Metabolic Obesity Phenotypes and Risk of Cellulitis: A Cohort Study


Abstract
:1. Introduction
2. Methods
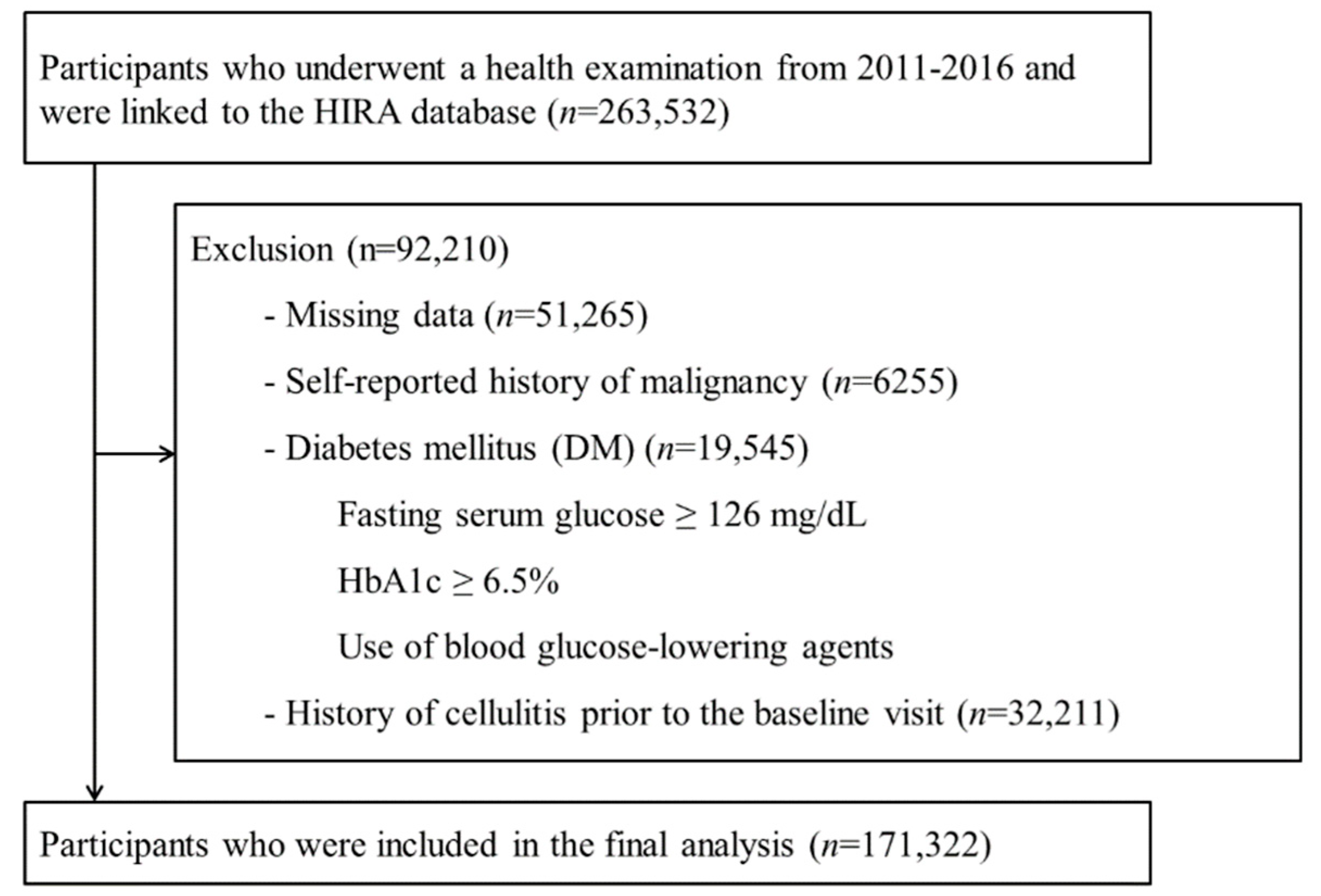
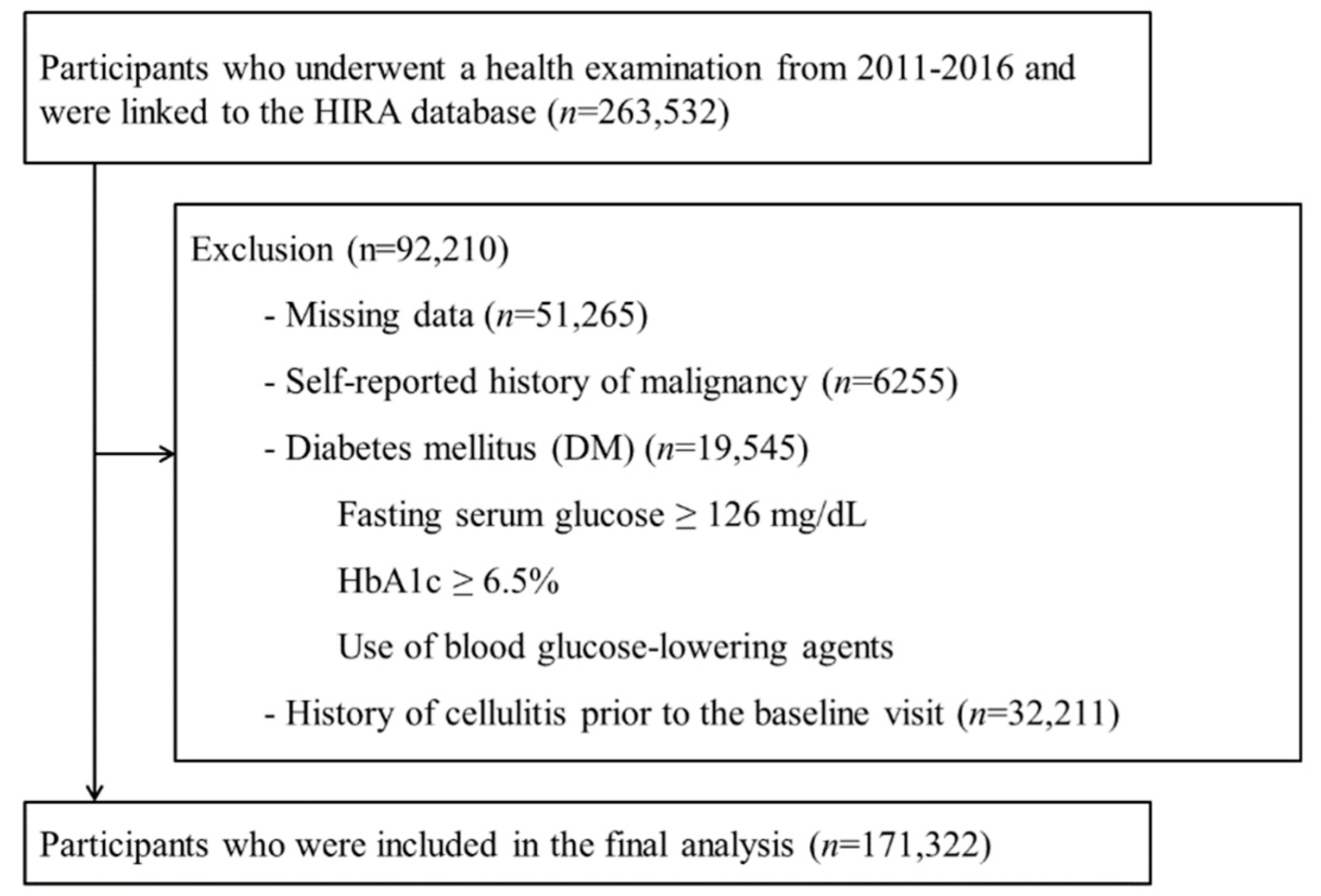
2.1. Study Population
2.2. Measurements
2.3. Ascertainment of Cellulitis, Cellulitis-Related Hospitalization, and Comorbidity Index
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bjornsdottir, S.; Gottfredsson, M.; Thorisdottir, A.S.; Gunnarsson, G.B.; Rikardsdottir, H.; Kristjansson, M.; Hilmarsdottir, I. Risk factors for acute cellulitis of the lower limb: A prospective case-control study. Clin. Infect. Dis. 2005, 41, 1416–1422. [Google Scholar] [CrossRef] [PubMed]
- Raff, A.B.; Kroshinsky, D. Cellulitis: A Review. JAMA 2016, 316, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Cranendonk, D.R.; Lavrijsen, A.P.M.; Prins, J.M.; Wiersinga, W.J. Cellulitis: Current insights into pathophysiology and clinical management. Neth. J. Med. 2017, 75, 366–378. [Google Scholar] [PubMed]
- Jenkins, T.C.; Sabel, A.L.; Sarcone, E.E.; Price, C.S.; Mehler, P.S.; Burman, W.J. Skin and soft-tissue infections requiring hospitalization at an academic medical center: Opportunities for antimicrobial stewardship. Clin. Infect. Dis. 2010, 51, 895–903. [Google Scholar] [CrossRef] [PubMed]
- Hersh, A.L.; Chambers, H.F.; Maselli, J.H.; Gonzales, R. National trends in ambulatory visits and antibiotic prescribing for skin and soft-tissue infections. Arch. Intern. Med. 2008, 168, 1585–1591. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Available online: http://www.who.int/classifications/icd/en/ (accessed on 3 March 2019).
- Seidell, J.C.; Halberstadt, J. The global burden of obesity and the challenges of prevention. Ann. Nutr. Metab. 2015, 66 (Suppl. 2), 7–12. [Google Scholar] [CrossRef]
- Falagas, M.E.; Kompoti, M. Obesity and infection. Lancet Infect. Dis. 2006, 6, 438–446. [Google Scholar] [CrossRef]
- Conway, E.L.; Sellick, J.A.; Kurtzhalts, K.; Mergenhagen, K.A. Obesity and Heart Failure as Predictors of Failure in Outpatient Skin and Soft Tissue Infections. Antimicrob. Agents Chemother. 2017, 61, 1–7. [Google Scholar] [CrossRef]
- Zhang, J.; Moore, E.; Bousfield, R. OPAT for cellulitis: Its benefits and the factors that predispose to longer treatment. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1013–1015. [Google Scholar] [CrossRef]
- Dupuy, A.; Benchikhi, H.; Roujeau, J.C.; Bernard, P.; Vaillant, L.; Chosidow, O.; Sassolas, B.; Guillaume, J.C.; Grob, J.J.; Bastuji-Garin, S. Risk factors for erysipelas of the leg (cellulitis): Case-control study. BMJ 1999, 318, 1591–1594. [Google Scholar] [CrossRef]
- Njim, T.; Aminde, L.N.; Agbor, V.N.; Toukam, L.D.; Kashaf, S.S.; Ohuma, E.O. Risk factors of lower limb cellulitis in a level-two healthcare facility in Cameroon: A case-control study. BMC Infect. Dis. 2017, 17, 418. [Google Scholar] [CrossRef] [PubMed]
- Karppelin, M.; Siljander, T.; Vuopio-Varkila, J.; Kere, J.; Huhtala, H.; Vuento, R.; Jussila, T.; Syrjanen, J. Factors predisposing to acute and recurrent bacterial non-necrotizing cellulitis in hospitalized patients: A prospective case-control study. Clin. Microbiol. Infect. 2010, 16, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Kaspersen, K.A.; Pedersen, O.B.; Petersen, M.S.; Hjalgrim, H.; Rostgaard, K.; Moller, B.K.; Juul-Sorensen, C.; Kotze, S.; Dinh, K.M.; Erikstrup, L.T.; et al. Obesity and risk of infection: Results from the Danish Blood Donor Study. Epidemiology 2015, 26, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Primeau, V.; Coderre, L.; Karelis, A.D.; Brochu, M.; Lavoie, M.E.; Messier, V.; Sladek, R.; Rabasa-Lhoret, R. Characterizing the profile of obese patients who are metabolically healthy. Int. J. Obes. 2011, 35, 971–981. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Kantartzis, K.; Machann, J.; Schick, F.; Thamer, C.; Rittig, K.; Balletshofer, B.; Machicao, F.; Fritsche, A.; Haring, H.U. Identification and characterization of metabolically benign obesity in humans. Arch. Intern. Med. 2008, 168, 1609–1616. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Ryu, S.; Choi, Y.; Zhang, Y.; Cho, J.; Kwon, M.J.; Hyun, Y.Y.; Lee, K.B.; Kim, H.; Jung, H.S.; et al. Metabolically Healthy Obesity and Development of Chronic Kidney Disease: A Cohort Study. Ann. Intern. Med. 2016, 164, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Kim, B.K.; Yun, K.E.; Cho, J.; Zhang, Y.; Rampal, S.; Zhao, D.; Jung, H.S.; Choi, Y.; Ahn, J.; et al. Metabolically-healthy obesity and coronary artery calcification. J. Am. Coll. Cardiol. 2014, 63, 2679–2686. [Google Scholar] [CrossRef] [PubMed]
- Park, J.T.; Kim, B.G.; Jhun, H.J. Alcohol consumption and the CAGE questionnaire in Korean adults: Results from the Second Korea National Health and Nutrition Examination Survey. J. Korean Med. Sci. 2008, 23, 199–206. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Ryu, S.; Chang, Y.; Jung, H.S.; Yun, K.E.; Kwon, M.J.; Choi, Y.; Kim, C.W.; Cho, J.; Suh, B.S.; Cho, Y.K.; et al. Relationship of sitting time and physical activity with non-alcoholic fatty liver disease. J. Hepatol. 2015, 63, 1229–1237. [Google Scholar] [CrossRef]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; Regional Office for the Western Pacific. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000. [Google Scholar]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S. Payment system reform for health care providers in Korea. Health Policy Plan. 2003, 18, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Harpsoe, M.C.; Nielsen, N.M.; Friis-Moller, N.; Andersson, M.; Wohlfahrt, J.; Linneberg, A.; Nohr, E.A.; Jess, T. Body Mass Index and Risk of Infections Among Women in the Danish National Birth Cohort. Am. J. Epidemiol. 2016, 183, 1008–1017. [Google Scholar] [CrossRef] [PubMed]
- Wolf, A.M.; Wolf, D.; Rumpold, H.; Enrich, B.; Tilg, H. Adiponectin induces the anti-inflammatory cytokines IL-10 and IL-1RA in human leukocytes. Biochem. Biophys. Res. Commun. 2004, 323, 630–635. [Google Scholar] [CrossRef] [PubMed]
- Ozata, M.; Ozdemir, I.C.; Licinio, J. Human leptin deficiency caused by a missense mutation: Multiple endocrine defects, decreased sympathetic tone, and immune system dysfunction indicate new targets for leptin action, greater central than peripheral resistance to the effects of leptin, and spontaneous correction of leptin-mediated defects. J. Clin. Endocrinol. Metab. 1999, 84, 3686–3695. [Google Scholar] [PubMed]
- Yosipovitch, G.; DeVore, A.; Dawn, A. Obesity and the skin: Skin physiology and skin manifestations of obesity. J. Am. Acad. Dermatol. 2007, 56, 901–916, quiz 917–920. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, C. BMI, fat mass, abdominal adiposity and visceral fat: Where is the ‘beef’? Int. J. Obes. 2007, 31, 1552–1553. [Google Scholar] [CrossRef]
- Kim, J.A.; Yoon, S.; Kim, L.Y.; Kim, D.S. Towards Actualizing the Value Potential of Korea Health Insurance Review and Assessment (HIRA) Data as a Resource for Health Research: Strengths, Limitations, Applications, and Strategies for Optimal Use of HIRA Data. J. Korean Med. Sci. 2017, 32, 718–728. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef]
- GBD 2015 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1603–1658. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | Overall | BMI Category (kg/m2) | p for Trend | ||||
|---|---|---|---|---|---|---|---|
| <18.5 | 18.5–22.9 | 23–24.9 | 25–29.9 | ≥30 | |||
| Number | 171,322 | 9982 | 77,595 | 38,177 | 40,499 | 5069 | |
| Age (years) 1 | 37.9 (8) | 34.5 (6.5) | 37.2 (7.7) | 39.1 (8.4) | 39 (8.2) | 36.7 (7.4) | <0.001 |
| Male (%) | 54 | 12.1 | 36.5 | 70.7 | 79.6 | 75 | <0.001 |
| Fatty liver (%) | 25.9 | 0.5 | 7.4 | 29.5 | 57 | 84.3 | <0.001 |
| Current smoker (%) | 22.5 | 7.9 | 15.6 | 27.0 | 32.8 | 34.5 | <0.001 |
| Alcohol intake (%) 2 | 23.2 | 8.1 | 15.9 | 27.8 | 34.5 | 35.7 | <0.001 |
| HEPA (%) | 16.3 | 10.3 | 15.4 | 17.9 | 17.8 | 16.8 | <0.001 |
| Higher education (%) 3 | 79.7 | 79 | 79.5 | 80.5 | 80.2 | 75.7 | 0.675 |
| Systolic BP (mmHg) 1 | 109.1 (12.9) | 99.5 (9.8) | 104.7 (11.5) | 111.5 (11.7) | 116 (11.9) | 121.9 (12.9) | <0.001 |
| Diastolic BP (mmHg) 1 | 69.8 (9.8) | 64.4 (7.8) | 66.9 (8.8) | 71.2 (9.4) | 74.2 (9.8) | 77.1 (10.5) | <0.001 |
| Glucose (mg/dL) 1 | 93.3 (8.4) | 89.1 (7.5) | 91.4 (7.8) | 94.4 (8.1) | 96.2 (8.5) | 98 (9) | <0.001 |
| Total cholesterol (mg/dL) 1 | 193.2 (33.9) | 178 (28.7) | 186.4 (31.6) | 197.6 (33.7) | 203.9 (34.8) | 207.3 (35.6) | <0.001 |
| LDL-C (mg/dL) 1 | 119.6 (31.8) | 98.5 (24.5) | 111.3 (29.1) | 125.9 (30.9) | 132.7 (31.5) | 136.4 (31.6) | <0.001 |
| HDL-C (mg/dL) 1 | 58.9 (15.1) | 70.7 (14.3) | 63.8 (14.7) | 55.7 (13.3) | 51 (12.1) | 47.3 (10.9) | <0.001 |
| Triglycerides (mg/dL) 4 | 89 (63–131) | 62 (50–79) | 73 (56–101) | 100 (72–142) | 126 (89–179) | 149 (106–210) | <0.001 |
| ALT (U/L) 4 | 18 (12–27) | 12 (10–16) | 14 (11–20) | 20 (14–28) | 26 (18–39) | 37 (25–60) | <0.001 |
| hsCRP (mg/L) 4 | 0.4 (0.2–0.9) | 0.2 (0.2–0.4) | 0.3 (0.2–0.6) | 0.5 (0.3–0.9) | 0.7 (0.4–1.3) | 1.3 (0.7–2.6) | <0.001 |
| HOMA-IR 4 | 1.16 (0.77–1.72) | 0.80 (0.53–1.16) | 0.96 (0.65–1.37) | 1.21 (0.84–1.71) | 1.62 (1.13–2.28) | 2.67 (1.88–3.78) | <0.001 |
| Total energy intake (kcal/d) 2,5 | 1491.2 (1098.9–1899.6) | 1362.0 (991.0–1747.1) | 1435.7 (1049.0–1830.5) | 1527.6 (1138.9–1934.9) | 1584.3 (1192.6–2011.2) | 1652.9 (1236.3–2154.0) | <0.001 |
| Charlson comorbidity index | |||||||
| 1–2 (%) | 0.14 | 0.11 | 0.12 | 0.13 | 0.17 | 0.18 | 0.018 |
| ≥3 (%) | 0.01 | 0 | 0.01 | 0.01 | 0 | 0.02 | 0.756 |
| BMI Category (kg/m2) | Person-Years | Incident Cases | Incidence Rate (Cases per 1000 person-years) | Age- and Sex-Adjusted HR (95% CI) | Multivariable-Adjusted HR 1 (95% CI) | |
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | |||||
| Total (n = 171,322) | ||||||
| <18.5 | 36,448.7 | 834 | 22.9 | 1.07 (0.99–1.15) | 1.07 (1–1.15) | 1.06 (0.98–1.14) |
| 18.5–22.9 | 289,945.1 | 6315 | 21.8 | 1 (reference) | 1 (reference) | 1 (reference) |
| 23–24.9 | 144,254.6 | 3415 | 23.7 | 1.07 (1.03–1.12) | 1.07 (1.02–1.11) | 1.08 (1.04–1.13) |
| 25–29.9 | 150,300.0 | 3648 | 24.3 | 1.1 (1.05–1.15) | 1.09 (1.04–1.13) | 1.12 (1.07–1.18) |
| ≥30 | 17,292.1 | 460 | 26.6 | 1.22 (1.11–1.34) | 1.19 (1.08–1.31) | 1.28 (1.15–1.42) |
| p for trend | <0.001 | <0.001 | <0.001 | |||
| Metabolically healthy phenotype (n = 93,520) | ||||||
| <18.5 | 30,930.5 | 708 | 22.9 | 1.05 (0.97–1.14) | 1.06 (0.98–1.15) | 1.04 (0.96–1.13) |
| 18.5–22.9 | 198,867.9 | 4352 | 21.9 | 1 (reference) | 1 (reference) | 1 (reference) |
| 23–24.9 | 65,448.3 | 1609 | 24.6 | 1.12 (1.05–1.19) | 1.11 (1.04–1.17) | 1.13 (1.06–1.20) |
| 25–29.9 | 43,176.6 | 1022 | 23.7 | 1.08 (1–1.16) | 1.06 (0.99–1.14) | 1.1 (1.02–1.19) |
| ≥30 | 2109.4 | 58 | 27.5 | 1.26 (0.97–1.63) | 1.23 (0.95–1.60) | 1.31 (1.01–1.71) |
| p for trend | 0.013 | 0.0573 | 0.005 | |||
| Metabolically unhealthy phenotype (n = 77,802) | ||||||
| <18.5 | 5518.2 | 126 | 22.8 | 1.09 (0.91–1.30) | 1.1 (0.92–1.32) | 1.08 (0.9–1.3) |
| 18.5–22.9 | 91,077.2 | 1963 | 21.6 | 1 (reference) | 1 (reference) | 1 (reference) |
| 23–24.9 | 78,806.4 | 1806 | 22.9 | 1.05 (0.98–1.12) | 1.04 (0.97–1.11) | 1.05 (0.98–1.12) |
| 25–29.9 | 107,123.4 | 2626 | 24.5 | 1.12 (1.05–1.19) | 1.10 (1.04–1.17) | 1.13 (1.05–1.2) |
| ≥30 | 15,182.7 | 402 | 26.5 | 1.23 (1.1–1.37) | 1.20 (1.08–1.34) | 1.26 (1.12–1.42) |
| p for trend | <0.001 | <0.001 | <0.001 | |||
| BMI Category (kg/m2) | Person-Years | Incident Cases | Incidence Rate (cases per 100,000 person-years) | Age- and Sex-Adjusted HR (95% CI) | Multivariable-Adjusted HR 1 (95% CI) | |
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | |||||
| Total (n = 171,322) | ||||||
| <18.5 | 38,246.8 | 3 | 7.8 | 0.54 (0.17–1.73) | 0.55 (0.17–1.75) | 0.57 (0.18–1.83) |
| 18.5–22.9 | 303,902.3 | 54 | 17.8 | 1.00 (reference) | 1 (reference) | 1 (reference) |
| 23–24.9 | 151,692.7 | 53 | 34.9 | 1.59 (1.07–2.35) | 1.55 (1.05–2.3) | 1.48 (0.99–2.21) |
| 25–29.9 | 158,308.2 | 94 | 59.4 | 2.58 (1.8–3.68) | 2.47 (1.73–3.53) | 2.21 (1.5–3.26) |
| ≥30 | 18,305.5 | 21 | 114.7 | 5.22 (3.11–8.73) | 4.80 (2.86–8.05) | 3.78 (2.1–6.81) |
| p for trend | <0.001 | <0.001 | <0.001 | |||
| Metabolically healthy phenotype (n = 93,520) | ||||||
| <18.5 | 32,421.6 | 3 | 9.3 | 0.83 (0.25–2.77) | 0.82 (0.25–2.74) | 0.78 (0.23–2.6) |
| 18.5–22.9 | 208,329.0 | 27 | 13 | 1 (reference) | 1 (reference) | 1 (reference) |
| 23–24.9 | 68,842.8 | 22 | 32 | 2.01 (1.12–3.61) | 2.01 (1.12–3.61) | 2.16 (1.19–3.93) |
| 25–29.9 | 45,368.5 | 33 | 72.7 | 4.38 (2.54–7.54) | 4.31 (2.51–7.42) | 4.96 (2.74–8.99) |
| ≥30 | 2233.1 | 0 | – | – | – | – |
| p for trend | <0.001 | <0.001 | <0.001 | |||
| Metabolically unhealthy phenotype (n = 77,802) | ||||||
| <18.5 | 5825.2 | 0 | – | – | – | – |
| 18.5–22.9 | 95,573.3 | 27 | 28.3 | 1 (reference) | 1 (reference) | 1 (reference) |
| 23–24.9 | 82,849.9 | 31 | 37.4 | 1.15 (0.68–1.94) | 1.12 (0.66–1.9) | 1.04 (0.61–1.77) |
| 25–29.9 | 112,939.7 | 61 | 54 | 1.61 (1.01–2.58) | 1.55 (0.97–2.48) | 1.31 (0.8–2.14) |
| ≥30 | 16,072.4 | 21 | 130.7 | 4.12 (2.31–7.36) | 3.86 (2.15–6.92) | 2.77 (1.45–5.29) |
| p for trend | <0.001 | <0.001 | 0.006 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheong, H.S.; Chang, Y.; Joo, E.-J.; Cho, A.; Ryu, S. Metabolic Obesity Phenotypes and Risk of Cellulitis: A Cohort Study. J. Clin. Med. 2019, 8, 953. https://doi.org/10.3390/jcm8070953
Cheong HS, Chang Y, Joo E-J, Cho A, Ryu S. Metabolic Obesity Phenotypes and Risk of Cellulitis: A Cohort Study. Journal of Clinical Medicine. 2019; 8(7):953. https://doi.org/10.3390/jcm8070953
Chicago/Turabian StyleCheong, Hae Suk, Yoosoo Chang, Eun-Jung Joo, Ara Cho, and Seungho Ryu. 2019. "Metabolic Obesity Phenotypes and Risk of Cellulitis: A Cohort Study" Journal of Clinical Medicine 8, no. 7: 953. https://doi.org/10.3390/jcm8070953
APA StyleCheong, H. S., Chang, Y., Joo, E.-J., Cho, A., & Ryu, S. (2019). Metabolic Obesity Phenotypes and Risk of Cellulitis: A Cohort Study. Journal of Clinical Medicine, 8(7), 953. https://doi.org/10.3390/jcm8070953