Chronic Use of Proton-Pump Inhibitors and Iron Status in Renal Transplant Recipients

 ,
,  ,
, 
 ,
,
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Exposure Definition
2.3. Study Approval
2.4. Clinical Measurements and Iron Status Parameters
2.5. Assessment of Dietary Iron Intake
2.6. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Association of PPI Use with Iron Status Parameters
3.3. Association of PPI Use with ID
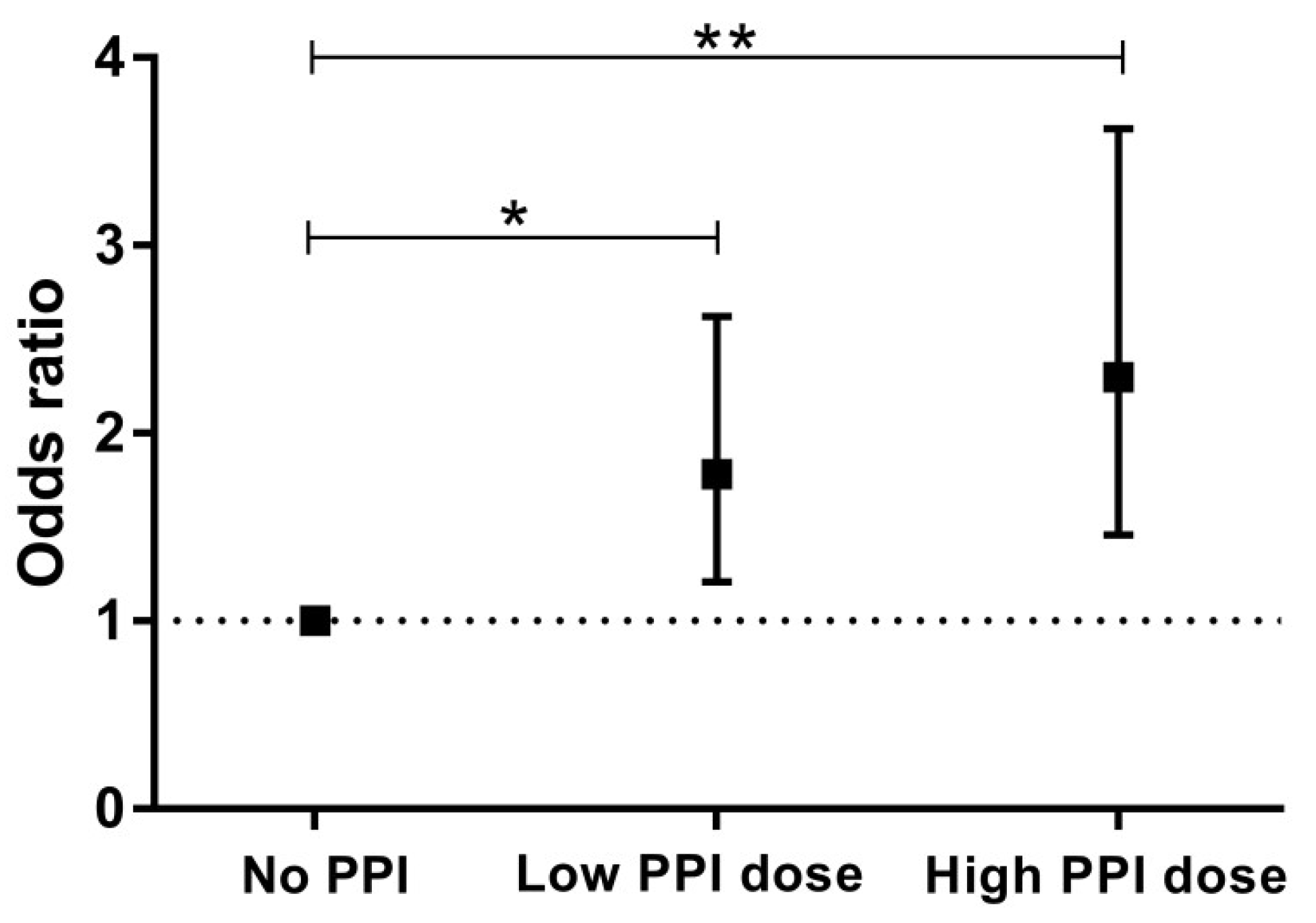
3.4. Dose-Response Analyses
3.5. Sensitivity Analyses for Risk of ID
3.6. Description of Excluded RTR Receiving Oral Iron Supplementation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lorenz, M.; Kletzmayr, J.; Perschl, A.; Furrer, A.; Horl, W.H.; Sunder-Plassmann, G. Anemia and iron deficiencies among long-term renal transplant recipients. J. Am. Soc. Nephrol. 2002, 13, 794–797. [Google Scholar] [PubMed]
- Yorgin, P.D.; Scandling, J.D.; Belson, A.; Sanchez, J.; Alexander, S.R.; Andreoni, K.A. Late post-transplant anemia in adult renal transplant recipients. An under-recognized problem? Am. J. Transplant. 2002, 2, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Eisenga, M.F.; Minovic, I.; Berger, S.P.; Kootstra-Ros, J.E.; van den Berg, E.; Riphagen, I.J.; Navis, G.; van der Meer, P.; Bakker, S.J.; Gaillard, C.A. Iron deficiency, anemia, and mortality in renal transplant recipients. Transpl. Int. 2016, 29, 1176–1183. [Google Scholar] [CrossRef] [PubMed]
- Imoagene-Oyedeji, A.E.; Rosas, S.E.; Doyle, A.M.; Goral, S.; Bloom, R.D. Posttransplantation anemia at 12 months in kidney recipients treated with mycophenolate mofetil: Risk factors and implications for mortality. J. Am. Soc. Nephrol. 2006, 17, 3240–3247. [Google Scholar] [CrossRef] [PubMed]
- Lim, A.K.H.; Kansal, A.; Kanellis, J. Factors associated with anaemia in kidney transplant recipients in the first year after transplantation: A cross-sectional study. BMC Nephrol. 2018, 19, 252. [Google Scholar] [CrossRef] [PubMed]
- Jones, H.; Talwar, M.; Nogueira, J.M.; Ugarte, R.; Cangro, C.; Rasheed, H.; Klassen, D.K.; Weir, M.R.; Haririan, A. Anemia after kidney transplantation; its prevalence, risk factors, and independent association with graft and patient survival: A time-varying analysis. Transplantation 2012, 93, 923–928. [Google Scholar] [CrossRef] [PubMed]
- Chhabra, D.; Grafals, M.; Skaro, A.I.; Parker, M.; Gallon, L. Impact of anemia after renal transplantation on patient and graft survival and on rate of acute rejection. Clin. J. Am. Soc. Nephrol. 2008, 3, 1168–1174. [Google Scholar] [CrossRef]
- Tran-Duy, A.; Connell, N.J.; Vanmolkot, F.H.; Souverein, P.C.; de Wit, N.J.; Stehouwer, C.D.A.; Hoes, A.W.; de Vries, F.; de Boer, A. Use of proton pump inhibitors and risk of iron deficiency: A population-based case-control study. J. Intern. Med. 2019, 285, 205–214. [Google Scholar] [CrossRef]
- Lam, J.R.; Schneider, J.L.; Quesenberry, C.P.; Corley, D.A. Proton Pump Inhibitor and Histamine-2 Receptor Antagonist Use and Iron Deficiency. Gastroenterology 2017, 152, 821–829. [Google Scholar] [CrossRef]
- Sarzynski, E.; Puttarajappa, C.; Xie, Y.; Grover, M.; Laird-Fick, H. Association between proton pump inhibitor use and anemia: A retrospective cohort study. Dig. Dis. Sci. 2011, 56, 2349–2353. [Google Scholar] [CrossRef]
- Hashimoto, R.; Matsuda, T.; Chonan, A. Iron-deficiency anemia caused by a proton pump inhibitor. Intern. Med. 2014, 53, 2297–2299. [Google Scholar] [CrossRef] [PubMed]
- Charlton, R.W.; Bothwell, T.H. Iron absorption. Annu. Rev. Med. 1983, 34, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Lawen, A.; Lane, D.J. Mammalian iron homeostasis in health and disease: Uptake, storage, transport, and molecular mechanisms of action. Antioxid. Redox Signal. 2013, 18, 2473–2507. [Google Scholar] [CrossRef] [PubMed]
- Ajmera, A.V.; Shastri, G.S.; Gajera, M.J.; Judge, T.A. Suboptimal response to ferrous sulfate in iron-deficient patients taking omeprazole. Am. J. Ther. 2012, 19, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, E.; Engberink, M.F.; Brink, E.J.; van Baak, M.A.; Joosten, M.M.; Gans, R.O.; Navis, G.; Bakker, S.J. Dietary acid load and metabolic acidosis in renal transplant recipients. Clin. J. Am. Soc. Nephrol. 2012, 7, 1811–1818. [Google Scholar] [CrossRef]
- Van den Berg, E.; Geleijnse, J.M.; Brink, E.J.; van Baak, M.A.; van der Heide, J.J.H.; Gans, R.O.; Navis, G.; Bakker, S.J. Sodium intake and blood pressure in renal transplant recipients. Nephrol. Dial. Transplant. 2012, 27, 3352–3359. [Google Scholar] [CrossRef] [PubMed]
- Eisenga, M.F.; van Londen, M.; Leaf, D.E.; Nolte, I.M.; Navis, G.; Bakker, S.J.L.; de Borst, M.H.; Gaillard, C.A.J.M. C-Terminal Fibroblast Growth Factor 23, Iron Deficiency, and Mortality in Renal Transplant Recipients. J. Am. Soc. Nephrol. 2017, 28, 3639–3646. [Google Scholar] [CrossRef]
- Charytan, C.; Levin, N.; Al-Saloum, M.; Hafeez, T.; Gagnon, S.; Van Wyck, D.B. Efficacy and Safety of Iron Sucrose for Iron Deficiency in Patients With Dialysis-Associated Anemia: North American Clinical Trial. Am. J. Kidney Dis. 2001, 37, 300–307. [Google Scholar] [CrossRef]
- Anker, S.D.; Comin Colet, J.; Filippatos, G.; Willenheimer, R.; Dickstein, K.; Drexler, H.; Lüscher, T.F.; Bart, B.; Banasiak, W.; Niegowska, J.; et al. Ferric Carboxymaltose in Patients with Heart Failure and Iron Deficiency. N. Engl. J. Med. 2009, 361, 2436–2448. [Google Scholar] [CrossRef]
- Van den Berg, E.; Engberink, M.F.; Brink, E.J.; van Baak, M.A.; Gans, R.O.B.; Navis, G.; Bakker, S.J.L. Dietary protein, blood pressure and renal function in renal transplant recipients. Br. J. Nutr. 2013, 109, 1463–1470. [Google Scholar] [CrossRef]
- Feunekes, I.J.; Van Staveren, W.A.; Graveland, F.; De Vos, J.; Burema, J. Reproducibility of a semiquantitative food frequency questionnaire to assess the intake of fats and cholesterol in The Netherlands. Int. J. Food Sci. Nutr. 1995, 46, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Dutch Food Composition Table NEVO-Tabel. Nederlands Voedingsstoffenbestand; RIVM/Netherlands Nutrition Centre: Bilthoven, The Netherlands, 2006. [Google Scholar]
- Kirchheiner, J.; Glatt, S.; Fuhr, U.; Klotz, U.; Meineke, I.; Seufferlein, T.; Brockmoller, J. Relative potency of proton-pump inhibitors-comparison of effects on intragastric pH. Eur. J. Clin. Pharmacol. 2009, 65, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Locatelli, F.; Bárány, P.; Covic, A.; De Francisco, A.; Del Vecchio, L.; Goldsmith, D.; Hörl, W.; London, G.; Vanholder, R.; Van Biesen, W.; et al. Kidney Disease: Improving Global Outcomes guidelines on anaemia management in chronic kidney disease: A European Renal Best Practice position statement. Nephrol. Dial. Transplant. 2013, 28, 1346–1359. [Google Scholar] [CrossRef] [PubMed]
- Ratcliffe, L.E.K.; Thomas, W.; Glen, J.; Padhi, S.; Pordes, B.A.J.; Wonderling, D.; Connell, R.; Stephens, S.; Mikhail, A.I.; Fogarty, D.G.; et al. Diagnosis and Management of Iron Deficiency in CKD: A Summary of the NICE Guideline Recommendations and Their Rationale. Am. J. Kidney Dis. 2016, 67, 548–558. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.R.; Brannon, M.A.; Carloss, E.A. Effect of omeprazole on oral iron replacement in patients with iron deficiency anemia. South. Med. J. 2004, 97, 887–889. [Google Scholar] [CrossRef] [PubMed]
- Abedini, S.; Holme, I.; Marz, W.; Weihrauch, G.; Fellstrom, B.; Jardine, A.; Cole, E.; Maes, B.; Neumayer, H.H.; Gronhagen-Riska, C.; et al. Inflammation in renal transplantation. Clin. J. Am. Soc. Nephrol. 2009, 4, 1246–1254. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, B.; Effenberger, M.; Zoller, H. Iron metabolism in transplantation. Transpl. Int. 2014, 27, 1109–1117. [Google Scholar] [CrossRef]
- Zheng, S.; Coyne, D.W.; Joist, H.; Schuessler, R.; Godboldo-Brooks, A.; Ercole, P.; Brennan, D.C. Iron deficiency anemia and iron losses after renal transplantation. Transpl. Int. 2009, 22, 434–440. [Google Scholar] [CrossRef]
- Hunfeld, N.G.; Touw, D.J.; Mathot, R.A.; Schaik, R.H.; Kuipers, E.J. A comparison of the acid-inhibitory effects of esomeprazole and rabeprazole in relation to pharmacokinetics and CYP2C19 polymorphism. Aliment. Pharmacol. Ther. 2012, 35, 810–818. [Google Scholar] [CrossRef]
- Sim, S.C.; Risinger, C.; Dahl, M.-L.; Aklillu, E.; Christensen, M.; Bertilsson, L.; Ingelman-Sundberg, M. A common novel CYP2C19 gene variant causes ultrarapid drug metabolism relevant for the drug response to proton pump inhibitors and antidepressants. Clin. Pharmacol. Ther. 2006, 79, 103–113. [Google Scholar] [CrossRef]
- Stewart, C.A.; Termanini, B.; Sutliff, V.E.; Serrano, J.; Yu, F.; Gibril, F.; Jensen, R.T. Iron absorption in patients with Zollinger-Ellison syndrome treated with long-term gastric acid antisecretory therapy. Aliment. Pharmacol. Ther. 1998, 12, 83–98. [Google Scholar] [CrossRef] [PubMed]
- Koop, H.; Bachem, M.G. Serum iron, ferritin, and vitamin B12 during prolonged omeprazole therapy. J. Clin. Gastroenterol. 1992, 14, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, C.; Geissler, C.A.; Powell, J.J.; Bomford, A. Proton pump inhibitors suppress absorption of dietary non-haem iron in hereditary haemochromatosis. Gut 2007, 56, 1291–1295. [Google Scholar] [CrossRef] [PubMed]
- Bezwoda, W.; Charlton, R.; Bothwell, T.; Torrance, J.; Mayet, F. The importance of gastric hydrochloric acid in the absorption of nonheme food iron. J. Lab. Clin. Med. 1978, 92, 108–116. [Google Scholar] [PubMed]
- Henry, E.B.; Carswell, A.; Wirz, A.; Fyffe, V.; McColl, K.E. Proton pump inhibitors reduce the bioavailability of dietary vitamin C. Aliment. Pharmacol. Ther. 2005, 22, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Sridharan, K.; Sivaramakrishnan, G. Interaction of Citrus Juices with Cyclosporine: Systematic Review and Meta-Analysis. Eur. J. Drug Metab. Pharmacokinet. 2016, 41, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Sotomayor, C.G.; Eisenga, M.F.; Gomes Neto, A.W.; Ozyilmaz, A.; Gans, R.O.B.; de Jong, W.H.A.; Zelle, D.M.; Berger, S.P.; Gaillard, C.A.J.M.; Navis, G.J.; et al. Vitamin C Depletion and All-Cause Mortality in Renal Transplant Recipients. Nutrients 2017, 9, 568. [Google Scholar] [CrossRef] [PubMed]
- Saha, P.; Yeoh, B.S.; Singh, R.; Chandrasekar, B.; Vemula, P.K.; Haribabu, B.; Vijay-Kumar, M.; Jala, V.R. Gut Microbiota Conversion of Dietary Ellagic Acid into Bioactive Phytoceutical Urolithin A Inhibits Heme Peroxidases. PLoS ONE 2016, 11, e0156811. [Google Scholar] [CrossRef] [PubMed]
- González, A.; Gálvez, N.; Martín, J.; Reyes, F.; Pérez-Victoria, I.; Dominguez-Vera, J.M. Identification of the key excreted molecule by Lactobacillus fermentum related to host iron absorption. Food Chem. 2017, 228, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, M.; Önning, G.; Berggren, A.; Hulthén, L. Probiotic strain Lactobacillus plantarum 299v increases iron absorption from 2 an iron-supplemented fruit drink: A double-isotope cross-over single-blind 3 study in women of reproductive age—Erratum. Br. J. Nutr. 2015, 114, 1948. [Google Scholar] [CrossRef] [PubMed]
- Imhann, F.; Bonder, M.J.; Vila, A.V.; Fu, J.; Mujagic, Z.; Vork, L.; Tigchelaar, E.F.; Jankipersadsing, S.A.; Cenit, M.C.; Harmsen, H.J.; et al. Proton pump inhibitors affect the gut microbiome. Gut 2016, 65, 740–748. [Google Scholar] [CrossRef] [PubMed]
- Pagès-Puigdemont, N.; Mangues, M.A.; Masip, M.; Gabriele, G.; Fernández-Maldonado, L.; Blancafort, S.; Tuneu, L. Patients’ Perspective of Medication Adherence in Chronic Conditions: A Qualitative Study. Adv. Ther. 2016, 33, 1740–1754. [Google Scholar] [CrossRef] [PubMed]
- Suliburska, J.; Skrypnik, K.; Szulińska, M.; Kupsz, J.; Markuszewski, L.; Bogdański, P. Diuretics, Ca-Antagonists, and Angiotensin-Converting Enzyme Inhibitors Affect Zinc Status in Hypertensive Patients on Monotherapy: A Randomized Trial. Nutrients 2018, 10, 1284. [Google Scholar] [CrossRef]
- Van Raaij, S.E.G.; Rennings, A.J.; Biemond, B.J.; Schols, S.E.M.; Wiegerinck, E.T.G.; Roelofs, H.M.J.; Hoorn, E.J.; Walsh, S.B.; Nijenhuis, T.; Swinkels, D.W.; et al. Iron handling by the human kidney: Glomerular filtration and tubular reabsorption both contribute to urinary iron excretion. Am. J. Physiol. Physiol. 2019, 316, F606–F614. [Google Scholar] [CrossRef] [PubMed]
- Bardet, V.; Junior, A.P.; Coste, J.; Lecoq-Lafon, C.; Chouzenoux, S.; Bernard, D.; Soubrane, O.; Lacombe, C.; Calmus, Y.; Conti, F. Impaired erythropoietin production in liver transplant recipients: The role of calcineurin inhibitors. Liver Transpl. 2006, 12, 1649–1654. [Google Scholar] [CrossRef]
- Naini, A.E.; Amra, B.; Mahmoodnia, L.; Taheri, S. Sleep apnea syndrome and restless legs syndrome in kidney transplant recipients. Adv. Biomed. Res. 2015, 4, 206. [Google Scholar]


{kind=link}
| Characteristics | Total Population | Non-PPI User | PPI User | p | |
|---|---|---|---|---|---|
| Number of subjects, n (%) | 646 (100) | 283 (43.8) | 363 (56.2) | n/a | |
| Demographics | |||||
| Age, years | 53 ± 13 | 51 ± 13 | 54 ± 12 | 0.001 | |
| Men, n (%) | 382 (59.1) | 170 (60.1) | 212 (58.4) | 0.7 | |
| BMI, kg/m2 | 26.7 ± 4.8 | 26.0 ± 4.6 | 27.3 ± 4.8 | <0.001 | |
| Diabetes Mellitus, n (%) | 157 (24.3) | 54 (19.1) | 103 (28.4) | 0.006 | |
| History of gastrointestinal disorders, n (%) | 42 (6.5) | 10 (3.5) | 32 (8.8) | 0.007 | |
| Time since transplantation, years | 5.3 (1.8–12.0) | 9.5 (4.1–15.0) | 4.0 (1.1–8.0) | <0.001 | |
| Lifestyle parameters | |||||
| Current smoker, n (%) | 79 (13.1) | 33 (12.4) | 46 (13.6) | 0.7 | |
| Alcohol consumer, n (%) | 409 (70.6) | 186 (72.7) | 223 (69.0) | 0.3 | |
| Iron intake, mg/d | 11.3 ± 2.9 | 11.2 ± 2.7 | 11.4 ± 3.0 | 0.5 | |
| Renal function parameters | |||||
| eGFR, mL/min/1.73 m2 | 53.5 ± 19.9 | 56.2 ± 19.7 | 51.4 ± 19.8 | 0.002 | |
| Serum creatinine, µmol/L | 122 (99–156) | 117 (98–150) | 126 (101–164) | 0.03 | |
| Proteinuria (≥0.5 g/24 h), n (%) | 135 (21.0) | 60 (21.2) | 75 (20.8) | 0.9 | |
| Laboratory parameters | |||||
| Iron deficiency, n (%) | 193 (29.9) | 63 (22.3) | 130 (35.8) | <0.001 | |
| Hb, g/dL | 13.3 ± 1.7 | 13.6 ± 1.6 | 13.1 ± 1.8 | <0.001 | |
| Iron, µmol/L | 15.2 ± 5.9 | 16.4 ± 6.1 | 14.2 ± 5.6 | <0.001 | |
| Ferritin, µg/L | 115.5 (53.0–216.3) | 136.0 (77.0–222.0) | 93.0 (42.0–196.0) | <0.001 | |
| Transferrin saturation, % | 25.1 ± 10.5 | 27.3 ± 10.1 | 23.3 ± 10.5 | <0.001 | |
| Glucose, mmol/L | 5.3 (4.8–6.0) | 5.2 (4.7–5.8) | 5.3 (4.9–6.2) | 0.01 | |
| HbA1c, mmol/mol | 40 (37–44) | 39 (36 – 42) | 41 (38 – 45) | <0.001 | |
| HsCRP, mg/L | 1.6 (0.8–4.2) | 1.6 (0.8–3.8) | 1.6 (0.7–4.6) | 0.8 | |
| Medication use | |||||
| Calcineurin inhibitors, n (%) | 369 (57.1) | 137 (48.4) | 232 (63.9) | <0.001 | |
| Mycophenolate mofetil, n (%) | 431 (66.7) | 171 (60.4) | 260 (71.6) | 0.003 | |
| Prednisolone, n (%) | 641 (99.2) | 282 (99.6) | 359 (98.9) | 0.4 | |
| Diuretics, n (%) | 253 (39.2) | 87 (30.7) | 166 (45.7) | <0.001 | |
| RAAS–inhibitors, n (%) | 314 (48.6) | 144 (50.9) | 170 (46.8) | 0.3 | |
| Antiplatelet drugs, n (%) | 131 (20.3) | 46 (16.3) | 85 (23.4) | 0.03 | |
| H2-receptor antagonists, n (%) | 20 (3.1) | 19 (6.7) | 1 (0.3) | <0.001 | |
| Serum Iron, µmol/L | Ln Serum Ferritin, µg/L | Transferrin Saturation, % | Hemoglobin, g/dL | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 646 | β | 95% CI | p | β | 95% CI | p | β | 95% CI | p | β | 95% CI | p |
| Crude | −2.18 | −3.09; −1.27 | <0.001 | −0.34 | −0.49; −0.18 | <0.001 | −3.92 | −5.52; −2.32 | <0.001 | −0.52 | −0.78; −0.25 | <0.001 |
| Model 1 | −2.03 | −2.94; −1.12 | <0.001 | −0.35 | −0.50; −0.20 | <0.001 | −3.80 | −5.40; −2.20 | <0.001 | −0.52 | −0.78; −0.26 | <0.001 |
| Model 2 | −1.61 | −2.57; −0.65 | 0.001 | −0.31 | −0.48; −0.15 | <0.001 | −2.85 | −4.55; −1.15 | 0.001 | −0.35 | −0.61; −0.10 | 0.007 |
| Model 3 | −1.67 | −2.67; −0.66 | 0.001 | −0.31 | −0.48; −0.14 | <0.001 | −3.00 | −4.80; −1.20 | 0.001 | −0.41 | −0.67; −0.14 | 0.003 |
| Model 4 | −1.54 | −2.48; −0.60 | 0.001 | −0.32 | −0.48; −0.16 | <0.001 | −2.75 | −4.43; −1.07 | 0.001 | −0.35 | −0.61; −0.09 | 0.007 |
| Model 5 | −1.62 | −2.58; −0.66 | 0.001 | −0.31 | −0.47; −0.15 | <0.001 | −2.90 | −4.60; −1.20 | 0.001 | −0.35 | −0.61; −0.01 | 0.007 |
| Model 6 | −1.37 | −2.33; −0.41 | 0.005 | −0.27 | −0.43; −0.11 | 0.001 | −2.33 | −4.03; −0.63 | 0.007 | −0.33 | −0.58; −0.07 | 0.01 |
| Iron Deficiency | |||
|---|---|---|---|
| n = 646 | Odds Ratio | 95% CI | p |
| Crude | 1.95 | 1.37–2.77 | <0.001 |
| Model 1 | 1.94 | 1.36–2.78 | <0.001 |
| Model 2 | 1.57 | 1.07–2.31 | 0.02 |
| Model 3 | 1.57 | 1.04–2.38 | 0.03 |
| Model 4 | 1.56 | 1.06–2.30 | 0.03 |
| Model 5 | 1.57 | 1.07–2.31 | 0.02 |
| Model 6 | 1.43 | 0.96–2.12 | 0.08 |
| Categories of PPI Use | |||||||
|---|---|---|---|---|---|---|---|
| No PPI | Low PPI Dose | High PPI Dose | p trend | ||||
| Number of subjects | 283 | 237 | 126 | ||||
| Odds ratio (95% CI) | p value | Odds ratio (95% CI) | p value | Odds ratio (95% CI) | p value | ||
| Iron deficiency | |||||||
| Crude | 1.00 (reference) | n/a | 1.78 (1.21–2.62) | 0.004 | 2.30 (1.46–3.62) | <0.001 | <0.001 |
| Model 1 | 1.00 (reference) | n/a | 1.76 (1.19–2.62) | 0.005 | 2.33 (1.47–3.69) | <0.001 | <0.001 |
| Model 2 | 1.00 (reference) | n/a | 1.38 (0.90–2.10) | 0.14 | 2.00 (1.23–3.25) | 0.005 | 0.005 |
| Model 3 | 1.00 (reference) | n/a | 1.43 (0.91–2.24) | 0.12 | 1.88 (1.11–3.16) | 0.02 | 0.02 |
| Model 4 | 1.00 (reference) | n/a | 1.39 (0.91–2.13) | 0.12 | 1.93 (1.18–3.15) | 0.009 | 0.008 |
| Model 5 | 1.00 (reference) | n/a | 1.38 (0.91–2.10) | 0.14 | 2.00 (1.23–3.26) | 0.005 | 0.005 |
| Model 6 | 1.00 (reference) | n/a | 1.29 (0.84–1.98) | 0.25 | 1.73 (1.05–2.86) | 0.03 | 0.03 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Douwes, R.M.; Gomes-Neto, A.W.; Eisenga, M.F.; Vinke, J.S.J.; de Borst, M.H.; van den Berg, E.; Berger, S.P.; Touw, D.J.; Hak, E.; Blokzijl, H.; et al. Chronic Use of Proton-Pump Inhibitors and Iron Status in Renal Transplant Recipients. J. Clin. Med. 2019, 8, 1382. https://doi.org/10.3390/jcm8091382
Douwes RM, Gomes-Neto AW, Eisenga MF, Vinke JSJ, de Borst MH, van den Berg E, Berger SP, Touw DJ, Hak E, Blokzijl H, et al. Chronic Use of Proton-Pump Inhibitors and Iron Status in Renal Transplant Recipients. Journal of Clinical Medicine. 2019; 8(9):1382. https://doi.org/10.3390/jcm8091382
Chicago/Turabian StyleDouwes, Rianne M., António W. Gomes-Neto, Michele F. Eisenga, Joanna Sophia J. Vinke, Martin H. de Borst, Else van den Berg, Stefan P. Berger, Daan J. Touw, Eelko Hak, Hans Blokzijl, and et al. 2019. "Chronic Use of Proton-Pump Inhibitors and Iron Status in Renal Transplant Recipients" Journal of Clinical Medicine 8, no. 9: 1382. https://doi.org/10.3390/jcm8091382
APA StyleDouwes, R. M., Gomes-Neto, A. W., Eisenga, M. F., Vinke, J. S. J., de Borst, M. H., van den Berg, E., Berger, S. P., Touw, D. J., Hak, E., Blokzijl, H., Navis, G., & Bakker, S. J. L. (2019). Chronic Use of Proton-Pump Inhibitors and Iron Status in Renal Transplant Recipients. Journal of Clinical Medicine, 8(9), 1382. https://doi.org/10.3390/jcm8091382