Economic Challenges in Nutritional Management

 ,
,
Abstract
:1. Introduction
- There will be costs for the detection of DRM and consequently for nutritional treatment,
- Treatment of DRM will lead to improvements in clinical outcomes that transfer to savings in the costs of basic treatment, and
- Patients may be attributed to DRGs with increased cost-weights, causing additional revenues for the hospital.
2. Materials and Methods
3. Input Data
3.1. Target Population
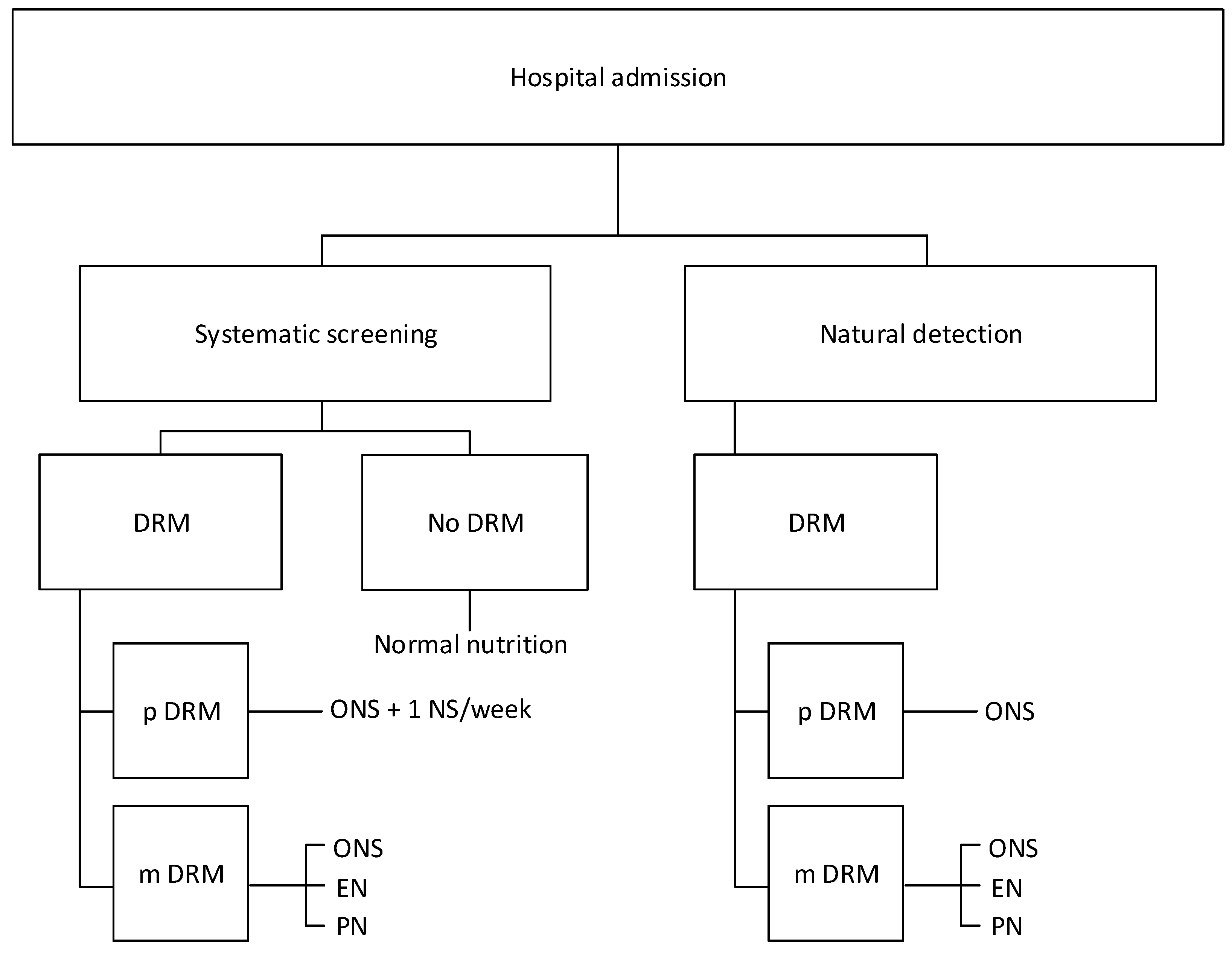
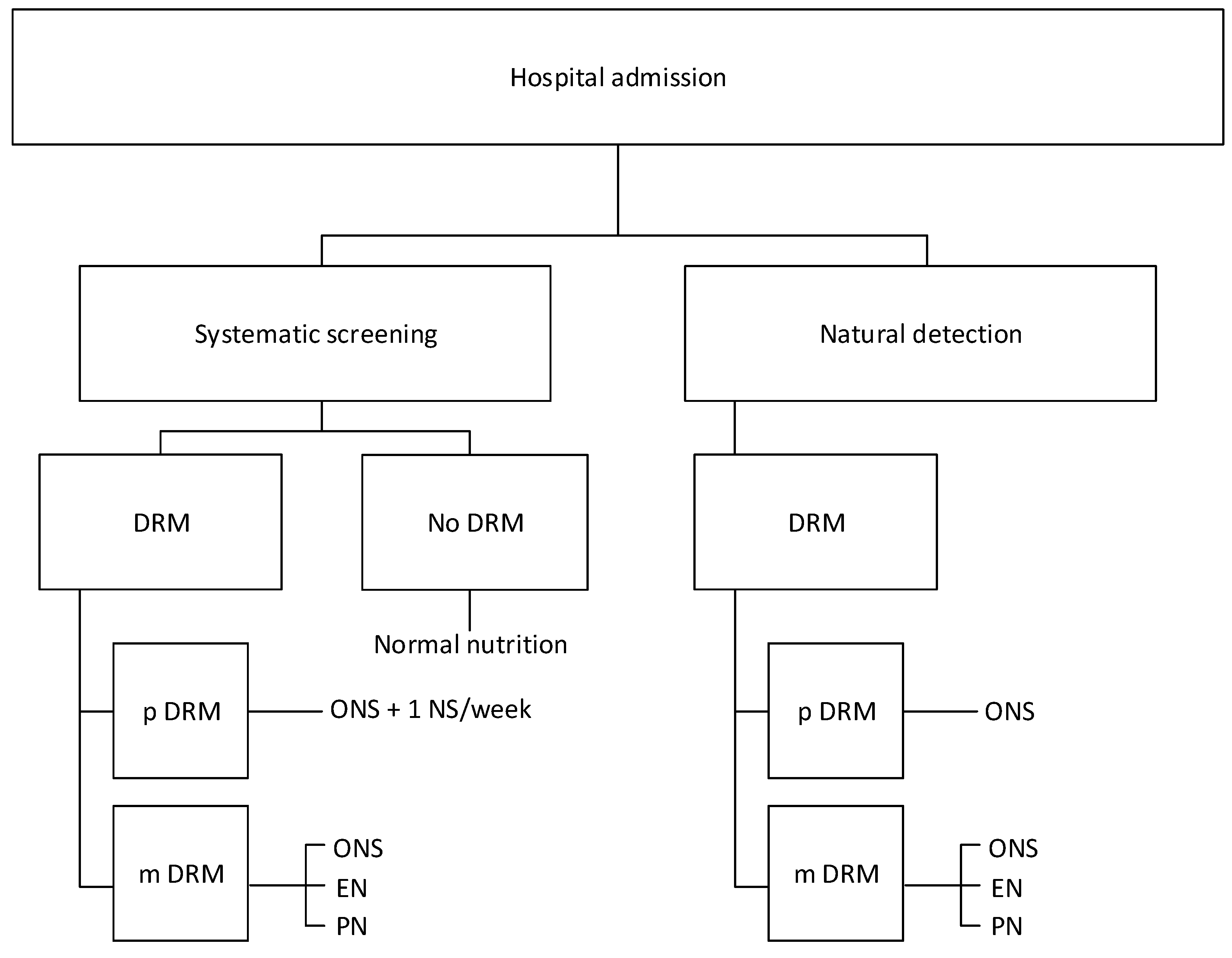
3.2. Detection Rate
3.3. Proportions with Potential and Manifest DRM
3.4. Number of Screenings
3.5. Types and Proportions of NI
3.6. Reduction of LOS
3.7. DRG Changes
3.8. Increase in Cost-Weight
3.9. Ethics
4. Cost and Savings
4.1. Cost of NS
4.2. Costs per Patient with NI
4.3. Savings per Prevented Inpatient Day
4.4. Additional Revenue due to SwissDRG Change
5. Results
5.1. Effect of a Systematic NS
5.2. Effects of ND, Treatment and Coding of DRM
5.3. Costs, Savings, and Additional Revenue Attributable to NS
5.4. Staff Needed
5.5. Scenario Analyses
6. Discussion
7. Cost Effectiveness of Nutritional Therapy in the Post-Hospital or Community Setting: A Brief Statement
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| Patients Flow and Performance | Proportion/Rate | Number |
|---|---|---|
| Target population | 20,000 | |
| Proportion/Rate | n | |
| Detection rate, of which: | 6.4% | 1280 |
| proportion p DRM | 0.25 | 320 |
| proportion m DRM | 0.75 | 960 |
| Nutritional interventions | ||
| Proportion | n | |
| ONS | 59% | 755 |
| EN | 29% | 371 |
| PN | 12% | 154 |
| Saved hospital days | Per Patient | total |
| Reduction in LOS, days | 1.2 | 1152 |
| SwissDRG changes | Detected Cases | |
| Proportion | n | |
| Changes in DRG attribution | 0.0833 | 107 |
| Number | Value | Costs | |
|---|---|---|---|
| Costs nutritional Interventions | |||
| ONS | 755 | 187.57 | 141,652 |
| EN | 371 | 842.96 | 312,906 |
| PN | 154 | 1557.84 | 239,284 |
| Total costs | 1280 | 693,842 | |
| Savings (reduction LOS) (−) | 1152 | 1373.46 | −1582,224 |
| Additional revenue (SwissDRG) (−) | 107 | 7564.70 | −806,579 |
| Net effect | −1,694,961 |
| Nutritional Therapy | Nursing | Physician | |
|---|---|---|---|
| Systematic nutritional screening | |||
| Hours total | 6052 | 13,700 | 1210 |
| Days total | 721 | 1631 | 144 |
| Positions needed | 4.09 | 9.27 | 0.82 |
| Natural Detection | |||
| Hours total | 1989 | 5327 | 398 |
| Days total | 237 | 634 | 47 |
| Positions needed | 1.35 | 3.60 | 0.27 |
| Additional needs for systematic nutritional screening | |||
| Hours total | 4063 | 8373 | 813 |
| Days total | 484 | 997 | 97 |
| Positions needed | 2.75 | 5.66 | 0.55 |
| Dietician | Nursing Staff | Physician | ||
|---|---|---|---|---|
| ONS | ||||
| Duration of therapy, days | 8.4 | |||
| Minutes/patient/day | 10 | 10 | 2 | |
| Minutes/patient | 84 | 84 | 16.8 | |
| N patients NS | 2797 | |||
| Minutes for NS | 234,976 | 234,976 | 46,995 | |
| N patients ND | 755 | |||
| Minutes for ND | 63,437 | 63,437 | 12,687 | |
| EN | ||||
| Duration of therapy, days | 10.3 | |||
| Minutes/patient/day | 10 | 40 | 2 | |
| Minutes/patient | 103 | 412 | 20.6 | |
| N patients NS | 851 | |||
| Minutes for NS | 87,619 | 350,475 | 17,524 | |
| N patients ND | 371 | |||
| Minutes for ND | 38,234 | 152,934 | 7647 | |
| PN | ||||
| Duration of therapy, days | 9.6 | |||
| Minutes/patient/day | 12 | 70 | 2.4 | |
| Minutes/patient | 115.2 | 672 | 23.04 | |
| N patients NS | 352 | |||
| Minutes for NS | 40,550 | 236,544 | 8110 | |
| N patients ND | 154 | |||
| Minutes for ND | 17,695 | 103,219 | 3539 |
| Nutritional Support After Hospital Discharge | ||||
|---|---|---|---|---|
| Author | Population | Type of Study | Cost Analysis | Results |
| Edington et al., 2004 [29] United Kingdom | mixed malnourished ≥ 65 y, (n = 100) | RCT intervention ONS for 8 weeks, 24 weeks follow-up | Cost-effectiveness analysis, direct and indirect costs | No difference regarding quality of life, post-hospital health care resource use or cost |
| Norman et al., 2011 [25] Germany | gastrointestinal disease, malnourished (n = 114) | RCT intervention Dietary counseling at discharge and high-protein ONS for months vs. dietary counseling at discharge | Cost-effectiveness analysis, direct costs of nutritional support | Intervention patients: increase in quality of life after 3 months ICER: EUR9497–12099/QALY |
| Neelemaat et al., 2012 [26] The Nederlands | mixed, malnourished ≥ 60 y (n = 210) | RCT: ONS, dietary counseling, vitamin D for 3 months after hospital discharge vs. usual care | Cost-effectiveness analysis, direct and indirect costs | No significant difference in QALYs at 3 months follow-up, intervention group: improvement in functional limitations, EUR618/functional limitation improvement (0.95 probability the intervention is cost effective) |
| Zhong et al., 2016 [27] United States of America | Mixed, malnourished ≥ 65 y (n = 622) | RCT: high-protein ONS, enriched b-hydroxy-b-methylbutyrate for 3 months after hospital discharge compared to placebo | Cost-effectiveness analysis, direct and indirect costs | Intervention group: increase in quality of life ICER: USD 33,818/QALY lifetime ICER: USD 524/LY |
| Nutritional support in the community or nursing home setting | ||||
| Author | Population | Type of study | Cost analysis | Results |
| Arnaud-Battandier et al., 2004 [30] France | Malnourished ≥ 70 y community or nursing home residents (n = 287) | prospective, cohort study of patients from 2 groups of physicians (high vs. low ONS prescription rate), 12-month follow-up | Comparison of direct costs | Higher costs of ONS in intervention group (EUR M, but lower costs of medical care: hospital admissions (EUR1631 vs. EUR 2203) and medical visits (EUR 299 vs. EUR 462) |
| Lorefält et al., 2011 [31] Sweden | nursing home residents, ≥ 65 y (n = 109) | Prospective cohort study of nutrition education and care (individualized meals) for 3 months | Comparison of direct costs | Higher costs in intervention group (EUR 830 vs. EUR 760 for nutritional support, EUR 652 vs. EUR 402 for education program) |
| Freijer et al., 2013 [32] The Nederlands | malnourished ≥ 65 y; community or nursing home residents (n = 720,223) | Health economic evaluation of published studies | Budget impact analysis | Annual cost savings of EUR 11.62 million due to intervention with ONS |
| Schilp et al., 2014 [28] The Nederlands | malnourished ≥ 65 y; community-dwelling old (n = 146) | RCT, dietary counseling vs. usual care | Cost-effectiveness analysis | No differences regarding gain in weight, QALY or costs |
| Simmons et al., 2015 [33] United States of America | Malnourished/at risk ≥ 65 y, nursing home residents (n = 154) | 3-arm RCT: ONS vs. in-between snacks vs. usual care for 6 months | Cost-effectiveness analysis | No change in body weight, intervention costs per person per day; ONS group 2.54 and snack group 3.85; ICER: 103 kcal/USD in ONS group vs. 79 kcal/USD in snack group |
| van der Pols-Vijlbrief et al., 2017 [34] The Nederlands | community-dwelling older adults receiving home care with or at risk of malnutrition ≥65 y (n = 155) | RCT, multifactorial personalized intervention for 6 months | Cost-effectiveness analysis | No differences regarding gain in weight, functional status, QALY or costs |
| Elia et al., 2018 [35] United Kingdom | Malnourished, nursing home residents ≥65 y (n = 104) | RCT, comparing ONS versus dietary advice for 3 months | Cost effectiveness analysis with direct and indirect costs | Intervention group improved quality of life: ICER: GBP 10,961/QALY |
References
- Aeberhard, C.; Abt, M.; Endrich, O.; Aubry, E.; Leuenberger, M.S.; Schütz, P.; Sterchi, A.B.; Stanga, Z. Auswirkung, der Kodierung der Mangelernährung im SwissDRGSystem. Aktuell. Ernährungsmed. 2018, 43, 92–100. [Google Scholar]
- Aeberhard, C.; Birrenbach, T.; Joray, M.; Muhlebach, S.; Perrig, M.; Stanga, Z. Simple training tool is insufficient for appropriate diagnosis and treatment of malnutrition: A pre-post intervention study in a tertiary center. Nutrition 2016, 32, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Elia, M. The Cost of Malnutrition in England and Potential Cost Savings from Nutritional Interventions (short version). BAPEN. 2015. Available online: www.bapen.org.uk/pdfs/economic-report-short.pdf (accessed on 8 July 2019).
- Imoberdorf, R.; Meier, R.; Krebs, P.; Hangartner, P.J.; Hess, B.; Staubli, M.; Wegmann, D.; Rühlin, M.; Ballmer, P.E. Prevalence of undernutrition on admission to Swiss hospitals. Clin. Nutr. 2010, 29, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Sriram, K.; Sulo, S.; VanDerBosch, G.; Partridge, J.; Feldstein, J.; Hegazi, R.A.; Summerfelt, W.T. A Comprehensive Nutrition-Focused Quality Improvement Program Reduces 30-Day Readmissions and Length of Stay in Hospitalized Patients. JPEN J. Parenter. Enteral Nutr. 2017, 41, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Bally, M.R.; Blaser Yildirim, P.Z.; Bounoure, L.; Gloy, V.L.; Mueller, B.; Briel, M.; Schuetz, P. Nutritional Support and Outcomes in Malnourished Medical Inpatients: A Systematic Review and Meta-analysis. JAMA Int. Med. 2016, 176, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Elia, M.; Normand, C.; Laviano, A.; Norman, K. A systematic review of the cost and cost effectiveness of using standard oral nutritional supplements in community and care home settings. Clin. Nutr. 2016, 35, 125–137. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE). Nutritional support for adults: oral nutrition support, enteral tube feeding and parenteral nutrition. Clinical Guideline 32, published February 2006m last modified August 2017. Available online: https://www.nice.org.uk/Guidance/CG32 (accessed on 8 July 2019).
- Stratton, R.J.; Green, C.J.; Elia, M. Disease-Related Malnutrition: An Evidence-Based Approach to Treatment; CABI: Wallingford, UK, 2003; pp. 1128–1129. [Google Scholar]
- Stratton, R.J.; Hebuterne, X.; Elia, M. A systematic review and meta-analysis of the impact of oral nutritional supplements on hospital readmissions. Ageing Res. Rev. 2013, 12, 884–897. [Google Scholar] [CrossRef]
- Schuetz, P.; Fehr, R.; Baechli, V.; Geiser, M.; Deiss, M.; Gomes, F.; Bilz, S.; Sigrist, S.; Brändle, M.; Benz, C.; et al. Individualised nutritional support in medical inpatients at nutritional risk: A randomised clinical trial. Lancet 2019, 393, 8–14. [Google Scholar] [CrossRef]
- Deutz, N.E.; Matheson, E.M.; Matarese, L.E.; Luo, M.; Baggs, G.E.; Nelson, J.L.; Hegazi, R.A.; Tappenden, K.A.; Ziegler, T.R. NOURISH Study Group. Readmission and mortality in malnourished, older, hospitalized adults treated with a specialized oral nutritional supplement: A randomized clinical trial. Clin. Nutr. 2016, 35, 18–26. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Krznaric, Z.; Singer, P.; Barazzoni, R.; Cederholm, T.; Golay, A.; Van Gossum, A.; Kennedy, N.; Kreymann, G.; Laviano, A.; et al. Effectiveness and efficacy of nutritional therapy: A systematic review following Cochrane methodology. Clin. Nutr. 2017, 36, 939–957. [Google Scholar] [CrossRef]
- Voltz, C.; Seegler, S.; Keil, J.-P.; Fleßa, S. Malnutrition in Hospital Care – Potential Revenues of Nutrition. Aktuelle Ernährungsmedizin. 2016, 41, 187–189. [Google Scholar]
- Vonzun, N.; Sterchi, A.-B.; Imoberdorf, R.; Rühlin, M. Malnutrition and DRG—The Swiss Solution. Aktuell. Ernährungsmed. 2014, 39, 392–396. [Google Scholar]
- Ockenga, J.; Freudenreich, M.; Zakonsky, R.; Norman, K.; Pirlich, M.; Lochs, H. Nutritional assessment and management in hospitalised patients: Implication for DRG-based reimbursement and health care quality. Clin. Nutr. 2005, 24, 913–919. [Google Scholar] [CrossRef]
- Reinbold, T.; Broß, I.; Lenfers, B. Malnutrition in the G-DRG-System—Effects of a Structured Nutritional Management on Codification and Revenues. Aktuell. Ernährungsmed. 2013, 38, 24–29. [Google Scholar]
- Kondrup, J.; Rasmussen, H.H.; Hamberg, O.; Stanga, Z. Nutritional risk screening (NRS 2002): A new method based on an analysis of controlled clinical trials. Clin. Nutr. 2003, 22, 321–336. [Google Scholar] [CrossRef]
- Wenger, C.; Hischier, T.; Rhyner, A.; Iff, S.; Sterchi, A.-B.; Stanga, Z. Introduction of Malnutrition Management on two Specialized University Clinics. Aktuell. Ernährungsmed. 2008, 33, 296–301. [Google Scholar] [CrossRef]
- Kruizenga, H.M.; Van Tulder, M.W.; Seidell, J.C.; Thijs, A.; Ader, H.J.; Van Bokhorst-de van der Schueren, M.A. Effectiveness and cost-effectiveness of early screening and treatment of malnourished patients. Am. J. Clin. Nutr. 2005, 82, 1082–1089. [Google Scholar] [CrossRef]
- Holyday, M.; Daniells, S.; Bare, M.; Caplan, G.A.; Petocz, P.; Bolin, T. Malnutrition screening and early nutrition intervention in hospitalised patients in acute aged care: A randomised controlled trial. J. Nutr. Health Aging 2012, 16, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Somanchi, M.; Tao, X.; Mullin, G.E. The facilitated early enteral and dietary management effectiveness trial in hospitalized patients with malnutrition. JPEN J. Parenter. Enteral Nutr. 2011, 35, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Elia, M.; Russell, C. Combating Malnutrition: Recommendations for Action; Nutrition Advisory Group on Malnutrition Led by BAPEN 2009; BAPEN: Redditch, UK, 2009. [Google Scholar]
- Abizanda, P.; Sinclair, A.; Barcons, N.; Lizan, L.; Rodriguez-Manas, L. Costs of Malnutrition in Institutionalized and Community-Dwelling Older Adults: A Systematic Review. J. Am. Med. Dir. Assoc. 2016, 17, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Pirlich, M.; Smoliner, C.; Kilbert, A.; Schulzke, J.D.; Ockenga, J.; Lochs, H.; Reinhold, T. Cost-effectiveness of a 3-month intervention with oral nutritional supplements in disease-related malnutrition: A randomised controlled pilot study. Eur. J. Clin. Nutr. 2011, 65, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Neelemaat, F.; Bosmans, J.E.; Thijs, A.; Seidell, J.C.; van Bokhorst-de van der Schueren, M.A. Oral nutritional support in malnourished elderly decreases functional limitations with no extra costs. Clin. Nutr. 2012, 31, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Cohen, J.T.; Goates, S.; Luo, M.; Nelson, J.; Neumann, P.J. The Cost-Effectiveness of Oral Nutrition Supplementation for Malnourished Older Hospital Patients. Appl. Health Econ. Health Policy. 2017, 15, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Schilp, J.; Bosmans, J.E.; Kruizenga, H.M.; Wijnhoven, H.A.H.; Visser, M. Is dietetic treatment for undernutrition in older individuals in primary care cost-effective? J. Am. Med. Dir. Assoc. 2014, 15, 226.e7–226.e13. [Google Scholar] [CrossRef] [PubMed]
- Edington, J.; Barnes, R.; Bryan, F.; Dupree, E.; Frost, G.; Hickson, M.; Lancaster, J.; Mongia, S.; Smith, J.; Torrance, A.; et al. A prospective randomised controlled trial of nutritional supplementation in malnourished elderly in the community: Clinical and health economic outcomes. Clin. Nutr. 2004, 23, 195–204. [Google Scholar] [CrossRef]
- Arnaud-Battandier, F.; Malvy, D.; Jeandel, C.; Schmitt, C.; Aussage, P.; Beaufrere, B.; Cynober, L. Use of oral supplements in malnourished elderly patients living in the community: A pharmaco-economic study. Clin. Nutr. 2004, 23, 1096–1103. [Google Scholar] [CrossRef] [PubMed]
- Lorefalt, B.; Andersson, A.; Wirehn, A.B.; Wilhelmsson, S. Nutritional status and health care costs for the elderly living in municipal residential homes--an intervention study. J. Nutr. Health Aging 2011, 15, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Freijer, K.; Nuijten, M.J.; Schols, J.M. The budget impact of oral nutritional supplements for disease related malnutrition in elderly in the community setting. Front. Pharmacol. 2012, 3, F78. [Google Scholar] [CrossRef] [PubMed]
- Simmons, S.F.; Keeler, E.; An, R.; Liu, X.; Shotwell, M.S.; Kuertz, B.; Silver, H.J.; Schnelle, J.F. Cost-Effectiveness of Nutrition Intervention in Long-Term Care. J. Am. Geriatr. Soc. 2015, 63, 2308–2316. [Google Scholar] [CrossRef] [PubMed]
- van der Pols-Vijlbrief, R.; Wijnhoven, H.A.H.; Bosmans, J.E.; Twisk, J.W.R.; Visser, M. Targeting the underlying causes of undernutrition. Cost-effectiveness of a multifactorial personalized intervention in community-dwelling older adults: A randomized controlled trial. Clin. Nutr. 2017, 36, 1498–1508. [Google Scholar] [CrossRef] [PubMed]
- Elia, M.; Parsons, E.L.; Cawood, A.L.; Smith, T.R.; Stratton, R.J. Cost-effectiveness of oral nutritional supplements in older malnourished care home residents. Clin. Nutr. 2018, 37, 651–658. [Google Scholar] [CrossRef] [PubMed]
| Item | Both | Natural Detection | Nutritional Screening |
|---|---|---|---|
| Target population | Variable | 20,000 | |
| Detection rate DRM | 6.4% | 20.0% | |
| Proportions p DRM:m DRM | 25% vs. 75% | 45% vs. 55% | |
| Number of nutritional screenings | No DRM, m DRM: 1; p DRM: 2 | ||
| Nutritional interventions | |||
| p DRM: ONS | 100% | 25% | 45% |
| m DRM: ONS | 45% | 34% | 25% |
| m DRM: EN | 39% | 29% | 21% |
| m DRM: PN | 16% | 12% | 9% |
| Reduction LOS in mDRM, days | 1.2 | ||
| SwissDRG attribution change | 8.3% | 15.0% | |
| Average increase cw | 0.694 | 0.44 |
| ONS | EN | PN | |
|---|---|---|---|
| Per day | |||
| Personnel costs, CHF | 17.36 | 40.91 | 66.37 |
| Materials costs, CHF | 4.97 | 40.09 | 75.02 |
| Personnel and materials costs, CHF | 22.33 | 81.00 | 141.39 |
| Per therapy | |||
| Duration of therapy, days | 8.4 | 10.3 | 9.6 |
| Personnel and material costs, CHF | 187.57 | 834.35 | 1357.36 |
| One-time costs, CHF | 8.61 | 200.48 | |
| Total therapy costs, CHF | 187.57 | 842.96 | 1557.84 |
| Patients Flow and Performance | Proportion/Rate | Number |
|---|---|---|
| Target population | 20,000 | |
| Detection rate, of which: | 20% | 4000 |
| - proportion p DRM | 0.45 | 1800 |
| - proportion m DRM | 0.55 | 2200 |
| Number of systematic nutritional screenings | ||
| - On hospital admission | 1 | 20,000 |
| - Weekly in cases with p DRM | 1 | 1800 |
| Total screenings | 21,800 | |
| Nutritional interventions | ||
| p DRM | ||
| - ONS | 45.0% | 1800 |
| m DRM | ||
| - ONS | 24.9% | 997 |
| - EN | 21.3% | 851 |
| - PN | 8.8% | 352 |
| Total nutritional interventions | 100.0% | 4000 |
| Saved hospital days | Per Patient | Total |
| expected LOS | 12 | |
| reduction % | 10% | |
| Reduction LOS, days | 1.2 | 2640 |
| Swiss DRG changes | Detected Cases | |
| Changes in DRG attribution | 0.15 | 600 |
| Number | Value | Costs | |
|---|---|---|---|
| Costs | |||
| Systematic nutritional screening | 21,800 | 3.93 | 85,583 |
| Nutritional interventions | |||
| ONS | 2797 | 187.57 | 524,694 |
| EN | 851 | 842.96 | 717,076 |
| PN | 352 | 1557.84 | 548,358 |
| Total nutritional interventions | 4000 | 1,790,128 | |
| Total costs | 1,875,711 | ||
| Savings (LOS reduction) (−) | 2640 | 1373.46 | −3,625,930 |
| Additional revenue (SwissDRG) (−) | 600 | 4796.00 | −2,877,600 |
| Net effect | −4,627,818 | ||
| Nutritional | Natural | Extra Costs/ | |
|---|---|---|---|
| Screening | Detection | Savings NS | |
| Costs | |||
| Systematic screening | 85,583 | 85,583 | |
| Nutritional interventions | 1,790,128 | 693,842 | 1,096,286 |
| Total costs | 1,875,711 | 693,842 | 1,181,869 |
| Savings (reduction LOS) (−) | −3,625,930 | −1,582,224 | −2,043,706 |
| Additional revenue (SwissDRG) (−) | −2,877,600 | −806,579 | −2,071,021 |
| Net effect | −4,627,818 | −1,694,961 | −2,932,858 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reber, E.; Norman, K.; Endrich, O.; Schuetz, P.; Frei, A.; Stanga, Z. Economic Challenges in Nutritional Management. J. Clin. Med. 2019, 8, 1005. https://doi.org/10.3390/jcm8071005
Reber E, Norman K, Endrich O, Schuetz P, Frei A, Stanga Z. Economic Challenges in Nutritional Management. Journal of Clinical Medicine. 2019; 8(7):1005. https://doi.org/10.3390/jcm8071005
Chicago/Turabian StyleReber, Emilie, Kristina Norman, Olga Endrich, Philipp Schuetz, Andreas Frei, and Zeno Stanga. 2019. "Economic Challenges in Nutritional Management" Journal of Clinical Medicine 8, no. 7: 1005. https://doi.org/10.3390/jcm8071005
APA StyleReber, E., Norman, K., Endrich, O., Schuetz, P., Frei, A., & Stanga, Z. (2019). Economic Challenges in Nutritional Management. Journal of Clinical Medicine, 8(7), 1005. https://doi.org/10.3390/jcm8071005