
- Chung, Y.; Kim, B.S.; Kim, Y.J.; Ko, H.J.; Ko, S.Y.; Kim, D.H.; Kang, C.Y. CD1d-restricted T cells license B cells to generate long-lasting cytotoxic antitumor immunity in vivo. Cancer Res. 2006, 66, 6843–6850. [Google Scholar] [CrossRef]
- Ko, H.J.; Lee, J.M.; Kim, Y.J.; Kim, Y.S.; Lee, K.A.; Kang, C.Y. Immunosuppressive myeloid-derived suppressor cells can be converted into immunogenic APCs with the help of activated NKT cells: An alternative cell-based antitumor vaccine. J. Immunol. 2009, 182, 1818–1828. [Google Scholar] [CrossRef]
- Kim, E.K.; Jeon, I.; Seo, H.; Park, Y.J.; Song, B.; Lee, K.A.; Jang, Y.; Chung, Y.; Kang, C.Y. Tumor-derived osteopontin suppresses antitumor immunity by promoting extramedullary myelopoiesis. Cancer Res. 2014, 74, 6705–6716. [Google Scholar] [CrossRef]
- Bae, E.A.; Seo, H.; Kim, B.S.; Choi, J.; Jeon, I.; Shin, K.S.; Koh, C.H.; Song, B.; Kim, I.K.; Min, B.S.; et al. Activation of NKT Cells in an Anti-PD-1-Resistant Tumor Model Enhances Antitumor Immunity by Reinvigorating Exhausted CD8 T Cells. Cancer Res. 2018, 78, 5315–5326. [Google Scholar] [CrossRef]
- Seo, H.; Jeon, I.; Kim, B.S.; Park, M.; Bae, E.A.; Song, B.; Koh, C.H.; Shin, K.S.; Kim, I.K.; Choi, K.; et al. IL-21-mediated reversal of NK cell exhaustion facilitates anti-tumour immunity in MHC class I-deficient tumours. Nat. Commun. 2017, 8, 15776. [Google Scholar] [CrossRef]
- Kitagawa, R.; Katsumata, N.; Shibata, T.; Kamura, T.; Kasamatsu, T.; Nakanishi, T.; Nishimura, S.; Ushijima, K.; Takano, M.; Satoh, T.; et al. Paclitaxel Plus Carboplatin Versus Paclitaxel Plus Cisplatin in Metastatic or Recurrent Cervical Cancer: The Open-Label Randomized Phase III Trial JCOG0505. J. Clin. Oncol. 2015, 33, 2129–2135. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patient ID | Dose (Cells) | HPV Type | Age | Histology | ECOG PS | * Prior Therapy | Metastases Location | Target Lesion Size (cm) |
|---|---|---|---|---|---|---|---|---|
| S02 | 1 × 107 | 16 | 34 | SCC | 1 | 1 | Pelvis | 2.8 |
| S04 | 1 × 107 | 18 | 62 | AD | 1 | 2 | Lung, Bone | 5.1 |
| S08 | 1 × 107 | 16 | 45 | SCC | 1 | 1 | LNs | 1.8 |
| S09 | 1 × 107 | 16 | 50 | SCC | 1 | 1 | Lung | 2.9 |
| S12 | 4 × 107 | 16 | 43 | AD | 1 | 3 | Lung, Peritoneal | 5.6 |
| S13 | 4 × 107 | 16 | 54 | SCC | 1 | 1 | LNs, Peritoneal | 9.2 |
| S14 | 4 × 107 | 16 | 43 | SCC | 1 | 2 | LNs | 7.9 |
| S15 | 1 × 108 | 16 | 35 | SCC | 1 | 1 | LNs, Liver, Pelvis | 9.6 |
| S16 | 1 × 108 | 16 | 35 | SCC | 1 | 2 | Pelvis, LNs, Lung | 7.1 |
| S31 | 1 × 108 | 16 | 62 | AD | 0 | 8 | Liver, Pelvis, Lung | 6.0 |
| S17 | 1 × 108 | 18 | 60 | AD | 1 | 5 | Lung | 1.1 |
| Adverse Events | 1 × 107 (n = 4) | 4 × 107 (n = 3) | 1 × 108 (n = 4) | Total, No. (N = 11, %) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| G1 | G2 | Total | G1 | G2 | Total | G1 | G2 | Total | G1 | G2 | Total | |
| Pyrexia | 1 | 0 | 1 | 2 | 0 | 2 | 3 | 0 | 3 | 6(55) | 0 | 6(55) |
| Chills | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 1(9) | 0 | 1(9) |
| Fatigue | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1(9) | 0 | 1(9) |
| Myalgia | 0 | 1 | 1 | 1 | 0 | 1 | 2 | 0 | 2 | 3(27) | 1(9) | 4(36) |
| Diarrhea | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1(9) | 1(9) |
| Vomiting | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 1(9) | 0 | 1(9) |
| Cytokine release syndrome | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1(9) | 1(9) |
| Headache | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 1(9) | 0 | 1(9) |
| Patient ID | Best Overall Response | PFS | OS | HPV-Specific T Cell b | IFN-γ ng/L c | TNF-α ng/L c |
|---|---|---|---|---|---|---|
| S02 | Partial response | 10.3 | 26 a | 1202 | 134.5 | 18.4 |
| S08 | Stable disease | 4.2 | 20 | 1337 | 110 | 62.2 |
| S09 | Stable disease | 11.0 | 22 a | 55 | 110.2 | 48.2 |
| S12 | Progressive disease | 3.2 | 3.8 | 382 | 45.1 | 49.1 |
| S13 | Progressive disease | 2.7 | 6.2 | 145 | 40.8 | 61.4 |
| S14 | Stable disease | 7.1 | 12 | 255 | 29.7 | 53.1 |
| S15 | Progressive disease | 2.7 | 12 | 247 | 56.2 | 89.7 |
| S31 | Stable disease | 5.7 | 13 a | NA | 441.9 | 281.7 |
| S17 | Stable disease | 6.8 | 9 a | 137 | 321.3 | 56.9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, C.H.; Choi, H.J.; Lee, J.-W.; Kang, E.-S.; Cho, D.; Park, B.K.; Kim, Y.-M.; Kim, D.-Y.; Seo, H.; Park, M.; et al. Phase I Study of a B Cell-Based and Monocyte-Based Immunotherapeutic Vaccine, BVAC-C in Human Papillomavirus Type 16- or 18-Positive Recurrent Cervical Cancer. J. Clin. Med. 2020, 9, 147. https://doi.org/10.3390/jcm9010147
Choi CH, Choi HJ, Lee J-W, Kang E-S, Cho D, Park BK, Kim Y-M, Kim D-Y, Seo H, Park M, et al. Phase I Study of a B Cell-Based and Monocyte-Based Immunotherapeutic Vaccine, BVAC-C in Human Papillomavirus Type 16- or 18-Positive Recurrent Cervical Cancer. Journal of Clinical Medicine. 2020; 9(1):147. https://doi.org/10.3390/jcm9010147
Chicago/Turabian StyleChoi, Chel Hun, Hyun Jin Choi, Jeong-Won Lee, Eun-Suk Kang, Duck Cho, Byung Kwan Park, Yong-Man Kim, Dae-Yeon Kim, Hyungseok Seo, Myunghwan Park, and et al. 2020. "Phase I Study of a B Cell-Based and Monocyte-Based Immunotherapeutic Vaccine, BVAC-C in Human Papillomavirus Type 16- or 18-Positive Recurrent Cervical Cancer" Journal of Clinical Medicine 9, no. 1: 147. https://doi.org/10.3390/jcm9010147
APA StyleChoi, C. H., Choi, H. J., Lee, J.-W., Kang, E.-S., Cho, D., Park, B. K., Kim, Y.-M., Kim, D.-Y., Seo, H., Park, M., Kim, W., Choi, K.-Y., Oh, T., Kang, C.-Y., & Kim, B.-G. (2020). Phase I Study of a B Cell-Based and Monocyte-Based Immunotherapeutic Vaccine, BVAC-C in Human Papillomavirus Type 16- or 18-Positive Recurrent Cervical Cancer. Journal of Clinical Medicine, 9(1), 147. https://doi.org/10.3390/jcm9010147