Systematic Review of the Long-Term Effects of Transgender Hormone Therapy on Bone Markers and Bone Mineral Density and Their Potential Effects in Implant Therapy




Abstract
1. Introduction
- First, to answer the following PICOT (Problem/Patient/Population, Intervention, Comparison, Outcome, Time) question: In adult transgender patients (transwoman and transmen), receiving long-term pharmacologic therapy, are the bone markers and bone mineral density affected differently?
- Second, to provide a theoretical basis for a better understanding of the implications of the long-term pharmacologic therapy in the adult transgender patient on therapies involving orthopedic or dental implants.
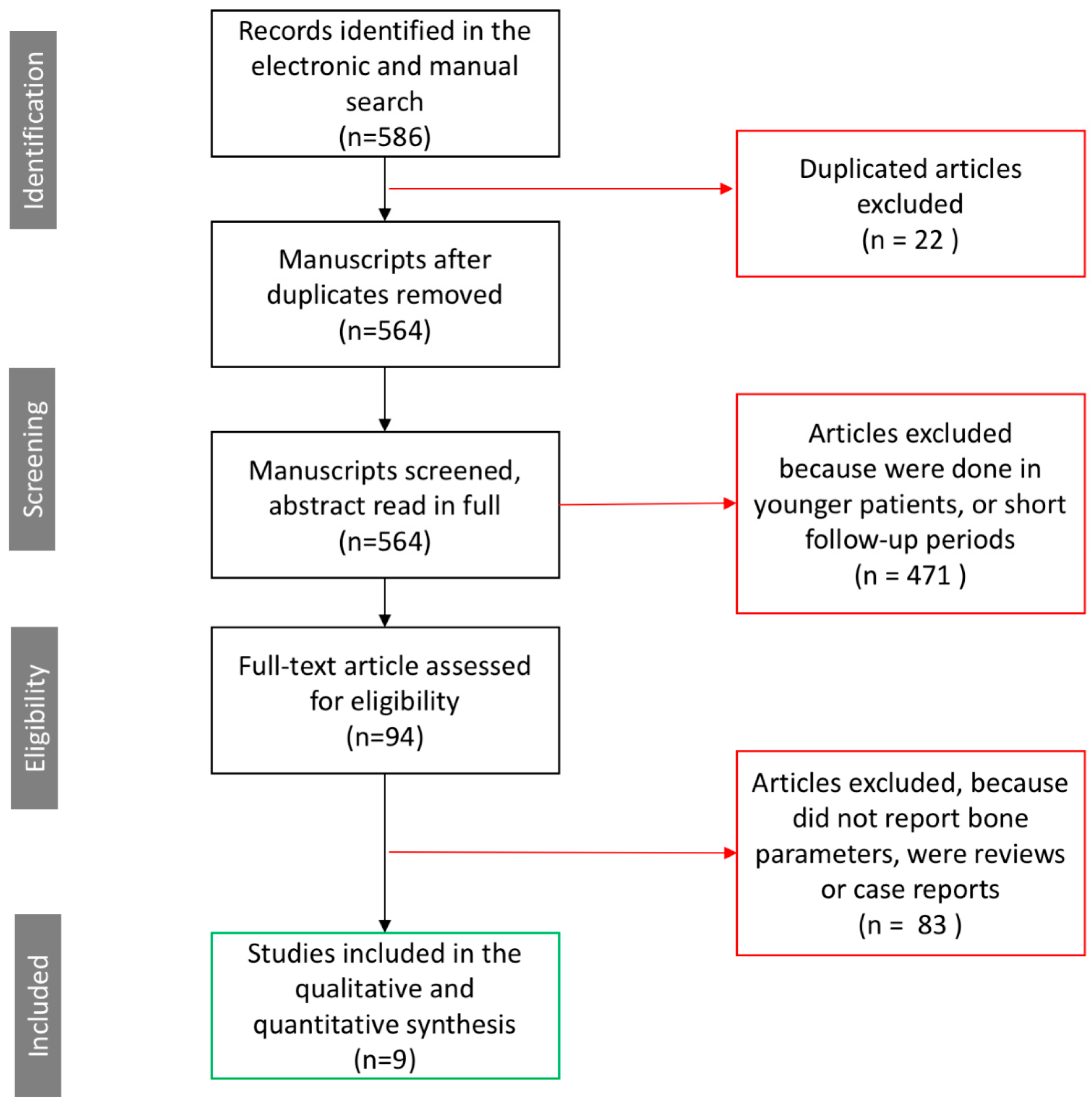
2. Materials and Methods
2.1. Study Inclusion Criteria
- Papers published in the English language from January 1990 through to December 2018;
- Publications reporting clinical studies with three or more years follow-up;
- Publications reporting the biological effects of cross-sex pharmacologic therapy in the bone markers, bone metabolism, and bone mineral density of transgender patients;
- Papers reporting the pharmacologic therapy used for transgender adults (including both retrospective and prospective studies).
2.2. Study Exclusion Criteria
- Articles published in languages other than English;
- Publications reporting less than three years of follow-up;
- Publications detailing the effects of cross-sex pharmacologic therapy in teenagers or young transgender patients;
- Publications reporting effects of cross-sex pharmacologic therapy not including the effects on bone
- Animal studies and in-vitro studies;
- Other systematic reviews and meta-analyses;
- Duplicated studies;
- Case reports.
2.3. Data Extraction
- Transgender demographics: Number of males to female (transwomen) or female to male (transmen) patients included in each study;
- The duration of hormone-therapy treatment expressed in years or months;
- Type of hormone received by the patient and dosage.
2.3.1. Primary Outcomes
- Changes in bone metabolism marker levels calcium (mmol/L), phosphate (mmol/L), alkaline phosphatase (U/L), and osteocalcin (µg/L). Changes were measured at baseline and after treatment or at different time points for each of the bone metabolism markers.
- Changes in the BTMs including Serum Procollagen type I N-Terminal pro-peptide (PINP) (ng/mL) for evaluation of the bone formation, and Serum Collagen type I cross-linked C-telopeptide (CTX) (ng/mL) for evaluation of bone resorption. Changes were recorded at baseline and at different time points.
- Changes in the BMD. BMD values were registered at baseline and after the completion of treatment or at baseline and at different time points.
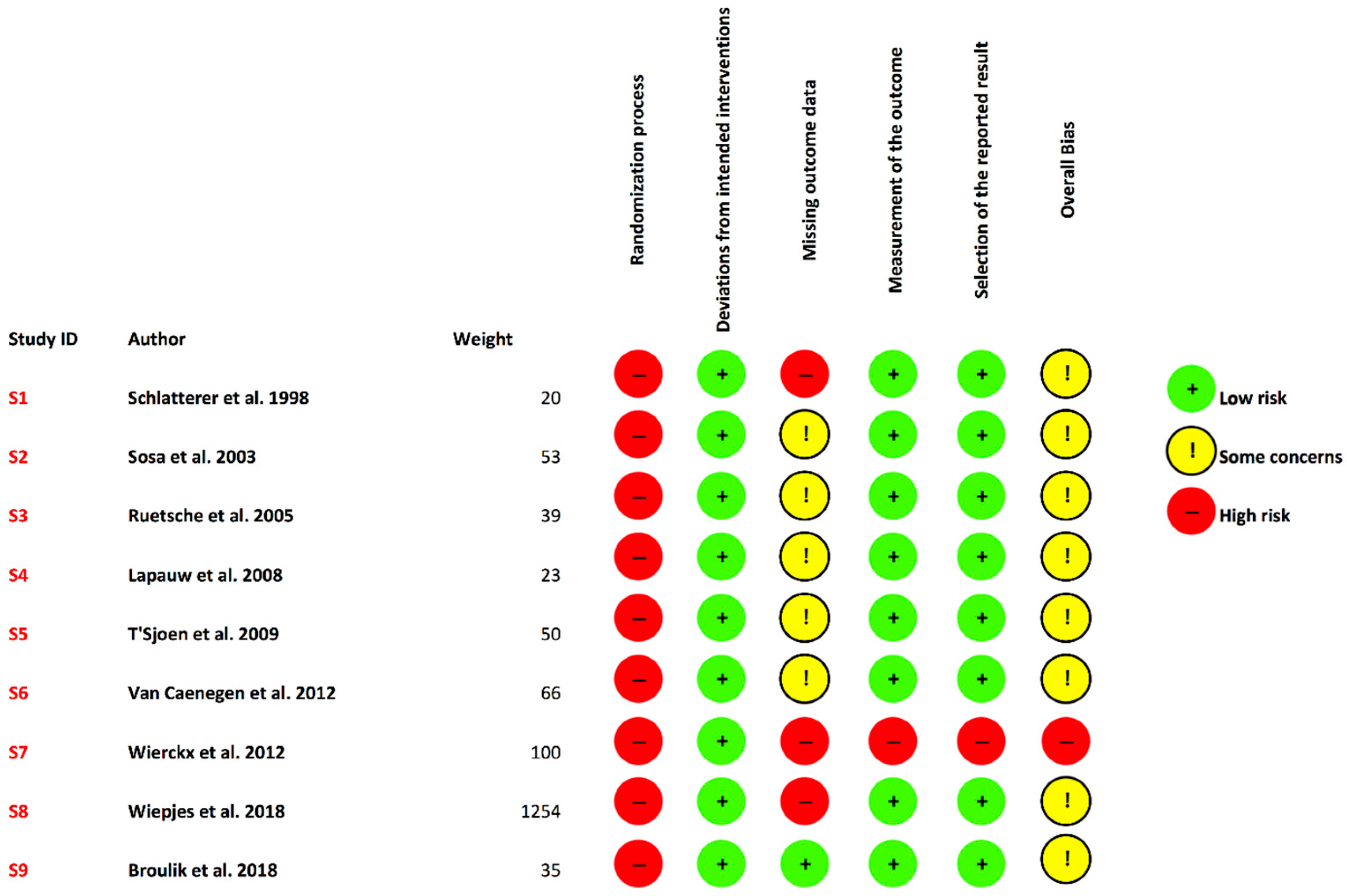
2.3.2. Risk of Bias
2.4. Statistical Analysis
3. Results
3.1. Transgender Demographics and Time under Treatment
3.2. Type of Hormone Received and Dosage
- Cyproterone + estrogens (high doses) [37].
- Ethinyl estradiol + cyproterone acetate and oral estrogens and estradiol valerate [38].
- Cyproterone acetate 2 mg/day + ethinyl estradiol 35–100 µg/day, after sex reassignment surgery estradiol valerate or 17-beta estradiol 2–4 mg/day [39].
- Cyproterone acetate 50–100 mg/day + ethinyl estradiol 25–50 μg/day, after surgery ethinyl estradiol 25–50 μg/day or estradiol valerate 2 mg/day or conjugated equine estrogens 1.25 mg/day.
- or transdermal estradiol [40].
- Cyproterone acetate 50–100 mg/day/1 year + exogenous estrogen, after surgery all received estrogens [41].
- Estrogens and anti-androgens until gonadectomy [42].
- Testosterone esters 250 mg/IM every 3 weeks, before and after surgery [38].
- Testosterone decanoate 100 mg, or testosterone isocaproate/fenylpropionate 60 mg, or testosterone propionate 30 mg/mL 2–3 weeks, or testosterone undecanoate 1000 mg 12 weeks, or transdermal testosterone 50 mg daily, or testosterone undecanoate 40 mg/day + testosterone gel 50 mg per 5 g, 50 mg daily [41].
- Testosterone [42].
- Different testosterone compounds [43].
- Testosterone isobutyrate, and after surgery, testosterone isobutyrate 25 mg intramuscular every week, or testosterone propionate 250 mg every 3 weeks intramuscular, or testosterone undecanoate 40 mg/4 times/day [45].
3.3. Bone Metabolism Marker Levels Before and After the Treatment
3.4. The Two Main Bone Turnover Markers
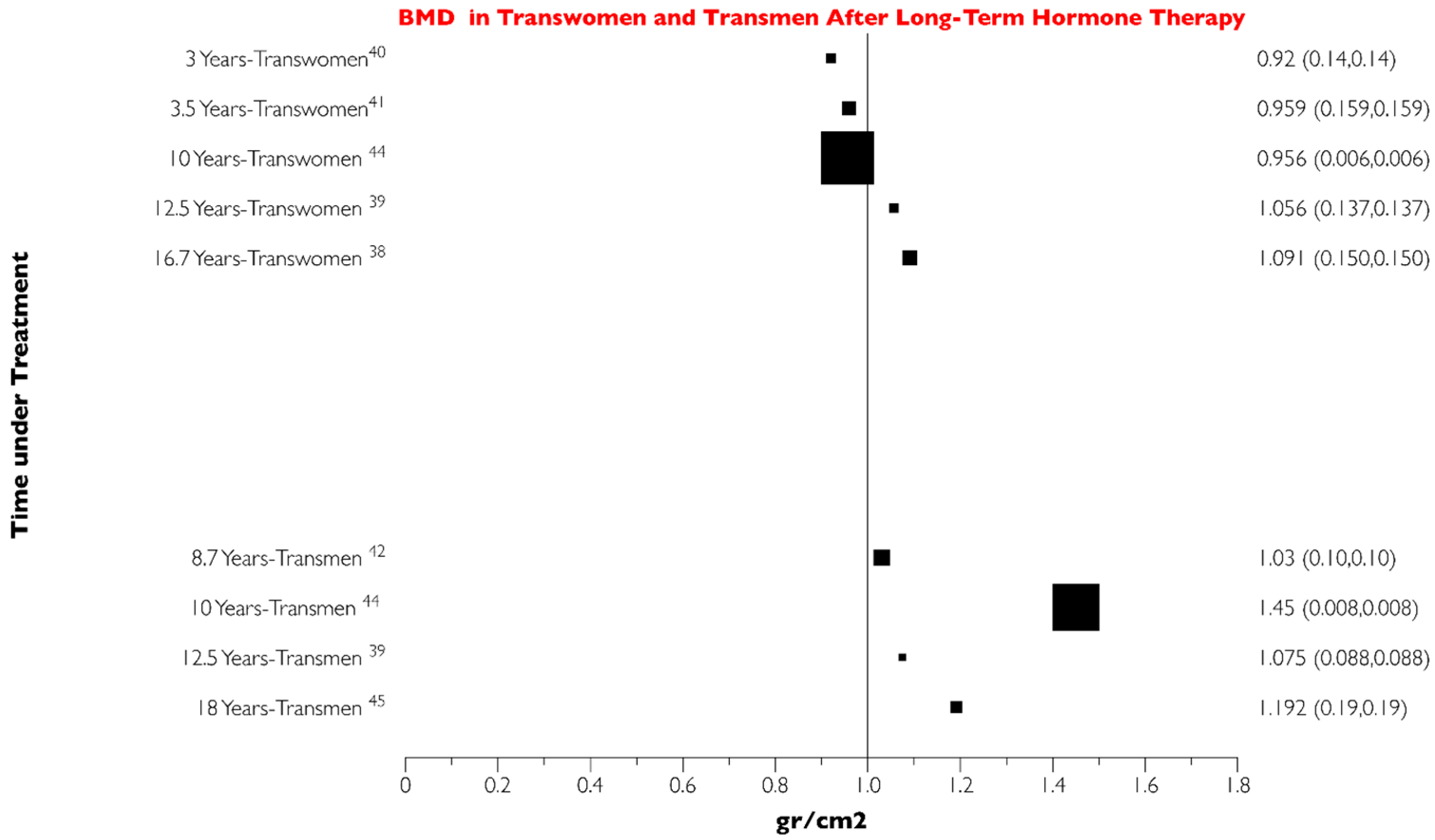
3.5. Bone Mineral Density (BMD), Method of Evaluation and Anatomical Areas Evaluated
3.6. Risk of Bias Assessment
4. Discussion
4.1. Transgender Demographics and Time under Treatment
4.2. Type of Pharmacotherapy Received and Dosage
4.3. Bone Metabolism Markers and Their Potential Effect on Implant Therapy
4.4. Two Main Bone Turnover Markers
4.5. Bone Mineral Density (BMD)
4.5.1. BMD Changes and their Potential Relationship to Dental Implants
4.5.2. Hypothesis for the Effects of Hormone Therapy for Transgender Patients on BMD and Its Potential Relation to Dental Implants
4.6. Strengths and Limitations of the Present Work
4.7. Recommended Future Steps
5. Conclusions
- Long-term pharmacotherapy for transgender patients does not alter the calcium, phosphate, alkaline phosphatase, and osteocalcin bone markers.
- Long-term pharmacotherapy for transgender patients will slightly increase the bone formation, expressed with increased PINP turnover markers.
- Long-term cross-sex pharmacotherapy for M to F transgender patients will produce a slight reduction in bone mineral density.
Author Contributions
Conflicts of Interest
References
- Beek, T.F.; Cohen-Kettenis, P.T.; Kreukels, B.P. Gender incongruence/gender dysphoria and its classification history. Int. Rev. Psychiatry 2016, 28, 5–12. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Levine, S.B. Ethical concerns about emerging treatment paradigms for gender dysphoria. J. Sex Marital Ther. 2018, 44, 29–44. [Google Scholar] [CrossRef]
- Ciccone, M.M.; Loverro, G.; Scicchitano, P.; Loverro, M.; Ricci, G.; Scaramuzzi, F.; Gesualdo, M.; Zito, A.; Campagna, M.; Moncelli, M.; et al. Surgical and pharmacological reassignment: Influence on transsexual cardiovascular risk profile. Intern. Med. J. 2017, 47, 1255–1262. [Google Scholar] [CrossRef] [PubMed]
- Factor, R.J.; Rothblum, E. Exploring gender identity and community among three groups of transgender individuals in the United States: MtFs, FtMs, and genderqueers. Health Sociol. Rev. 2008, 17, 235–253. [Google Scholar] [CrossRef]
- Wilczynski, C.; Emanuele, M.A. Treating a transgender patient: Overview of the guidelines. Postgrad. Med. 2014, 126, 121–128. [Google Scholar] [CrossRef]
- Levy, A.; Crown, A.; Reid, R. Endocrine intervention for transsexuals. Clin. Endocrinol. 2003, 59, 409–418. [Google Scholar] [CrossRef]
- Spack, N.P. Management of transgenderism. JAMA 2013, 309, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Gardner, I.H.; Safer, J.D. Progress on the road to better medical care for transgender patients. Curr. Opin. Endocrinol. Diabetes Obes. 2013, 20, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Hembree, W.C.; Cohen-Kettenis, P.; Delemarre-van de Waal, H.A.; Gooren, L.J.; Meyer, W.J., III; Spack, N.P.; Tangpricha, V.; Montori, V.M. Endocrine treatment of transsexual persons: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2009, 94, 3132–3154. [Google Scholar] [CrossRef]
- Meriggiola, M.C.; Berra, M. Safety of hormonal treatment in transgenders. Curr. Opin. Endocrinol. Diabetes Obes. 2013, 20, 565–569. [Google Scholar] [CrossRef] [PubMed]
- Klaver, M.; de Blok, C.J.M.; Wiepjes, C.M.; Nota, N.M.; Dekker, M.J.; de Mutsert, R.; Schreiner, T.; Fisher, A.D.; T’Sjoen, G.; Den Heijer, M. Changes in regional body fat, lean body mass and body shape in trans persons using cross-sex hormonal therapy: results from a multicenter prospective study. Eur. J. Endocrinol. 2018, 178, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Mueller, A.; Kiesewetter, F.; Binder, H.; Beckmann, M.W.; Dittrich, R. Long-term administration of testosterone undecanoate every 3 months for testosterone supplementation in female-to-male transsexuals. J. Clin. Endocrinol. Metab. 2007, 92, 3470–3475. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.P.; Madison, C.M.; Milne, N.M. Gonadal suppressive and cross-sex hormone therapy for gender dysphoria in adolescents and adults. Pharmacotherapy 2014, 34, 1282–1297. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, M.; Tangpricha, V. Osteoporosis and Bone Health in Transgender Persons. Endocrinol. Metab. Clin. N. Am. 2019, 48, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Clarke, B.L.; Khosla, S. Androgens and bone. Steroids 2009, 74, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Vandenput, L.; Ohlsson, C. Estrogens as regulators of bone health in men. Nat. Rev. Endocrinol. 2009, 5, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Cauley, J.A. Estrogen and bone health in men and women. Steroids 2015, 99 Pt A, 11–15. [Google Scholar] [CrossRef]
- Garnero, P.; Sornay-Rendu, E.; Claustrat, B.; Delmas, P.D. Biochemical markers of bone turnover, endogenous hormones and the risk of fractures in postmenopausal women: The OFELY study. J. Bone Miner. Res. 2000, 15, 1526–1536. [Google Scholar] [CrossRef]
- Szulc, P.; Naylor, K.; Pickering, M.E.; Hoyle, N.; Eastell, R.; Leary, E. Use of CTX-I and PINP as bone turnover markers: National Bone Health Alliance recommendations to standardize sample handling and patient preparation to reduce pre-analytical variability. Ann. Biol. Clin. 2018, 76, 373–391. [Google Scholar] [CrossRef]
- Kanis, J.A.; Melton, L.J., 3rd; Christiansen, C.; Johnston, C.C.; Khaltaev, N. The diagnosis of osteoporosis. J. Bone Miner. Res. 1994, 9, 1137–1141. [Google Scholar] [CrossRef]
- Biver, E. Use of bone turnover markers in clinical practice. Curr. Opin. Endocrinol. Diabetes Obes. 2012, 19, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Flores, A.R.; Herman, J.L.; Gates, G.J.; Brown, T.N. How Many Adults Identify as Transgender in the United States? The Williams Institute: Los Angeles, CA, USA, 2016; Available online: http://williamsinstitute.law.ucla.edu/wp-content/uploads/How-Many-Adults-Identify-as-Transgender-in-the-United-States.pdf (accessed on 20 February 2019).
- Glen, F.; Hurrell, K. Technical Note: Measuring Gender Identity; Equality and Human Rights Commission: Manchester, UK, 2012. [Google Scholar]
- Van Caenegem, E.; Wierckx, K.; Elaut, E.; Buysse, A.; Dewaele, A.; van Nieuwerburgh, F.; de Cuypere, G.; T’Sjoen, G. Prevalence of gender nonconformity in Flanders, Belgium. Arch. Sex. Behav. 2015, 44, 1281–1287. [Google Scholar] [CrossRef] [PubMed]
- Kuyper, L.; Wijsen, C. Gender identities and gender dysphoria in the Netherlands. Arch. Sex. Behav. 2014, 43, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Winter, S.; Diamond, M.; Green, J.; Karasic, D.; Reed, T.; Whittle, S.; Wylie, K. Transgender people: Health at the margins of society. Lancet 2016, 388, 390–400. [Google Scholar] [CrossRef]
- Chipkin, S.R.; Kim, F. Ten most important things to know about caring for transgender patients. Am. J. Med. 2017, 130, 1238–1245. [Google Scholar] [CrossRef]
- Heima, M.; Heaton, L.J.; Ng, H.H.; Roccoforte, E.C. Dental fear among transgender individuals: A cross sectional survey. Spec. Care Dent. 2017, 37, 212–222. [Google Scholar] [CrossRef] [PubMed]
- More, F.G.; Whitehead, A.W.; Gonthier, M. Strategies for student services for lesbian, gay, bisexual, and transgender students in dental schools. J. Dent. Educ. 2004, 68, 623–632. [Google Scholar]
- Temple, H.; Inglehart, M.R. LGBT coverage in U.S. dental schools and dental hygiene programs: Results of a national survey. J. Dent. Educ. 2016, 80, 1440–1449. [Google Scholar]
- Russell, S.; More, F. Addressing health disparities via coordination of care and interprofessional education: Lesbian, gay, bisexual, and transgender health and oral health care. Dent. Clin. 2016, 60, 891–906. [Google Scholar]
- Nishimura, B.J. Treatment considerations for a full mouth reconstruction of a transgender patient. Compend. Contin. Educ. Dent. 2017, 38, 544–551. [Google Scholar]
- Ludwig, D.C.; Morrison, S.D. Should dental care make a transition? J. Am. Dent. Assoc. 2018, 149, 79–80. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Sterne, J.A.C.; Savović, J.; Page, M.J.; Hróbjartsson, A.; Boutron, I.; Reeves, B.; Eldridge, S. A revised tool for assessing risk of bias in randomized trials. Cochrane Database Syst. Rev. 2016, 10 (Suppl. 1), 29–31. [Google Scholar] [CrossRef]
- Schlatterer, K.; Auer, D.; Yassouridis, A.; von Werder, K.; Stalla, G. Transsexualism and osteoporosis. Exp. Clin. Endocrinol. Diabetes 1998, 106, 365–368. [Google Scholar] [CrossRef] [PubMed]
- Sosa, M.; Jódar, E.; Arbelo, E.; Domínguez, C.; Saavedra, P.; Torres, A.; Salido, E.; Gómezde Tejada, M.J.; Hernández, D. Bone mass, bone turnover, vitamin, D.; and estrogen receptor gene polymorphisms in male to female transsexuals: Effects of estrogenic treatment on bone metabolism of the male. J. Clin. Densitom. 2003, 6, 297–304. [Google Scholar] [CrossRef]
- Ruetsche, A.G.; Kneubuehl, R.; Birkhaeuser, M.H.; Lippuner, K. Cortical and trabecular bone mineral density in transsexuals after long-term cross-sex hormonal treatment: A cross-sectional study. Osteoporos Int. 2005, 16, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Lapauw, B.; Taes, Y.; Simoens, S.; Van Caenegem, E.; Weyers, S.; Goemaere, S.; Toye, K.; Kaufman, J.M.; T’Sjoen, G.G. Body composition, volumetric and areal bone parameters in male-to-female transsexual persons. Bone 2008, 43, 1016–1021. [Google Scholar] [CrossRef]
- T’Sjoen, G.; Weyers, S.; Taes, Y.; Lapauw, B.; Toye, K.; Goemaere, S.; Kaufman, J. Prevalence of low bone mass in relation to estrogen treatment and body composition in male-to-female transsexual persons. J. Clin. Densitom. 2009, 12, 306–313. [Google Scholar] [CrossRef]
- Van Caenegem, E.; Wierckx, K.; Taes, Y.; Dedecker, D.; Van de Peer, F.; Toye, K.; Kaufman, J.M.; T’Sjoen, G. Bone mass, bone geometry, and body composition in female-to-male transsexual persons after long-term cross-sex hormonal therapy. J. Clin. Endocrinol. Metab. 2012, 97, 2503–2511. [Google Scholar] [CrossRef] [PubMed]
- Wierckx, K.; Mueller, S.; Weyers, S.; Van Caenegem, E.; Roef, G.; Heylens, G.; T’Sjoen, G. Long-term evaluation of cross-sex hormone treatment in transsexual persons. J. Sex. Med. 2012, 9, 2641–2651. [Google Scholar] [CrossRef]
- Wiepjes, C.M.; de Jongh, R.T.; de Blok, C.J.; Vlot, M.C.; Lips, P.; Twisk, J.W.; den Heijer, M. Bone safety during the first ten years of gender-affirming hormonal treatment in transwomen and transmen. J. Bone Miner. Res. 2018, 34, 447–454. [Google Scholar] [CrossRef]
- Broulik, P.D.; Urbánek, V.; Libanský, P. Eighteen-year effect of androgen therapy on bone mineral density in trans(gender) men. Horm. Metab. Res. 2018, 50, 133–137. [Google Scholar] [CrossRef]
- Langdahl, B.; Ferrari, S.; Dempster, D.W. Bone modeling and remodeling: Potential as therapeutic targets for the treatment of osteoporosis. Ther. Adv. Musculoskelet. Dis. 2016, 8, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.B.; Minami, K.; Raposo, J.F.; Matsuura, N.; Koizumi, M.; Yokota, H.; Ferreira, H.G. Transient modulation of calcium and parathyroid hormone stimulates bone formation. Endocrine 2016, 54, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Body, J.; Niepel, D.; Tonini, G. Hypercalcaemia and hypocalcaemia: Finding the balance. Support. Care Cancer 2017, 25, 1639–1649. [Google Scholar] [CrossRef] [PubMed]
- Okyay, E.; Ertugrul, C.; Acar, B.; Sisman, A.R.; Onvural, B.; Ozaksoy, D. Comparative evaluation of serum levels of main minerals and postmenopausal osteoporosis. Maturitas 2013, 76, 320–325. [Google Scholar] [CrossRef]
- Katsumata, S.; Matsuzaki, H.; Uehara, M.; Suzuki, K. Effects of dietary calcium supplementation on bone metabolism, kidney mineral concentrations, and kidney function in rats fed a high-phosphorus diet. J. Nutr. Sci. Vitaminol. 2015, 61, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Szulc, P.; Bauer, D.C. Biochemical markers of bone turnover in osteoporosis. In Osteoporosis, 4th ed.; Marcus, R., Feldman, D., Dempster, D.W., Cauley, J., Feldman, D., Eds.; Academic Press: Cambridge, MA, USA, 2013; pp. 1573–1610. [Google Scholar]
- Garnero, P.; Delmas, P.D. Assessment of the serum levels of bone alkaline phosphatase with a new immunoradiometric assay in patients with metabolic bone disease. J. Clin. Endocrinol. Metab. 1993, 77, 1046–1053. [Google Scholar]
- Mizokami, A.; Kawakubo-Yasukochi, T.; Hirata, M. Osteocalcin and its endocrine functions. Biochem. Pharmacol. 2017, 132, 1–8. [Google Scholar] [CrossRef]
- Ensrud, K.E. Epidemiology of fracture risk with advancing age. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 68, 1236–1242. [Google Scholar] [CrossRef]
- Moyer, V.A.; U.S. Preventive Services Task Force. Vitamin D and calcium supplementation to prevent fractures in adults: U.S. Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2013, 158, 691–696. [Google Scholar]
- Fanghänel, J.; Gedrange, T.; Proff, P. Bone quality, quantity and metabolism in terms of dental implantation. Biomed. Eng. 2008, 53, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Reid, I.R.; Ames, R.; Mason, B.; Reid, H.E.; Bacon, C.J.; Bolland, M.J.; Gamble, G.D.; Grey, A.; Horne, A. Randomized controlled trial of calcium supplementation in healthy, non-osteoporotic, older men. Arch. Intern. Med. 2008, 168, 2276–2282. [Google Scholar] [CrossRef] [PubMed]
- Riggs, B.L.; O’Fallon, W.M.; Muhs, J.; O’Connor, M.K.; Kumar, R.; Melton, L.J., III. Long-term effects of calcium supplementation on serum parathyroid hormone level, bone turnover, and bone loss in elderly women. J. Bone Miner. Res. 1998, 13, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Vasikaran, S.; Cooper, C.; Eastell, R.; Griesmacher, A.; Morris, H.; Trenti, T.; Kanis, J. International Osteoporosis Foundation and International Federation of Clinical Chemistry and Laboratory Medicine position on bone marker standards in osteoporosis. Clin. Chem. Lab. Med. 2011, 49, 1271–1274. [Google Scholar] [CrossRef] [PubMed]
- Szulc, P. Bone turnover: Biology and assessment tools. Best Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 725–738. [Google Scholar] [CrossRef]
- Basler, S.; Traxler, J.; Müller, R.; van Lenthe, G. Peri-implant bone microstructure determines dynamic implant cut-out. Med. Eng. Phys. 2013, 35, 1442–1449. [Google Scholar] [CrossRef] [PubMed]
- Schiuma, D.; Brianza, S.; Tami, E. Development of a novel method for surgical implant design optimization through noninvasive assessment of local bone properties. Med. Eng. Phys. 2011, 33, 256–262. [Google Scholar] [CrossRef]
- Javed, F.; Ahmed, H.; Crespi, R.; Romanos, G. Role of primary stability for successful osseointegration of dental implants: Factors of influence and evaluation. Interv. Med. Appl. Sci. 2013, 5, 162–167. [Google Scholar] [CrossRef]
- Wilson, T.G., Jr.; Miller, R.J.; Trushkowsky, R.; Dard, M. Tapered Implants in dentistry: Revitalizing Concepts with technology: A review. Adv. Dent. Res. 2016, 28, 4–9. [Google Scholar] [CrossRef]
- Stocchero, M.; Toia, M.; Cecchinato, D.; Becktor, J.; Coelho, P.; Jimbo, R. Biomechanical, biologic, and clinical outcomes of undersized implant surgical preparation: A systematic review. Int. J. Oral Maxillofac. Implant. 2016, 31, 1247–1263. [Google Scholar] [CrossRef]
- Guobis, Z.; Pacauskiene, I.; Astramskaite, I. General diseases influence on peri-Implantitis development: A systematic review. J. Oral Maxillofac. Res. 2016, 7, e5. [Google Scholar] [CrossRef]
- Dereka, X.; Calciolari, E.; Donos, N.; Mardas, N. Osseointegration in osteoporotic-like condition: A systematic review of preclinical studies. J. Periodontal Res. 2018, 53, 933–940. [Google Scholar] [CrossRef]
- Radi, I.; Ibrahim, W.; Iskandar, S.; AbdelNabi, N. Prognosis of dental implants in patients with low bone density: A systematic review and meta-analysis. J. Prosthet. Dent. 2018, 120, 668–677. [Google Scholar] [CrossRef]
- De Medeiros, F.; Kudo, G.; Leme, B.; Saraiva, P.; Verri, F.; Honório, H.; Pellizzer, E.; Santiago Junior, J. Dental implants in patients with osteoporosis: A systematic review with meta-analysis. Int. J. Oral Maxillofac. Surg. 2018, 47, 480–491. [Google Scholar] [CrossRef] [PubMed]
- Famili, P.; Zavoral, J. Low Skeletal Bone Mineral Density Does Not Affect Dental Implants. J. Oral Implantol. 2015, 41, 550–553. [Google Scholar] [CrossRef]
- Marquezan, M.; Osório, A.; Sant’Anna, E.; Souza, M.; Maia, L. Does bone mineral density influence the primary stability of dental implants? A systematic review. Clin. Oral Implants. Res. 2012, 23, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Unger, C. Hormone therapy for transgender patients. Transl. Androl. Urol. 2016, 5, 877–884. [Google Scholar] [CrossRef]
- He, J.; Zhao, B.; Deng, C.; Shang, D.; Zhang, C. Assessment of implant cumulative survival rates in sites with different bone density and related prognostic factors: An 8-year retrospective study of 2,684 implants. Int. J. Oral Maxillofac. Implants 2015, 30, 360–371. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author, Year of Publication, Location | Sample | Time Receiving the Treatment | Hormone and Dosage | Method of Evaluation for the Bone Mineral Density (BMD) and Area of Evaluation | Bone Mineral Density (Adjusted) | Study Conclusions Related to Bone Structure, Bone Metabolism and BMD | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| M to F Transwomen | F to M Transmen | M to F | F to M | Before OR Controls | After OR Test | |||||
| Schlatterer K et al. 1998 [37] Berlin, Germany | 10 | 10 | 11.5 years | Parenteral high doses of estrogens + Cyproterone Acetate or Estrogens alone (2–8 mg/day) | Parenteral testosterone esters (250 mg every 2–4 weeks) | Conventional whole-body CT scanner | M to F | 195 ± 20 mgr/ccm | 174 ± 3 mgr/ccm | Slight reduction in the BMD of M to F M to F and F to M transsexuals treated with the proposed cross-gender hormone concept possess low risk of osteoporotic change |
| F to M | 174 ± 3 mgr/ccm | 172 ± 2 mgr/ccm | ||||||||
| Sosa M et al. 2003 [38] Canary Islands, Spain | 53 | - | 201 ± 108 months or (16.75 ± 9) years | Ethinyl oestradiol + ciproterone acetate, -Oral estrogens and oestradiol valerate Specific dosages were not provided | - | Densitometer BMD of the lumbar spine and femoral neck | M to F | Lumbar Spine 1.002 ± 0.155 (gr/cm2) | Lumbar Spine 1.091 ± 0.150 (gr/cm2) | The chronic administration of estrogens in men may produce an increase in serum estradiol, a decrease in free testosterone levels, and an increase in BMD—Both in lumbar spine and in femoral neck. This study suggests that the bone of adult men is sensitive to estrogens. |
| Femoral Neck 0.808 ± 0.135 (gr/cm2) | Femoral Neck 0.904 ± 0.135 (gr/cm2) | |||||||||
| Ruetsche AG et al. 2005 [39] Berne, Switzerland | 24 | 15 | 12.5 years M-F 2.1 years before surgery and 9.7 years after surgery F-M 1.3 Years before surgery and 6.1 years after surgery | Cyproterone acetate 2 mg/day + Ethinyl estradiol 35 µg/day or a free combination of Cyproterone acetate 2 mg/day + Ethinyl estradiol 35–100 µg/day After surgery, Estradiol valerate or Micronized 17-beta estradiol 2–4 mg/day. | Parenteral testosterone esters 250 mg/IM every 3 weeks Continued after surgery | Dual-energy X-ray absorptiometry (DXA) BMD of the lumbar spine, femoral neck, whole body, distal epiphysis, and other 5 areas | M to F | Lumbar spine 1.078 ± 0.131 (gr/cm2) | Lumbar spine 1.056 ± 0.137 (gr/cm2) | Biochemical values of calcium phosphate metabolism parameters were within normal ranges and comparable across groups. In transsexual genetic males and females under long term cross-sex hormone treatment, BMD values are generally preserved or increased. Non-compliance with cross-sex hormone treatment may lead to low BMD, only in genetic males. IGF-1 (Insulin like growth factor) could play a role in the mediation of the effect of androgens on bone in F-M transsexuals. |
| Femoral neck 0.835 ± 0.100 (gr/cm2) | Femoral Neck 0.774 ± 0.095 (gr/cm2) | |||||||||
| - | Whole body 1.216 ± 0.098 (gr/cm2) | |||||||||
| F to M | Lumbar spine 1.100 ± 0.139 (gr/cm2) | Lumbar spine 1.075 ± 0.088 (gr/cm2) | ||||||||
| Femoral neck 0.937 ± 0.121 (gr/cm2) | Femoral Neck 0.842 ± 0.058 (gr/cm2) | |||||||||
| - | Whole body 1.179 ± 0.035 (gr/cm2) | |||||||||
| Lapauw B et al. 2008 [40] Ghent, Belgium | 23 | - | >3 years At least 3 years under hormone treatment. Al the patients had sex reassignment surgery | Before surgery Cyproterone acetate 50–100 mg/day + ethinyl estradiol 25–50 μg/day After surgery either: -Ethinyl estradiol 25–50 μg/day (8 participants) -Estradiol valerate 2 mg/day (10 participants) -Conjugated equine estrogens1.25 mg/day (2 participants) -Transdermal estradiol gels (3 persons) | - | Dual-energy X-ray absorptiometry (DXA) BMD at the lumbar spine, distal forearm and Peripheral quantitative computed tomography (pQCT), at the same areas for analysis of the bone architecture | M to F | Lumbar spine 1.05 ± 0.11 (gr/cm2) | Lumbar spine 0.92 ± 0.14 (gr/cm2) | M to F transsexual persons presents: Lower muscle mass and strength and higher fat mass Lower trabecular bone density and BMD at various sites and smaller cortical bone size as compared to healthy age- and height-matched controls. The lower level of sports-related physical activity as well as the pharmacological and surgical withdrawal from endogenous T production could contribute to these findings. Male-to-female transsexuals may be at increased risk for developing osteoporosis and related fractures. Bone health should be a parameter of interest in the long-term follow-up care for male-to-female transsexual persons. |
| Distal forearm 0.49 ± 0.05 (gr/cm2) | Distal forearm 0.42 ± 0.07 (gr/cm2) | |||||||||
| T’Sjoen G et al. 2009 [41] Ghent, Belgium | 50 | - | >3 years and at least 1 year after sex reassignment | Cyproterone acetate 50–100 mg/day (1 year) + exogenous estrogen administration | - | Dual-energy X-ray absorptiometry (DXA) BMD at the lumbar spine, proximal femur and the distal radius of the nondominant site AND pQCT for the analysis of bone architecture | M to F | - | Lumbar spine 0.959 ± 0.159 | Low bone mass, smaller bone size, and reduced muscle mass. Are highly prevalent in the described group of M-F transsexual persons Androgen deficiency or an inadequate estrogen dosage could be the cause Hormonal protocols differ between different centers and individual changes in BMD are highly variable There is a need for longitudinal single- and multi-center data on low bone mass risk in the M/F transsexual group. |
| Total hip 0.940 ± 0.150 | ||||||||||
| Radius and 0.432 ± 0.077 | ||||||||||
| Van Caenegem, et al. 2012 [42] Ghent, Belgium | - | 66 50 undergone surgery and received hormone therapy 16 Just hormone therapy | 8.7 years after sex reassignment surgery (SRS) with a minimum of 9 months and a maximum of 22 years. | - | Testosterone decanoate 100 mg, Testosterone isocaproate OR fenylpropionate 60 mg, Testosterone propionate 30 mg/mL; 2–3 weeks (35 patients); Testosterone undecanoate 1000 mg; 12 weeks (7 patients); Transdermal testosterone 50 mg daily (8 patients) Testosterone undecanoate 40 mg/day + testosterone gel 50 mg per 5 g, 50 mg daily (1 Patient) | Dual-energy X-ray absorptiometry (DXA); BMD at the lumbar spine, and left proximal femur (total hip and femoral neck region) | F to M | Lumbar spine 1.06 ± 0.11 (gr/cm2) | Lumbar spine 1.03 ± 0.10 (gr/cm2) | Transmen (F-M) with hormone treatment and after SRS possess a bone and body composition comparable to men, compared with age-matched female controls. This is less fat mass, more central pattern of adiposity, more muscle mass, strength, and larger cortical bone size. The differences may result from the effects of long-term testosterone administration and of diminished estrogen exposure and/or from indirect effects through muscle mass and strength. Transsexual men (F to M) on long-term hormonal therapy do not have an increased risk of low bone mass but associated cardiovascular risk factors are important to address. |
| Femoral neck 0.84 ± 0.10 (gr/cm2) | Femoral neck 0.82 ± 0.11 (gr/cm2) | |||||||||
| Total hip 0.95 ± 0.10 (gr/cm2) | Total hip 0.96 ± 0.12 (gr/cm2) | |||||||||
| Wierckx K et al. 2012 [43] Ghent, Belgium | 50 | 50 | ±10 years | Before surgery Cyproterone acetate 50–100 mg/day/1 year different +exogenous estrogen After surgery all received estrogens (3 patients did not followed the estrogen protocol) | Testosterone | Dual-energy X-ray absorptiometry (DXA); BMD at the lumbar spine, at the proximal femur (total hip region), and a both distal forearms | M to F | Data not shown | Data not shown | After an average of 10 years of hormone treatment no important side effects were reported and osteoporosis was not observed in transsexual men (F to M). Transsexual women (M to F) suffered from osteoporosis at the lumbar spine and distal arm. Twelve percent of transsexual women (M to F) experienced thromboembolic and/or other cardiovascular events during hormone treatment, possibly related to older age, estrogen treatment, and lifestyle factors. In order to decrease cardiovascular morbidity, more attention should be paid to decrease cardiovascular risk factors during hormone therapy management. |
| F to M | Data not shown | Data not shown | ||||||||
| Wiepjes C et al. 2018 [44] Amsterdam, Netherland | 711 | 543 | 10 years | Oral or transdermal estrogens and anti-androgens until gonadectomy | Oral, transdermal, or intramuscular testosterone. | Dual-energy X-ray absorptiometry (DEXA) at 2, 5, and 10 years Absolute BMD | M to F | Male and Female adult reference population | 0.956 (+0.006) (gr/cm2) | This study showed that hormone therapy does not negatively affect the BMD Regularly assessing BMD should be completed just when osteoporotic risk is present (>60 years age) High percentage of low BMD was found prior to hormone therapy in transwomen. Therefore, evaluation of BMD before start of hormone therapy may be considered. |
| F to M | Male and Female adult reference population | 1.45 (+0.008) (gr/cm2) | ||||||||
| Broulik PD et al. 2018 [45] Prague, Czech Republic | - | 35 | 18 years | - | Before surgery Testosterone isobutyrate Sex reassignment surgery (hysterectomy, ovariectomy, and bilateral mastectomy) After surgery Testosterone isobutyrate 25 mg intramuscular every week, OR Testosterone propionate 250 mg every third week intramuscular OR Testosterone undecanoate 40 mg 4 times day. | Dual-energy X-ray absorptiometry (DXA); BMD at the lumbar spine and femoral neck | F to M | Male controls | Lumbar spine 1.213 ± 0.15 | BMD after adequate dose of testosterone therapy is higher after 18 years of testosterone administration BMD at the spine its similar to baseline after 18 years of testosterone administration. Androgens compensate for the low estrogen level in the bone metabolism |
| Lumbar spine 1.203 ± 0.065 | ||||||||||
| Femoral neck 1.192 ± 0.19 | ||||||||||
| Female controls | Femoral neck 0.950 ± 0.11 | |||||||||
| Lumbar spine 1.192 ± 0.19 | ||||||||||
| Femoral neck 0.822 ± 0.09 | ||||||||||
| Summary of Findings | M to F 921 | F to M 719 | Time Receiving the Treatment (Range) >3 years to 18 years | M to F Hormone Therapy Cyproterone Acetate (Antiandrogen) Estrogens | F to M Hormone Therapy Testosterone | BMD Method of Evaluation Conventional whole-body scanner; Dual-energy X-ray absorptiometry (DXA) | - | - | BMD Contradictory results, the BMD was preserved or increased in 788 M to F patients (82.66%); BMD decreased in 73 M to F patients (8.47%); BMD Increased in 35 F to M patients (4.93%); BMD preserved in 674 F to M patients (95.06%) | |
| Author and Year of Publication | Sample | Bone Metabolism Markers | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| M to F | F to M | Calcium (mmol/L) or (mg/dL) | Phosphate (mmol/L) | Alkaline phosphatase (U/L) | Osteocalcin (µg/L) or (ng/mL) | ||||||
| Before or Controls | After or Tests | Before or Controls | After or Tests | Before or Controls | After or Tests | Before or Controls | After or Tests | ||||
| Schlatterer K et al. 1998 [37] | 10 | 10 | M to F | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated |
| F to M | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | |||||
| Sosa M et al. 2003 [38] | 53 | - | M to F | 9.4 ± 0.520 mg/dL | 9.156 ± 0.564 mg/dL | 3.348 ± 0.457 mg/dL | 3.16 ± 0.619 (mg/dL) | Not evaluated | Not evaluated | Not evaluated | Not evaluated |
| Ruetsche AG et al. 2005 [39] | 24 | 15 | M to F | 2.10–2.55 mmol/L | 2.33 ± 0.08 (2.18–2.53) mmol/L | 0.74–1.55 mmol/L | 1.15 ± 0.12 (0.76–1.49) (mmol/L) | 36–108 (μkat/L) | 63 ± 15 (32–159) (μkat/L) | 2.3–13.8 (ng/mL) | 5.0 ± 1.0 (2.3–9.1) (ng/mL) |
| F to M | 2.10–2.55 mmol/L | 2.38 ± 0.02 (2.32–2.52) mmol/L | 0.74–1.55 mmol/L | 1.05 ± 0.08 (0.69–1.23) (mmol/L) | 36–120 (μkat/L) | 6.3 ± 1.5 (3.4–11.4) (μkat/L) | 1.2–10.5 (ng/mL) | 6.3 ± 1.5 (3.4–11.4) (ng/mL) | |||
| Lapauw B et al. 2008 [40] | 23 | - | M to F | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated |
| T’Sjoen G et al. 2009 [41] | 50 | M to F | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | |
| Van Caenegem, et al. 2012 [42] | - | 66 | F to M | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated |
| Wierckx K et al. 2012 [43] | 50 | 50 | T to F | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated |
| F to M | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | |||
| Wiepjes C et al. 2018 [44] | 711 | 543 | M to F | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated |
| F to M | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | |||
| Broulik PD et al. 2018 [45] | - | 35 | F to M | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Female controls 1.51 ± 0.10 (μkat/L) | 1.48 ± 0.12 (μkat/L) | Female controls 24.05 ± 6.8 (µg/L) | 22.04 ± 7.92 (µg/L) |
| Male controls 1.39 ± 0.14 (μkat/L) | Male controls 23.5 ± 8.0 (µg/L) | ||||||||||
| Author and Year of Publication | Sample | Bone Turnover Markers | |||||
|---|---|---|---|---|---|---|---|
| M to F | F to M | Serum Procollagen Type I N-Terminal Propeptide (P1NP) Formation (ng/mL) | Serum Collagen type I Crosslinked C-Telopeptide (CTX) Resorption (ng/mL) | ||||
| Before or Controls | After or Tests | Before or Controls | After or Tests | ||||
| Schlatterer K et al. 1998 [37] | 10 | 10 | M to F | M to F | Not evaluated | Not evaluated | Not evaluated |
| F to M | F to M | Not evaluated | Not evaluated | Not evaluated | |||
| Sosa M et al. 2003 [38] | 53 | - | M to F | Not evaluated | Not evaluated | Not evaluated | Not evaluated |
| Ruetsche AG et al. 2005 [39] | 24 | 15 | M to F | Not evaluated | Not evaluated | Not evaluated | Not evaluated |
| F to M | Not evaluated | Not evaluated | Not evaluated | Not evaluated | |||
| Lapauw B et al. 2008 [40] | 23 | - | M to F | 32 [24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45] (46 controls) | 49 [36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62] (23 patients) | 0.36 ± 0.16 (46 controls) | 0.24 ± 0.14 (23 patients) |
| T’Sjoen G et al. 2009 [41] | 50 | - | M to F | Lumbar spine 36.6 ± 22.6 | Lumbar spine 45.2 ± 24.4 | 0.31 ± 0.20 | 0.32 ± 0.23 |
| Van Caenegem, et al. 2012 [42] | - | 66 | F to M Before Surgery | 40 ± 12 | 50 ± 24 | 0.20 ± 0.10 | 0.36 ± 0.15 |
| Wierckx K et al. 2012 [43] | 50 | 50 | M to F | 102 ng/mL | 106–125 (ng/mL) (2 patients, all the others were within normal ranges) | <0.58 (ng/dL) | 0.62–1.24 (ng/dL) (4 patients, all the others were within normal ranges) |
| F to M | Normal range | Normal range | Normal range | Normal range | |||
| Wiepjes C et al. 2018 [44] | 711 | 543 | M to F | Not evaluated | Not evaluated | Not evaluated | Not evaluated |
| F to M | Not evaluated | Not evaluated | Not evaluated | Not evaluated | |||
| Broulik PD et al. 2018 [45] | - | 35 | F to M | Not evaluated | Not evaluated | Control Female 400 ± 124 | 302 ± 190 |
| Control Male 390 ± 140 | |||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delgado-Ruiz, R.; Swanson, P.; Romanos, G. Systematic Review of the Long-Term Effects of Transgender Hormone Therapy on Bone Markers and Bone Mineral Density and Their Potential Effects in Implant Therapy. J. Clin. Med. 2019, 8, 784. https://doi.org/10.3390/jcm8060784
Delgado-Ruiz R, Swanson P, Romanos G. Systematic Review of the Long-Term Effects of Transgender Hormone Therapy on Bone Markers and Bone Mineral Density and Their Potential Effects in Implant Therapy. Journal of Clinical Medicine. 2019; 8(6):784. https://doi.org/10.3390/jcm8060784
Chicago/Turabian StyleDelgado-Ruiz, Rafael, Patricia Swanson, and Georgios Romanos. 2019. "Systematic Review of the Long-Term Effects of Transgender Hormone Therapy on Bone Markers and Bone Mineral Density and Their Potential Effects in Implant Therapy" Journal of Clinical Medicine 8, no. 6: 784. https://doi.org/10.3390/jcm8060784
APA StyleDelgado-Ruiz, R., Swanson, P., & Romanos, G. (2019). Systematic Review of the Long-Term Effects of Transgender Hormone Therapy on Bone Markers and Bone Mineral Density and Their Potential Effects in Implant Therapy. Journal of Clinical Medicine, 8(6), 784. https://doi.org/10.3390/jcm8060784