Long-Term Neurodevelopmental Outcome in Twin-to-Twin Transfusion Syndrome: Is there still Room for Improvement?

 , and
, and
Abstract
:1. Introduction
2. Experimental Section
Statistical Analysis
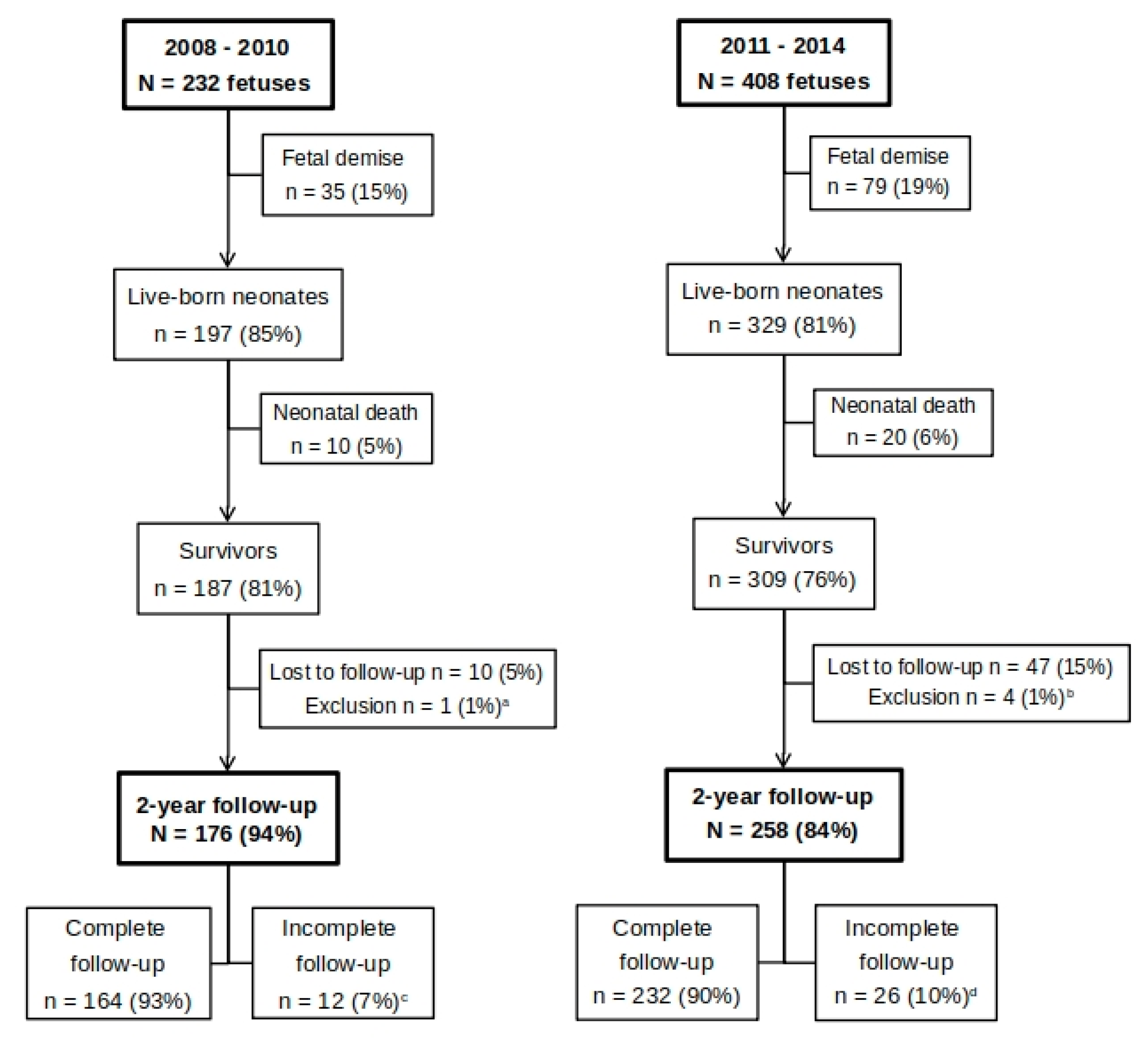
3. Results
3.1. Perinatal Characteristics of Included TTTS Pregnancies
3.2. Long-Term Follow-Up
Neurodevelopmental Outcome
3.3. Risk Factors
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- De Lia, J.E.; Kuhlmann, R.S.; Cruikshank, D.P.; O’Bee, L.R. Placental surgery: A new frontier. Placenta 1993, 14, 477–485. [Google Scholar] [CrossRef]
- Minakami, H.; Honma, Y.; Matsubara, S.; Uchida, A.; Shiraishi, H.; Sato, I. Effects of placental chorionicity on outcome in twin pregnancies. A cohort study. J. Reprod. Med. 1999, 44, 595–600. [Google Scholar] [PubMed]
- Hecher, K.; Plath, H.; Bregenzer, T.; Hansmann, M.; Hackeloer, B.J. Endoscopic laser surgery versus serial amniocenteses in the treatment of severe twin-twin transfusion syndrome. Am. J. Obstet. Gynecol. 1999, 180, 717–724. [Google Scholar] [CrossRef]
- Roberts, D.; Neilson, J.P.; Kilby, M.D.; Gates, S. Interventions for the treatment of twin-twin transfusion syndrome. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.C.; D’Addario, V. Laser therapy and serial amnioreduction as treatment for twin-twin transfusion syndrome: A metaanalysis and review of literature. Am. J. Obstet. Gynecol. 2008, 198, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Senat, M.V.; Deprest, J.; Boulvain, M.; Paupe, A.; Winer, N.; Ville, Y. Endoscopic laser surgery versus serial amnioreduction for severe twin-to-twin transfusion syndrome. N. Engl. J. Med. 2004, 351, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Van Klink, J.M.; Koopman, H.M.; van Zwet, E.W.; Oepkes, D.; Walther, F.J.; Lopriore, E. Cerebral injury and neurodevelopmental impairment after amnioreduction versus laser surgery in twin-twin transfusion syndrome: A systematic review and meta-analysis. Fetal Diagn. Ther. 2013, 33, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Lopriore, E.; Ortibus, E.; Acosta-Rojas, R.; Le Cessie, S.; Middeldorp, J.M.; Oepkes, D.; Gratacos, E.; Vandenbussche, F.P.; Deprest, J.; Walther, F.J.; et al. Risk factors for neurodevelopment impairment in twin-twin transfusion syndrome treated with fetoscopic laser surgery. Obstetr. Gynecol. 2009, 113, 361–366. [Google Scholar] [CrossRef]
- Van Klink, J.M.; Koopman, H.M.; van Zwet, E.W.; Middeldorp, J.M.; Walther, F.J.; Oepkes, D.; Lopriore, E. Improvement in neurodevelopmental outcome in survivors of twin-twin transfusion syndrome treated with laser surgery. Am. J. Obstet. Gynecol. 2014, 210, 540.e1–540.e7. [Google Scholar] [CrossRef]
- Papanna, R.; Biau, D.J.; Mann, L.K.; Johnson, A.; Moise, K.J., Jr. Use of the Learning Curve-Cumulative Summation test for quantitative and individualized assessment of competency of a surgical procedure in obstetrics and gynecology: Fetoscopic laser ablation as a model. Am. J. Obstet. Gynecol. 2011, 204, 218.e1–218.e9. [Google Scholar] [CrossRef]
- Hecher, K.; Gardiner, H.M.; Diemert, A.; Bartmann, P. Long-term outcomes for monochorionic twins after laser therapy in twin-to-twin transfusion syndrome. Lancet Child Adolesc. Health 2018, 2, 525–535. [Google Scholar] [CrossRef]
- Quintero, R.A.; Morales, W.J.; Allen, M.H.; Bornick, P.W.; Johnson, P.K.; Kruger, M. Staging of twin-twin transfusion syndrome. J. Perinatol. 1999, 19, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Wittmann, B.K.; Baldwin, V.J.; Nichol, B. Antenatal diagnosis of twin transfusion syndrome by ultrasound. Obstetr. Gynecol. 1981, 58, 123–127. [Google Scholar]
- Slaghekke, F.; Lopriore, E.; Lewi, L.; Middeldorp, J.M.; van Zwet, E.W.; Weingertner, A.S.; Klumper, F.J.; DeKoninck, P.; Devlieger, R.; Kilby, M.D.; et al. Fetoscopic laser coagulation of the vascular equator versus selective coagulation for twin-to-twin transfusion syndrome: An open-label randomised controlled trial. Lancet 2014, 383, 2144–2151. [Google Scholar] [CrossRef]
- Slaghekke, F.; Kist, W.J.; Oepkes, D.; Pasman, S.A.; Middeldorp, J.M.; Klumper, F.J.; Walther, F.J.; Vandenbussche, F.P.; Lopriore, E. Twin anemia-polycythemia sequence: Diagnostic criteria, classification, perinatal management and outcome. Fetal Diagn. Ther. 2010, 27, 181–190. [Google Scholar] [CrossRef]
- Lopriore, E.; van Wezel-Meijler, G.; Middeldorp, J.M.; Sueters, M.; Vandenbussche, F.P.; Walther, F.J. Incidence, origin, and character of cerebral injury in twin-to-twin transfusion syndrome treated with fetoscopic laser surgery. Am. J. Obstet. Gynecol. 2006, 194, 1215–1220. [Google Scholar] [CrossRef]
- Spruijt, M.; Steggerda, S.; Rath, M.; van Zwet, E.; Oepkes, D.; Walther, F.; Lopriore, E. Cerebral injury in twin-twin transfusion syndrome treated with fetoscopic laser surgery. Obstetr. Gynecol. 2012, 120, 15–20. [Google Scholar] [CrossRef]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef]
- Van Baar, A.L.; Steenis, L.J.; Verhoeven, M.; Hessen, D.J. Bayley-III-NL Technische Handleiding; Pearson Assessment and Information BV.: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Rossi, A.C.; Vanderbilt, D.; Chmait, R.H. Neurodevelopmental outcomes after laser therapy for twin-twin transfusion syndrome: A systematic review and meta-analysis. Obstetr. Gynecol. 2011, 118, 1145–1150. [Google Scholar] [CrossRef]
- Steenis, L.J.; Verhoeven, M.; Hessen, D.J.; van Baar, A.L. Performance of Dutch children on the Bayley III: A comparison study of US and Dutch norms. PloS ONE 2015, 10, e0132871. [Google Scholar] [CrossRef]
- Sharp, M.; DeMauro, S.B. Counterbalanced Comparison of the BSID-II and Bayley-III at Eighteen to Twenty-two Months Corrected Age. J. Dev. Behav. Pediatr. 2017, 38, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Banek, C.S.; Hecher, K.; Hackeloer, B.J.; Bartmann, P. Long-term neurodevelopmental outcome after intrauterine laser treatment for severe twin-twin transfusion syndrome. Am. J. Obstet. Gynecol. 2003, 188, 876–880. [Google Scholar] [CrossRef] [PubMed]
- Korsakissok, M.; Groussolles, M.; Dicky, O.; Alberge, C.; Casper, C.; Azogui-Assouline, C. Mortality, morbidity and 2-years neurodevelopmental prognosis of twin to twin transfusion syndrome after fetoscopic laser therapy: A prospective, 58 patients cohort study. J. Gynecol. Obstet. Hum. Reprod. 2018, 47, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Lenclen, R.; Ciarlo, G.; Paupe, A.; Bussieres, L.; Ville, Y. Neurodevelopmental outcome at 2 years in children born preterm treated by amnioreduction or fetoscopic laser surgery for twin-to-twin transfusion syndrome: Comparison with dichorionic twins. Am. J. Obstet. Gynecol. 2009, 201, 291.e1–291.e5. [Google Scholar] [CrossRef] [PubMed]
- Korzeniewski, S.J.; Allred, E.N.; Joseph, R.M.; Heeren, T.; Kuban, K.C.K.; O’Shea, T.M.; Leviton, A. Neurodevelopment at Age 10 Years of Children Born <28 Weeks with Fetal Growth Restriction. Pediatrics 2017, 140. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.L.; Huppi, P.S.; Mallard, C. The consequences of fetal growth restriction on brain structure and neurodevelopmental outcome. J. Physiol. 2016, 594, 807–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weisz, B.; Hoffmann, C.; Ben-Baruch, S.; Yinon, Y.; Gindes, L.; Katorza, E.; Shrim, A.; Bar Yosef, O.; Schiff, E.; Lipitz, S. Early detection by diffusion-weighted sequence magnetic resonance imaging of severe brain lesions after fetoscopic laser coagulation for twin-twin transfusion syndrome. Ultrasound Obstet. Gynecol. 2014, 44, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Robinson, A.; Teoh, M.; Edwards, A.; Fahey, M.; Goergen, S. Fetal brain injury in complicated monochorionic pregnancies: Diagnostic yield of prenatal MRI following surveillance ultrasound and influence on prognostic counselling. Prenat. Diagn. 2017, 37, 611–627. [Google Scholar] [CrossRef]
- Chmait, R.H.; Chon, A.H.; Schrager, S.M.; Llanes, A.; Hamilton, A.H.; Vanderbilt, D.L. Neonatal cerebral lesions predict 2-year neurodevelopmental impairment in children treated with laser surgery for twin-twin transfusion syndrome. J. Maternal-Fetal Neonat. Med. 2019, 32, 80–84. [Google Scholar] [CrossRef]
- Graeve, P.; Banek, C.; Stegmann-Woessner, G.; Maschke, C.; Hecher, K.; Bartmann, P. Neurodevelopmental outcome at 6 years of age after intrauterine laser therapy for twin-twin transfusion syndrome. Acta Paediatr. 2012, 101, 1200–1205. [Google Scholar] [CrossRef]


{kind=link}
| Previous Cohort: 2008–2010 N = 176 | New Cohort: 2011–2014 N = 258 | p | |
|---|---|---|---|
| Donor | 90 (51) | 130 (50) | 0.685 |
| Gestational age at laser (weeks) | 20.3 ± 3.4 | 20.0 ± 3.4 | 0.663 |
| TTTS stage—median (range) I II III IV | 3 (1–4) 24 (14) 48 (27) 102 (58) 2 (1) | 3 (1–4) 35 (14) 89 (34) 127 (49) 7 (3) | 0.515 |
| Post-laser TAPS or recurrent TTTS | 20/176 (11) | 25/258 (10) | 0.523 |
| Fetal demise of co-twin | 18 (10) | 29 (11) | 0.771 |
| Gestational age at birth (weeks) >37 weeks 33–36 weeks 26–32 weeks 24–25 weeks | 32.4 ± 3.4 16 (9) 74 (42) 86 (49) 0 | 32.9 ± 3.1 21 (8) 116 (45) 112 (43) 9 (3) | 0.516 |
| Birth weight (grams) | 1771 ± 596 | 1826 ± 610 | 0.717 |
| Small for gestational age a | 16 (9) | 22 (9) | 0.835 |
| Severe cerebral injury b | 9 (5) | 11 (4) | 0.681 |
| Female | 95 (54) | 127 (49) | 0.353 |
| Previous Cohort: 2008–2010 N = 176 | New Cohort: 2011–2014 N = 258 | p | |
|---|---|---|---|
| Severe NDI a | 10/169 (6) | 7/241 (3) | 0.189 |
| Disease-free survival b | 162/215 (75%) | 241/340 (71%) | 0.263 |
| Cerebral Palsy Cerebral Palsy grade I Cerebral Palsy grade II–V | 5/176 (3) 1 (1) 4 (2) | 4/258 (2) 3 (1) 1 (0.4) | 0.356 |
| Cognitive composite score | 101 ± 14 | 99 ± 13 | 0.220 |
| Cognitive composite score < −2SD | 5/169 (3) | 1/240 (0.4) | 0.097 |
| Motor composite score | 102 ± 15 | 97 ± 14 | 0.003 |
| Motor composite score < −2SD | 5/164 (3) | 6/234 (3) | 0.723 |
| Risk Factor | Cognitive Composite Score Univariate | Motor Composite Score Univariate | ||
|---|---|---|---|---|
| B (95% CI) | p | B (95% CI) | p | |
| Donor | −1.10 (−2.46–0.27) | 0.115 | 1.29 (−0.67–3.25) | 0.196 |
| TTTS stage | 0.10 (−2.108–2.30) | 0.928 | 0.51 (−1.64–2.66) | 0.642 |
| GA at laser | −0.27 (−0.77–0.23) | 0.291 | −0.13 (−0.66–0.40) | 0.634 |
| Incomplete laser | −2.96 (−8.20–2.28) | 0.268 | −4.65 (−9.69–0.39) | 0.071 |
| Fetal demise co-twin | 3.17 (−1.02–7.36) | 0.138 | 1.89 (−2.71–6.48) | 0.421 |
| GA at birth | 0.49 (−0.01–0.99) | 0.056 | −0.10 (−0.64–0.43) | 0.707 |
| Birth weight a | 0.41 (0.18–0.64) | 0.000 | −0.79 (−0.32–0.16) | 0.521 |
| Growth restriction b | −5.67 (−9.35 to −1.99) | 0.003 | −0.47 (−4.52–3.58) | 0.822 |
| Severe cerebral injury | −2.11 (−8.96–4.73) | 0.545 | −14.10 (−25.04 to −3.16) | 0.012 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spruijt, M.S.; Lopriore, E.; Tan, R.N.G.B.; Slaghekke, F.; Klumper, F.J.C.M.; Middeldorp, J.M.; Haak, M.C.; Oepkes, D.; Rijken, M.; van Klink, J.M.M. Long-Term Neurodevelopmental Outcome in Twin-to-Twin Transfusion Syndrome: Is there still Room for Improvement? J. Clin. Med. 2019, 8, 1226. https://doi.org/10.3390/jcm8081226
Spruijt MS, Lopriore E, Tan RNGB, Slaghekke F, Klumper FJCM, Middeldorp JM, Haak MC, Oepkes D, Rijken M, van Klink JMM. Long-Term Neurodevelopmental Outcome in Twin-to-Twin Transfusion Syndrome: Is there still Room for Improvement? Journal of Clinical Medicine. 2019; 8(8):1226. https://doi.org/10.3390/jcm8081226
Chicago/Turabian StyleSpruijt, Marjolijn S., Enrico Lopriore, Ratna N.G.B. Tan, Femke Slaghekke, Frans J.C.M. Klumper, Johanna M. Middeldorp, Monique C. Haak, Dick Oepkes, Monique Rijken, and Jeanine M.M. van Klink. 2019. "Long-Term Neurodevelopmental Outcome in Twin-to-Twin Transfusion Syndrome: Is there still Room for Improvement?" Journal of Clinical Medicine 8, no. 8: 1226. https://doi.org/10.3390/jcm8081226