Low Muscle Mass as a Prognostic Factor for Early Postoperative Outcomes in Pediatric Patients Undergoing the Fontan Operation: A Retrospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants and Measurements
2.2. Clinical Variables and Postoperative Outcomes
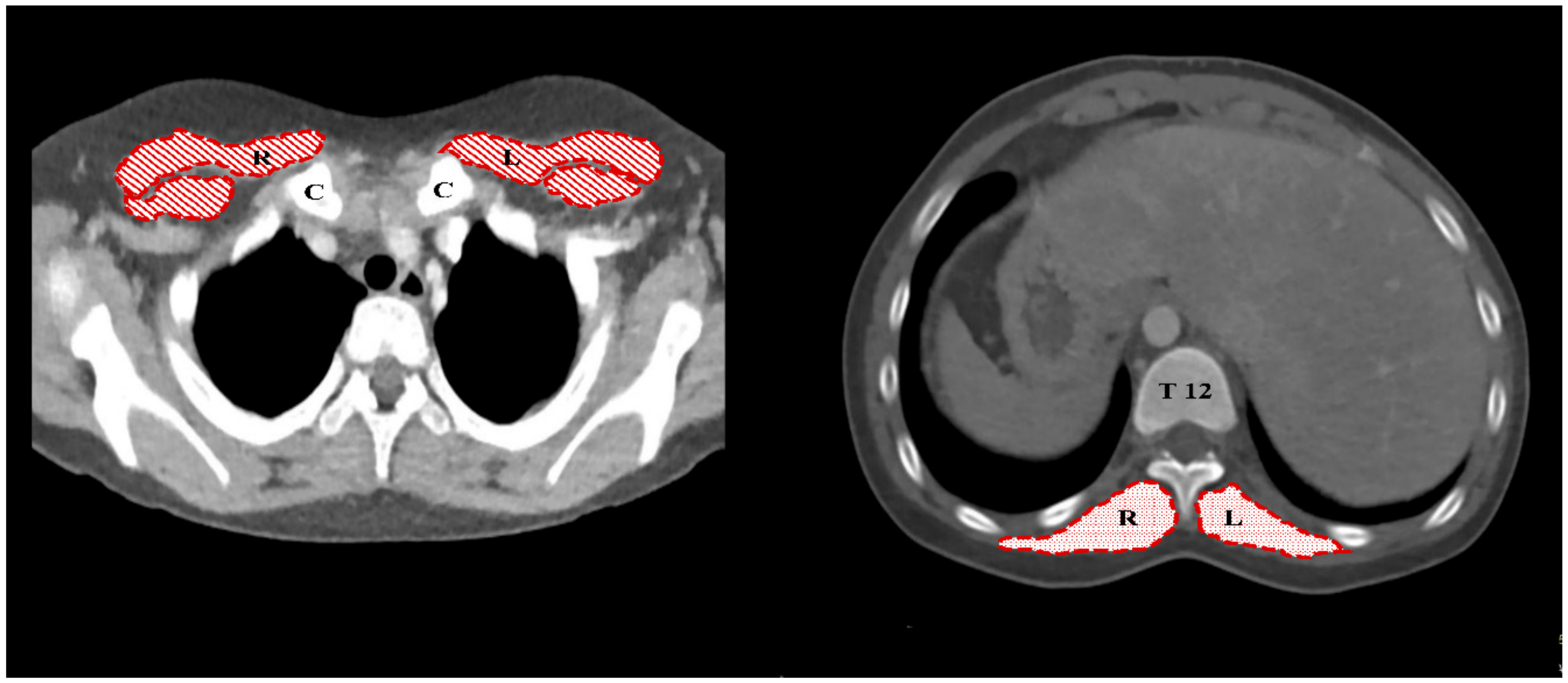
2.3. Skeletal Muscle Mass Measurement Using Chest CT and the Definition of Low Muscle Mass
2.4. Statistical Analysis
3. Results
3.1. Study Population
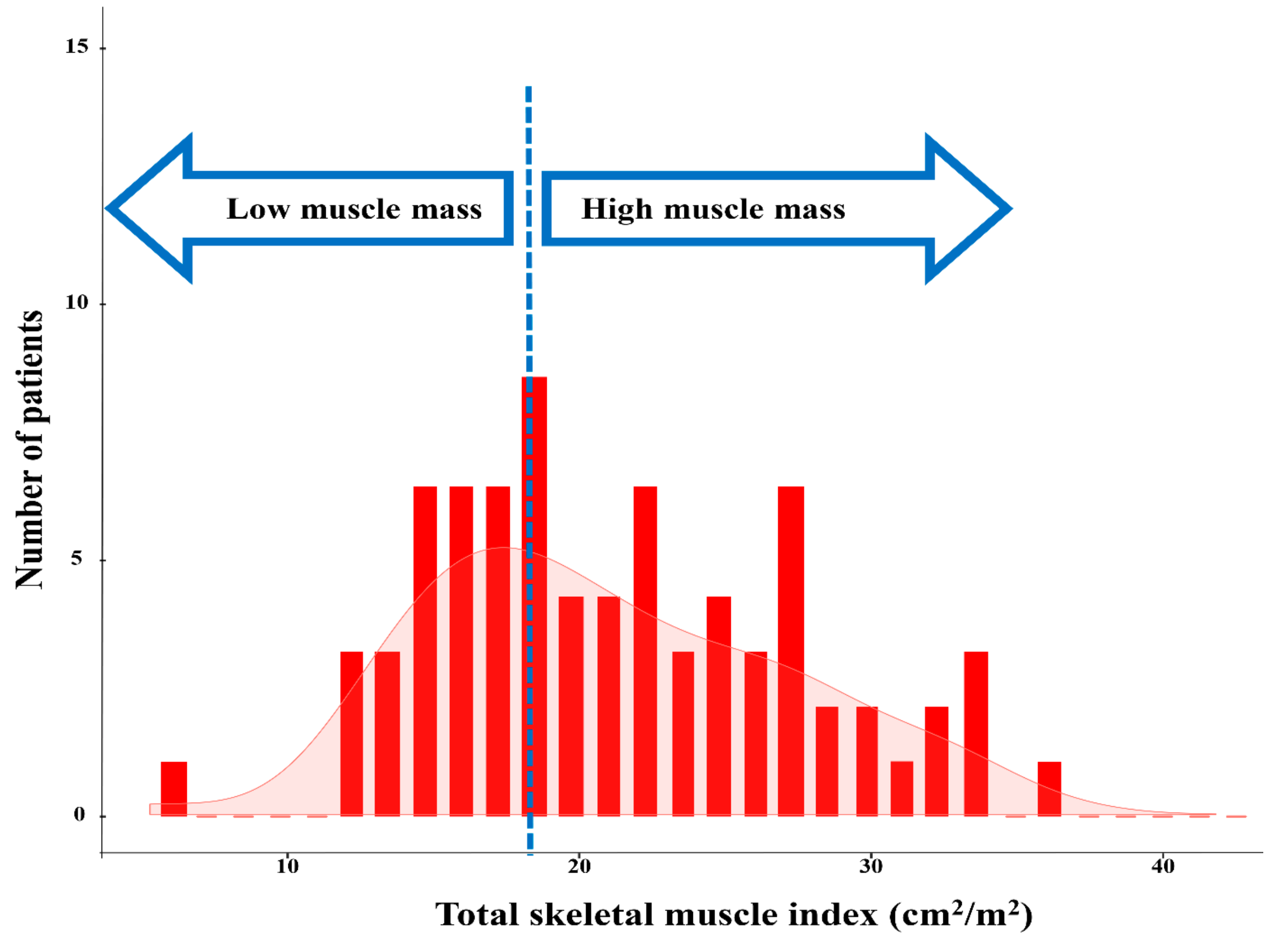
3.2. Low Muscle Mass Assessment
3.3. Correlation Between Low Muscle Mass and Early Postoperative Complications
3.4. Association between Low Muscle Mass and Poor Postoperative Outcomes
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Ohuchi, H. Adult patients with Fontan circulation: What we know and how to manage adults with Fontan circulation? J. Cardiol. 2016, 68, 181–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Mourik, M.S.; Janmaat, Y.C.; van Kesteren, F.; Vendrik, J.; Planken, R.N.; Henstra, M.J.; Velu, J.F.; Vlastra, W.; Zwinderman, A.H.; Koch, K.T.; et al. CT determined psoas muscle area predicts mortality in women undergoing transcatheter aortic valve implantation. Catheter. Cardiovasc. Interv. 2019, 93, E248–E254. [Google Scholar] [CrossRef] [PubMed]
- Mager, D.R.; Hager, A.; Ooi, P.H.; Siminoski, K.; Gilmour, S.M.; Yap, J.Y.K. Persistence of sarcopenia after pediatric liver transplantation is associated with poorer growth and recurrent hospital admissions. JPEN J. Parenter. Enteral Nutr. 2019, 43, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Choussat, A.; Fontan, F.; Besse, P.; Vallot, F.; Chauve, A.; Bricaud, H. Selection Criteria for Fontan’s Procedure. In Paediatric Cardiology; Anderson, R., Shineborne, E., Eds.; Churchill Livingstone: New York, NY, USA, 1977; pp. 559–566. [Google Scholar]
- Gaies, M.G.; Gurney, J.G.; Yen, A.H.; Napoli, M.L.; Gajarski, R.J.; Ohye, R.G.; Charpie, J.R.; Hirsch, J.C. Vasoactive–inotropic score as a predictor of morbidity and mortality in infants after cardiopulmonary bypass*. Pediatr. Crit. Care Med. 2010, 11, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Goo, H.W. Image quality and radiation dose of high-pitch dual-source spiral cardiothoracic computed tomography in young children with congenital heart disease: Comparison of non-electrocardiography synchronization and prospective electrocardiography triggering. Korean J. Radiol. 2018, 19, 1031–1041. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.A.; Harris, K.; Roche, C.; Dhillon, S.; Battoo, A.; Demmy, T.; Nwogu, C.E.; Dexter, E.U.; Hennon, M.; Picone, A.; et al. Sarcopenia is a predictor of outcomes after lobectomy. J. Thorac. Dis. 2018, 10, 432–440. [Google Scholar] [CrossRef] [Green Version]
- Khairy, P.; Fernandes, S.M.; Mayer, J.E.; Triedman, J.K.; Walsh, E.P.; Lock, J.E.; Landzberg, M.J. Long-term survival, modes of death, and predictors of mortality in patients with Fontan surgery. Circulation 2008, 117, 85–92. [Google Scholar] [CrossRef]
- Iyengar, A.J.; Winlaw, D.S.; Galati, J.C.; Wheaton, G.R.; Gentles, T.L.; Grigg, L.E.; Justo, R.N.; Radford, D.J.; Weintraub, R.G.; Bullock, A.; et al. The extracardiac conduit Fontan procedure in Australia and New Zealand: Hypoplastic left heart syndrome predicts worse early and late outcomes. Eur. J. Cardio-Thoracic Surg. 2014, 46, 465–473. [Google Scholar] [CrossRef]
- Ovroutski, S.; Sohn, C.; Barikbin, P.; Miera, O.; Alexi-Meskishvili, V.; Hübler, M.; Ewert, P.; Hetzer, R.; Berger, F. Analysis of the risk factors for early failure after extracardiac Fontan operation. Ann. Thorac. Surg. 2013, 95, 1409–1416. [Google Scholar] [CrossRef]
- Sundar, P.; Austin, C.; Alphonso, N.; Baghai, M.; Tulloh, R.; Anderson, D. Intermediate-term outcome following the fontan operation: A survival, functional and risk-factor analysis. Eur. J. Cardio-Thoracic Surg. 2005, 28, 529–535. [Google Scholar]
- Rayar, M.; Webber, C.E.; Nayiager, T.; Sala, A.; Barr, R.D. Sarcopenia in children with acute lymphoblastic leukemia. J. Pediatr. Hematol. 2013, 35, 98–102. [Google Scholar] [CrossRef]
- Wong, J.J.; Cheifetz, I.M.; Ong, C.; Nakao, M.; Lee, J.H. Nutrition support for children undergoing congenital heart surgeries: A narrative review. World J. Pediatr. Congenit. Heart Surg. 2015, 6, 443–454. [Google Scholar] [CrossRef]
- Costello, C.L.; Gellatly, M.; Daniel, J.; Justo, R.N.; Weir, K. Growth restriction in infants and young children with congenital heart disease. Congenit. Heart Dis. 2015, 10, 447–456. [Google Scholar] [CrossRef]
- Huysentruyt, K.; Devreker, T.; Dejonckheere, J.; De Schepper, J.; Vandenplas, Y.; Cools, F. The accuracy of nutritional screening tools in assessing the risk of under-nutrition in hospitalized children. J. Pediatr. Gastroenterol. Nutr. 2015, 61, 1–166. [Google Scholar] [CrossRef]
- Chourdakis, M.; Hecht, C.; Gerasimidis, K.; Joosten, K.F.; Karagiozoglou-Lampoudi, T.; A Koetse, H.; Ksiazyk, J.; Lazea, C.; Shamir, R.; Szajewska, H.; et al. Malnutrition risk in hospitalized children: Use of 3 screening tools in a large European population. Am. J. Clin. Nutr. 2016, 103, 1301–1310. [Google Scholar] [CrossRef]
- Cordina, R.; O’Meagher, S.; Gould, H.; Rae, C.; Kemp, G.; A Pasco, J.; Celermajer, D.S. Skeletal muscle abnormalities and exercise capacity in adults with a Fontan circulation. Heart 2013, 99, 1530–1534. [Google Scholar] [CrossRef]
- Zoico, E.; Rossi, A.; Di Francesco, V.; Sepe, A.; Olioso, D.; Pizzini, F.; Fantin, F.; Bosello, O.; Cominacini, L.; Harris, T.B.; et al. Adipose tissue infiltration in skeletal muscle of healthy elderly men: relationships with body composition, insulin resistance, and inflammation at the systemic and tissue level. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 295–299. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef]
- Nemec, U.; Heidinger, B.; Sokas, C.; Chu, L.; Eisenberg, R.L. Diagnosing sarcopenia on thoracic computed tomography: Quantitative assessment of skeletal muscle mass in patients undergoing transcatheter aortic valve replacement. Acad. Radiol. 2017, 24, 1154–1161. [Google Scholar] [CrossRef]
- McCarthy, H.D.; Samani-Radia, D.; Jebb, S.A.; Prentice, A.M. Skeletal muscle mass reference curves for children and adolescents. Pediatr. Obes. 2014, 9, 249–259. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 74) | Low Muscle Mass (n = 31) | High Muscle Mass (n = 43) | |
|---|---|---|---|
| Demographic Variables | |||
| Age, year | 2.9 (2.8–3.3) | 3.0 (2.8–3.0) | 3.0 (2.7–3.5) |
| Sex, male | 38 (51) | 16 (52) | 22 (51) |
| Weight, kg | 14.0 (13.0–15.6) | 13.9 (12.8–14.8) | 14.2 (13.1–16.2) |
| Height, cm | 93.3 (91.3–96.1) | 93.3 (91.7–94.8) | 93.4 (91.2–96.9) |
| Body surface area, m2 | 0.60 (0.58–0.64) | 0.60 (0.58–0.65) | 0.60 (0.57–0.68) |
| Birth weight, kg | 3.17 (2.80–3.46) | 3.10 (2.73–3.37) | 3.19 (2.84–3.49) |
| Premature birth | 11 (15) | 4 (13) | 7 (16) |
| Computed Tomography Measurements | |||
| PMI, cm2/m2 | 13.1 (9.8–15.9) | 9.5 (9.0–10.8) | 15.8 (13.1–17.2) * |
| ESMI, cm2/m2 | 8.6 (6.5–10.5) | 6.3 (5.6–7.0) | 10.4 (8.9–11.7) * |
| TSMI, cm2/m2 | 21.7 (16.9–26.4) | 16.5(14.7–17.8) | 24.9 (22.2–28.8) * |
| Intraoperative Variables | |||
| Anesthesia duration, min | 391 ± 112 | 410 ± 149 | 379 ± 77 |
| Surgical duration, min | 331 ± 107 | 348 ± 140 | 318 ± 75 |
| CPB duration, min | 110 ± 78 | 128 ± 117 | 99 ± 34 |
| VISmax1 | 5.0 (5.0–9.4) | 7.0 (5.0–10.0) | 5.0 (5.0–8.0) * |
| Postoperative Variables | |||
| VISmax2 | 10.0 (5.5–12.5) | 10.0 (7.0–17.5) | 8.0 (5.0–10.0) |
| Duration of MV, h | 20 (13–43) | 22 (16–53) | 17 (13–33) |
| ICU stay, days | 3 (2–7) | 4 (2–9) | 3 (2–4) * |
| Hospital stay, days | 24 (12–30) | 15 (12–45) | 15 (12–20) |
| Major postoperative complications | 21 (28) | 15 (48) | 6 (14) * |
| Univariate | Multivariable | |||
|---|---|---|---|---|
| OR (95% CI) | P | OR (95% CI) | P | |
| Major Postoperative Complications | ||||
| Age, year | 0.70 (0.40–1.21) | 0.202 | ||
| Sex, male | 0.62 (0.20–2.00) | 0.428 | ||
| Body weight, kg | 1.24 (0.97–1.60) | 0.087 | ||
| Premature birth | 1.93 (0.35–10.6) | 0.447 | ||
| CPB duration, min | 1.00 (0.99–1.01) | 0.432 | ||
| TSMI, cm2/m2 | 0.89 (0.81–0.99) | 0.031 | 0.90 (0.82–0.99) | 0.039 |
| Duration of ICU Stay > 5 Days | ||||
| Age, year | 1.17 (0.66–2.06) | 0.585 | ||
| Sex, male | 1.56 (0.47–5.13) | 0.156 | ||
| Body weight, kg | 0.88 (0.69–1.12) | 0.306 | ||
| Premature birth | 4.97 (0.52–47.1) | 0.162 | ||
| CPB duration, min | 1.00 (1.00–1.01) | 0.318 | ||
| TSMI, cm2/m2 | 0.87 (0.78–0.97) | 0.014 | 0.86 (0.77–0.96) | 0.006 |
| Duration of Hospital Stay > 14 days | ||||
| Age, year | 1.35 (0.88–2.08) | 0.175 | ||
| Sex, male | 0.90 (0.31–2.61) | 0.841 | ||
| Body weight, kg | 0.88 (0.73–1.05) | 0.882 | ||
| Premature birth | 2.13 (0.52–8.75) | 0.292 | ||
| CPB duration, min | 1.00 (1.00–1.01) | 0.444 | ||
| TSMI, cm2/m2 | 0.92 (0.85–0.99) | 0.039 | 0.92 (0.85–0.99) | 0.035 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, J.; Shin, W.-J.; Jeong, D.; Yun, T.-J.; Park, C.S.; Choi, E.S.; Choi, J.M.; Gwak, M.; Song, I.-K. Low Muscle Mass as a Prognostic Factor for Early Postoperative Outcomes in Pediatric Patients Undergoing the Fontan Operation: A Retrospective Cohort Study. J. Clin. Med. 2019, 8, 1257. https://doi.org/10.3390/jcm8081257
Oh J, Shin W-J, Jeong D, Yun T-J, Park CS, Choi ES, Choi JM, Gwak M, Song I-K. Low Muscle Mass as a Prognostic Factor for Early Postoperative Outcomes in Pediatric Patients Undergoing the Fontan Operation: A Retrospective Cohort Study. Journal of Clinical Medicine. 2019; 8(8):1257. https://doi.org/10.3390/jcm8081257
Chicago/Turabian StyleOh, Jimi, Won-Jung Shin, DaUn Jeong, Tae-Jin Yun, Chun Soo Park, Eun Seok Choi, Jae Moon Choi, Mijeung Gwak, and In-Kyung Song. 2019. "Low Muscle Mass as a Prognostic Factor for Early Postoperative Outcomes in Pediatric Patients Undergoing the Fontan Operation: A Retrospective Cohort Study" Journal of Clinical Medicine 8, no. 8: 1257. https://doi.org/10.3390/jcm8081257
APA StyleOh, J., Shin, W.-J., Jeong, D., Yun, T.-J., Park, C. S., Choi, E. S., Choi, J. M., Gwak, M., & Song, I.-K. (2019). Low Muscle Mass as a Prognostic Factor for Early Postoperative Outcomes in Pediatric Patients Undergoing the Fontan Operation: A Retrospective Cohort Study. Journal of Clinical Medicine, 8(8), 1257. https://doi.org/10.3390/jcm8081257