1. Introduction
Pain is an unpleasant experience with complex interactions between sensorimotoric, affective, and cognitive brain networks. As such, pain, especially chronic pain, is influenced by and interacts with physical, psychological, social, and contextual factors [
1,
2,
3]. One-fifth of the European population has moderate to severe chronic pain conditions [
4]. These conditions are associated with psychological distress, low health, sick leave, and high socioeconomic costs [
5]. Therefore, a biopsychosocial (BPS) framework should be considered in clinical practice [
6,
7,
8].
Unlike single/unimodal interventions, interdisciplinary multimodal pain rehabilitation programs (IMMRPs) for chronic pain—an interdisciplinary treatment according to the International Association for the Study of Pain (IASP)—distinguish themselves as well-coordinated complex interventions. Typically, IMMRPs are based on cognitive behavioural therapy (CBT) models (including Acceptance Commitment Therapy, ACT) and are administered over several weeks to months [
9,
10,
11,
12]. The Swedish programs generally include group activities such as pain education, supervised physical activity, training in simulated environments, and CBT coordinated by an interdisciplinary team (e.g., physician, occupational therapist, physiotherapist, psychologist, and social worker) based on a BPS framework [
9,
10,
11,
12]. The components of IMMRP are most often chosen based on the available evidence for unimodal interventions for chronic pain, for example, with respect to education, exercise, psychological interventions, and interventions for return to work. The core goals of rehabilitation programs in general [
13] and especially for patients with chronic pain [
14] are broad and multifactorial in combination with the individualised goals of the patient. These include increased ability to participate in valued activities such as work. Hence, IMMRP is a complex intervention [
13,
15] and, unlike pharmacological intervention, focusses on the whole person rather than just biochemical processes, implying complex patient conditions matched with complex IMMRPs [
16,
17]. The components of IMMRP can be active independently or interdependently [
15], resulting in a combination of effects explained by known and unknown mechanisms. The effects are assumed to be greater than the sum of its components [
18].
Systematic reviews (SRs) have generally reported higher efficacy both on a general level and for specific outcomes of IMMRP compared with single-treatment or treatment-as-usual programs [
10,
12,
19,
20,
21,
22,
23]. SRs and Randomised Controlled Trials (RCTs) may be associated with risk for bias resulting from, for example, an unrepresentative selection of patients and researcher allegiance [
24,
25,
26]. Thus, it is necessary to investigate whether the evidence obtained from SRs and RCTs can be replicated within a consecutive non-selected flow of patients in practice settings using prospective observational cohort study designs such as practice-based evidence (PBE). PBE has also been applied in the field of rehabilitation research [
27]. The importance of such an approach is also emphasised in the real-effectiveness medicine framework [
28]. IMMRPs are time consuming and expensive, even when most of the activities are group-based. From an ethical, individual, and socioeconomic perspective, it is indeed remarkable to note the lack of studies investigating effect sizes (ES) in patient populations in real-life practice settings. A recent study from two Swedish university clinics reported effect sizes of 0.51–0.61 (i.e., moderate ES) for two pain intensity variables at 12-month follow-up [
29]. These effect sizes should be confirmed in larger studies based not only on patients at university hospitals, but also on specialist units in general. It would be motivating for patients to endure increases in pain, which is often observed in clinical practise during the start-up period of rehabilitation characterised by an increase in activity levels, if it were known that the long-term effects include the reduction of pain levels.
Complex interventions such as IMMRP should have several outcomes measured at multiple levels and strategies for handling multiple outcomes [
17,
30]. IMMRPs are evaluated using many outcomes. For example, one SR including 46 RCTs reported nine outcomes per RCT (median) [
10]. However, outcomes are not usually divided into primary and secondary outcomes [
10]. In addition, although it is most likely that changes in several of the selected outcomes are correlated, most SRs of IMMRPs evaluate the outcomes as independent from each other. Patterns of potential correlations (i.e., multivariate correlation patterns) are mainly unknown/uninvestigated, even though they could give valuable information regarding how to optimise IMMRPs. Hence, there is a need to develop clinically applicable ways to evaluate the multiple outcomes of MMPRs both for individual patients and within research studies.
The above knowledge gaps motivated this PBE study of chronic pain patients based on patient reported outcome measures (PROMs) from the Swedish Quality Registry for Pain Rehabilitation (SQRP) [
31]. This registry offers an opportunity to investigate clinical outcomes and patterns of change, since all the relevant specialist care units throughout Sweden deliver data to SQRP. Hence, this PBE study has the general aim of investigating the effects of IMMRP in specialist care in Sweden considering the multivariate complexity of outcomes. We hypothesised that IMMRP in special care is associated with small-to-medium ES, that changes in outcomes generally are intercorrelated, and that the baseline situation (pre-IMMRP) can predict the multivariate outcomes. More specifically, we defined the following four aims:
To investigate the outcome effect sizes of IMMRP immediately post-IMMRP and at 12-month follow-up.
To analyse the multivariate correlation patterns of changes in outcomes of IMMRP: pre-IMMRP versus post IMMRP and pre-IMMRP versus 12-month follow-up.
To define a multivariate outcome measure of IMMRP.
To investigate if the clinical self-reported presentation pre-IMMRP can predict the multivariate outcome measure.
4. Discussions
The major findings of the present large PROM study from SQRP are listed below:
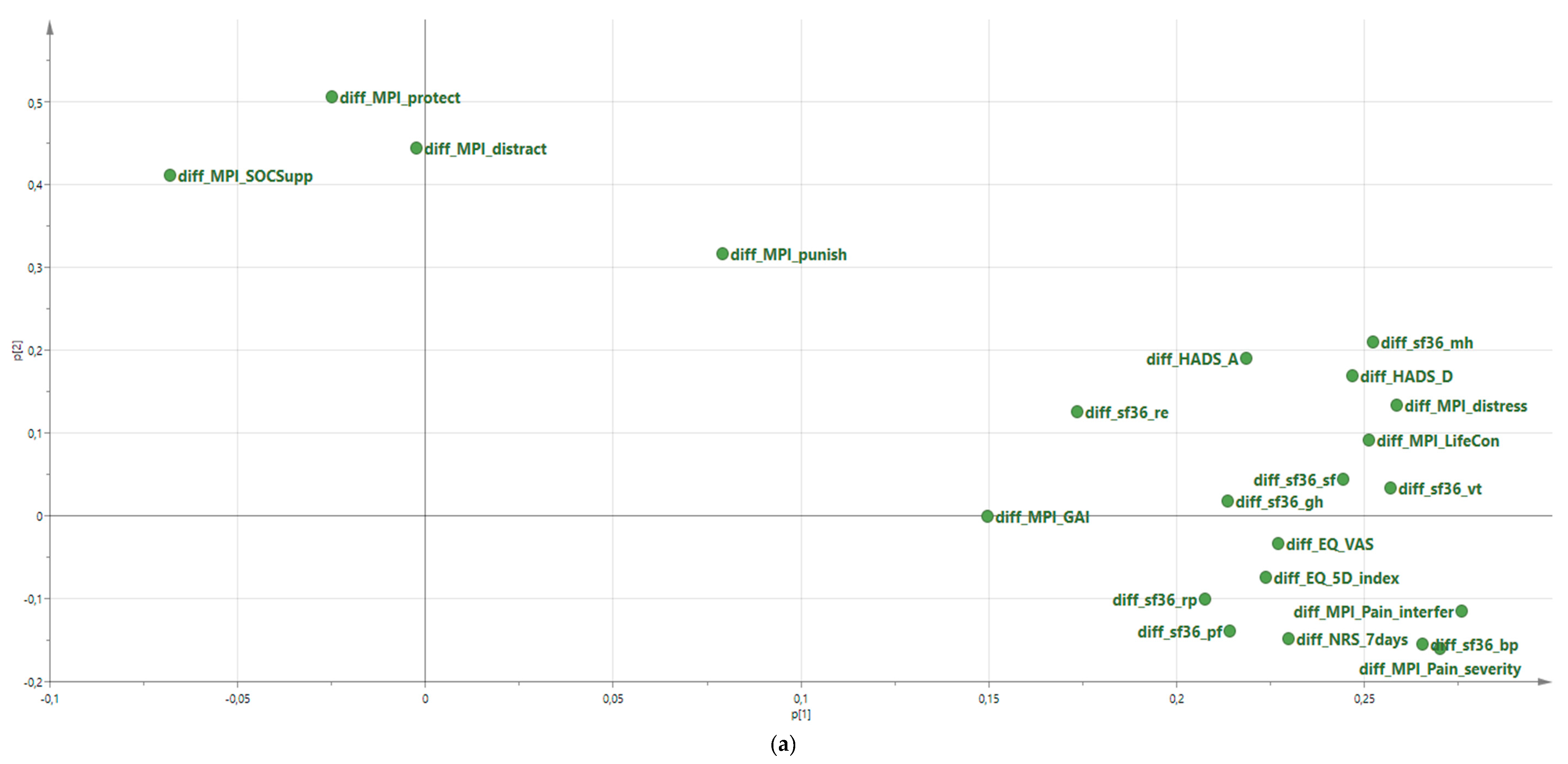
Moderate long-term ES were found for pain intensity (MPI Pain severity and SF-36 bodily pain), interference in daily life (MPI Interference), and state of health (EQ-5D-index); most other variables showed small ES. Vitality also displayed moderate effect sizes immediately after IMMRP but fell slightly under cut-off for moderate change at 12-month follow-up. The majority of the 22 investigated outcomes were significantly improved.
Significant intercorrelations between changes in pain intensity, interference, control, psychological distress, and mental health were confirmed. The changes in 22 outcomes reflected one (pre-IMMRP versus post-IMMRP) or three (pre-IMMRP versus 12-month follow-up) latent components (groups of variables).
The outcomes were best for patients with the worst self-reported clinical presentation pre-IMMRP. Based on a defined multivariate improvement score (MIS), three clusters were identified. Cluster 1—overall, the worst situation pre-IMMRP—showed positive multivariate improvements in outcomes. Cluster 3—deteriorated—showed negative scores. Cluster 2, the intermediate cluster, was associated with overall slightly positive multivariate improvements.
Certain variables (especially psychological distress and life impact variables, pain, and health and vitality aspects) pre-IMMRP were associated with improvements according to MIS both post-IMMRP and at 12-month FU. However statistically significant, the pre-IMMRP situation could only explain a small part of the variation in MIS (8%); therefore, for clinical use, it was not possible to predict those who would benefit most from IMMRP.
The outcome variables mandatory in SQRP and presented in the present study are in good agreement with the BSP model of chronic pain and the outcome domains presented by the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) [
7,
52] and the Validation and Application of a patient-relevant core set of outcome domains to assess multimodal PAIN therapy (VAPAIN) [
14] initiatives.
The present study was not primarily designed to evaluate the efficacy of IMMRP, which requires RCTs and SRs/meta-analyses. However, our results for the repeated measurements (
Table 2 and
Table 3) of chronic pain patients in real-life practice settings are in agreement with the positive evidence for IMMRPs reported in SRs [
10,
11,
12] and in other studies [
22,
23,
53]. As such, the small to moderate ES are noteworthy as these patients, who receive pain rehabilitation in specialist care centres, often have tried other treatments for their chronic pain with no or little effect. That is, these patients have severe problems and relative treatment resistance. Interestingly, the changes in outcomes with moderate ES are broad and not limited to a single outcome domain, and the most stable moderate ES were demonstrated for pain intensity aspects with moderate improvement both immediately after IMMRPs and at 12-month follow-up. Pain interference demonstrated moderate ES improvement at 12-month follow-up, and vitality was moderately improved immediately after IMMRPs. Both objective registrations (e.g., sick-leave registrations and actigraphic recordings [
54]) and subjective PROM data may be important for understanding the efficacy of IMMRPs. Very recently, a SQRP study using a subgroup of the same cohort of patients reported that sick leave benefits according to the Swedish Social Insurance Agency decreased as a consequence of IMMRP [
55]. Hence, both PROM data and objective sick leave data indicate clinically important positive changes in response to IMMRPs for patients in real-life practice settings. As a comparison, SRs conclude that common pharmacological treatments—e.g., paracetamol, non-steroidal anti-inflammatory drugs, and opioids—for patients with chronic pain have no effects, small effects, and/or lack of long-term follow-up effects [
56,
57,
58].
The present study reported medium ES for two of three pain intensity variables both post-IMMRP and at 12-month FU (i.e., for MPI-pain-severity and sf36-bp); the third pain intensity variable had effect sizes near medium ES. These results contrasted some SRs reporting of no evidence for efficacy with respect to pain intensity [
10,
11]. However, not all RCTs of IMMRP included pain intensity outcomes, since the interventions are not focused on the pain itself but rather on its consequences [
10,
11]. Obviously, many pain patients consider pain intensity improvement to be the most important aspect of treatments [
59]. However, changing this perspective is considered important in IMMPRs, since focusing on pain reduction in many cases leads to short-sighted attempts to control pain, and this may, when not successful, lead to increased physical and psychological disability and reduced life quality [
60,
61]. Thus, specialist care IMMRPs in Sweden have largely adopted the idea of introducing acceptance as a cornerstone of the psychological component of IMMRP (i.e., the willingness to have the experiences of pain as it is and to encourage patients to set up activity-related rehabilitation goals and risk initial pain flare-ups). This also means that patients are advised against establishing pain reduction goals. Thus, it could be considered problematic to communicate the present results showing medium effect sizes in real-world practice settings on pain. On the other hand, it may also be ethically problematic if both clinical practice and research ignore the reports and wishes of the patients regarding pain intensity. However, health care providers should not underestimate their patients’ ability to grasp, once explained, the complex pain experience. Therefore, health care providers should emphasise pain education, including descriptions of the affective and cognitive elements of pain as rational for the different components of IMMRPs, and stress the need to experiment with new behaviours and risk short-term pain flare-ups. Since the results are obtained in this context, no change in clinical practise as far as pain communication is called for.
SRs of IMMRP report that it is an effective intervention with small to moderate effects for patients with chronic pain conditions [
11,
12,
62,
63]. The present results concerning ES agree with most SRs of IMMRP, but it may also be appropriate to compare with ES results reported in other clinical studies. The moderate ES for two of the pain intensity variables agree with studies in clinical routine care (n = 65–395), and therefore, for long-term follow-up (6–12 months), such studies report small (Cohen’s d: 0.20–0.33 [
64,
65]) to moderate (Cohen’s d: 0.59–0.70 [
26,
66,
67]) ES for pain intensity. For psychological distress variables, these studies agree with the present results: they generally found small ES for long-term follow-up (i.e., Cohen’s d = 0–0.38 for depressive symptoms [
26,
64,
65] and Cohen’s d = 0.22–0.34 for anxiety) [
26,
65]. In a recent RCT comparing transdiagnostic emotion-focused exposure treatment (Hybrid) and Internet-delivered pain management treatment (ICBT) for chronic pain patients with comorbid anxiety and depression, we found that within group ES pre versus follow-up for pain interference were reported both for hybrid (ES = 1.17) and for ICBT (ES = 0.65) compared the present effect size of 0.49 [
68]. However, the patients were not exclusively recruited from specialist care (i.e., clinical departments of pain rehabilitation); they were also recruited via advertisements in local newspapers and social media [
68], and the numbers investigated were considerably smaller. An important observation from the present study is that moderate ES found at 12-month follow-up covered broad aspects (e.g., pain intensity, interference in daily life, and perceived health).
The number of outcomes in IMMRPs in RCTs are generally high, which reasonably reflects the broad goals of the complex intervention. The present study used 22 outcomes that are mandatory in SQRP measured on up to three occasions (i.e., pre-IMMRP, post-IMMRP, and 12-month follow-up). PCA was applied to handle the pattern of changes in potentially intercorrelated outcomes as suggested by the Medical Research Council of the United Kingdom [
69]. From these analyses, it can be concluded that changes in pain intensity, pain interference, psychological distress, vitality, etc. were positively intercorrelated (
Table 5). In fact, our study showed that the changes in the majority of the 22 outcomes are significantly intercorrelated. Hence, the changes in these variables cannot be considered independent of each other. As a consequence of this observation, the appropriateness to evaluate changes in outcomes separately, as done in a recent SR [
70], must be questioned, since the treatment was not designed to target only a single outcome. Moreover, the ES must be seen in this complex context. Thus, small changes in many outcomes may be more important than one prominent change in a single or few outcomes. Furthermore, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) used for evidence ratings in SRs may not adequately describe the evidence base of complex interventions [
71]. Different definitions of positive outcomes of IMMRP interventions exist (e.g., the majority of outcomes had to be significantly better than for the control intervention) [
10,
11]. Another approach was that the authors of the SR predetermined primary and secondary outcomes and what was necessary to classify an intervention as positive before reviewing the RCTs [
12].
The presented PCAs also highlight that it may be possible to reduce the number of outcome variables, since several of these appear to measure similar aspects of the chronic pain condition. The fact that 22 outcomes were analysed (
Table 2 and
Table 3) may raise an issue of multiple comparisons. In such situations, Bonferroni corrections are frequently used [
72,
73]. This is a conservative approach when the number of tests increases [
72,
74,
75], the chances to detect real treatment effects decrease, and corrections were designed for corrections of
independent comparisons [
74]. The latter is obviously not present for most changes in outcome variables according to the PCAs performed (
Table 5). Hierarchal or ‘gatekeeping’ procedures do not require adjustment for multiplicity [
73], but require a natural hierarchy of the outcomes, as such a hierarchy is not obvious for IMMRP, as discussed above. Another approach is that outcomes are combined into a single composite outcome (i.e., a composite outcome consists of two or more component outcomes) [
76], but this may be problematic with respect to missing cases and when the components of the composite endpoint are measured on different scales (i.e., non-commensurate outcomes) [
76]. However, some multivariate methods such as PCA and OPLS can handle non-commensurate outcomes [
76]. We used advanced PCA, including the NIPALS algorithm, to handling missing data and non-commensurate outcomes. We calculated the
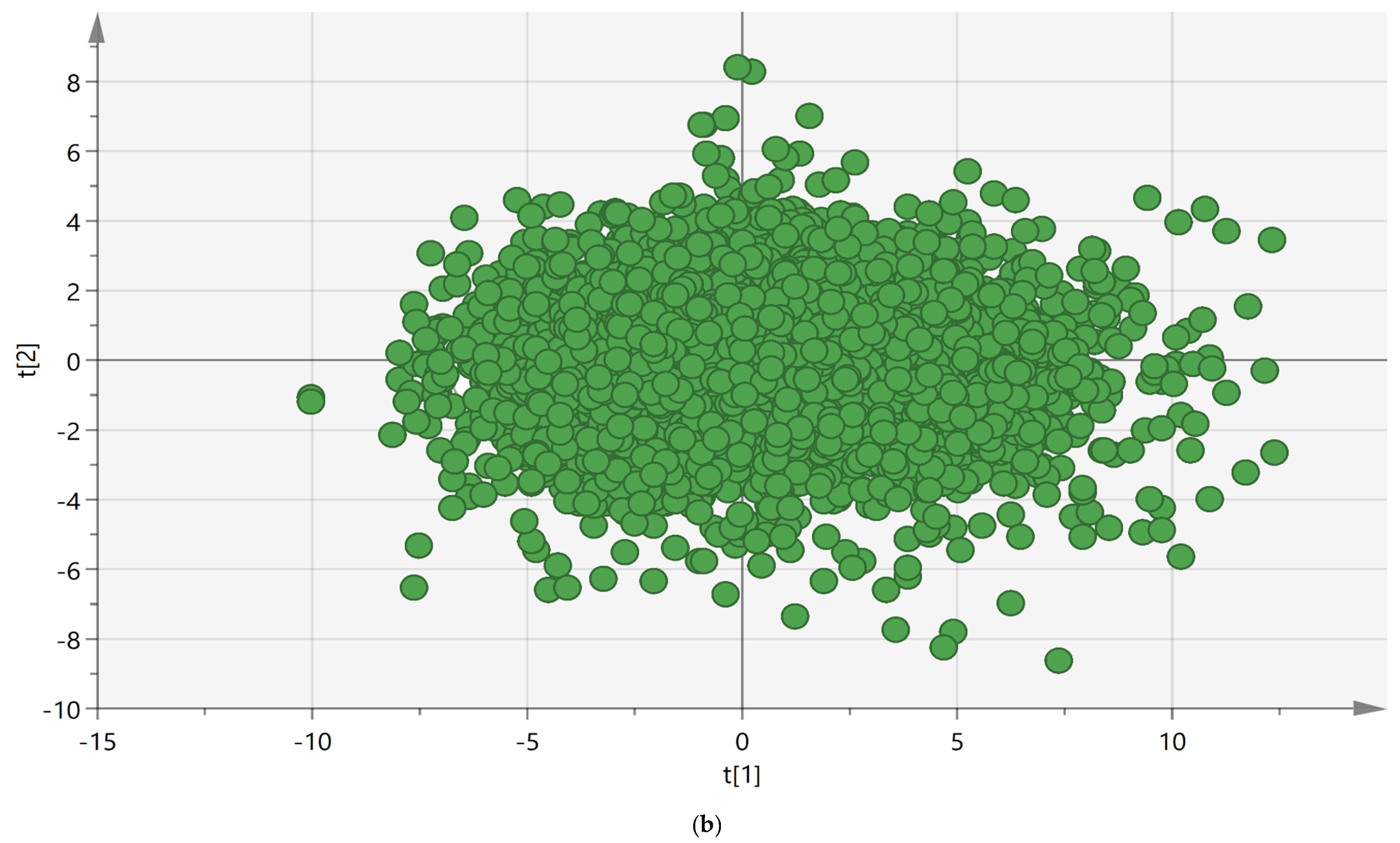
t-scores for the most relevant latent factor (component). Hence, we defined an objective Multivariate Improvement Score (MIS; the
t-score of the first PCA component), which on an individual patient level defines the multivariate improvement; a positive MIS indicates multivariate improvements because of IMMRP.
Three clearly separated clusters based on MIS were identified. On a group level, clusters 1 and 2 were associated with various degrees of improvements, whereas cluster 3 showed negative MIS, indicating deterioration. Although the greater improvement in cluster 1 can be interpreted as a sign of regression to the mean and that these patients did not benefit from IMMRP more than cluster 2, this cluster still improves from IMMRP at least as well as those with e.g., less severe psychological distress symptoms (clusters 2 and 3). This may seem unexpected, but it is important to recognise that addressing psychological symptoms with CBT is an important component of IMMRPs. The patients at post-IMMRP and 12-month follow-up estimated the degree of positive change in pain (i.e., Change-pain) and the ability to handle life situation in general (i.e., Change-life situation). Most patients reported improvements according to both the Change-pain and Change-life situations (
Table 4). Relatively small proportions of the patients reported worse situations post-IMMRP and at the 12-month follow-up, which are results that agree with other studies [
29,
77,
78]. These two variables have retrospective elements even though they are not explicitly expressed. There are several problems with such items in general—e.g., desirability and memory aspects, recall time [
79,
80,
81], and in treatment context (e.g., overly optimistic assessments) [
82]. However, on a general level, these estimations and the two MIS variables (
Table 6 and
Table 7) agreed.
We found that cluster 1, which had high MIS values (i.e., prominent improvements), had a more severe clinical picture at baseline/pre-IMMRP than those with lower MIS (i.e., less improvements). These results agree with another SQRP study (
N > 35,000) that identified clusters based on the clinical presentation at assessment (decision not taken about participation in IMMRP); the study found that patients with the most severe clinical situation who later participated in IMMRP had the most prominent improvements in six investigated outcomes [
34]. Although IMMRP has been commended for its effectiveness (‘of all approaches to the treatment of chronic pain, none has a stronger evidence basis for efficacy, cost-effectiveness, and lack of iatrogenic complications’) [
83], both this and our recent study [
34] indicate that not all patients show important improvements in several domains of outcome after IMMRP. Both this and our previous study identified a large subgroup of patients that do not seem to significantly benefit from IMMRP. Presumably, these patients—in the present study, those with negative MIS (i.e., cluster 3)—need other interventions. In a relative context, they have a somewhat less complicated self-reported clinical picture pre-IMMRP than those in clusters 1 and 2, even though they are referred to specialist care and hence represent patients with complex needs.
The longitudinal regressions of MIS using background variables and pre-IMMRP data as regressors were significant (
Table 10). A blend of variables was important; psychological distress variables were most important, but life impact variables, pain aspects, and health and vitality aspects contributed. Our results appear to be in line with a recent meta-analysis on prognostic factors for IMMRP outcome, demonstrating that both pre-treatment general emotional distress and pain-specific cognitive behavioural factors are related to worse long-term (>6 months) physical functioning [
84]. Unfortunately, these regressions cannot be used clinically, since they only explained 8% of variations in MIS. Although the prediction does not work clinically, this and a previous study from our group give clear indications that patients with a severe clinical situation benefit from IMMRP [
34].
4.1. Important Clinical Implications
Outcomes of IMMRP in real-life practice settings agree with the conclusions from SRs. Partly in contrast to SRs, this registry study of patients managed within specialist care found that pain intensity was positively affected because of IMMRP. It was also obvious that not all patients benefit from IMMRP. Hence, there is a need to develop better matching between clinical presentation and participation in MMRP in real-life practice settings. Moreover, the intercorrelations of most changes in outcomes also opens up the possibility of reducing the number of outcome variables and hereby reduce the burden upon patients included in the SQRP.
4.2. Strengths and Limitations
This study’s strengths include a large number of patients with complex chronic pain conditions with a nation-wide representation. However, these patients were referred to specialist clinics and thus represent a selection of the most difficult cases, so our results cannot be generalised to other settings. Another strength was the use of MVDA methods such as PCA and OPLS to handle correlation patterns, repeated measures, and regressions when there were obvious risks for multicollinearity. Changes in the social context may have changed and influenced the longitudinal analyses; however, we used validated and well-known instruments. Repeated evaluations using PROM questionnaires in treatment studies may be problematic [
85]. Thus, the changes that the patient undergo because of the intervention (i.e., IMMRP) may affect the interpretations of the questions when presented at follow-up. The fact that no control group or treatment-as-usual group was available, which ethically is complicated to arrange for a registry of real-life practice patients, might have influenced our interpretation of changes after IMMRP. Data for the time period 2008–2016 from the SQRP was used in the present study, and changes in the content of IMMRP may have occurred. Unfortunately, no data concerning such changes are available.






{kind=link}
{kind=link}