Real World Patterns of Antimicrobial Use and Microbiology Investigations in Patients with Sepsis outside the Critical Care Unit: Secondary Analysis of Three Nation-Wide Point Prevalence Studies

 , , , , , , , , , and
, , , , , , , , , and  add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Experimental Section
2.1. Study Design and Participants
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Antibiotics Characteristics
3.3. Organism Characteristics
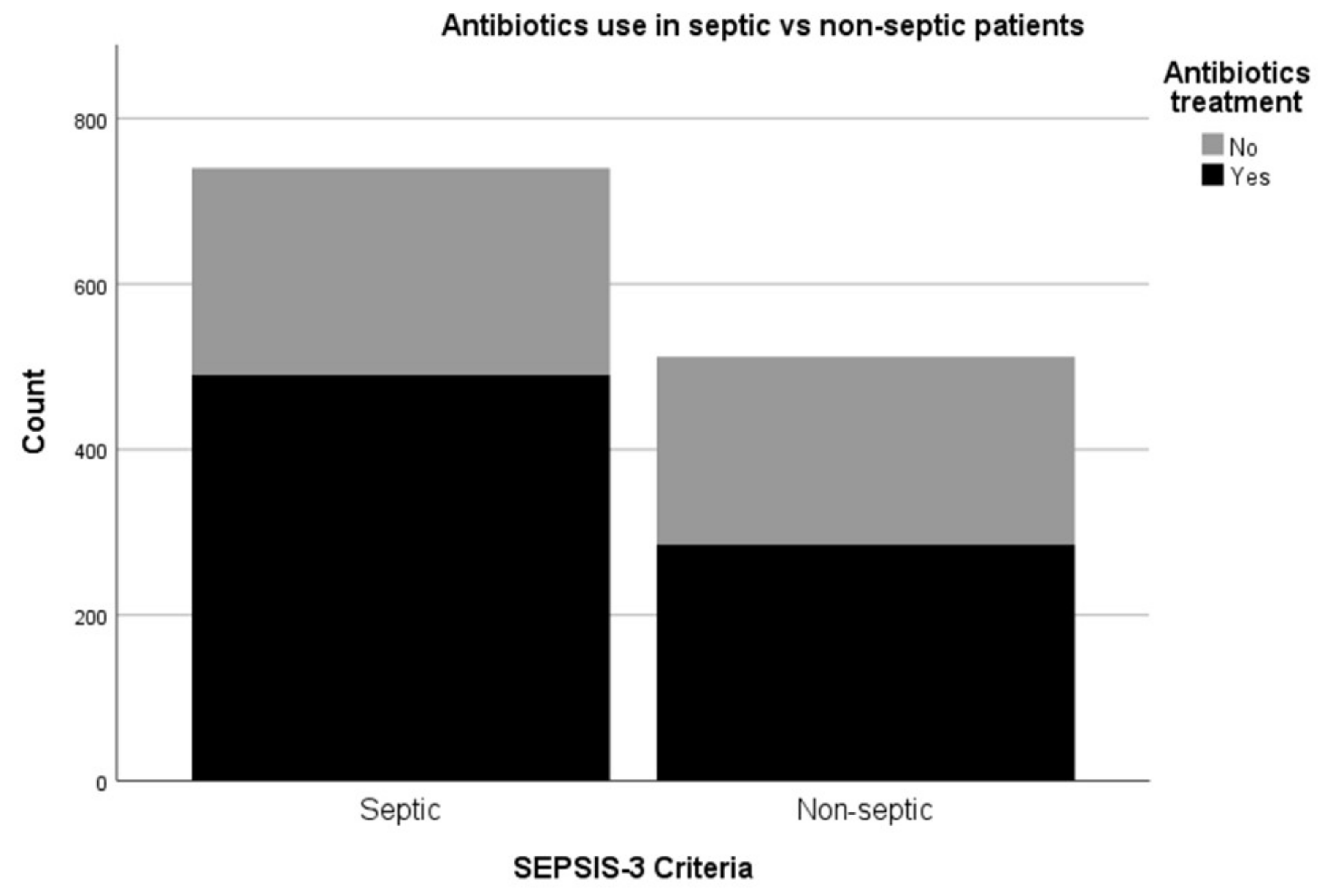
3.4. Antibiotics Use in Patients Fulfilling SEPSIS-3 Criteria
3.5. Antibiotics and Microbiological Investigations
3.6. Factors Influencing Antibiotics Administration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Jaschinski, U.; Wittebole, X.; Szakmany, T.; Lipman, J.; Ñamendys-Silva, S.A.; Martin-Loeches, I.; Leone, M.; Lupu, M.N.; Vincent, J.L.; et al. Sepsis in Intensive Care Unit Patients: Worldwide Data from the Intensive Care over Nations Audit. Open Forum Infectious Diseases 2018, 5, ofy313. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Lefrant, J.Y.; Kotfis, K.; Nanchal, R.; Martin-Loeches, I.; Wittebole, X.; Sakka, S.G.; Pickkers, P.; Moreno, R.; Sakr, Y. Comparison of European ICU patients in 2012 (ICON) versus 2002 (SOAP). Intensive Care Med. 2018, 44, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, A.; Phillips, G.; Beale, R.; Cecconi, M.; Chiche, J.D.; De Backer, D.; Divatia, J.; Du, B.; Evans, L.; Ferrer, R.; et al. The Surviving Sepsis Campaign bundles and outcome: Results from the International Multicentre Prevalence Study on Sepsis (the IMPreSS study). Intensive Care Med. 2015, 41, 1620–1628. [Google Scholar] [CrossRef] [PubMed]
- Daniels, R.; Nutbeam, T.; McNamara, G.; Galvin, C. The sepsis six and the severe sepsis resuscitation bundle: A prospective observational cohort study. Emerg. Med. J. 2011, 28, 507. [Google Scholar] [CrossRef]
- Levy, M.M.; Rhodes, A.; Phillips, G.S.; Townsend, S.R.; Schorr, C.A.; Beale, R.; Osborn, T.; Lemeshow, S.; Chiche, J.D.; Artigas, A.; et al. Surviving Sepsis Campaign: Association Between Performance Metrics and Outcomes in a 7.5-Year Study. Crit. Care Med. 2015, 43, 3–12. [Google Scholar]
- Hancock, C. A national quality improvement initiative for reducing harm and death from sepsis in Wales. Int. Crit. Care Nurs. 2015, 31, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Szakmany, T.; Lundin, R.M.; Sharif, B.; Ellis, G.; Morgan, P.; Kopczynska, M.; Dhadda, A.; Mann, C.; Donoghue, D.; Rollason, S.; et al. Sepsis Prevalence and Outcome on the General Wards and Emergency Departments in Wales: Results of a Multi-Centre, Observational, Point Prevalence Study. PLoS ONE 2016, 11, e0167230. [Google Scholar] [CrossRef]
- Szakmany, T.; Pugh, R.; Kopczynska, M.; Lundin, R.M.; Sharif, B.; Morgan, P.; Ellis, G.; Abreu, J.; Kulikouskaya, S.; Bashir, K.; et al. Defining sepsis on the wards: Results of a multi-centre point-prevalence study comparing two sepsis definitions. Anaesthesia 2018, 73, 195–204. [Google Scholar] [CrossRef]
- Kopczynska, M.; Sharif, B.; Cleaver, S.; Spencer, N.; Kurani, A.; Lee, C.; Davis, J.; Durie, C.; Joseph-Gubral, J.; Sharma, A.; et al. Red-flag sepsis and SOFA identifies different patient population at risk of sepsis-related deaths on the general ward. Medicine 2018, 97, e13238. [Google Scholar] [CrossRef]
- Burke, J.; Wood, S.; Hermon, A.; Szakmany, T. Improving outcome of sepsis on the ward: Introducing the ‘Sepsis Six’ bundle. Nurs. Crit. Care. 2019, 24, 33–39. [Google Scholar] [CrossRef]
- Marik, P.E.; Malbrain, M.L.N.G. The SEP-1 quality mandate may be harmful: How to drown a patient with 30 mL per kg fluid! Anaesthesiol. Intensive Ther. 2017, 49, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Perner, A.; Singer, M. Fixed minimum fluid volume for resuscitation: Con. Intensive Care Med. 2017, 43, 1681–1682. [Google Scholar] [CrossRef] [PubMed]
- Sharif, B.; Lundin, R.M.; Morgan, P.; Hall, J.E.; Dhadda, A.; Mann, C.; Donoghue, D.; Brownlow, E.; Hill, F.; Carr, G.; et al. Developing a digital data collection platform to measure the prevalence of sepsis in Wales. J. Am. Med. Inf. Assoc. 2016, 23, 1185. [Google Scholar] [CrossRef] [PubMed]
- Seymour, C.W.; Gesten, F.; Prescott, H.C.; Friedrich, M.E.; Iwashyna, T.J.; Phillips, G.S.; Lemeshow, S.; Osborn, T.; Terry, K.M.; Levy, M.M. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. NEJM 2017, 376, 2235–2244. [Google Scholar] [CrossRef] [PubMed]
- Liu, V.X.; Fielding-Singh, V.; Greene, J.D.; Baker, J.M.; Iwashyna, T.J.; Bhattacharya, J.; Escobar, G.J. The Timing of Early Antibiotics and Hospital Mortality in Sepsis. Am. J. Respir. Crit. Care Med. 2017, 196, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- Harper, N.J.; Cook, T.M.; Garcez, T.; Farmer, L.; Floss, K.; Marinho, S.; Torevell, H.; Warner, A.; Ferguson, K.; Hitchman, J.; et al. Anaesthesia, surgery, and life-threatening allergic reactions: Epidemiology and clinical features of perioperative anaphylaxis in the 6th National Audit Project (NAP6). Br. J. Anaesth. 2018, 121, 159–171. [Google Scholar] [CrossRef]
- Klompas, M.; Calandra, T.; Singer, M. Antibiotics for Sepsis—Finding the Equilibrium. JAMA 2018, 320, 1433–1434. [Google Scholar] [CrossRef]
- Bloos, F.; Rüddel, H.; Thomas-Rüddel, D.; Schwarzkopf, D.; Pausch, C.; Harbarth, S.; Schreiber, T.; Gründling, M.; Marshall, J.; Simon, P.; et al. Effect of a multifaceted educational intervention for anti-infectious measures on sepsis mortality: A cluster randomized trial. Intensive Care Med. 2017, 43, 1602–1612. [Google Scholar] [CrossRef]
- Alam, N.; Oskam, E.; Stassen, P.M.; van Exter, P.; van de Ven, P.M.; Haak, H.R.; Holleman, F.; van Zanten, A.; van Leeuwen-Nguyen, H.; Bon, V.; et al. Prehospital antibiotics in the ambulance for sepsis: A multicentre, open label, randomised trial. Lancet Respir. Med. 2018, 6, 40–50. [Google Scholar] [CrossRef]
- Kopczynska, M.; Sharif, B.; Cleaver, S.; Spencer, N.; Kurani, A.; Lee, C.; Davis, J.; Durie, C.; Joseph-Gubral, J.; Sharma, A.; et al. Sepsis-related deaths in the at-risk population on the wards: Attributable fraction of mortality in a large point-prevalence study. BMC Res. Notes 2018, 11, 720. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.; Jones, T.M.; Hamad, Y.; Pande, A.; Varon, J.; O’Brien, C.; Anderson, D.J.; Warren, D.K.; Dantes, R.B.; Epstein, L.; et al. Prevalence, Underlying Causes, and Preventability of Sepsis-Associated Mortality in US Acute Care Hospitals. JAMA Netw. Open 2019, 2, e187571. [Google Scholar] [CrossRef] [PubMed]
- Septimus, E.J.; Coopersmith, C.M.; Whittle, J.; Hale, C.P.; Fishman, N.O.; Kim, T.J. Sepsis National Hospital Inpatient Quality Measure (SEP-1): Multistakeholder Work Group Recommendations for Appropriate Antibiotics for the Treatment of Sepsis. Clin. Infect. Dis. 2017, 65, 1565–1569. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The Surviving Sepsis Campaign Bundle: 2018 update. Intensive Care Med. 2018, 44, 925–928. [Google Scholar] [CrossRef] [PubMed]
- Garnacho-Montero, J.; Garcia-Garmendia, J.L.; Barrero-Almodovar, A.; Jimenez-Jimenez, F.J.; Perez-Paredes, C.; Ortiz-Leyba, C. Impact of adequate empirical antibiotic therapy on the outcome of patients admitted to the intensive care unit with sepsis. Crit. Care Med. 2003, 31, 2742–2751. [Google Scholar] [CrossRef] [PubMed]
- Harbarth, S.; Garbino, J.; Pugin, J.; Romand, J.A.; Lew, D.; Pittet, D. Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis. Am. J. Med. 2003, 115, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Morgan, M.P.; Szakmany, T.; Power, S.G.; Olaniyi, P.; Hall, J.E.; Rowan, K.; Eberl, M. Sepsis Patients with First and Second-Hit Infections Show Different Outcomes Depending on the Causative Organism. Front. Microbiol. 2016, 7, 207. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Evans, T.W.; Finney, S.J. Bench-to-bedside review: Sepsis, severe sepsis and septic shock-does the nature of the infecting organism matter? Crit. Care. 2008, 12, 213. [Google Scholar] [CrossRef] [PubMed]
- Loonen, A.J.M.; Wolffs, P.F.G.; Bruggeman, C.A.; van den Brule, A.J.C. Developments for improved diagnosis of bacterial bloodstream infections. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1687–1702. [Google Scholar] [CrossRef]
- Heginbothom, M.; Howe, R.; McArtney, B.; Parry-Jones, J.; Smithies, M.; Szakmany, T. The Microbiology of Severe Sepsis; Public Health Wales: Cardiff, UK, 2013; Available online: http://www.wales.nhs.uk/sites3/page.cfm?orgId=457&pid=289062013 (accessed on 2 July 2019).
- Jamal, W.; Tamaray, G.; Pazhoor, A.; Rotimi, V.O. Comparative Evaluation of BacT/ALERT 3D and BACTEC Systems for the Recovery of Pathogens Causing Bloodstream Infections. Med. Princ. Pract. 2006, 15, 223–227. [Google Scholar] [CrossRef]
- Angus, D.C.; Linde-Zwirble, W.T.; Lidicker, J.; Clermont, G.; Carcillo, J.; Pinsky, M.R. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 2001, 29, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Churpek, M.M.; Snyder, A.; Han, X.; Sokol, S.; Pettit, N.; Howell, M.D.; Edelson, D.P. Quick Sepsis-related Organ Failure Assessment, Systemic Inflammatory Response Syndrome, and Early Warning Scores for Detecting Clinical Deterioration in Infected Patients outside the Intensive Care Unit. Am. J. Respir. Crit. Care Med. 2017, 195, 906–911. [Google Scholar] [CrossRef] [PubMed]
- Keep, J.W.; Messmer, A.S.; Sladden, R.; Burrell, N.; Pinate, R.; Tunnicliff, M.; Glucksman, E. National early warning score at Emergency Department triage may allow earlier identification of patients with severe sepsis and septic shock: A retrospective observational study. Emerg. Med. J. 2016, 33, 37–41. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Median | Interquartile Range (Q3–Q1) | |
|---|---|---|
| Age (years) | 73 | 22 |
| Number of co-morbidities (n) | 1 | 2 |
| Frailty Score | 5 | 3 |
| NEWS score | 4 | 3 |
| SIRS score | 2 | 2 |
| SOFA score | 2 | 2 |
| Number of Patients, n (%) | ||
| Sex, male | 624 (49.8) | |
| SEPSIS-3 criteria present | 740 (59.1) | |
| ED admission | 193 (15.4) | |
| General medical admission | 544 (43.5) | |
| General surgical admission | 197 (15.7) | |
| Admission to other ward | 321 (25.6) | |
| Ceiling of care documented | 263 (21.0) | |
| DNA-CPR documented | 305 (24.4) | |
| COPD | 347 (27.7) | |
| Diabetes | 262 (20.9) | |
| Heart failure | 144 (11.5) | |
| Hypertension | 417 (33.3) | |
| Ischaemic heart disease | 210 (16.8) | |
| Liver disease | 43 (3.4) | |
| Neuromuscular disease | 40 (3.2) | |
| Recent chemotherapy | 50 (4.0) | |
| Chronic antibiotics | 94 (7.5) | |
| Blood Culture (n) | Sputum Culture (n) | Urine Culture (n) | Wound Culture (n) | Other Culture (n) |
|---|---|---|---|---|
| Escherichia coli (17) | Respiratory flora (33) | Escherichia coli (33) | Mixed growth (27) | MRSA (4) |
| Gram positive cocci (16) | Haemophilus influenzae (11) | Mixed growth (18) | Staphylococcus aureus (16) | Aspergillus (2) |
| Coagulase negative Staphylococcus (6) | Candida albicans (9) | KESC group (3) | Coliform (2) | Escherichia coli (2) |
| MSSA (6) | Pseudomonas aeruginosa (9) | Contamination (2) | Serratia marcescens (2) | Rhinovirus (2) |
| Pseudomonas aeruginosa (6) | Mixed growth (8) | Enterococcus bacteria (2) | Skin flora (2) | Aggregatibacter aphrophilus (1) |
| Streptococcus pneumoniae (5) | Moraxella catarrhalis (3) | Pseudomonas aeruginosa (2) | Candida albicans (1) | Clostridium difficile (1) |
| Klebsiella pneumoniae (3) | Staphylococcus aureus (3) | Proteus mirabilis (1) | Enterococcus (1) | Enterovirus (1) |
| Gram negative bacilli (2) | Streptococcus pneumoniae (2) | Yeast (1) | Escherichia coli (1) | Staphylococcus aureus (1) |
| MRSA (2) | Corynebacterium striatum (1) | No growth (259) | Group B Streptococcus (1) | Streptococcus intermedius (1) |
| Proteus mirabilis (2) | Escherichia coli (1) | Pseudomonas aeruginosa (1) | Yeast (1) | |
| Staphylococcus aureus (2) | Klebsiella pneumoniae (1) | Streptococcus viridans (1) | No growth (175) | |
| Enterobacter cloacae (1) | Coliform (1) | No growth (30) | ||
| Erysipelothrix rhusiopathiae (1) | No growth (26) | |||
| Parabacteroides distasonis (1) | ||||
| Salmonella (1) | ||||
| Serratia marcescens (1) | ||||
| Staphylococcus epidermidis (1) | ||||
| Staphylococcus lugdunensis (1) | ||||
| Streptococcus agalactiae (1) | ||||
| Streptococcus intermedius (1) | ||||
| Streptococcus oralis (1) | ||||
| No growth (344) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kopczynska, M.; Sharif, B.; Unwin, H.; Lynch, J.; Forrester, A.; Zeicu, C.; Cleaver, S.; Kulikouskaya, S.; Chandy, T.; Ang, E.; et al. Real World Patterns of Antimicrobial Use and Microbiology Investigations in Patients with Sepsis outside the Critical Care Unit: Secondary Analysis of Three Nation-Wide Point Prevalence Studies. J. Clin. Med. 2019, 8, 1337. https://doi.org/10.3390/jcm8091337
Kopczynska M, Sharif B, Unwin H, Lynch J, Forrester A, Zeicu C, Cleaver S, Kulikouskaya S, Chandy T, Ang E, et al. Real World Patterns of Antimicrobial Use and Microbiology Investigations in Patients with Sepsis outside the Critical Care Unit: Secondary Analysis of Three Nation-Wide Point Prevalence Studies. Journal of Clinical Medicine. 2019; 8(9):1337. https://doi.org/10.3390/jcm8091337
Chicago/Turabian StyleKopczynska, Maja, Ben Sharif, Harry Unwin, John Lynch, Andrew Forrester, Claudia Zeicu, Sian Cleaver, Svetlana Kulikouskaya, Tom Chandy, Eshen Ang, and et al. 2019. "Real World Patterns of Antimicrobial Use and Microbiology Investigations in Patients with Sepsis outside the Critical Care Unit: Secondary Analysis of Three Nation-Wide Point Prevalence Studies" Journal of Clinical Medicine 8, no. 9: 1337. https://doi.org/10.3390/jcm8091337
APA StyleKopczynska, M., Sharif, B., Unwin, H., Lynch, J., Forrester, A., Zeicu, C., Cleaver, S., Kulikouskaya, S., Chandy, T., Ang, E., Murphy, E., Asim, U., Payne, B., Nicholas, J., Waller, A., Owen, A., Tan, Z. X., Ross, R., Wellington, J., ... Szakmany, T. (2019). Real World Patterns of Antimicrobial Use and Microbiology Investigations in Patients with Sepsis outside the Critical Care Unit: Secondary Analysis of Three Nation-Wide Point Prevalence Studies. Journal of Clinical Medicine, 8(9), 1337. https://doi.org/10.3390/jcm8091337