Multimodal Imaging Assessment of Vascular and Neurodegenerative Retinal Alterations in Type 1 Diabetic Patients without Fundoscopic Signs of Diabetic Retinopathy


 , ,
, ,  ,
, 

Abstract
1. Introduction
2. Methods
2.1. Structural SD-OCT Measurements
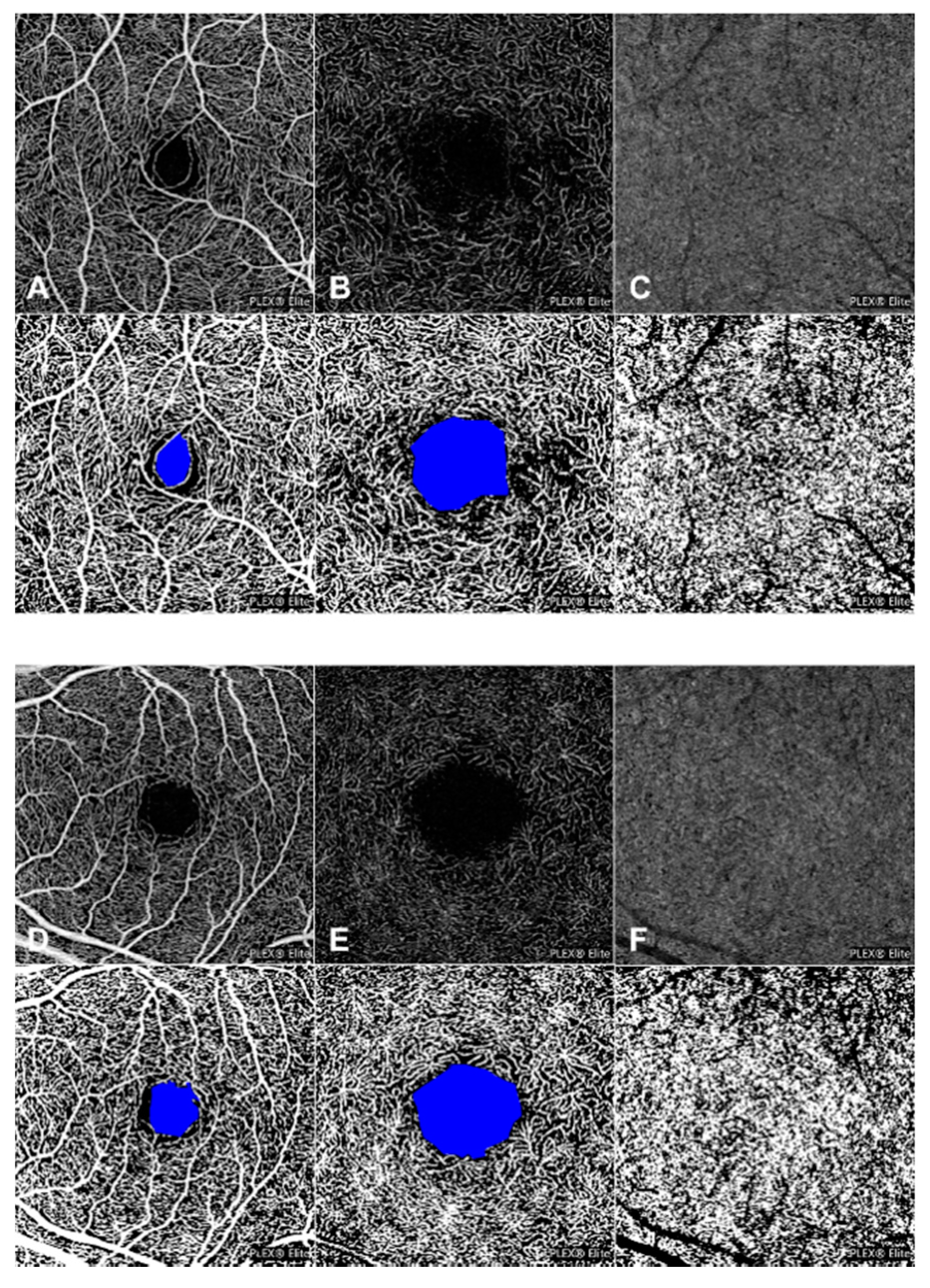
2.2. OCT-A Image Acquisition and Analysis
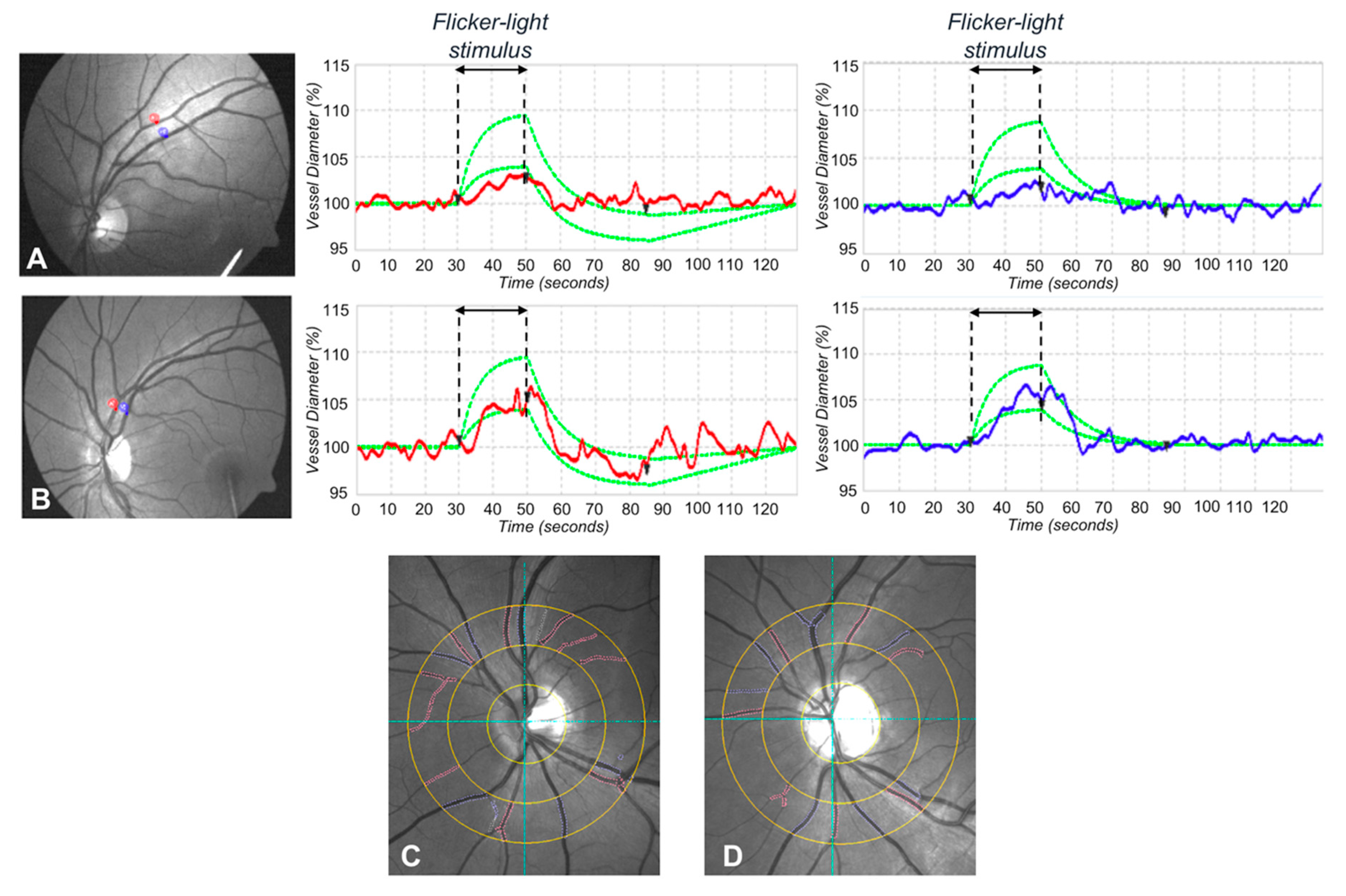
2.3. Dynamic Vessel Analysis
2.4. Static Vessel Analysis
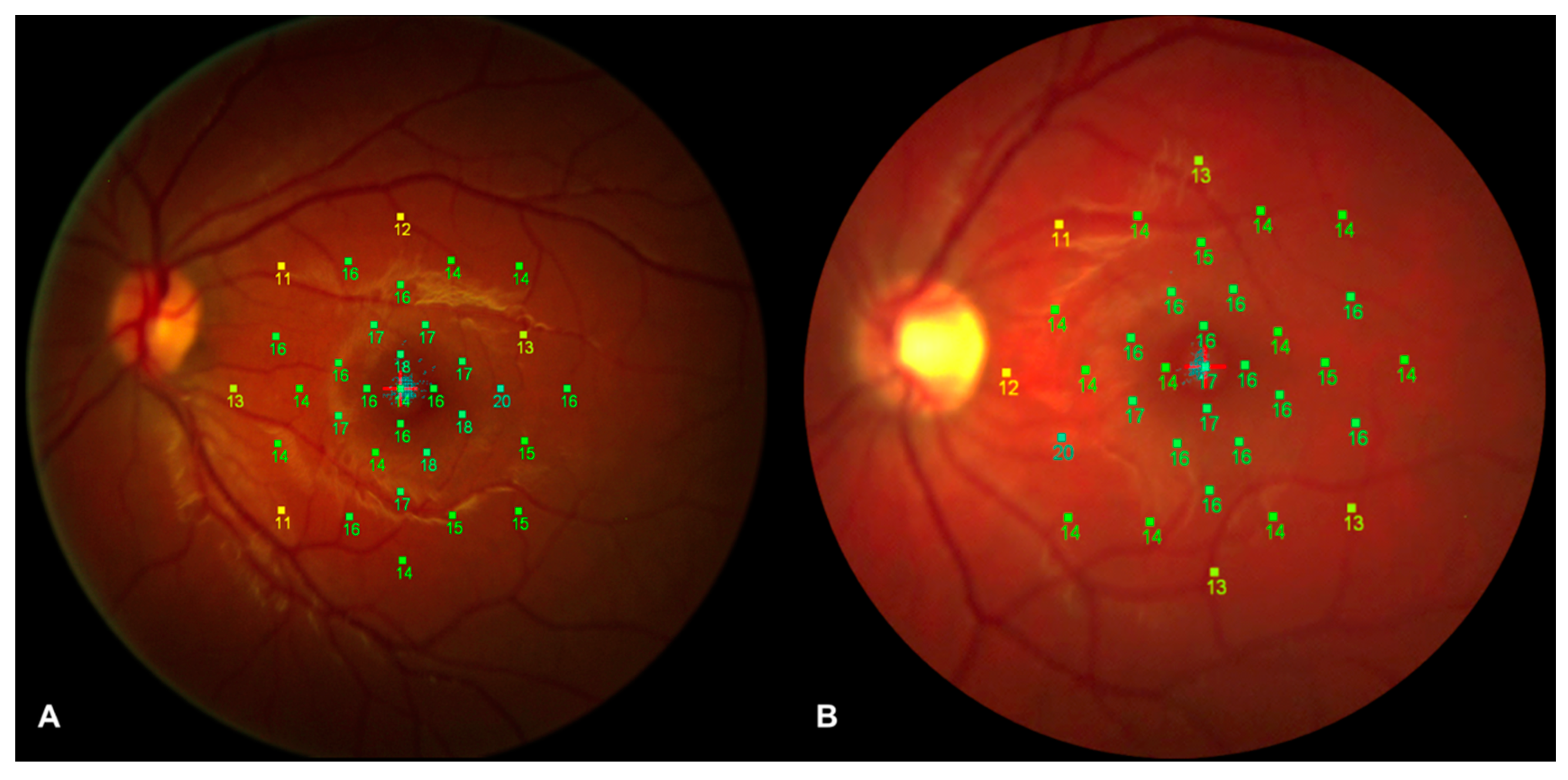
2.5. Microperimetry Assessment
2.6. Statistical Analysis
3. Results
3.1. Patients Demographics and Main Clinical Findings
3.2. Structural OCT Analysis
3.3. OCT-A Analysis
3.4. Dynamic Vessel Analysis
3.5. Static Vessel Analysis
3.6. Microperimetry Analysis
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Cheung, N.; Mitchell, P.; Wong, T.Y. Diabetic retinopathy. Lancet 2010, 376, 124–136. [Google Scholar] [CrossRef]
- Nazir, S.U.R.; Hassali, M.A.; Saleem, F.; Bashir, S.; Aljadhey, H. Disease related knowledge, medication adherence and glycaemic control among patients with type 2 diabetes mellitus in Pakistan. Prim. Care Diabetes 2016, 10, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Ogurtsova, K.; da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF diabetes atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Ajvazi, A.; Lutaj, P.; Goranci, I. Management of diabetic retinopathy, prevalence and clinical classification. Oftalmologia 2014, 58, 47–50. [Google Scholar] [PubMed]
- Early Treatment Diabetic Retinopathy Study Research Group. Photocoagulation for diabetic macular edema. Early treatment diabetic retinopathy study report number 1. Arch. Ophthalmol. 1985, 103, 1796–1806. [Google Scholar] [CrossRef]
- El-Fayoumi, D.; Badr Eldine, N.M.; Esmael, A.F.; Ghalwash, D.; Soliman, H.M. Retinal nerve fiber layer and ganglion cell complex thicknesses are reduced in children with type 1 Diabetes with no evidence of vascular retinopathy. Invest. Ophthalmol. Vis. Sci. 2016, 57, 5355–5360. [Google Scholar] [CrossRef]
- Simonett, J.M.; Scarinci, F.; Picconi, F.; Giorno, P.; De Geronimo, D.; Di Renzo, A.; Varano, M.; Frontoni, S.; Parravano, M. Early microvascular retinal changes in optical coherence tomography angiography in patients with type 1 diabetes mellitus. Acta Ophthalmol. 2017, 95, e751–e755. [Google Scholar] [CrossRef] [PubMed]
- Carnevali, A.; Sacconi, R.; Corbelli, E.; Tomasso, L.; Querques, L.; Zerbini, G.; Scorcia, V.; Bandello, F.; Querques, G. Optical coherence tomography angiography analysis of retinal vascular plexuses and choriocapillaris in patients with type 1 diabetes without diabetic retinopathy. Acta Diabetol. 2017, 54, 695–702. [Google Scholar] [CrossRef]
- Cao, D.; Yang, D.; Huang, Z.; Zeng, Y.; Wang, J.; Hu, Y.; Zhang, L. Optical coherence tomography angiography discerns preclinical diabetic retinopathy in eyes of patients with type 2 diabetes without clinical diabetic retinopathy. Acta Diabetol. 2018, 55, 469–477. [Google Scholar] [CrossRef]
- Garhofer, G.; Bek, T.; Boehm, A.G.; Gherghel, D.; Grunwald, J.; Jeppesen, P.; Kergoat, H.; Kotliar, K.; Lanzl, I.; Lovasik, J.V.; et al. Use of the retinal vessel analyzer in ocular blood flow research. Acta Ophthalmol. 2010, 88, 717–722. [Google Scholar] [CrossRef]
- Hwang, T.S.; Jia, Y.; Gao, S.S.; Bailey, S.T.; Lauer, A.K.; Flaxel, C.J.; Wilson, D.J.; Huang, D. Optical coherence tomography angiography features of diabetic retinopathy. Retina 2015, 35, 2371–2376. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, H.W.; Verbraak, F.D.; Kok, P.H.; Stehouwer, M.; Garvin, M.K.; Sonka, M.; DeVries, J.H.; Schlingemann, R.O.; Abramoff, M.D. Early neurodegeneration in the retina of type 2 diabetic patients. Invest. Ophthalmol. Vis. Sci. 2012, 53, 2715–2719. [Google Scholar] [CrossRef] [PubMed]
- Vujosevic, S.; Midena, E. Retinal layers changes in human preclinical and early clinical diabetic retinopathy support early retinal neuronal and Muller cells alterations. J. Diabetes Res. 2013, 2013, 905058. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.T.; Proença, R.; Alves, M.; Dias-Santos, A.; Santos, B.O.; Cunha, J.P.; Papoila, A.L.; Pinto, L.A. Retina and choroid of diabetic patients without observed retinal vascular changes: A longitudinal study. Am. J. Ophthalmol. 2017, 176, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Dimitrova, G.; Chihara, E.; Takahashi, H.; Amano, H.; Okazaki, K. Quantitative retinal optical coherence tomography angiography in patients with diabetes without diabetic retinopathy. Invest. Ophthalmol. Vis. Sci. 2017, 58, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Salz, D.A.; Talisa, E.; Adhi, M.; Moult, E.; Choi, W.; Baumal, C.R.; Witkin, A.J.; Duker, J.S.; Fujimoto, J.G.; Waheed, N.K. Select features of diabetic retinopathy on swept-source optical coherence tomographic angiography compared with fluorescein angiography and normal eyes. JAMA Ophthalmol. 2016, 134, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.Y.; Chu, Z.; Shahidzadeh, A.; Wang, R.K.; Puliafito, C.A.; Kashani, A.H. Quantifying microvascular density and morphology in diabetic retinopathy using spectral-domain optical coherence tomography angiography. Invest. Ophthalmol. Vis. Sci. 2016, 57, OCT362–OCT370. [Google Scholar] [CrossRef]
- Hwang, T.S.; Gao, S.S.; Liu, L.; Lauer, A.K.; Bailey, S.T.; Flaxel, C.J.; Wilson, D.J.; Huang, D.; Jia, Y. Automated quantification of capillary nonperfusion using optical coherence tomography angiography in diabetic retinopathy. JAMA Ophthalmol. 2016, 134, 367–373. [Google Scholar] [CrossRef]
- Ting, D.S.W.; Tan, G.S.W.; Agrawal, R.; Yanagi, Y.; Sie, N.M.; Wong, C.W.; San Yeo, I.Y.; Lee, S.Y.; Cheung, C.M.G.; Wong, T.Y. Optical coherence tomographic angiography in type 2 diabetes and diabetic retinopathy. JAMA Ophthalmol. 2017, 135, 306–312. [Google Scholar] [CrossRef]
- Rohrschneider, K.; Bultmann, S.; Springer, C. Use of fundus perimetry (microperimetry) to quantify macular sensitivity. Prog. Retin. Eye Res. 2008, 27, 536–548. [Google Scholar] [CrossRef]
- Newman, E.A. Functional hyperemia and mechanisms of neurovascular coupling in the retinal vasculature. J. Cereb. Blood Flow Metab. 2013, 33, 1685–1695. [Google Scholar] [CrossRef]
- Sacconi, R.; Corbelli, E.; Carnevali, A.; Querques, L.; Bandello, F.; Querques, G. Optical coherence tomography angiography in geographic atrophy. Retina 2018, 38, 2350–2355. [Google Scholar] [CrossRef] [PubMed]
- Sacconi, R.; Borrelli, E.; Corbelli, E.; Capone, L.; Rabiolo, A.; Carnevali, A.; Casaluci, M.; Gelormini, F.; Querques, L.; Bandello, F.; et al. Quantitative changes in the ageing choriocapillaris as measured by swept source optical coherence tomography angiography. Br. J. Ophthalmol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Polak, K.; Schmetterer, L.; Riva, C.E. Influence of flicker frequency on flicker-induced changes of retinal vessel diameter. Invest. Ophthalmol. Vis. Sci. 2002, 43, 2721–2726. [Google Scholar] [PubMed]
- Riva, C.E.; Falsini, B.; Logean, E. Flicker-evoked responses of human optic nerve head blood flow: Luminance versus chromatic modulation. Invest. Ophthalmol. Vis. Sci. 2001, 42, 756–762. [Google Scholar]
- Falsini, B.; Riva, C.E.; Logean, E. Flicker-evoked changes in human optic nerve blood flow: Relationship with retinal neural activity. Invest. Ophthalmol. Vis. Sci. 2002, 43, 2309–2316. [Google Scholar]
- Kotliar, K.E.; Vilser, W.; Nagel, E.; Lanzl, I.M. Retinal vessel reaction in response to chromatic flickering light. Graefes Arch. Clin. Exp. Ophthalmol. 2004, 242, 377–392. [Google Scholar] [CrossRef]
- Zeng, Y.; Cao, D.; Yu, H.; Yang, D.; Zhuang, X.; Hu, Y.; Li, J.; Yang, J.; Wu, Q.; Liu, B.; et al. Early retinal neurovascular impairment in patients with diabetes without clinically detectable retinopathy. Br. J. Ophthalmol. 2019. [Google Scholar] [CrossRef]
- Song, S.H. Complication characteristics between young-onset type 2 versus type 1 diabetes in a UK population. BMJ Open Diabetes Res. Care 2015, 3, e000044. [Google Scholar] [CrossRef]
- Talisa, E.; Chin, A.T.; Bonini Filho, M.A.; Adhi, M.; Branchini, L.; Salz, D.A.; Baumal, C.R.; Crawford, C.; Reichel, E.; Witkin, A.J.; et al. Detection of microvascular changes in eyes of patients with diabetes but not clinical diabetic retinopathy using optical coherence tomography angiography. Retina 2015, 35, 2364–2370. [Google Scholar]
- Scarinci, F.; Picconi, F.; Giorno, P.; Boccassini, B.; De Geronimo, D.; Varano, M.; Frontoni, S.; Parravano, M. Deep capillary plexus impairment in patients with type 1 diabetes mellitus with no signs of diabetic retinopathy revealed using optical coherence tomography angiography. Acta Ophthalmol. 2018, 96, e264–e265. [Google Scholar] [CrossRef]
- Picconi, F.; Parravano, M.; Ylli, D.; Pasqualetti, P.; Coluzzi, S.; Giordani, I.; Malandrucco, I.; Lauro, D.; Scarinci, F.; Giorno, P.; et al. Retinal neurodegeneration in patients with type 1 diabetes mellitus: The role of glycemic variability. Acta Diabetol. 2017, 54, 489–497. [Google Scholar] [CrossRef]
- Liu, H.; Tang, J.; Du, Y.; Saadane, A.; Samuels, I.; Veenstra, A.; Kiser, J.Z.; Palczewski, K.; Kern, T.S. Transducin 1, phototransduction and the development of early diabetic retinopathy. Invest. Ophthalmol. Vis. Sci. 2019, 60, 1538–1546. [Google Scholar] [CrossRef]
- Lim, L.S.; Ling, L.H.; Ong, P.G.; Foulds, W.; Tai, E.S.; Wong, E.; Lee, S.Y.; Wong, D.; Cheung, C.M.G.; Wong, T.Y. Dynamic responses in retinal vessel caliber with flicker light stimulation in eyes with diabetic retinopathy. Invest. Ophthalmol. Vis. Sci. 2014, 55, 5207–5213. [Google Scholar] [CrossRef]
- Zonta, M.; Angulo, M.C.; Gobbo, S.; Rosengarten, B.; Hossmann, K.A.; Pozzan, T.; Carmignoto, G. Neuron-to-astrocyte signaling is central to the dynamic control of brain microcirculation. Nat. Neurosci. 2003, 6, 43–50. [Google Scholar] [CrossRef]
- Takano, T.; Tian, G.F.; Peng, W.; Lou, N.; Libionka, W.; Han, X.; Nedergaard, M. Astrocyte-Mediated control of cerebral blood flow. Nat. Neurosci. 2006, 9, 260–267. [Google Scholar] [CrossRef]
- Metea, M.R.; Newman, E.A. Glial cells dilate and constrict blood vessels: A mechanism of neurovascular coupling. J. Neurosci. 2006, 26, 2862–2870. [Google Scholar] [CrossRef]
- Werblin, F.S.; Dowling, J.E. Organization of the retina of the mudpuppy, Necturus maculosus. II. Intracellular recording. J. Neurophysiol. 1969, 32, 339–355. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Diabetic Eyes (n = 34) | Control Eyes (n = 32) | p Value | |
|---|---|---|---|
| Gender (male/female) | 18/16 | 16/16 | 0.811 * |
| DM duration (mean ± SD), years | 12 ± 4 | \ | \ |
| HbA1c, % | 7.6 ± 0.7 | \ | \ |
| Age (mean ± SD), years | 21 ± 2 | 22 ± 2 | 0.141 + |
| BCVA (mean ± SD), LogMAR | 0 ± 0 | 0 ± 0 | 1.000 + |
| CMT (mean ± SD), µm | 277 ± 16 | 273 ± 17 | 0.285 + |
| Subfoveal ChT (mean ± SD), µm | 299 ± 62 | 280 ± 81 | 0.443 + |
| Subfield Analyzed | Diabetic Eyes (n = 34) | Control Eyes (n = 32) | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | p Value * | |
| GCC thickness (µm) | |||
| 1-mm central circle | 16.1 ± 3.3 | 15.7 ± 3.3 | 0.653 |
| 3-mm S subfield | 54.9 ± 5.8 | 54.6 ± 3.4 | 0.789 |
| 6-mm S subfield | 37.5 ± 3.2 | 34.9 ± 3.1 | 0.001 |
| 3-mm I subfield | 53.8 ± 5.2 | 53.6 ± 3.3 | 0.854 |
| 6-mm I subfield | 37.2 ± 4.8 | 34.9 ± 3.2 | 0.025 |
| 3-mm N subfield | 54.2 ± 5.0 | 52.9 ± 3.5 | 0.229 |
| 6-mm N subfield | 40.0 ± 4.1 | 38.7 ± 3.3 | 0.167 |
| 3-mm T subfield | 49.3 ± 6.0 | 49.9 ± 4.2 | 0.651 |
| 6-mm T subfield | 39.6 ± 4.7 | 36.5 ± 3.5 | 0.004 |
| Macular RNFL thickness (µm) | |||
| 1-mm central circle | 12.7 ± 1.7 | 12.6 ± 1.3 | 0.832 |
| 3-mm S subfield | 24.2 ± 3.1 | 23.6 ± 3.0 | 0.390 |
| 6-mm S subfield | 36.9 ± 5.0 | 35.6 ± 4.4 | 0.262 |
| 3-mm I subfield | 24.5 ± 2.4 | 24.1 ± 2.5 | 0.477 |
| 6-mm I subfield | 39.9 ± 6.7 | 37.7 ± 5.3 | 0.130 |
| 3-mm N subfield | 21.2 ± 1.9 | 20.7 ± 1.8 | 0.227 |
| 6-mm N subfield | 50.5 ± 6.4 | 48.6 ± 6.8 | 0.240 |
| 3-mm T subfield | 16.2 ± 0.9 | 16.0 ± 1.1 | 0.334 |
| 6-mm T subfield | 17.7 ± 0.9 | 17.9 ± 1.2 | 0.332 |
| Peripapillary RNFL thickness (µm) | |||
| G | 87.7 ± 8.0 | 88.0 ± 9.8 | 0.912 |
| N subfield | 67.7 ± 9.5 | 73.6 ± 15.1 | 0.234 |
| NS subfield | 102.4 ± 17.9 | 100.6 ± 22.8 | 0.720 |
| TS subfield | 116.3 ± 25.1 | 121.0 ± 19.1 | 0.415 |
| T subfield | 67.0 ± 9.9 | 66.2 ± 15.6 | 0.798 |
| TI subfield | 126.1 ± 26.0 | 132.3 ± 19.8 | 0.297 |
| NI subfield | 100.6 ± 24.9 | 93.6 ± 24.7 | 0.268 |
| Subfield Analyzed | Diabetic Eyes (n = 34) | Control Eyes (n = 32) | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | p Value * | |
| OPL thickness (µm) | |||
| 1-mm central circle | 26.8 ± 4.9 | 25.9 ± 4.3 | 0.475 |
| 3-mm S subfield | 38.0 ± 8.8 | 35.0 ± 9.9 | 0.179 |
| 6-mm S subfield | 27.9 ± 2.8 | 26.0 ± 3.1 | 0.015 |
| 3-mm I subfield | 31.5 ± 4.0 | 30.7 ± 6.5 | 0.599 |
| 6-mm I subfield | 26.5 ± 1.7 | 24.9 ± 1.8 | 0.001 |
| 3-mm N subfield | 32.8 ± 7.7 | 30.3 ± 4.7 | 0.133 |
| 6-mm N subfield | 28.4 ± 2.9 | 26.4 ± 2.7 | 0.007 |
| 3-mm T subfield | 33.8 ± 5.8 | 34.4 ± 7.0 | 0.713 |
| 6-mm T subfield | 27.9 ± 2.1 | 26.9 ± 3.1 | 0.132 |
| ONL thickness (µm) | |||
| 1-mm central circle | 91.5 ± 9.3 | 88.7 ± 11.1 | 0.274 |
| 3-mm S subfield | 67.8 ± 11.2 | 65.7 ± 12.0 | 0.474 |
| 6-mm S subfield | 63.4 ± 7.4 | 61.2 ± 8.1 | 0.242 |
| 3-mm I subfield | 72.7 ± 7.8 | 69.2 ± 9.0 | 0.100 |
| 6-mm I subfield | 58.1 ± 7.4 | 55.4 ± 7.3 | 0.147 |
| 3-mm N subfield | 75.1 ± 11.4 | 74.5 ± 11.2 | 0.834 |
| 6-mm N subfield | 61.1 ± 7.5 | 59.5 ± 8.9 | 0.438 |
| 3-mm T subfield | 71.5 ± 10.5 | 66.6 ± 10.3 | 0.061 |
| 6-mm T subfield | 61.4 ± 7.9 | 56.8 ± 7.1 | 0.017 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sacconi, R.; Casaluci, M.; Borrelli, E.; Mulinacci, G.; Lamanna, F.; Gelormini, F.; Carnevali, A.; Querques, L.; Zerbini, G.; Bandello, F.; et al. Multimodal Imaging Assessment of Vascular and Neurodegenerative Retinal Alterations in Type 1 Diabetic Patients without Fundoscopic Signs of Diabetic Retinopathy. J. Clin. Med. 2019, 8, 1409. https://doi.org/10.3390/jcm8091409
Sacconi R, Casaluci M, Borrelli E, Mulinacci G, Lamanna F, Gelormini F, Carnevali A, Querques L, Zerbini G, Bandello F, et al. Multimodal Imaging Assessment of Vascular and Neurodegenerative Retinal Alterations in Type 1 Diabetic Patients without Fundoscopic Signs of Diabetic Retinopathy. Journal of Clinical Medicine. 2019; 8(9):1409. https://doi.org/10.3390/jcm8091409
Chicago/Turabian StyleSacconi, Riccardo, Marco Casaluci, Enrico Borrelli, Giacomo Mulinacci, Francesca Lamanna, Francesco Gelormini, Adriano Carnevali, Lea Querques, Gianpaolo Zerbini, Francesco Bandello, and et al. 2019. "Multimodal Imaging Assessment of Vascular and Neurodegenerative Retinal Alterations in Type 1 Diabetic Patients without Fundoscopic Signs of Diabetic Retinopathy" Journal of Clinical Medicine 8, no. 9: 1409. https://doi.org/10.3390/jcm8091409
APA StyleSacconi, R., Casaluci, M., Borrelli, E., Mulinacci, G., Lamanna, F., Gelormini, F., Carnevali, A., Querques, L., Zerbini, G., Bandello, F., & Querques, G. (2019). Multimodal Imaging Assessment of Vascular and Neurodegenerative Retinal Alterations in Type 1 Diabetic Patients without Fundoscopic Signs of Diabetic Retinopathy. Journal of Clinical Medicine, 8(9), 1409. https://doi.org/10.3390/jcm8091409