The Mediating Effects of Affect on Associations between Impulsivity or Resilience and Internet Gaming Disorder

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Young’s Internet Addiction Test (Y-IAT)
2.2.2. Barratt Impulsiveness Scale-11 (BIS-11)
2.2.3. Connor-Davidson Resilience Scale (CD-RISC)
2.2.4. The Positive and Negative Affect Schedule (PANAS)
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Correlation Analysis of Internet Gaming Disorder Symptoms, Impulsivity, Resilience, and Affect Status
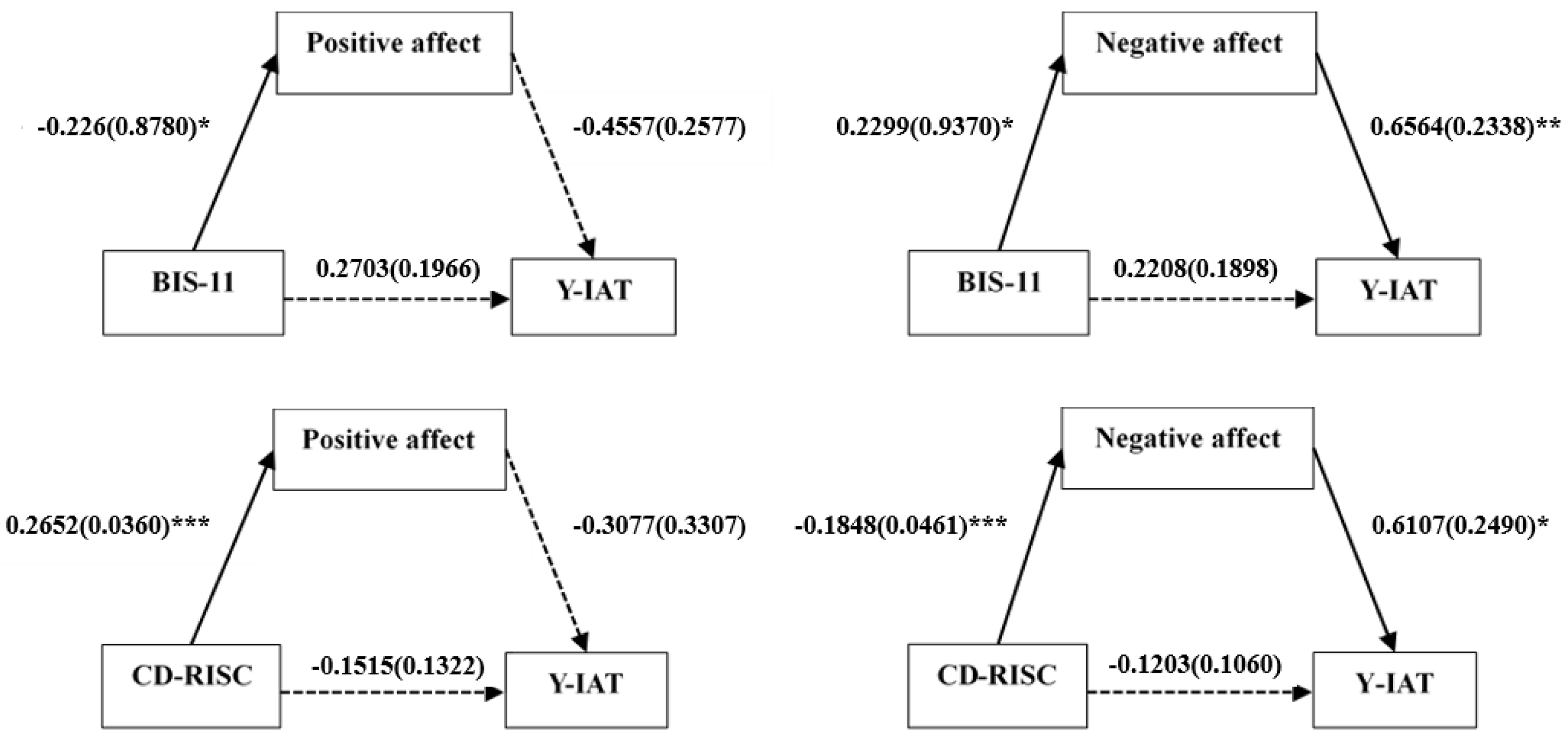
3.3. Mediation Analysis for Relationships between Impulsivity, Resilience, Affect Status, and IGD Symptoms in the IGD Group
3.4. Mediation Analysis for Relationships between Impulsivity, Resilience, Affect, and IGD Symptoms in the HC Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| IGD | Internet gaming disorder |
| HC | Healthy control |
| Y-IAT | Young’s internet addiction test |
| BIS-11 | Barratt impulsiveness scale-11 |
| CD-RISC | Connor-Davidson resilience scale |
| PANAS | The positive and negative affect schedule |
| LLCI | Lower-level confidence interval |
| ULCI | Upper-level confidence interval |
References
- Ng, B.D.; Wiemer-Hastings, P. Addiction to the internet and online gaming. Cyberpsychol. Behav. 2005, 8, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Arlington, V. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Reed, G.M.; First, M.B.; Kogan, C.S.; Hyman, S.E.; Gureje, O.; Gaebel, W.; Maj, M.; Stein, D.J.; Maercker, A.; Tyrer, P.; et al. Innovations and changes in the ICD-11 classification of mental, behavioural and neurodevelopmental disorders. World Psychiatry 2019, 18, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Lemmens, J.S.; Valkenburg, P.M.; Gentile, D.A. The Internet Gaming Disorder Scale. Psychol. Assess. 2015, 27, 567. [Google Scholar] [CrossRef]
- Rehbein, F.; Kliem, S.; Baier, D.; Mossle, T.; Petry, N.M. Prevalence of Internet gaming disorder in German adolescents: Diagnostic contribution of the nine DSM-5 criteria in a state-wide representative sample. Addiction 2015, 110, 842–851. [Google Scholar] [CrossRef] [PubMed]
- Thomas, N.J.; Martin, F.H. Video-arcade game, computer game and Internet activities of Australian students: Participation habits and prevalence of addiction. Aust. J. Psychol. 2010, 62, 59–66. [Google Scholar] [CrossRef]
- Gentile, D. Pathological video-game use among youth ages 8 to 18: A national study. Psychol. Sci. 2009, 20, 594–602. [Google Scholar] [CrossRef]
- Kim, N.R.; Hwang, S.S.; Choi, J.S.; Kim, D.J.; Demetrovics, Z.; Király, O.; Nagygyörgy, K.; Griffiths, M.D.; Hyun, S.Y.; Youn, H.C.; et al. Characteristics and Psychiatric Symptoms of Internet Gaming Disorder among Adults Using Self-Reported DSM-5 Criteria. Psychiatry Investig. 2016, 13, 58–66. [Google Scholar] [CrossRef]
- Crews, F.T.; Boettiger, C.A. Impulsivity, frontal lobes and risk for addiction. Pharmacol. Biochem. Behav. 2009, 93, 237–247. [Google Scholar] [CrossRef]
- Gentile, D.A.; Choo, H.; Liau, A.; Sim, T.; Li, D.; Fung, D.; Khoo, A. Pathological video game use among youths: A two-year longitudinal study. Pediatrics 2011, 127, e319–e329. [Google Scholar] [CrossRef]
- Ryu, H.; Lee, J.Y.; Choi, A.; Park, S.; Kim, D.J.; Choi, J.S. The Relationship between Impulsivity and Internet Gaming Disorder in Young Adults: Mediating Effects of Interpersonal Relationships and Depression. Int. J. Environ. Res. Public Health 2015, 27, 567. [Google Scholar] [CrossRef]
- Choi, S.W.; Kim, H.; Kim, G.Y.; Jeon, Y.; Park, S.; Lee, J.Y.; Jung, H.; Sohn, B.; Choi, J.S.; Kim, D.J. Similarities and differencesamong Internet gaming disorder, gambling disorder and alcohol use disorder: A focus on impulsivity andcompulsivity. J. Behav. Addict. 2014, 3, 246–253. [Google Scholar] [CrossRef]
- Fauth-Bühler, M.; Mann, K. Neurobiological correlates of internet gaming disorder: Similarities to pathological gambling. Addict. Behav. 2017, 64, 349–356. [Google Scholar] [CrossRef]
- Lee, D.; Namkoong, K.; Lee, J.; Jung, Y.C. Abnormal gray matter volume and impulsivity in young adults with Internet gaming disorder. Addict. Biol. 2018, 23, 1160–1167. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Qi, X.; Yang, Y.; Du, G.; Gao, P.; Zhang, Y.; Qin, W.; Li, X.; Zhang, Q. Altered Structural Correlates of Impulsivity in Adolescents with Internet Gaming Disorder. Front. Behav. Neurosci. 2016, 10, 1160–1167. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Chun, J.W.; Park, C.H.; Cho, H.; Choi, J.; Yang, S.; Ahn, K.J. The Correlation between the Frontostriatal Network and Impulsivity in Internet Gaming Disorder. Sci. Rep. 2019, 9, 1191. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Hu, Y.; Xu, J.; Zhou, H.; Lin, X.; Du, X.; Dong, G. Dysfunctional Prefrontal Function Is Associated with Impulsivity in People with Internet Gaming Disorder during a Delay Discounting Task. Front. Psychiatry 2017, 8, 287. [Google Scholar] [CrossRef]
- Yu, H.; Cho, J. Prevalence of Internet Gaming Disorder among Korean Adolescents and Associations with Non-psychotic Psychological Symptoms, and Physical Aggression. Am. J. Health Behav. 2016, 40, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.R.; Cho, H.; Kim, D.J. Prevalence and correlates of comorbid depression in a nonclinical online sample with DSM-5 internet gaming disorder. J. Affect. Disord. 2018, 226, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Tong, K.; Wu, A.; Lau, J.; Zhang, M. The Comorbidity of Gambling Disorder among Macao Adult Residents and the Moderating Role of Resilience and Life Purpose. Int. J. Environ. Res. Public Health 2018, 15, 2774. [Google Scholar] [CrossRef]
- Lin, P.-C.; Su, C.-H.; Yen, J.-Y.; Ko, C.-H. The association between comorbid psychiatric symptoms and remission of internet gaming disorder among college students and non-student adults. Taiwan J. Psychiatry 2016, 30, 279–288. [Google Scholar]
- Dong, G.; Li, H.; Wang, L.; Potenza, M.N. The correlation between mood states and functional connectivity within the default mode network can differentiate Internet gaming disorder from healthy controls. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2017, 77, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Yen, J.Y.; Yeh, Y.C.; Wang, P.W.; Liu, T.L.; Chen, Y.Y.; Ko, C.H. Emotional Regulation in Young Adults with Internet Gaming Disorder. Int. J. Environ. Res. Public Health 2017, 15, 30. [Google Scholar] [CrossRef] [PubMed]
- Southwick, S.M.; Bonanno, G.A.; Masten, A.S.; Panter-Brick, C.; Yehuda, R. Resilience definitions, theory, and challenges: Interdisciplinary perspectives. Eur. J. Psychotraumatology 2014, 5, 25338. [Google Scholar] [CrossRef] [PubMed]
- Tugade, M.M.; Fredrickson, B.L. Resilient individuals use positive emotions to bounce back from negative emotional experiences. J. Personal. Soc. Psychol. 2004, 86, 320. [Google Scholar] [CrossRef] [PubMed]
- Mak, K.K.; Jeong, J.; Lee, H.K.; Lee, K. Mediating Effect of Internet Addiction on the Association between Resilience and Depression among Korean University Students: A Structural Equation Modeling Approach. Psychiatry Investig. 2018, 15, 962–969. [Google Scholar] [CrossRef]
- Lee, J.Y.; Choi, J.S.; Kwon, J.S. Neurophysiological Mechanisms of Resilience as a Protective Factor in Patients with Internet Gaming Disorder: A Resting-State EEG Coherence Study. J. Clin. Med. 2019, 8, 49. [Google Scholar] [CrossRef]
- Son, K.L.; Choi, J.S.; Lee, J.; Park, S.M.; Lim, J.A.; Lee, J.Y.; Kim, S.N.; Oh, S.; Kim, D.J.; Kwon, J.S. Neurophysiological features of Internet gaming disorder and alcohol use disorder: A resting-state EEG study. Transl. Psychiatry 2015, 5, e628. [Google Scholar] [CrossRef]
- Park, M.; Choi, J.-S.; Park, S.M.; Lee, J.-Y.; Jung, H.Y.; Sohn, B.K.; Kim, S.N.; Kwon, J.S. Dysfunctional information processing during an auditory event-related potential task in individuals with Internet gaming disorder. Transl. Psychiatry 2016, 6, e721. [Google Scholar] [CrossRef]
- Davis, M.; Suveg, C. Focusing on the positive: A review of the role of child positive affect in developmental psychopathology. Clin. Child Fam. Psychol. Rev. 2014, 17, 97–124. [Google Scholar] [CrossRef]
- Hirsch, J.K.; Floyd, A.R.; Duberstein, P.R. Perceived health in lung cancer patients: The role of positive and negative affect. Qual. Life Res. 2012, 21, 187–194. [Google Scholar] [CrossRef]
- Seebach, C.L.; Kirkhart, M.; Lating, J.M.; Wegener, S.T.; Song, Y.; Riley, L.H., 3rd; Archer, K.R. Examining the role of positive and negative affect in recovery from spine surgery. Pain 2012, 153, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Xing, C.; Sun, J.M. The role of psychological resilience and positive affect in risky decision-making. Int. J. Psychol. 2013, 48, 935–943. [Google Scholar] [CrossRef] [PubMed]
- Veilleux, J.C.; Conrad, M.; Kassel, J.D. Cue-induced cigarette craving and mixed emotions: A role for positive affect in the craving process. Addict. Behav. 2013, 38, 1881–1889. [Google Scholar] [CrossRef] [PubMed]
- Goschke, T.; Bolte, A. Emotional modulation of control dilemmas: The role of positive affect, reward, and dopamine in cognitive stability and flexibility. Neuropsychologia 2014, 62, 403–423. [Google Scholar] [CrossRef] [PubMed]
- Figueira, J.S.B.; Pacheco, L.B.; Lobo, I.; Volchan, E.; Pereira, M.G.; de Oliveira, L.; David, I.A. “Keep That in Mind!” The Role of Positive Affect in Working Memory for Maintaining Goal-Relevant Information. Front. Psychol. 2018, 9, 1228. [Google Scholar] [CrossRef] [PubMed]
- Ramey, T.; Regier, P.S. Cognitive impairment in substance use disorders. CNS Spectr. 2018, 24, 102–113. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, K.; Hook, R.; Goudriaan, A.E.; Vlies, S.; Fineberg, N.A.; Grant, J.E.; Chamberlain, S.R. Cognitive deficits in problematic internet use: Meta-analysis of 40 studies. Br. J. Psychiatry 2019, 1–8. [Google Scholar] [CrossRef]
- Yao, Y.W.; Chen, P.R.; Li, S.; Wang, L.J.; Zhang, J.T.; Yip, S.W.; Chen, G.; Deng, L.Y.; Liu, Q.X.; Fang, X.Y. Decision-making for risky gains and losses among college students with Internet gaming disorder. PLoS ONE 2015, 10, e0116471. [Google Scholar] [CrossRef]
- Zhang, Y.; Lin, X.; Zhou, H.; Xu, J.; Du, X.; Dong, G. Brain Activity toward Gaming-Related Cues in Internet Gaming Disorder during an Addiction Stroop Task. Front. Psychol. 2016, 7, 714. [Google Scholar] [CrossRef]
- Qi, X.; Du, X.; Yang, Y.; Du, G.; Gao, P.; Zhang, Y.; Qin, W.; Li, X.; Zhang, Q. Decreased modulation by the risk level on the brain activation during decision making in adolescents with internet gaming disorder. Front. Behav. Neurosci. 2015, 9, 296. [Google Scholar] [CrossRef]
- Ko, C.H.; Wang, P.W.; Liu, T.L.; Chen, C.S.; Yen, C.F.; Yen, J.Y. The adaptive decision-making, risky decision, and decision-making style of Internet gaming disorder. Eur. Psychiatry 2017, 44, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wu, L.; Zhou, H.; Lin, X.; Zhang, Y.; Du, X.; Dong, G. Impaired executive control and reward circuit in Internet gaming addicts under a delay discounting task: Independent component analysis. Eur. Arch. Psychiatry Clin. Neurosci. 2017, 267, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Bendahan, S.; Goette, L.; Thoresen, J.; Loued-Khenissi, L.; Hollis, F.; Sandi, C. Acute stress alters individual risk taking in a time-dependent manner and leads to anti-social risk. Eur. J. Neurosci. 2017, 45, 877–885. [Google Scholar] [CrossRef] [PubMed]
- Ellis, B.J.; Bianchi, J.; Griskevicius, V.; Frankenhuis, W.E. Beyond Risk and Protective Factors: An Adaptation-Based Approach to Resilience. Perspect. Psychol. Sci. 2017, 12, 561–587. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T. Cognitive models of depression. Clin. Adv. Cognit. Psychother. Theory Appl. 2002, 14, 29–61. [Google Scholar]
- Teasdale, J.D.; Fennell, M.J. Immediate effects on depression of cognitive therapy interventions. Cognit. Ther. Res. 1982, 6, 343–351. [Google Scholar] [CrossRef]
- Reinecke, M.A.; Ryan, N.E.; DuBOIS, D.L. Cognitive-behavioral therapy of depression and depressive symptoms during adolescence: A review and meta-analysis. J. Am. Acad. Child Adolesc. Psychiatry 1998, 37, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Korthauer, L.E.; Goveas, J.; Espeland, M.A.; Shumaker, S.A.; Garcia, K.R.; Tindle, H.; Salmoirago-Blotcher, E.; Sink, K.M.; Vaughan, L.; Rapp, S.R.; et al. Negative Affect Is Associated With Higher Risk of Incident Cognitive Impairment in Nondepressed Postmenopausal Women. J. Gerontol. Ser. A 2018, 73, 506–512. [Google Scholar] [CrossRef] [PubMed]
- Meynen, G. Depression, possibilities, and competence: A phenomenological perspective. Theor. Med. Bioeth. 2011, 32, 181–193. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Giorgetta, C.; Grecucci, A.; Zuanon, S.; Perini, L.; Balestrieri, M.; Bonini, N.; Sanfey, A.G.; Brambilla, P. Reduced risk-taking behavior as a trait feature of anxiety. Emotion 2012, 12, 1373–1383. [Google Scholar] [CrossRef]
- Broman-Fulks, J.J.; Urbaniak, A.; Bondy, C.L.; Toomey, K.J. Anxiety sensitivity and risk-taking behavior. Anxiety Stress Coping 2014, 27, 619–632. [Google Scholar] [CrossRef] [PubMed]
- Passie, T.; Schneider, U.; Borsutzky, M.; Breyer, R.; Emrich, H.M.; Bandelow, B.; Schmid-Ott, G. Impaired perceptual processing and conceptual cognition in patients with anxiety disorders: A pilot study with the binocular depth inversion paradigm. Psychol. Health Med. 2013, 18, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Vytal, K.; Cornwell, B.; Arkin, N.; Grillon, C. Describing the interplay between anxiety and cognition: From impaired performance under low cognitive load to reduced anxiety under high load. Psychophysiology 2012, 49, 842–852. [Google Scholar] [CrossRef] [PubMed]
- Cadet, J.L. Epigenetics of Stress, Addiction, and Resilience: Therapeutic Implications. Mol. Neurobiol. 2016, 53, 545–560. [Google Scholar] [CrossRef] [PubMed]
- LeDoux, J.E.; Gorman, J.M. A call to action: Overcoming anxiety through active coping. Am. J. Psychiatry 2001, 158, 1953–1955. [Google Scholar] [CrossRef] [PubMed]
- Chiavarino, C.; Rabellino, D.; Ardito, R.B.; Cavallero, E.; Palumbo, L.; Bergerone, S.; Gaita, F.; Bara, B.G. Emotional coping is a better predictor of cardiac prognosis than depression and anxiety. J. Psychosom. Res. 2012, 73, 473–475. [Google Scholar] [CrossRef] [PubMed]
- Chassin, L.; Presson, C.C.; Rose, J.; Sherman, S.J. What is addiction? Age-related differences in the meaning of addiction. Drug Alcohol Depend. 2007, 87, 30–38. [Google Scholar] [CrossRef]
- Ko, C.-H.; Yen, J.-Y.; Chen, C.-C.; Chen, S.-H.; Yen, C.-F. Gender differences and related factors affecting online gaming addiction among Taiwanese adolescents. J. Nerv. Ment. Dis. 2005, 193, 273–277. [Google Scholar] [CrossRef]
- Cohen, S.; Janicki-Deverts, D.; Miller, G.E. Psychological stress and disease. JAMA 2007, 298, 1685–1687. [Google Scholar] [CrossRef]
- Zhao, X.; Lynch, J.G.; Chen, Q. Reconsidering Baron and Kenny: Myths and Truths about Mediation Analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | IGD (n = 71), M ± SD | HC (n = 79), M ± SD | t | p-Value |
|---|---|---|---|---|
| Age | 25.56 ± 5.669 | 25.57 ± 4.593 | −0.007 | 0.994 |
| Y-IAT | 57.45 ± 15.979 | 35.89 ± 14.587 | 8.641 *** | <0.001 |
| BIS-11 | 66.35 ± 9.811 | 57.96 ± 9.830 | 5.224 *** | <0.001 |
| CD-RISC | 50.79 ± 18.723 | 66.11 ± 16.534 | −5.324 *** | <0.001 |
| PANAS-Positive | 24.55 ± 7.485 | 30.28 ± 6.567 | −4.993 *** | <0.001 |
| PANAS-Negative | 27.32 ± 7.966 | 21.72 ± 7.546 | 4.422 *** | <0.001 |
| IGD (n = 71) | Y-IAT | BIS-11 | CD-RISC | PANAS-Positive | PANAS-Negative |
| Y-IAT | 1 | ||||
| BIS-11 | 0.228 | 1 | |||
| CD-RISC | −0.273 * | −0.442 *** | 1 | ||
| PANAS-Positive | −0.262 * | −0.292 * | 0.663 *** | 1 | |
| PANAS-Negative | 0.366 ** | 0.283 | −0.434 *** | −0.055 | 1 |
| HC (n = 79) | Y-IAT | BIS-11 | CD-RISC | PANAS-Positive | PANAS-Negative |
| Y-IAT | 1 | ||||
| BIS-11 | 0.262 * | 1 | |||
| CD-RISC | −0.459 *** | −0.601 *** | 1 | ||
| PANAS-Positive | −0.330 ** | −0.315 ** | 0.551 *** | 1 | |
| PANAS-Negative | 0.343 ** | 0.516 *** | −0.511 *** | −0.200 | 1 |
| Paths | Boot Indirect Effect | Boot SE | LLCI | ULCI |
|---|---|---|---|---|
| Impulsivity → positive affect → IGD | 0.1014 | 0.0737 | 0.0014 | 0.3088 |
| Impulsivity → negative affect → IGD | 0.1509 | 0.0790 | 0.0317 | 0.3505 |
| Resilience → positive affect → IGD | −0.0816 | 0.0804 | −0.2753 | 0.0530 |
| Resilience → negative affect → IGD | −0.1129 | 0.0519 | −0.2427 | −0.0296 |
| Paths | Boot Indirect Effect | Boot SE | LLCI | ULCI |
|---|---|---|---|---|
| Impulsivity → positive affect → IGD | 0.1284 | 0.0803 | 0.0154 | 0.3351 |
| Impulsivity → negative affect → IGD | 0.2167 | 0.1333 | −0.0112 | 0.5268 |
| Resilience → positive affect → IGD | −0.0537 | 0.0721 | −0.1991 | 0.0835 |
| Resilience → negative affect → IGD | −0.0661 | 0.0649 | −0.2084 | 0.0457 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, D.; Choi, A.R.; Lee, J.; Chung, S.J.; Kim, B.; Park, M.; Jung, M.H.; Kim, D.J.; Choi, J.-S. The Mediating Effects of Affect on Associations between Impulsivity or Resilience and Internet Gaming Disorder. J. Clin. Med. 2019, 8, 1102. https://doi.org/10.3390/jcm8081102
Shin D, Choi AR, Lee J, Chung SJ, Kim B, Park M, Jung MH, Kim DJ, Choi J-S. The Mediating Effects of Affect on Associations between Impulsivity or Resilience and Internet Gaming Disorder. Journal of Clinical Medicine. 2019; 8(8):1102. https://doi.org/10.3390/jcm8081102
Chicago/Turabian StyleShin, Daun, A Ruem Choi, Jiyoon Lee, Sun Ju Chung, Bomi Kim, Minkyung Park, Myung Hun Jung, Dai Jin Kim, and Jung-Seok Choi. 2019. "The Mediating Effects of Affect on Associations between Impulsivity or Resilience and Internet Gaming Disorder" Journal of Clinical Medicine 8, no. 8: 1102. https://doi.org/10.3390/jcm8081102
APA StyleShin, D., Choi, A. R., Lee, J., Chung, S. J., Kim, B., Park, M., Jung, M. H., Kim, D. J., & Choi, J.-S. (2019). The Mediating Effects of Affect on Associations between Impulsivity or Resilience and Internet Gaming Disorder. Journal of Clinical Medicine, 8(8), 1102. https://doi.org/10.3390/jcm8081102