Growth Differentiation Factor-8 (GDF8)/Myostatin Is a Predictor of Troponin I Peak and a Marker of Clinical Severity after Acute Myocardial Infarction

 , and
, and
Abstract
1. Introduction
2. Methods
2.1. Patients
2.2. Data Collection
2.3. Determination of Serum GDF8
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
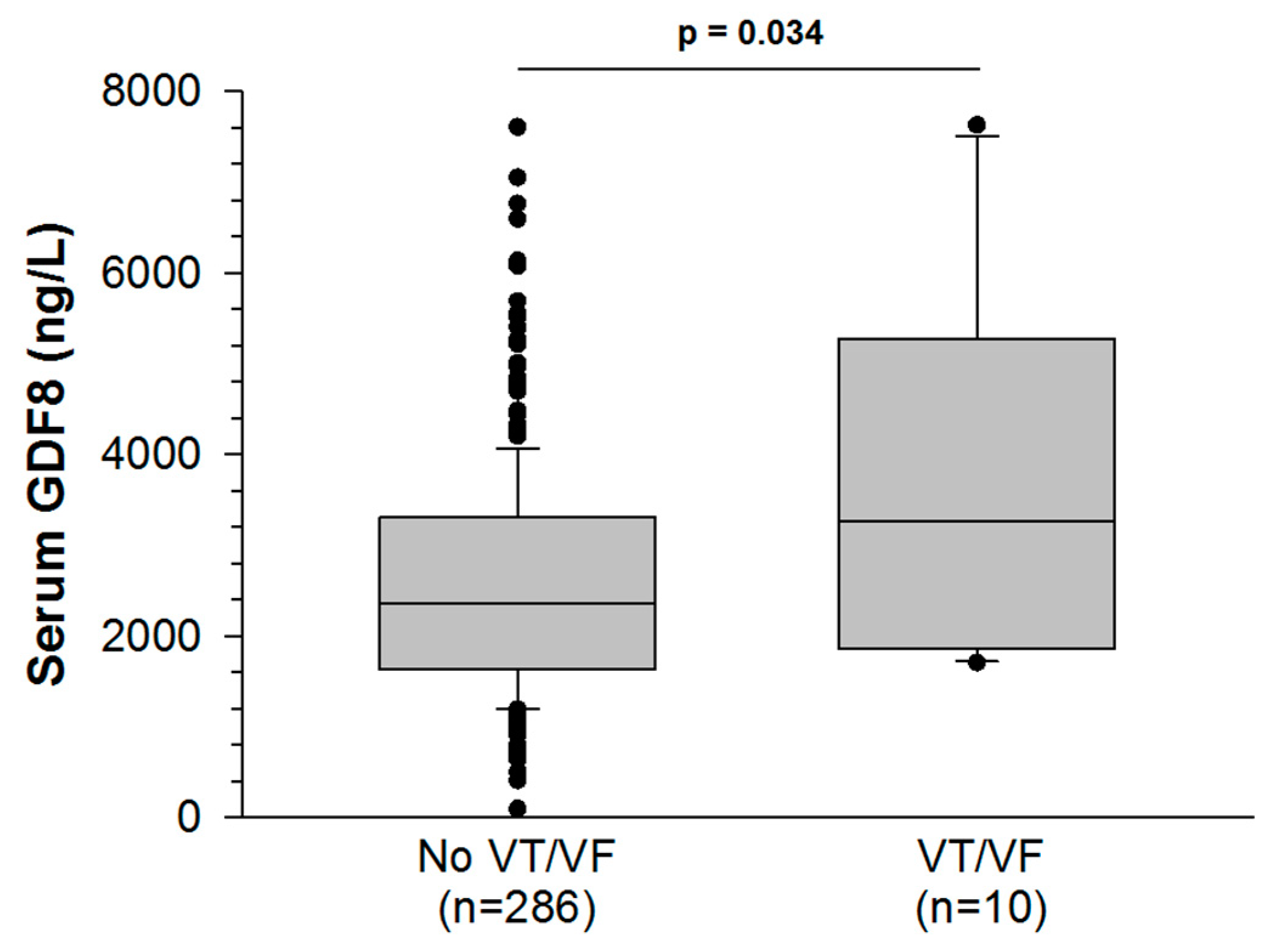
3.2. Associations between GDF8 Levels and in-Hospital Development of Ventricular Tachycardia or Fibrillation
3.3. Associations between GDF8 Levels and Peak Troponin Ic
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wollert, K.C.; Kempf, T.; Wallentin, L. Growth Differentiation Factor 15 as a Biomarker in Cardiovascular Disease. Clin Chem. 2017, 63, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.G.; Poggioli, T.; Katsimpardi, L.; Buchanan, S.M.; Oh, J.; Wattrus, S.; Heidecker, B.; Fong, Y.W.; Rubin, L.L.; Ganz, P.; et al. Biochemistry and Biology of GDF11 and Myostatin: Similarities, Differences, and Questions for Future Investigation. Circ. Res. 2016, 118, 1125–1141. [Google Scholar] [CrossRef] [PubMed]
- Rochette, L.; Zeller, M.; Cottin, Y.; Vergely, C. Growth and differentiation factor 11 (GDF11): Functions in the regulation of erythropoiesis and cardiac regeneration. Pharmacol. Ther. 2015, 156, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Argiles, J.M.; Orpi, M.; Busquets, S.; Lopez-Soriano, F.J. Myostatin: More than just a regulator of muscle mass. Drug Discov. Today 2012, 17, 702–709. [Google Scholar] [CrossRef]
- McPherron, A.C.; Lee, S.J. Double muscling in cattle due to mutations in the myostatin gene. Proc. Natl. Acad. Sci. USA 1997, 94, 12457–12461. [Google Scholar] [CrossRef]
- Mosher, D.S.; Quignon, P.; Bustamante, C.D.; Sutter, N.B.; Mellersh, C.S.; Parker, H.G.; Ostrander, E.A. A mutation in the myostatin gene increases muscle mass and enhances racing performance in heterozygote dogs. PLoS Genet. 2007, 3, e79. [Google Scholar] [CrossRef]
- Sharma, M.; Kambadur, R.; Matthews, K.G.; Somers, W.G.; Devlin, G.P.; Conaglen, J.V.; Fowke, P.J.; Bass, J.J. Myostatin, a transforming growth factor-beta superfamily member, is expressed in heart muscle and is upregulated in cardiomyocytes after infarct. J. Cell Physiol. 1999, 180, 1–9. [Google Scholar] [CrossRef]
- George, I.; Bish, L.T.; Kamalakkannan, G.; Petrilli, C.M.; Oz, M.C.; Naka, Y.; Lee Sweeney, H.; Maybaum, S. Myostatin activation in patients with advanced heart failure and after mechanical unloading. Eur. J. Heart Fail. 2010, 12, 444–453. [Google Scholar] [CrossRef]
- Bish, L.T.; George, I.; Maybaum, S.; Yang, J.; Chen, J.M.; Sweeney, H.L. Myostatin is elevated in congenital heart disease and after mechanical unloading. PLoS ONE 2011, 6, e23818. [Google Scholar] [CrossRef]
- Castillero, E.; Akashi, H.; Wang, C.; Najjar, M.; Ji, R.; Kennel, P.J.; Sweeney, H.L.; Schulze, P.C.; George, I. Cardiac myostatin upregulation occurs immediately after myocardial ischemia and is involved in skeletal muscle activation of atrophy. Biochem. Biophys. Res. Commun. 2015, 457, 106–111. [Google Scholar] [CrossRef][Green Version]
- Zeller, M.; Steg, P.G.; Ravisy, J.; Lorgis, L.; Laurent, Y.; Sicard, P.; Janin-Manificat, L.; Beer, J.C.; Makki, H.; Lagrost, A.C.; et al. Relation between body mass index, waist circumference, and death after acute myocardial infarction. Circulation 2008, 118, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D. Third universal definition of myocardial infarction. Circulation 2012, 126, 2020–2035. [Google Scholar] [CrossRef] [PubMed]
- Schafer, M.J.; Atkinson, E.J.; Vanderboom, P.M.; Kotajarvi, B.; White, T.A.; Moore, M.M.; Bruce, C.J.; Greason, K.L.; Suri, R.M.; Khosla, S.; et al. Quantification of GDF11 and Myostatin in Human Aging and Cardiovascular Disease. Cell Metab. 2016, 23, 1207–1215. [Google Scholar] [CrossRef] [PubMed]
- Szulc, P.; Schoppet, M.; Goettsch, C.; Rauner, M.; Dschietzig, T.; Chapurlat, R.; Hofbauer, L.C. Endocrine and clinical correlates of myostatin serum concentration in men--the STRAMBO study. J. Clin. Endocrinol. Metab. 2012, 97, 3700–3708. [Google Scholar] [CrossRef]
- Olson, K.A.; Beatty, A.L.; Heidecker, B.; Regan, M.C.; Brody, E.N.; Foreman, T.; Kato, S.; Mehler, R.E.; Singer, B.S.; Hveem, K.; et al. Association of growth differentiation factor 11/8, putative anti-ageing factor, with cardiovascular outcomes and overall mortality in humans: Analysis of the Heart and Soul and HUNT3 cohorts. Eur. Heart J. 2015, 36, 3426–3434. [Google Scholar] [CrossRef]
- Fife, E.; Kostka, J.; Kroc, L.; Guligowska, A.; Piglowska, M.; Soltysik, B.; Kaufman-Szymczyk, A.; Fabianowska-Majewska, K.; Kostka, T. Relationship of muscle function to circulating myostatin, follistatin and GDF11 in older women and men. BMC Geriatr. 2018, 18, 200. [Google Scholar] [CrossRef]
- Zhao, B.; Wall, R.J.; Yang, J. Transgenic expression of myostatin propeptide prevents diet-induced obesity and insulin resistance. Biochem. Biophys. Res. Commun. 2005, 337, 248–255. [Google Scholar] [CrossRef]
- Brandt, C.; Nielsen, A.R.; Fischer, C.P.; Hansen, J.; Pedersen, B.K.; Plomgaard, P. Plasma and muscle myostatin in relation to type 2 diabetes. PLoS ONE 2012, 7, e37236. [Google Scholar] [CrossRef]
- Hittel, D.S.; Berggren, J.R.; Shearer, J.; Boyle, K.; Houmard, J.A. Increased secretion and expression of myostatin in skeletal muscle from extremely obese women. Diabetes 2009, 58, 30–38. [Google Scholar] [CrossRef]
- Zhang, C.; McFarlane, C.; Lokireddy, S.; Bonala, S.; Ge, X.; Masuda, S.; Gluckman, P.D.; Sharma, M.; Kambadur, R. Myostatin-deficient mice exhibit reduced insulin resistance through activating the AMP-activated protein kinase signalling pathway. Diabetologia 2011, 54, 1491–1501. [Google Scholar] [CrossRef]
- Butcher, J.T.; Mintz, J.D.; Larion, S.; Qiu, S.; Ruan, L.; Fulton, D.J.; Stepp, D.W. Increased Muscle Mass Protects Against Hypertension and Renal Injury in Obesity. J. Am. Heart Assoc. 2018, 7, e009358. [Google Scholar] [CrossRef] [PubMed]
- Tu, P.; Bhasin, S.; Hruz, P.W.; Herbst, K.L.; Castellani, L.W.; Hua, N.; Hamilton, J.A.; Guo, W. Genetic disruption of myostatin reduces the development of proatherogenic dyslipidemia and atherogenic lesions in Ldlr null mice. Diabetes 2009, 58, 1739–1748. [Google Scholar] [CrossRef] [PubMed]
- Kesik, V.; Honca, T.; Gulgun, M.; Uysal, B.; Kurt, Y.G.; Cayci, T.; Babacan, O.; Gocgeldi, E.; Korkmazer, N. Myostatin as a Marker for Doxorubicin Induced Cardiac Damage. Ann. Clin. Lab. Sci. 2016, 46, 26–31. [Google Scholar] [PubMed]
- Biesemann, N.; Mendler, L.; Wietelmann, A.; Hermann, S.; Schafers, M.; Kruger, M.; Boettger, T.; Borchardt, T.; Braun, T. Myostatin regulates energy homeostasis in the heart and prevents heart failure. Circ. Res. 2014, 115, 296–310. [Google Scholar] [CrossRef]
- Heineke, J.; Auger-Messier, M.; Xu, J.; Sargent, M.; York, A.; Welle, S.; Molkentin, J.D. Genetic deletion of myostatin from the heart prevents skeletal muscle atrophy in heart failure. Circulation 2010, 121, 419–425. [Google Scholar] [CrossRef]
- Damatto, R.L.; Lima, A.R.; Martinez, P.F.; Cezar, M.D.; Okoshi, K.; Okoshi, M.P. Myocardial myostatin in spontaneously hypertensive rats with heart failure. Int. J. Cardiol. 2016, 215, 384–387. [Google Scholar] [CrossRef]
- Chen, P.; Liu, Z.; Luo, Y.; Chen, L.; Li, S.; Pan, Y.; Lei, X.; Wu, D.; Xu, D. Predictive value of serum myostatin for the severity and clinical outcome of heart failure. Eur. J. Intern. Med. 2019, 64, 33–40. [Google Scholar] [CrossRef]
- Lim, S.; McMahon, C.D.; Matthews, K.G.; Devlin, G.P.; Elston, M.S.; Conaglen, J.V. Absence of Myostatin Improves Cardiac Function Following Myocardial Infarction. Heart Lung Circ. 2018, 27, 693–701. [Google Scholar] [CrossRef]
- Flachskampf, F.A.; Schmid, M.; Rost, C.; Achenbach, S.; DeMaria, A.N.; Daniel, W.G. Cardiac imaging after myocardial infarction. Eur. Heart J. 2011, 32, 272–283. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar]


{kind=link}
| N (%) or Median (IQR) N = 296 | |
|---|---|
| Risk factors | |
| Age, y | 68 (58–78) |
| Female | 81 (27%) |
| BMI, kg/m² | 26 (24–30), n = 295 |
| Hypertension | 178 (60%) |
| Diabetes | 75 (25%) |
| Hypercholesterolemia | 117 (40%) |
| Family history of CAD | 74 (25%) |
| Current smoking | 85 (29%) |
| Cardiovascular history | |
| CAD | 53 (18%) |
| Stroke | 17 (6%) |
| Chronic kidney disease | 16 (5%) |
| Clinical data | |
| LVEF, % | 55 (50–60), n = 294 |
| LVEF <40% | 22 (7%) |
| HR, bpm | 76 (64–87), n = 283 |
| SBP, mmHg | 142 (123–165), n = 275 |
| DBP, mmHg | 82 (70–94), n = 274 |
| STEMI | 143 (48%) |
| HF | 56 (19%) |
| GRACE risk score | 141 (116–170), n = 268 |
| ICU length of stay, d | 3 (3–4), n = 290 |
| Coronary angiography | 294 (99%) |
| SYNTAX score | 12 (7–18), n = 284 |
| Multivessel disease | 184 (63%) |
| Percutaneous coronary intervention | 252 (86%) |
| Biological data | |
| GDF8 relative expression | 2375.0 (1640.0–3346.7) |
| CRP > 3 mg/L | 158 (54%) |
| Creatinine, µmol/L | 79 (68–95), n = 295 |
| eGFR CKD, mL/min | 82.7 (65.9–95.5), n = 295 |
| eGFR CKD < 45 mL/min | 34 (12%) |
| CK peak, UI/L | 583 (195–1483), n = 291 |
| Troponin Ic peak, ng/mL | 15.00 (3.21–70.00), n = 295 |
| Nt-ProBNP, pg/mL | 394 (93–1588), n = 295 |
| LDL cholesterol, g/L | 1.24 (0.92–1.53), n = 293 |
| HDL cholesterol, g/L | 0.50 (0.40–0.60), n = 293 |
| Total cholesterol, g/L | 2.06 (1.70–2.35), n = 293 |
| Triglycerides, g/L | 1.21 (0.84–1.76), n = 293 |
| Glycemia, mmol/L | 6.80 (5.80–8.63), n = 295 |
| In-hospital events | |
| Death | 7 (2%) |
| Cardiovascular death | 6 (2%) |
| Recurrent MI | 7 (2%) |
| Stroke | 2 (1%) |
| HF | 75 (26%) |
| VT or VF | 10 (3%) |
| Chronic medications | |
| Antiplatelet therapy | 24 (8%) |
| Aspirin | 72 (24%) |
| ARB | 63 (21%) |
| ACE inhibitor | 58 (20%) |
| Statin | 92 (31%) |
| Beta blocker | 83 (28%) |
| Diuretic | 57 (19%) |
| Acute medications | |
| Antiplatelet therapy | 283 (96%) |
| Aspirin | 290 (98%) |
| ARB | 36 (12%) |
| ACE inhibitor | 179 (60%) |
| Statin | 270 (91%) |
| Beta blocker | 207 (70%) |
| Diuretic | 65 (22%) |
| Patients (n = 296) | GDF8 Relative Expression or r | p Value | ||
|---|---|---|---|---|
| CV risk factors | ||||
| Age (years) | 68 (58–78) | −0.26 | <0.001 | |
| Female | Yes | 81 (27) | 2002 (1284–2785) | <0.001 |
| No | 215 (73) | 2554.9 (1759–3489) | ||
| BMI (kg/m²) | 26 (24–30) | 0.08 | 0.191 | |
| Hypertension | Yes | 178 (60) | 2247 (1532–3321) | 0.063 |
| No | 118 (40) | 2585 (1756–3381) | ||
| Diabetes | Yes | 75 (25) | 1946 (1429–2621) | <0.001 |
| No | 221 (75) | 2574 (1751–3526) | ||
| Hypercholesterolemia | Yes | 117 (40) | 2501 (1697–3397) | 0.396 |
| No | 179 (60) | 2311 (1621–3304) | ||
| Current smoking | Yes | 85 (29) | 2482 (1689–3396) | 0.306 |
| No | 211 (71) | 2256 (1633–3320) | ||
| Cardiovascular history | ||||
| CAD | Yes | 53 (18) | 2209 (1477–2991) | 0.189 |
| No | 243 (82) | 2426 (1688–3381) | ||
| Stroke | Yes | 17 (6) | 1742 (1070–2636) | 0.062 |
| No | 279 (94) | 2431 (1679–3372) | ||
| Chronic kidney disease | Yes | 16 (5) | 2712 (1315–3416) | 0.885 |
| No | 280 (95) | 2368 (1663–3346) | ||
| Clinical data | ||||
| LVEF | 55 (50–60) | −0.05 | 0.396 | |
| HR (bpm) | 76 (64–87) | −0.06 | 0.304 | |
| SBP (mmHg) | 142 (123–165) | 0.14 | 0.022 | |
| DBP (mmHg) | 82 (70–94) | 0.22 | <0.001 | |
| STEMI | Yes | 143 (48) | 2748 (1802–3445) | 0.001 |
| No | 153 (52) | 2141 (1519–2973) | ||
| Heart failure | Yes | 56 (19) | 2018 (1252–2775) | 0.006 |
| No | 238 (81) | 2511 (1695–3413) | ||
| GRACE risk score | 141 (116–170) | −0.22 | <0.001 | |
| ICU stay length (days) | 3 (3–4) | −0.01 | 0.877 | |
| Biological data | ||||
| CRP ≥ 3 mg/L | Yes | 158 (54) | 2102 (1471–3197) | <0.001 |
| No | 136 (46) | 2722 (1957–3525) | ||
| Creatinine clearance (CKD EPI) (mL/min) | 83 (66–96) | 0.15 | 0.010 | |
| CK peak (UI/L) | 583 (195–1493) | 0.26 | <0.001 | |
| Peak troponin Ic (ng/mL) | 15 (3–70) | 0.25 | <0.001 | |
| NT-proBNP (pg/mL) | 394 (93–1588) | −0.27 | <0.001 | |
| Glucose (mmol/L) | 7 (6–9) | −0.02 | 0.684 | |
| LDL cholesterol (g/L) | 1.2 (0.9–1.5) | 0.25 | <0.001 | |
| HDL cholesterol (g/L) | 0.5 (0.4–0.6) | 0.07 | 0.211 | |
| Triglycerides (g/L) | 1.2 (0.8–1.8) | 0.02 | 0.773 |
| GDF 8 ≤ 2400 ng/L N = 151 | GDF 8 > 2400 ng/L N = 145 | p Value | |
|---|---|---|---|
| In-hospital VF/VT | 3 (2.0%) | 7 (4.8%) | 0.211 |
| Troponin Ic peak, ng/mL | 8.30 (2.10–36.00) | 29.50 (4.22–92.75) | <0.001 |
| LVEF, % | 56 (50–60) | 55 (50–60) | 0.498 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Diabetes | 11.82 | −3.49–43.03 | 0.095 | 12.98 | 7.86–59.00 | 0.011 |
| Smoking | 11.34 | 0.78–45.40 | 0.043 | 13.19 | 10.32–62.28 | 0.006 |
| LVEF > 40% | 19.53 | 10.88–87.76 | 0.012 | 22.23 | 6.75–94.34 | 0.024 |
| GRACE risk score | 0.15 | 0.16–0.76 | 0.003 | 0.168 | 0.39–1.05 | <0.001 |
| Time to admission, per min | 0.01 | −0.02–0.00 | 0.065 | 0.01 | −0.02–0.01 | 0.233 |
| Log GDF8, per unit | 21.59 | 34.08–119.05 | <0.001 | 26.68 | 67.05–172.17 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meloux, A.; Rochette, L.; Maza, M.; Bichat, F.; Tribouillard, L.; Cottin, Y.; Zeller, M.; Vergely, C. Growth Differentiation Factor-8 (GDF8)/Myostatin Is a Predictor of Troponin I Peak and a Marker of Clinical Severity after Acute Myocardial Infarction. J. Clin. Med. 2020, 9, 116. https://doi.org/10.3390/jcm9010116
Meloux A, Rochette L, Maza M, Bichat F, Tribouillard L, Cottin Y, Zeller M, Vergely C. Growth Differentiation Factor-8 (GDF8)/Myostatin Is a Predictor of Troponin I Peak and a Marker of Clinical Severity after Acute Myocardial Infarction. Journal of Clinical Medicine. 2020; 9(1):116. https://doi.org/10.3390/jcm9010116
Chicago/Turabian StyleMeloux, Alexandre, Luc Rochette, Maud Maza, Florence Bichat, Laura Tribouillard, Yves Cottin, Marianne Zeller, and Catherine Vergely. 2020. "Growth Differentiation Factor-8 (GDF8)/Myostatin Is a Predictor of Troponin I Peak and a Marker of Clinical Severity after Acute Myocardial Infarction" Journal of Clinical Medicine 9, no. 1: 116. https://doi.org/10.3390/jcm9010116
APA StyleMeloux, A., Rochette, L., Maza, M., Bichat, F., Tribouillard, L., Cottin, Y., Zeller, M., & Vergely, C. (2020). Growth Differentiation Factor-8 (GDF8)/Myostatin Is a Predictor of Troponin I Peak and a Marker of Clinical Severity after Acute Myocardial Infarction. Journal of Clinical Medicine, 9(1), 116. https://doi.org/10.3390/jcm9010116