Clinical Value of Muscle Mass Assessment in Clinical Conditions Associated with Malnutrition


Abstract
1. Introduction
2. Methods to Assess Muscle Mass in Clinical Practice
2.1. Mid-Arm Muscle Circumference
2.2. Bioelectrical Impedance Analysis
2.3. Dual-Energy X-ray Absorptiometry
2.4. Computed Tomography
3. Impact of Muscle Mass on Clinical Outcomes
3.1. Chronic Diseases
3.1.1. Chronic Obstructive Pulmonary Disease
3.1.2. Chronic Heart Failure
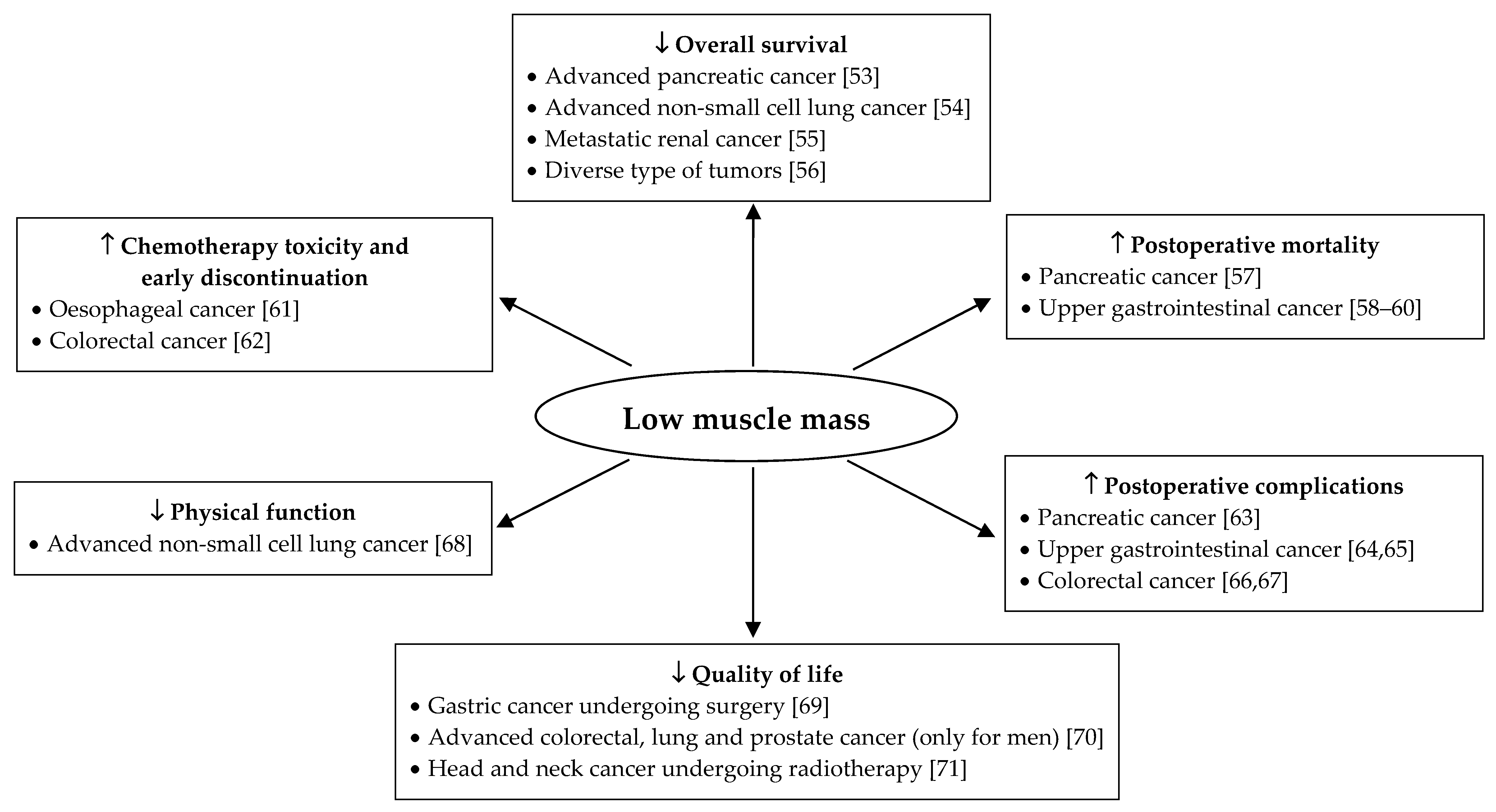
3.1.3. Cancer
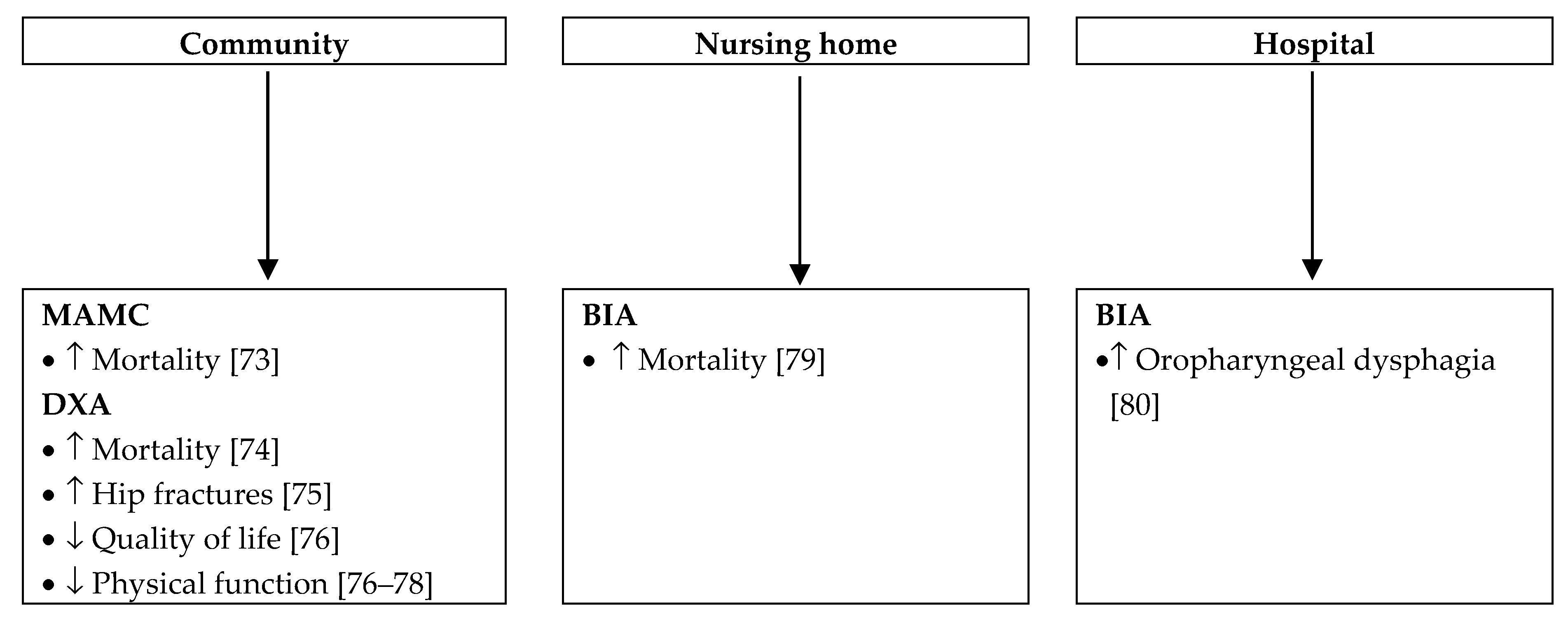
3.2. Older Adults
4. Improvement in Muscle Mass: Strategies and Clinical Benefits
4.1. Chronic Diseases
4.1.1. Chronic Obstructive Pulmonary Disease
4.1.2. Chronic Heart Failure
4.1.3. Cancer
4.2. Older Adults
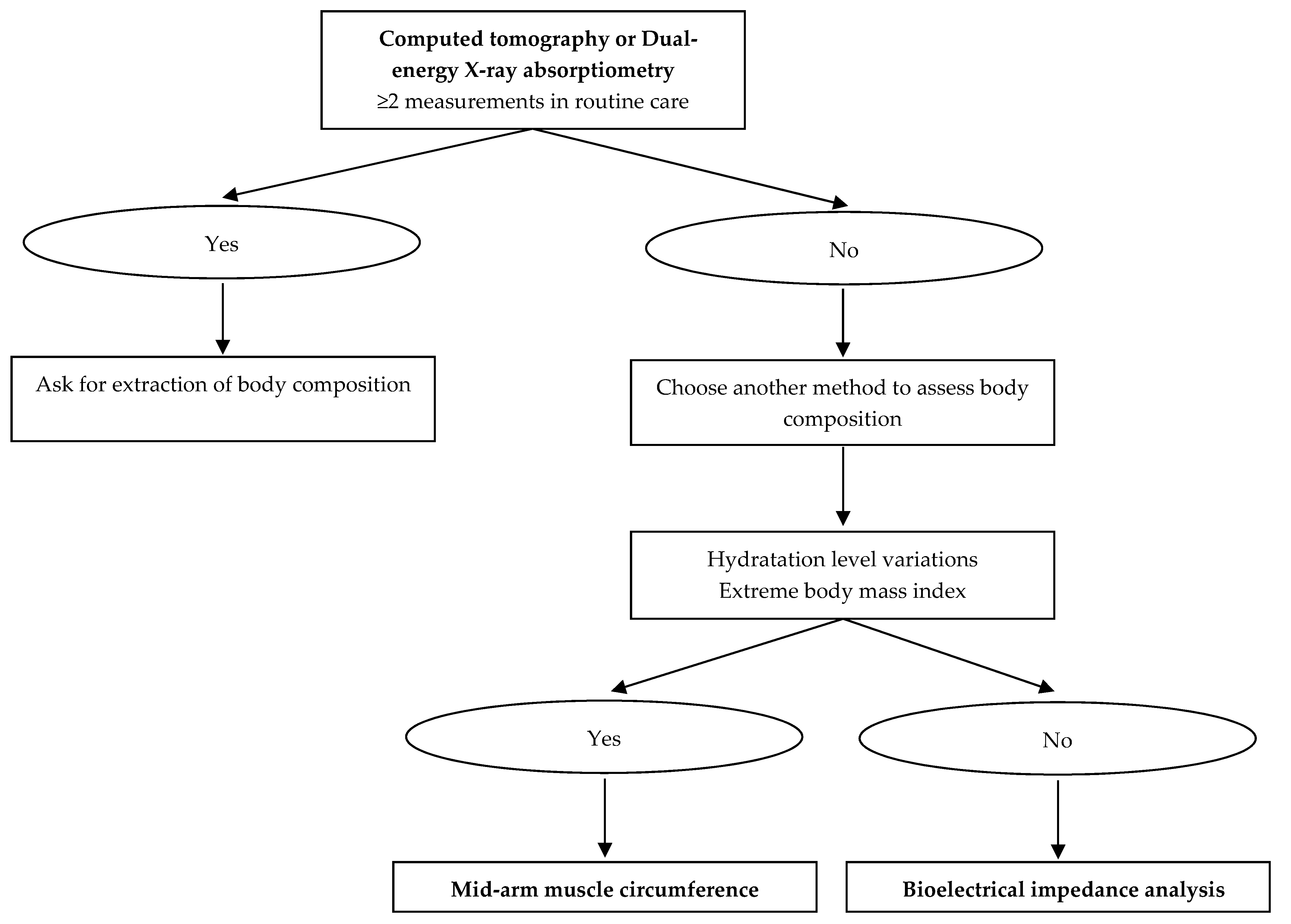
5. Use of Body Composition in Clinical Practice
6. Conclusions
Author Contributions
Conflicts of Interest
Abbreviations
| GLIM | Global Leadership Initiative on Malnutrition |
| BMI | body mass index |
| MAMC | mid-arm muscle circumference |
| BIA | bioelectrical impedance analysis |
| DXA | dual-energy X-ray absorptiometry |
| CT | computed tomography |
| FFM | fat-free mass |
| ASMM | appendicular skeletal muscle mass |
| FFMI | fat-free mass index |
| ASMMI | appendicular skeletal muscle mass index |
| SMI | skeletal muscle index |
| COPD | chronic obstructive pulmonary disease |
| CHF | chronic heart failure |
| BNP | brain natriuretic peptide |
| GOLD | Global Initiative for Obstructive Lung Disease |
| BODE | Body mass index/Airflow obstruction/Dyspnea/Exercise capacity |
| REE | resting energy expenditure |
References
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Ljungqvist, O.; Van Gossum, A.; Sanz, M.L.; De Man, F. The European fight against malnutrition. Clin. Nutr. 2010, 29, 149–150. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Pichard, C.; Lochs, H.; Pirlich, M. Prognostic impact of disease-related malnutrition. Clin. Nutr. 2008, 27, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Jensen, G.; Correia, M.; Gonzalez, M.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. J. Cachexia Sarcopenia Muscle 2019, 10, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Bigaard, J.; Frederiksen, K.; Tjønneland, A.; Thomsen, B.L.; Overvad, K.; Heitmann, B.L.; Sørensen, T.I. Body Fat and Fat-Free Mass and All-Cause Mortality. Obes. Res. 2004, 12, 1042–1049. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.C.; Pastore, C.A.; Orlandi, S.P.; Heymsfield, S.B. Obesity paradox in cancer: New insights provided by body composition. Am. J. Clin. Nutr. 2014, 99, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Janssens, J.-P.; Rochat, T.; Raguso, C.A.; Pichard, C. Body composition in patients with chronic hypercapnic respiratory failure. Respir. Med. 2006, 100, 244–252. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Leal, V.O.; Moraes, C.; Stockler-Pinto, M.B.; Lobo, J.C.; Farage, N.E.; Velarde, L.G.; Fouque, D.; Mafra, D. Is a body mass index of 23 kg/m2 a reliable marker of protein–energy wasting in hemodialysis patients? Nutrition 2012, 28, 973–977. [Google Scholar] [CrossRef] [PubMed]
- Scafoglieri, A.; Provyn, S.; Bautmans, I.; Van Roy, P.; Clarys, J.P. Direct relationship of body mass index and waist circumference with body tissue distribution in elderly persons. J. Nutr. Health Aging 2011, 15, 924–931. [Google Scholar] [CrossRef]
- Seidell, J.C.; Oosterlee, A.; Thijssen, M.A.; Burema, J.; Deurenberg, P.; Hautvast, J.G.; Ruijs, J.H. Assessment of intra-abdominal and subcutaneous abdominal fat: Relation between anthropometry and computed tomography. Am. J. Clin. Nutr. 1987, 45, 7–13. [Google Scholar] [CrossRef]
- Guglielmi, G.; Ponti, F.; Agostini, M.; Amadori, M.; Battista, G.; Bazzocchi, A. The role of DXA in sarcopenia. Aging Clin. Exp. Res. 2016, 28, 1047–1060. [Google Scholar] [CrossRef] [PubMed]
- Antonelli Incalzi, R.; Landi, F.; Cipriani, L.; Bruno, E.; Pagano, F.; Gemma, A.; Capparella, O.; Carbonin, P. Nutritional assessment: A primary component of multidimensional geriatric assessment in the acute care setting. J. Am. Geriatr. Soc. 1996, 44, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, V.; Castriotta, V.; Piscitelli, P.A.; Nieddu, L.; Mattera, M.; Guglielmi, G.; Scillitani, A. Assessment of Skeletal Muscle Mass in Older People: Comparison Between 2 Anthropometry-Based Methods and Dual-Energy X-ray Absorptiometry. J. Am. Med. Dir. Assoc. 2018, 19, 793–796. [Google Scholar] [CrossRef] [PubMed]
- Noori, N.; Kopple, J.D.; Kovesdy, C.P.; Feroze, U.; Sim, J.J.; Murali, S.B.; Luna, A.; Gomez, M.; Luna, C.; Bross, R.; et al. Mid-Arm Muscle Circumference and Quality of Life and Survival in Maintenance Hemodialysis Patients. Clin. J. Am. Soc. Nephrol. 2010, 5, 2258–2268. [Google Scholar] [CrossRef] [PubMed]
- Wijnhoven, H.A.; de Boer, M.R.; van Maanen, M.J.; van Dongen, D.M.; Kraaij, S.F.; Smit, T.; Visser, M. Reproducibility of measurements of mid-upper arm circumference in older persons. J. Hum. Nutr. Diet. 2013, 26, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Duren, D.L.; Sherwood, R.J.; Czerwinski, S.A.; Lee, M.; Choh, A.C.; Siervogel, R.M.; Chumlea, W.C. Body Composition Methods: Comparisons and Interpretation. J. Diabetes Sci. Technol. 2008, 2, 1139–1146. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical impedance analysis?part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Genton, L.; Karsegard, L.; Slosman, D.O.; Pichard, C. Single prediction equation for bioelectrical impedance analysis in adults aged 20–94 years. Nutr. 2001, 17, 248–253. [Google Scholar] [CrossRef]
- Kyle, U.; Genton, L.; Hans, D.; Pichard, C. Validation of a bioelectrical impedance analysis equation to predict appendicular skeletal muscle mass (ASMM). Clin. Nutr. 2003, 22, 537–543. [Google Scholar] [CrossRef]
- Bosaeus, I.; Wilcox, G.; Rothenberg, E.; Strauss, B.J. Skeletal muscle mass in hospitalized elderly patients: Comparison of measurements by single-frequency BIA and DXA. Clin. Nutr. 2014, 33, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Peniche, D.B.R.; Giorguli, G.R.; Alemán-Mateo, H. Accuracy of a predictive bioelectrical impedance analysis equation for estimating appendicular skeletal muscle mass in a non-Caucasian sample of older people. Arch. Gerontol. Geriatr. 2015, 61, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Diaz, E.O.; Villar, J.; Immink, M.; Gonzales, T. Bioimpedance or anthropometry? Eur. J. Clin. Nutr. 1989, 43, 129–137. [Google Scholar] [PubMed]
- Kyle, U.G.; Genton, L.; Slosman, D.O.; Pichard, C. Fat-free and fat mass percentiles in 5225 healthy subjects aged 15 to 98 years. Nutrition 2001, 17, 534–541. [Google Scholar] [CrossRef]
- Norman, K.; Stobäus, N.; Pirlich, M.; Bosy-Westphal, A. Bioelectrical phase angle and impedance vector analysis—Clinical relevance and applicability of impedance parameters. Clin. Nutr. 2012, 31, 854–861. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical impedance analysis—part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef] [PubMed]
- Andreoli, A.; Garaci, F.; Cafarelli, F.P.; Guglielmi, G. Body composition in clinical practice. Eur. J. Radiol. 2016, 85, 1461–1468. [Google Scholar] [CrossRef] [PubMed]
- Deutz, N.E.; Ashurst, I.; Ballesteros, M.D.; Bear, D.E.; Cruz-Jentoft, A.J.; Genton, L.; Landi, F.; Laviano, A.; Norman, K.; Prado, C.M. The Underappreciated Role of Low Muscle Mass in the Management of Malnutrition. J. Am. Med. Dir. Assoc. 2019, 20, 22–27. [Google Scholar] [CrossRef]
- Genton, L.; Hans, D.; Kyle, U.G.; Pichard, C. Dual-Energy X-ray absorptiometry and body composition: Differences between devices and comparison with reference methods. Nutrition 2002, 18, 66–70. [Google Scholar] [CrossRef]
- Andreoli, A.; Scalzo, G.; Masala, S.A.; Tarantino, U.; Guglielmi, G. Body composition assessment by dual-energy X-ray absorptiometry (DXA). La Radiol. Med. 2009, 114, 286–300. [Google Scholar] [CrossRef]
- Kelly, T.; Berger, N.; Richardson, T. DXA body composition: Theory and practice. Appl. Radiat. Isot. 1998, 49, 511–513. [Google Scholar] [CrossRef]
- Bredella, M.A.; Ghomi, R.H.; Thomas, B.J.; Torriani, M.; Brick, D.J.; Gerweck, A.V.; Misra, M.; Klibanski, A.; Miller, K.K. Comparison of DXA and CT in the Assessment of Body Composition in Premenopausal Women with Obesity and Anorexia Nervosa. Obesity 2010, 18, 2227–2233. [Google Scholar] [CrossRef] [PubMed]
- Amini, B.; Boyle, S.P.; Boutin, R.D.; Lenchik, L. Approaches to Assessment of Muscle Mass and Myosteatosis on Computed Tomography (CT): A Systematic Review. J. Gerontol. Ser. A 2019. [Google Scholar] [CrossRef] [PubMed]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; Macdonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Shen, W.; Punyanitya, M.; Wang, Z.; Gallagher, D.; St-Onge, M.P.; Albu, J.; Heymsfield, S.B.; Heshka, S. Total body skeletal muscle and adipose tissue volumes: Estimation from a single abdominal cross-sectional image. J. Appl. Physiol. 2004, 97, 2333–2338. [Google Scholar] [CrossRef] [PubMed]
- Mattsson, S.; Thomas, B.J. Development of methods for body composition studies. Phys. Med. Boil. 2006, 51, R203–R228. [Google Scholar] [CrossRef] [PubMed]
- Heymsfield, S.B.; Wang, Z.; Baumgartner, R.N.; Ross, R. Human Body Composition: Advances in Models and Methods. Annu. Rev. Nutr. 1997, 17, 527–558. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Heymsfield, S.B. Lean tissue imaging: A new era for nutritional assessment and intervention. JPEN J. Parenter Enter. Nutr. 2014, 38, 940–953. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Birdsell, L.A.; Baracos, V.E. The emerging role of computerized tomography in assessing cancer cachexia. Curr. Opin. Support. Palliat. Care 2009, 3, 269–275. [Google Scholar] [CrossRef]
- Visser, M.; Fuerst, T.; Lang, T.; Salamone, L.; Harris, T.B. Validity of fan-beam dual-energy X-ray absorptiometry for measuring fat-free mass and leg muscle mass. Health, aging, and body composition study--dual-energy X-ray absorptiometry and body composition working group. J. Appl. Physiol. 1999, 87, 1513–1520. [Google Scholar] [CrossRef]
- Hickson, M. Malnutrition and ageing. Postgrad. Med. J. 2006, 82, 2–8. [Google Scholar] [CrossRef]
- Von Haehling, S.; Anker, M.S.; Anker, S.D. Prevalence and clinical impact of cachexia in chronic illness in Europe, USA, and Japan: Facts and numbers update 2016. J. Cachexia Sarcopenia Muscle 2016, 7, 507–509. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Lopez, A.D. Measuring the Global Burden of Disease. N. Engl. J. Med. 2013, 369, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Narumi, T.; Arimoto, T.; Funayama, A.; Kadowaki, S.; Otaki, Y.; Nishiyama, S.; Takahashi, H.; Shishido, T.; Miyashita, T.; Miyamoto, T.; et al. The prognostic importance of objective nutritional indexes in patients with chronic heart failure. J. Cardiol. 2013, 62, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Montes de Oca, M.; Talamo, C.; Perez-Padilla, R.; Jardim, J.R.; Muino, A.; Lopez, M.V.; Valdivia, G.; Pertuzé, J.; Moreno, D.; Halbert, R.J.; et al. Chronic obstructive pulmonary disease and body mass index in five Latin America cities: The PLATINO study. Respir. Med. 2008, 102, 642–650. [Google Scholar] [CrossRef] [PubMed]
- Michallet, M.; De Montreuil, C.B.; Hébuterne, X.; Lemarié, E.; Schneider, S.M.; Goldwasser, F. Prevalence of Malnutrition and Current Use of Nutrition Support in Patients with Cancer. J. Parenter. Enter. Nutr. 2014, 38, 196–204. [Google Scholar] [CrossRef]
- Costa, T.M.R.L.; Costa, F.M.; Jonasson, T.H.; Moreira, C.A.; Boguszewski, C.L.; Borba, V.Z.C. Body composition and sarcopenia in patients with chronic obstructive pulmonary disease. Endocrine 2018, 60, 95–102. [Google Scholar] [CrossRef]
- Matkovic, Z.; Cvetko, D.; Rahelic, D.; Esquinas, C.; Zarak, M.; Miravitlles, M.; Tudoric, N. Nutritional Status of Patients with Chronic Obstructive Pulmonary Disease in Relation to their Physical Performance. COPD J. Chronic Obstr. Pulm. Dis. 2017, 14, 626–634. [Google Scholar] [CrossRef]
- Celli, B.R.; Locantore, N.; Tal-Singer, R.; Riley, J.; Miller, B.; Vestbo, J.; Yates, J.C.; Silverman, E.K.; Owen, C.A.; Divo, M.; et al. Emphysema and extrapulmonary tissue loss in COPD: A multi-organ loss of tissue phenotype. Eur. Respir. J. 2018, 51. [Google Scholar] [CrossRef]
- Bekfani, T.; Pellicori, P.; Morris, D.A.; Ebner, N.; Valentova, M.; Steinbeck, L.; Wachter, R.; Elsner, S.; Sliziuk, V.; Schefold, J.C.; et al. Sarcopenia in patients with heart failure with preserved ejection fraction: Impact on muscle strength, exercise capacity and quality of life. Int. J. Cardiol. 2016, 222, 41–46. [Google Scholar] [CrossRef]
- Tsuchida, K.; Fujihara, Y.; Hiroki, J.; Hakamata, T.; Sakai, R.; Nishida, K.; Sudo, K.; Tanaka, K.; Hosaka, Y.; Takahashi, K.; et al. Significance of Sarcopenia Evaluation in Acute Decompensated Heart Failure. Int. Heart J. 2018, 59, 143–148. [Google Scholar] [CrossRef]
- Sanada, K.; Miyachi, M.; Tanimoto, M.; Yamamoto, K.; Murakami, H.; Okumura, S.; Gando, Y.; Suzuki, K.; Tabata, I.; Higuchi, M. A cross-sectional study of sarcopenia in Japanese men and women: Reference values and association with cardiovascular risk factors. Eur. J. Appl. Physiol. 2010, 110, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Doust, J.A.; Pietrzak, E.; Dobson, A.; Glasziou, P. How well does B-type natriuretic peptide predict death and cardiac events in patients with heart failure: Systematic review. BMJ 2005, 330, 625. [Google Scholar] [CrossRef] [PubMed]
- Bian, X.; Dai, H.; Feng, J.; Ji, H.; Fang, Y.; Jiang, N.; Li, W.; Liu, Y. Prognostic values of abdominal body compositions on survival in advanced pancreatic cancer. Medicine 2018, 97, e10988. [Google Scholar] [CrossRef] [PubMed]
- Sjøblom, B.; Grønberg, B.H.; Wentzel-Larsen, T.; Baracos, V.E.; Hjermstad, M.J.; Aass, N.; Bremnes, R.M.; Fløtten, Ø.; Bye, A.; Jordhøy, M. Skeletal muscle radiodensity is prognostic for survival in patients with advanced non-small cell lung cancer. Clin. Nutr. 2016, 35, 1386–1393. [Google Scholar] [CrossRef] [PubMed]
- Gu, W.; Wu, J.; Liu, X.; Zhang, H.; Shi, G.; Zhu, Y.; Ye, D. Early skeletal muscle loss during target therapy is a prognostic biomarker in metastatic renal cell carcinoma patients. Sci. Rep. 2017, 7, 7587. [Google Scholar] [CrossRef] [PubMed]
- Otten, L.; Stobäus, N.; Franz, K.; Genton, L.; Müller-Werdan, U.; Wirth, R.; Norman, K. Impact of sarcopenia on 1-year mortality in older patients with cancer. Age Ageing 2019, 48, 413–418. [Google Scholar] [CrossRef] [PubMed]
- El Amrani, M.; Vermersch, M.; Fulbert, M.; Prodeau, M.; Lecolle, K.; Hebbar, M.; Ernst, O.; Pruvot, F.-R.; Truant, S. Impact of sarcopenia on outcomes of patients undergoing pancreatectomy: A retrospective analysis of 107 patients. Medicine 2018, 97, e12076. [Google Scholar] [CrossRef]
- Choi, M.H.; Kim, K.A.; Hwang, S.S.; Byun, J.Y.; Schaller, B. CT-quantified muscle and fat change in patients after surgery or endoscopic resection for early gastric cancer and its impact on long-term outcomes. Medicine 2018, 97, e13878. [Google Scholar] [CrossRef]
- Kudou, K.; Saeki, H.; Nakashima, Y.; Edahiro, K.; Korehisa, S.; Taniguchi, D.; Tsutsumi, R.; Nishimura, S.; Nakaji, Y.; Akiyama, S.; et al. Prognostic Significance of Sarcopenia in Patients with Esophagogastric Junction Cancer or Upper Gastric Cancer. Ann. Surg. Oncol. 2017, 24, 1804–1810. [Google Scholar] [CrossRef]
- Park, H.S.; Kim, H.S.; Beom, S.H.; Rha, S.Y.; Chung, H.C.; Kim, J.H.; Chun, Y.J.; Lee, S.W.; Choe, E.-A.; Heo, S.J.; et al. Marked Loss of Muscle, Visceral Fat, or Subcutaneous Fat After Gastrectomy Predicts Poor Survival in Advanced Gastric Cancer: Single-Center Study from the CLASSIC Trial. Ann. Surg. Oncol. 2018, 25, 3222–3230. [Google Scholar] [CrossRef]
- Anandavadivelan, P.; Brismar, T.B.; Nilsson, M.; Johar, A.M.; Martin, L. Sarcopenic obesity: A probable risk factor for dose limiting toxicity during neo-adjuvant chemotherapy in oesophageal cancer patients. Clin. Nutr. 2016, 35, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Feliciano, E.M.C.; Lee, V.S.; Prado, C.M.; Meyerhardt, J.A.; Alexeeff, S.; Kroenke, C.H.; Xiao, J.; Castillo, A.L.; Caan, B.J. Muscle mass at diagnosis of non-metastatic colon cancer and early discontinuation of chemotherapy, delays and dose reductions on adjuvant FOLFOX: The C-SCANS Study. Cancer 2017, 123, 4868–4877. [Google Scholar] [CrossRef] [PubMed]
- Pecorelli, N.; Capretti, G.; Sandini, M.; Damascelli, A.; Cristel, G.; De Cobelli, F.; Gianotti, L.; Zerbi, A.; Braga, M. Impact of sarcopenic obesity on failure to rescue from major complications following pancreaticoduodenectomy for cancer: Results from a multicenter study. Ann. Surg. Oncol. 2018, 25, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.-J.; Zhang, F.-M.; Zhang, F.-Y.; Yu, Z.; Chen, X.-L.; Shen, X.; Zhuang, C.-L.; Chen, X.-X. Sarcopenia: A new predictor of postoperative complications for elderly gastric cancer patients who underwent radical gastrectomy. J. Surg. Res. 2017, 211, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Elliott, J.A.; Doyle, S.L.; Murphy, C.F.; King, S.; Guinan, E.M.; Beddy, P.; Ravi, N.; Reynolds, J.V. Sarcopenia: Prevalence, and impact on operative and oncologic outcomes in the multimodal management of locally advanced esophageal cancer. Ann. Surg. 2017, 266, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Van Vugt, J.L.A.; Coebergh van den Braak, R.R.J.; Lalmahomed, Z.S.; Vrijland, W.W.; Dekker, J.W.T.; Zimmerman, D.D.E.; Vles, W.J.; Coene, P.-P.L.O.; IJzermans, J.N.M. Impact of low skeletal muscle mass and density on short and long-term outcome after resection of stage I-III colorectal cancer. Eur. J. Surg. Oncol. 2018, 44, 1354–1360. [Google Scholar] [CrossRef]
- Reisinger, K.W.; Derikx, J.P.; Van Vugt, J.L.; Von Meyenfeldt, M.F.; Hulsewé, K.W.; Damink, S.W.O.; Stoot, J.H.; Poeze, M.; Information, P.E.K.F.C. Sarcopenia is associated with an increased inflammatory response to surgery in colorectal cancer. Clin. Nutr. 2016, 35, 924–927. [Google Scholar] [CrossRef] [PubMed]
- Naito, T.; Okayama, T.; Aoyama, T.; Ohashi, T.; Masuda, Y.; Kimura, M.; Shiozaki, H.; Murakami, H.; Kenmotsu, H.; Taira, T.; et al. Skeletal muscle depletion during chemotherapy has a large impact on physical function in elderly Japanese patients with advanced non–small-cell lung cancer. BMC Cancer 2017, 17, 571. [Google Scholar] [CrossRef]
- Huang, D.-D.; Ji, Y.-B.; Zhou, D.-L.; Li, B.; Wang, S.-L.; Chen, X.-L.; Yu, Z.; Zhuang, C.-L. Effect of surgery-induced acute muscle wasting on postoperative outcomes and quality of life. J. Surg. Res. 2017, 218, 58–66. [Google Scholar] [CrossRef]
- Neefjes, E.C.; Hurk, R.M.V.D.; Blauwhoff-Buskermolen, S.; Van Der Vorst, M.J.; Becker-Commissaris, A.; De Van Der Schueren, M.A.; Buffart, L.M.; Verheul, H.M.; Vorst, M.J.; Schueren, M.A. Muscle mass as a target to reduce fatigue in patients with advanced cancer. J. Cachexia Sarcopenia Muscle 2017, 8, 623–629. [Google Scholar] [CrossRef]
- Citak, E.; Tulek, Z.; Uzel, O. Nutritional status in patients with head and neck cancer undergoing radiotherapy: A longitudinal study. Support. Care Cancer 2019, 27, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Aihie Sayer, A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Calvani, R.; Tosato, M.; Martone, A.M.; Bernabei, R.; Onder, G.; Marzetti, E. Impact of physical function impairment and multimorbidity on mortality among community-living older persons with sarcopaenia: Results from the ilSIRENTE prospective cohort study. BMJ Open 2016, 6, e008281. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Kim, K.I.; Paik, N.J.; Kim, K.W.; Jang, H.C.; Lim, J.Y. Muscle strength: A better index of low physical performance than muscle mass in older adults. Geriatr. Gerontol. Int. 2016, 16, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Zaslavsky, O.; Li, W.; Going, S.; Datta, M.; Snetselaar, L.; Zelber-Sagi, S. Association between body composition and hip fractures in older women with physical frailty. Geriatr. Gerontol. Int. 2017, 17, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Verlaan, S.; Aspray, T.J.; Bauer, J.M.; Cederholm, T.; Hemsworth, J.; Hill, T.R.; McPhee, J.S.; Piasecki, M.; Seal, C.; Sieber, C.C.; et al. Nutritional status, body composition, and quality of life in community-dwelling sarcopenic and non-sarcopenic older adults: A case-control study. Clin. Nutr. 2017, 36, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Chiles Shaffer, N.; Ferrucci, L.; Shardell, M.; Simonsick, E.M.; Studenski, S. Agreement and predictive validity using less-conservative foundation for the national institutes of health sarcopenia project weakness cutpoints. J. Am. Geriatr. Soc. 2017, 65, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Resnick, B.; Hebel, J.R.; Gruber-Baldini, A.L.; Hicks, G.E.; Hochberg, M.C.; Orwig, D.; Eastlack, M.; Magaziner, J. The impact of body composition, pain and resilience on physical activity, physical function and physical performance at 2 months post hip fracture. Arch. Gerontol. Geriatr. 2018, 76, 34–40. [Google Scholar] [CrossRef]
- Yalcin, A.; Aras, S.; Atmis, V.; Cengiz, O.K.; Cinar, E.; Atli, T.; Varli, M. Sarcopenia and mortality in older people living in a nursing home in Turkey. Geriatr. Gerontol. Int. 2017, 17, 1118–1124. [Google Scholar] [CrossRef]
- Carrión, S.; Roca, M.; Costa, A.; Arreola, V.; Ortega, O.; Palomera, E.; Serra-Prat, M.; Cabré, M.; Clavé, P. Nutritional status of older patients with oropharyngeal dysphagia in a chronic versus an acute clinical situation. Clin. Nutr. 2017, 36, 1110–1116. [Google Scholar] [CrossRef]
- Coats, A.J.S. Clinical utility of exercise training in chronic systolic heart failure. Nat. Rev. Cardiol. 2011, 8, 380–392. [Google Scholar] [CrossRef] [PubMed]
- Maltais, F.; Decramer, M.; Casaburi, R.; Barreiro, E.; Burelle, Y.; Debigare, R.; Dekhuijzen, P.N.R.; Franssen, F.; Gayan-Ramirez, G.; Gea, J.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Update on Limb Muscle Dysfunction in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2014, 189, e15–e62. [Google Scholar] [CrossRef] [PubMed]
- Fong, D.Y.T.; Ho, J.W.C.; Hui, B.P.H.; Lee, A.M.; Macfarlane, D.J.; Leung, S.S.K.; Cerin, E.; Chan, W.Y.Y.; Leung, I.P.F.; Lam, S.H.S.; et al. Physical activity for cancer survivors: Meta-analysis of randomised controlled trials. BMJ 2012, 344, e70. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [PubMed]
- Gullett, N.P.; Hebbar, G.; Ziegler, T.R. Update on clinical trials of growth factors and anabolic steroids in cachexia and wasting1234. Am. J. Clin. Nutr. 2010, 91, 1143S–1147S. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Bravata, D.M.; Olkin, I.; Nayak, S.; Roberts, B.; Garber, A.M.; Hoffman, A.R. Systematic Review: The Safety and Efficacy of Growth Hormone in the Healthy Elderly. Ann. Internal Med. 2007, 146, 104. [Google Scholar] [CrossRef]
- Calder, P.C.; Laviano, A.; Lonnqvist, F.; Muscaritoli, M.; Ohlander, M.; Schols, A. Targeted medical nutrition for cachexia in chronic obstructive pulmonary disease: A randomized, controlled trial. J. Cachexia Sarcopenia Muscle 2018, 9, 28–40. [Google Scholar] [CrossRef]
- Van De Bool, C.; Rutten, E.P.; Van Helvoort, A.; Franssen, F.M.; Wouters, E.F.; Schols, A.M.; Bool, C.; Helvoort, A. A randomized clinical trial investigating the efficacy of targeted nutrition as adjunct to exercise training in COPD. J. Cachexia Sarcopenia Muscle 2017, 8, 748–758. [Google Scholar] [CrossRef]
- Schutz, Y.; Kyle, U.U.G.; Pichard, C. Fat-free mass index and fat mass index percentiles in Caucasians aged 18–98 y. Int. J. Obes. 2002, 26, 953–960. [Google Scholar] [CrossRef]
- Dos Santos, M.R.; Sayegh, A.L.; Bacurau, A.V.; Arap, M.A.; Brum, P.C.; Pereira, R.M.; Takayama, L.; Barretto, A.C.P.; Negrão, C.E.; de Nazaré NunesAlves, M.L. Effect of exercise training and testosterone replacement on skeletal muscle wasting in patients with heart failure with testosterone deficiency. Mayo Clin. Proc. 2016, 91, 575–586. [Google Scholar] [CrossRef]
- Ritch, C.R.; Cookson, M.S.; Clark, P.E.; Chang, S.S.; Fakhoury, K.; Ralls, V.; Thu, M.H.; Penson, D.F.; Smith, J.A.; Silver, H.J. Perioperative Oral Nutrition Supplementation Reduces Prevalence of Sarcopenia following Radical Cystectomy: Results of a Prospective Randomized Controlled Trial. J. Urol. 2019, 201, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Burden, S.T.; Gibson, D.J.D.J.; Lal, S.; Hill, J.; Pilling, M.; Soop, M.; Ramesh, A.; Todd, C.; Burden, S.T.S.T. Pre-operative oral nutritional supplementation with dietary advice versus dietary advice alone in weight-losing patients with colorectal cancer: Single-blind randomized controlled trial. J. Cachexia Sarcopenia Muscle 2017, 8, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Galvao, D.A.; Taaffe, D.R.; Spry, N.; Cormie, P.; Joseph, D.; Chambers, S.K.; Chee, P.; Peddle-Mcintyre, C.J.; Hart, N.H.; Baumann, F.T.; et al. Exercise preserves physical function in prostate cancer patients with bone metastases. Med. Sci. Sports Exerc. 2018, 50, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Taaffe, D.R.; Buffart, L.M.; Newton, R.U.; Spry, N.; Denham, J.; Joseph, D.; Lamb, D.; Chambers, S.K.; Galvão, D.A. Time on androgen deprivation therapy and adaptations to exercise: Secondary analysis from a 12-month randomized controlled trial in men with prostate cancer. BJU Int. 2018, 121, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.C.; Segal, R.J.; McKenzie, D.C.; Vallerand, J.R.; Morielli, A.R.; Mackey, J.R.; Gelmon, K.; Friedenreich, C.M.; Reid, R.D.; Courneya, K.S. Impact of resistance and aerobic exercise on sarcopenia and dynapenia in breast cancer patients receiving adjuvant chemotherapy: A multicenter randomized controlled trial. Breast Cancer Res. Treat. 2016, 158, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Cramer, J.T.; Cruz-Jentoft, A.J.; Landi, F.; Hickson, M.; Zamboni, M.; Pereira, S.L.; Hustead, D.S.; Mustad, V.A. Impacts of High-Protein Oral Nutritional Supplements Among Malnourished Men and Women with Sarcopenia: A Multicenter, Randomized, Double-Blinded, Controlled Trial. J. Am. Med. Dir. Assoc. 2016, 17, 1044–1055. [Google Scholar] [CrossRef] [PubMed]
- Malafarina, V.; Uriz-Otano, F.; Malafarina, C.; Martinez, J.A.; Zulet, M.A. Effectiveness of nutritional supplementation on sarcopenia and recovery in hip fracture patients. A multi-centre randomized trial. Maturitas 2017, 101, 42–50. [Google Scholar] [CrossRef]
- Englund, D.A.; Kirn, D.R.; Koochek, A.; Zhu, H.; Travison, T.G.; Reid, K.F.; Von Berens, Å.; Melin, M.; Cederholm, T.; Gustafsson, T.; et al. Nutritional Supplementation with Physical Activity Improves Muscle Composition in Mobility-Limited Older Adults, The VIVE2 Study: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Gerontol. Ser. A 2017, 73, 95–101. [Google Scholar] [CrossRef]
- Fielding, R.A.; Travison, T.G.; Kirn, D.R.; Koochek, A.; Reid, K.F.; Von Berens, Å.; Zhu, H.; Folta, S.C.; Sacheck, J.M.; Nelson, M.E.; et al. Effect of structured physical activity and nutritional supplementation on physical function in mobility-limited older adults: Results from the VIVE2 randomized trial. J. Nutr. Health Aging 2017, 21, 936–942. [Google Scholar] [CrossRef]
- Van Oostrom, S.H.; Gijsen, R.; Stirbu, I.; Korevaar, J.C.; Schellevis, F.G.; Picavet, H.S.J.; Hoeymans, N. Time trends in prevalence of chronic diseases and multimorbidity not only due to aging: Data from general practices and health surveys. PLoS ONE 2016, 11, e0160264. [Google Scholar] [CrossRef]
- Health AgingBody Composition Study; Delmonico, M.J.; Harris, T.B.; Visser, M.; Park, S.W.; Conroy, M.B.; Velasquez-Mieyer, P.; Boudreau, R.; Manini, T.M.; Nevitt, M.; et al. Longitudinal study of muscle strength, quality, and adipose tissue infiltration. Am. J. Clin. Nutr. 2009, 90, 1579–1585. [Google Scholar] [CrossRef] [PubMed]
- Kiyama, T.; Mizutani, T.; Okuda, T.; Fujita, I.; Tokunaga, A.; Tajiri, T.; Barbul, A. Postoperative Changes in Body Composition after Gastrectomy. J. Gastrointest. Surg. 2005, 9, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Mourtzakis, M.; Prado, C.M.; Lieffers, J.R.; Reiman, T.; McCargar, L.J.; Baracos, V.E. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl. Physiol. Nutr. Metab. 2008, 33, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Raman, M.; Mourtzakis, M.; Merli, M.; Tandon, P. A practical approach to nutritional screening and assessment in cirrhosis. Hepatology 2017, 65, 1044–1057. [Google Scholar] [CrossRef]
- Hopkins, M.; Finlayson, G.; Duarte, C.; Whybrow, S.; Ritz, P.; Horgan, G.W.; Blundell, J.E.; Stubbs, R.J. Modelling the associations between fat-free mass, resting metabolic rate and energy intake in the context of total energy balance. Int. J. Obes. 2016, 40, 312–318. [Google Scholar] [CrossRef]
- Cunningham, J.J. Body composition as a determinant of energy expenditure: A synthetic review and a proposed general prediction equation. Am. J. Clin. Nutr. 1991, 54, 963–969. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MAMC | BIA | DXA | CT | |
|---|---|---|---|---|
| Accuracy | - | + | ++ | +++ |
| Interobserver variability | +++ | + | - | - |
| Simplicity | ++ | ++ | + | - |
| Radiation | - | - | + | +++ |
| Cost | ||||
| If device already available | - | - | - 1 | + 2 |
| If device not available | - | + | ++ | +++ |
| Time to measurement | 5 min | 5 min | 5–10 min 3 | 10–15 min 3 |
| Studies | Population | Intervention Group | Comparison Group | Muscle Mass | Significant Results | |
|---|---|---|---|---|---|---|
| Nutrition | Ritch et al. 2019 [91] | Urothelial bladder carcinoma undergoing radical cystectomy INT = 31/CO = 30 | Daily oral nutritional supplement with ω-3 and HMB(700 kcal, 26 g proteins) 4 weeks before and after surgery | Oral micronutrients 2×/day | CT | 30 days post-operatively: - ↓ patients with SMI loss - No impact on hospital length of stay, postoperative complications, readmissions and mortality |
| Burden et al. 2017 [92] | Colorectal cancer INT = 55/CO = 46 | Daily oral nutritional supplement (600 kcal, 24 g proteins) ≥5 days before surgery+ dietary advice | Dietary advice | BIA | 5–7 days post-operatively: - No impact on FFMI and postoperative complications - ↓ % weight loss and surgical site infection | |
| Physical exercise | Galvao et al. 2018 [93] | Metastatic prostate cancer INT = 28/CO = 29 | Supervised endurance, resistance and flexibility exercises 3 months, 3×/week, 60 min | Usual physical activity | DXA | After 3-month intervention: - No impact on lean soft tissue - ↑ self reporting physical functioning and leg strength |
| Taaffe et al. 2018 [94] | Prostate cancer with previous androgen deprivation therapy and radiotherapy INT = 50/CO = 50 | Supervised endurance and resistance exercises 6 months, 2×/week, 60 min followed by home-based endurance, resistance and flexibility exercises 6 months, 2×/week, 60 min | Recommendation for 150 min/week of moderate intensity physical exercise for 12 months based on educational material | DXA | After 6-month intervention: - ↑ ASMM, chair rise time, leg and arm strength - No impact on for lean soft tissue After 12-month intervention: - No impact on ASMM, leg strength and lean soft tissue - ↑ chair rise time and arm strength | |
| Wall et al. 2017 [32] | Prostate cancer undergoing androgen deprivation therapy INT = 60/CO = 47 | Supervised endurance and resistance exercises 6 months, 2×/week, 60 min + home-based endurance exercise 6 months, 150 min/week | Usual physical activity | DXA | After 6-month intervention: - ↑ lean soft tissue, V02max, fat oxidation - No impact on resting metabolic rate, carbohydrate oxidation and body weight | |
| Adams et al.2016 [95] | Breast cancer undergoing adjuvant chemotherapy INT endurance = 66 INT resistance = 64 CO = 70 | During chemotherapy: INT endurance 3×/week, 105 min INT resistance 3×/week | Usual physical activity | DXA | At the end of chemotherapy: INT resistance VS CO: - ↑ lean soft tissue index, leg and arm strengthINT endurance VS CO: - No impact on lean soft tissue, leg and arm strength INT resistance VS INT endurance:- No impact on lean soft tissue - ↑ leg and arm strength |
| Studies | Population | Intervention Group | Comparison Group | Muscle Mass | Significant Results | |
|---|---|---|---|---|---|---|
| Nutrition | Cramer et al. 2016 [96] | Malnutrition and sarcopenia in the community INT = 165/CO = 165 | Daily oral nutritional supplement with HMB (660 kcal, 40 g proteins) + Usual diet during 24 weeks | Daily oral nutritional supplement (660 kcal, 28 g proteins) + Usual diet | DXA | After 24-week intervention, in both groups: - No impact on lean soft tissue - ↑ FM, handgrip strength, gait speed, muscle quality and isokenetic peak torque leg strength - No outcome difference between groups |
| Malafarina et al. 2017 [97] | Traumatic hip fracture in rehabilitation hospital INT = 55/CO = 52 | Daily oral nutritional supplement with HMB (660 kcal, 40 g proteins) + Standard diet 1500 kcal, 87.4 g protein during rehabilitation stay | Standard diet 1500 kcal, 87.4 g protein | BIA | At the end of the rehabilitation: - ↓ FFM, ASMM and BMI decrease - No impact on handgrip strength, gait speed | |
| Nutrition and physical exercise | Englund et al. 2017 [98] Fielding et al. 2017 [99] | Mobility-limitation and vitamin D insufficiency in the community INT = 74/CO = 75 | Daily oral nutritional supplement (150 kcal, 20 g whey protein, 800UI vit D) + Supervised endurance, resistance, balance and flexibility exercises 3×/week, 60 min during 6 months | Daily placebo (30 kcal) + Supervised endurance, resistance, balance and flexibility exercises 3×/week, 60 min during 6 months | DXA | After 6-month intervention, in both groups: - No impact on ASMM - ↑ muscle strength, thigh muscle composition, gait speed, short physical performance battery score - ↓ FM - ↑ lean soft tissue only for control group - ↑ 25(OH)D only for intervention group - No outcome difference between groups |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mareschal, J.; Achamrah, N.; Norman, K.; Genton, L. Clinical Value of Muscle Mass Assessment in Clinical Conditions Associated with Malnutrition. J. Clin. Med. 2019, 8, 1040. https://doi.org/10.3390/jcm8071040
Mareschal J, Achamrah N, Norman K, Genton L. Clinical Value of Muscle Mass Assessment in Clinical Conditions Associated with Malnutrition. Journal of Clinical Medicine. 2019; 8(7):1040. https://doi.org/10.3390/jcm8071040
Chicago/Turabian StyleMareschal, Julie, Najate Achamrah, Kristina Norman, and Laurence Genton. 2019. "Clinical Value of Muscle Mass Assessment in Clinical Conditions Associated with Malnutrition" Journal of Clinical Medicine 8, no. 7: 1040. https://doi.org/10.3390/jcm8071040
APA StyleMareschal, J., Achamrah, N., Norman, K., & Genton, L. (2019). Clinical Value of Muscle Mass Assessment in Clinical Conditions Associated with Malnutrition. Journal of Clinical Medicine, 8(7), 1040. https://doi.org/10.3390/jcm8071040